

Volume 4, Issue 3 (Spring 2019)
Health in Emergencies and Disasters Quarterly 2019, 4(3): 157-164 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Kheyrati L, Keshvari H, Fatehi F, Hemmati M, Khankeh H, Habibisaravi R et al . Presenting a Model for Telemedicine in Earthquake for Iran. Health in Emergencies and Disasters Quarterly 2019; 4 (3) :157-164
URL: http://hdq.uswr.ac.ir/article-1-258-en.html
URL: http://hdq.uswr.ac.ir/article-1-258-en.html
Leila Kheyrati1 

 , Hamid Keshvari 2, Farhad Fatehi3 , Masoud Hemmati4 , Hamidreza Khankeh5 , Reza Habibisaravi6 , Mohammadreza Kheyrati7
, Hamid Keshvari 2, Farhad Fatehi3 , Masoud Hemmati4 , Hamidreza Khankeh5 , Reza Habibisaravi6 , Mohammadreza Kheyrati7
, Hamid Keshvari 2, Farhad Fatehi3 , Masoud Hemmati4 , Hamidreza Khankeh5 , Reza Habibisaravi6 , Mohammadreza Kheyrati7
1- Manager of Medical Care Monitoring Center (MCMC), Ministry of health and Medical Education, Tehran, Iran.
2- Faculty of Medical Engineering, Amirkabir University, Tehran, Iran. , hamid.keshvari@yahoo.com
3- Center for online Health, The University of Queensland, Brisbane, Australia.; & Adjunct Fellow, Tehran University of Medical Sciences, Tehran, Iran.
4- Head of Information Technology Center, Islamic Azad University, Tehran, Iran.
5- Postdoc Fellow, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
6- Information and Communication Technology Administration, Mazandaran University of Medical Sciences, Sari, Iran.
7- Information Technology Management, Information Technology Center, Islamic Azad University, Tehran, Iran.
2- Faculty of Medical Engineering, Amirkabir University, Tehran, Iran. , hamid.keshvari@yahoo.com
3- Center for online Health, The University of Queensland, Brisbane, Australia.; & Adjunct Fellow, Tehran University of Medical Sciences, Tehran, Iran.
4- Head of Information Technology Center, Islamic Azad University, Tehran, Iran.
5- Postdoc Fellow, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
6- Information and Communication Technology Administration, Mazandaran University of Medical Sciences, Sari, Iran.
7- Information Technology Management, Information Technology Center, Islamic Azad University, Tehran, Iran.
Full-Text [PDF 609 kb]
(1149 Downloads)
| Abstract (HTML) (3879 Views)

All key themes of telemedicine in the disaster were extracted from articles. With the discussion in the expert panel of 10 selected professionals, all elements were categorized as 6 key themes with 38 subthemes. The participants gave a score to all items from 1 to 5. Mean, median, mode, and standard deviation values of each item were calculated. Finally, themes and subthemes were ranked by mean scores.
In the second phase, a group of 35 selected volunteer experts (Table 2) enrolled in Delphi to finalize the initial framework. A researcher-made questionnaire was used for data collection, which was validated by face validity, and its reliability was positively evaluated by the Cochran’s formula with the Cronbach alpha coefficient of 0.911. The participants scored each item from 1 to 10 for the final scoring and ranking. At the end of this phase, the applicable model of telemedicine in the disaster was determined.

Subsequently, in the third phase, the second round of Delphi with 29 remaining experts performed to finalize modeling of telemedicine in disasters with the focus on the earthquake. SPSS V. 18 was used for doing statistical analyses and preparing descriptive results.
3. Results
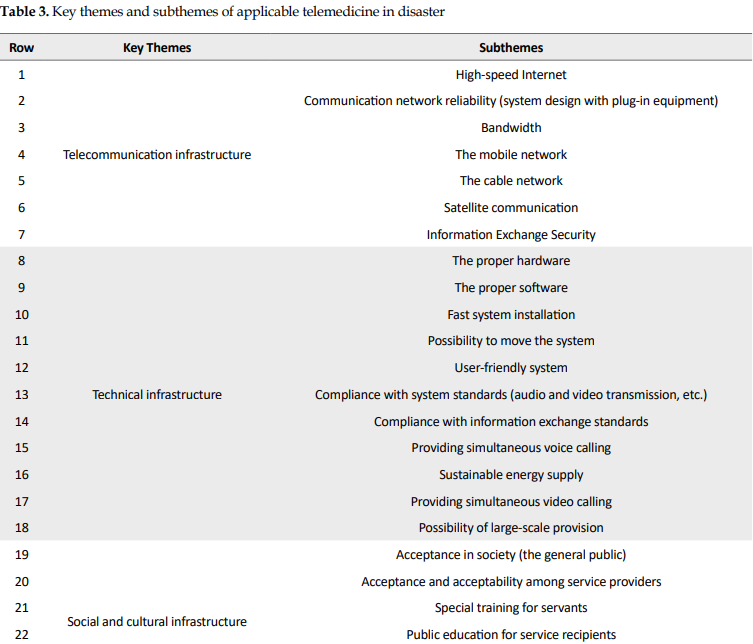
According to the first phase of the study, 6 key themes with 38 subthemes of applicable telemedicine for implementing in the disaster were obtained. Technical infrastructure with 11 subthemes and financial infrastructure with 4 subthemes had maximum and minimum subthemes, respectively (Table 3).
In this phase, 5 subthemes were removed from the criteria because they obtained scores less than expectation. The “cable network” subtheme from telecommunication infrastructure theme, “acceptance in society” (the general public) and “public education for service recipients” subthemes from social and cultural infrastructure theme, the “cost-effective service delivery” and “fee for service providers” subthemes from financial infrastructure theme were removed from the criteria.
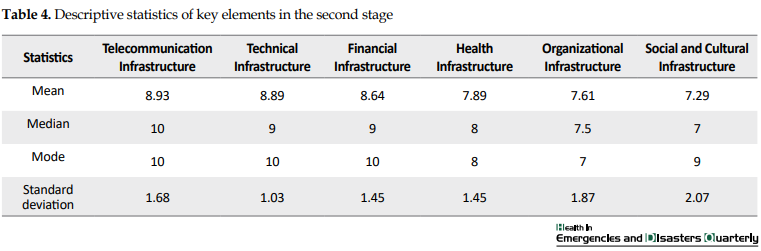
In the third phase, validation of the model was performed after rearranging subthemes. In this phase, the remaining 28 participated experts scored key themes and subthemes. Then, the highest priority went to telecommunication infrastructure with a maximum score of 9.24 and least priority to social and cultural infrastructure theme with a minimum score of 7.53 (Table 5).
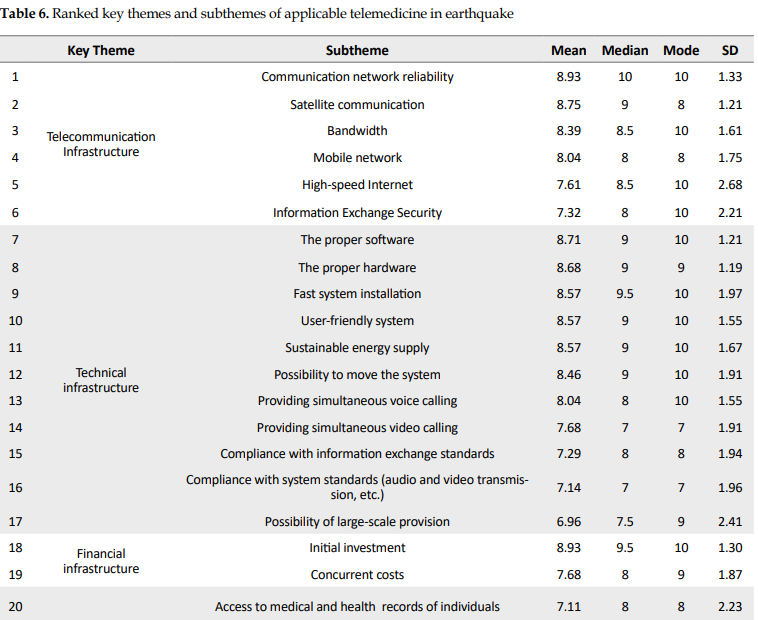
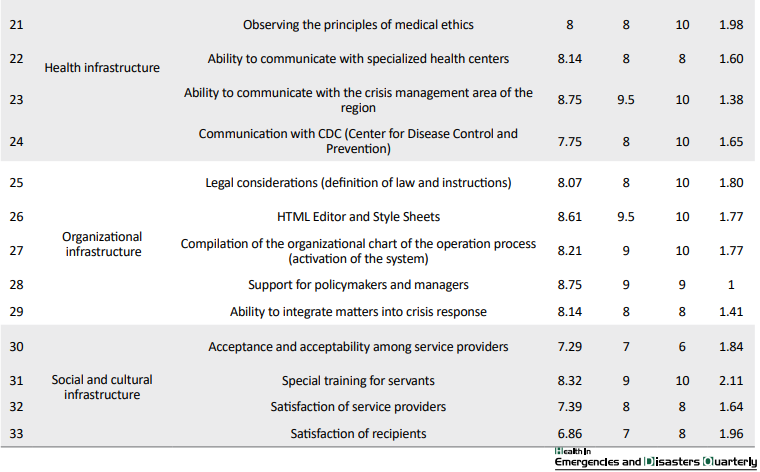
According to the scores of themes and their subthemes, the final model was created with 6 key themes and 35 subthemes (Table 6).
Full-Text: (1254 Views)
1. Introduction
In recent decades, longer life expectancy resulted in an increasing demand for health care. The use of information and communication technology (ICT) is a way to expand health services to these growing needs [1]. ICT has various applications in health services in many fields. The health information network, remote medical networks, and patient’s electronic records are examples of health information technology applications [2].
Telemedicine, as a new technology in the 21st century, is one of the latest ICT technologies that can be used for delivering health services remotely [3] . High-speed telecommunications systems and the invention of devices capable of capturing and transmitting images in digital form had main roles in development [4] . Not only using proper hardware and software is essential, but we also need expert users [5]. There are four factors for prospering telemedicine: therapists’ motivation, proper infrastructure, ongoing investment, and technical support [6].
Providing health services in disasters is one of the essential applications of telemedicine. In the event of disasters, local health facilities can be severely damaged– local hospitals and clinics may be physically damaged or inaccessible. In this situation, various telemedicine services could be applicable. Distance counseling, distance education, remote monitoring, and remote operation, as well as various types of data transmission (text, audio, image, etc.), are among these services [7]. The implementation of the telemedicine system can be effective in solving health problems in affected areas, especially during the early hours of the disaster.
The National Aeronautics and Space Administration (NASA) was the first organization that used telecommunication technology in the Mexico City earthquake in 1985. The disaster managers and rescue and relief personnel communicate with each other by satellite voice communication [8].
So many disasters occurred in Iran previously and placed it among the top 10 countries with disaster occurrence in the world. Seismic activity is the most frequent hazard in Iran, and several major faults cross most area of the country [9].
Iran has special environmental and geographical conditions as well. There are many mountainous and desert areas in Iran [10]. In these conditions, we need new technologies to meet the health requirements of the disaster-affected population. Given the special circumstances of Iran, telemedicine can be considered as one of the ways to provide health services in disasters. The present study was designed to provide a practical model for telemedicine implementation in disasters in Iran, especially in earthquakes.
2. Materials and methods:
According to the research objectives, the present study was carried out using a mixed-methods research in three phases: a review of articles, qualitative study (modeling), and Delphi method (validation of model).
In the first phase, available articles were reviewed to determine the factors affecting the successful deployment of telemedicine in disaster. All databases such as Google Scholar, Web of Science, Scopus were searched from 1990 to the end of 2017 with the keywords of “telemedicine” And “disaster” Or “emergency” And “earthquake”. The inclusion criteria were articles in English or Farsi published up to 2019, about telemedicine, disaster, or emergency and earthquake. According to title and abstract, of 3024 articles, all irrelevant documents ruled out. After reading the content of 76 remaining articles, 13 articles with full text remained for further analysis (Table 1).
In recent decades, longer life expectancy resulted in an increasing demand for health care. The use of information and communication technology (ICT) is a way to expand health services to these growing needs [1]. ICT has various applications in health services in many fields. The health information network, remote medical networks, and patient’s electronic records are examples of health information technology applications [2].
Telemedicine, as a new technology in the 21st century, is one of the latest ICT technologies that can be used for delivering health services remotely [3] . High-speed telecommunications systems and the invention of devices capable of capturing and transmitting images in digital form had main roles in development [4] . Not only using proper hardware and software is essential, but we also need expert users [5]. There are four factors for prospering telemedicine: therapists’ motivation, proper infrastructure, ongoing investment, and technical support [6].
Providing health services in disasters is one of the essential applications of telemedicine. In the event of disasters, local health facilities can be severely damaged– local hospitals and clinics may be physically damaged or inaccessible. In this situation, various telemedicine services could be applicable. Distance counseling, distance education, remote monitoring, and remote operation, as well as various types of data transmission (text, audio, image, etc.), are among these services [7]. The implementation of the telemedicine system can be effective in solving health problems in affected areas, especially during the early hours of the disaster.
The National Aeronautics and Space Administration (NASA) was the first organization that used telecommunication technology in the Mexico City earthquake in 1985. The disaster managers and rescue and relief personnel communicate with each other by satellite voice communication [8].
So many disasters occurred in Iran previously and placed it among the top 10 countries with disaster occurrence in the world. Seismic activity is the most frequent hazard in Iran, and several major faults cross most area of the country [9].
Iran has special environmental and geographical conditions as well. There are many mountainous and desert areas in Iran [10]. In these conditions, we need new technologies to meet the health requirements of the disaster-affected population. Given the special circumstances of Iran, telemedicine can be considered as one of the ways to provide health services in disasters. The present study was designed to provide a practical model for telemedicine implementation in disasters in Iran, especially in earthquakes.
2. Materials and methods:
According to the research objectives, the present study was carried out using a mixed-methods research in three phases: a review of articles, qualitative study (modeling), and Delphi method (validation of model).
In the first phase, available articles were reviewed to determine the factors affecting the successful deployment of telemedicine in disaster. All databases such as Google Scholar, Web of Science, Scopus were searched from 1990 to the end of 2017 with the keywords of “telemedicine” And “disaster” Or “emergency” And “earthquake”. The inclusion criteria were articles in English or Farsi published up to 2019, about telemedicine, disaster, or emergency and earthquake. According to title and abstract, of 3024 articles, all irrelevant documents ruled out. After reading the content of 76 remaining articles, 13 articles with full text remained for further analysis (Table 1).
All key themes of telemedicine in the disaster were extracted from articles. With the discussion in the expert panel of 10 selected professionals, all elements were categorized as 6 key themes with 38 subthemes. The participants gave a score to all items from 1 to 5. Mean, median, mode, and standard deviation values of each item were calculated. Finally, themes and subthemes were ranked by mean scores.
In the second phase, a group of 35 selected volunteer experts (Table 2) enrolled in Delphi to finalize the initial framework. A researcher-made questionnaire was used for data collection, which was validated by face validity, and its reliability was positively evaluated by the Cochran’s formula with the Cronbach alpha coefficient of 0.911. The participants scored each item from 1 to 10 for the final scoring and ranking. At the end of this phase, the applicable model of telemedicine in the disaster was determined.
Subsequently, in the third phase, the second round of Delphi with 29 remaining experts performed to finalize modeling of telemedicine in disasters with the focus on the earthquake. SPSS V. 18 was used for doing statistical analyses and preparing descriptive results.
3. Results
According to the first phase of the study, 6 key themes with 38 subthemes of applicable telemedicine for implementing in the disaster were obtained. Technical infrastructure with 11 subthemes and financial infrastructure with 4 subthemes had maximum and minimum subthemes, respectively (Table 3).
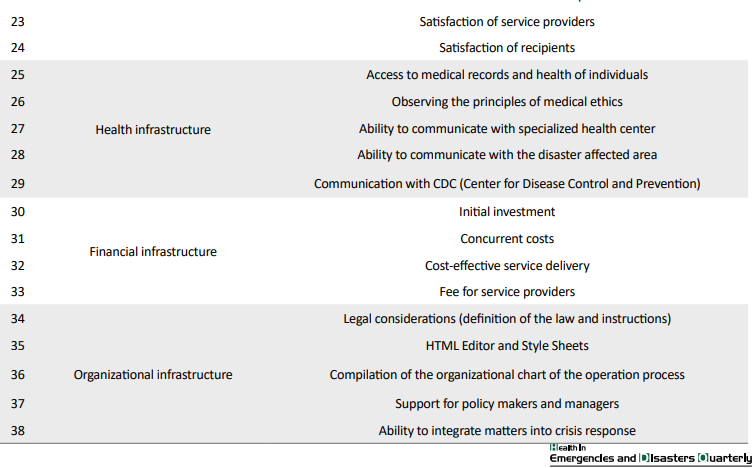
In the second phase, all key themes and subthemes are scored by the participants individually. In this phase, social and cultural infrastructure themes obtained the minimum mean±SD score of mean±SD=7.29±2.07 and telecommunication infrastructure the maximum mean±SD score of mean±SD=8.93±1.68 (Table 4).
In this phase, 5 subthemes were removed from the criteria because they obtained scores less than expectation. The “cable network” subtheme from telecommunication infrastructure theme, “acceptance in society” (the general public) and “public education for service recipients” subthemes from social and cultural infrastructure theme, the “cost-effective service delivery” and “fee for service providers” subthemes from financial infrastructure theme were removed from the criteria.
In the third phase, validation of the model was performed after rearranging subthemes. In this phase, the remaining 28 participated experts scored key themes and subthemes. Then, the highest priority went to telecommunication infrastructure with a maximum score of 9.24 and least priority to social and cultural infrastructure theme with a minimum score of 7.53 (Table 5).
According to the scores of themes and their subthemes, the final model was created with 6 key themes and 35 subthemes (Table 6).
In the final model, 2 subthemes obtained maximum scores, i.e. the communication network reliability of the telecommunication infrastructure theme and the initial investment of the financial infrastructure theme. The satisfaction of recipients’ subtheme of the social and cultural infrastructure theme with the least score of 6.86 was placed in the bottom.
4. Discussion
In this study, we tried to create an applicable model of telemedicine in disasters for Iran, with the focus on earthquake. Given that earthquake is one of the most important natural disasters in our country, and about 93% of Iran are at risk of the earthquake [11], we need new technologies such as telemedicine to provide health services in the affected areas. Because of the rapid development of telecommunication industry in Iran with the improvement of communication all over the country, there is a good chance for using telemedicine [12].
There are many successful implementations of remote health services in the world from the beginning of their usage since the mid-1980s. Past experiences allow scientists to extrapolate how telemedicine will evolve to meet future needs in disasters [8]. From the first usage of telecommunication technology in Mexico City earthquake in 1985 to remote surgery in recent years, telemedicine has developed unbelievably. In recent years with the development of cellular phones, counseling and medical diagnostic interventions are available. Surgeons can do complicated operations with the help of reliable communication technology, such as long-term evolution [13].
In our study, the experts categorized key elements of a telemedicine application in 6 themes. Our study results indicated that having the appropriate telecommunication tools along with financing for the proper maintenance of the equipment is very important. The importance of these cases in other studies shows clearly the telemedicine conceptual framework. Innovation in Information and Communication Technology (ICT) with considerable investments in the field of healthcare informatics, resulted in improving and extending medical services in remote, unprivileged areas with important social and economic benefits [14].
To implement telemedicine in Iran, it is first necessary to identify the principle and partner organizations with a clear task description. Then the essential infrastructure should be developed according to specific goals. The most important infrastructures are the technical and telecommunication infrastructure (including telemedicine equipment, strong and efficient communications and the development of platforms, increased bandwidth and access to intranets and the Internet), social and cultural infrastructure (public education, special education for users, specialist physicians, medical and paramedical students and emergency aid staff), security infrastructure (coordination with network police, security information centers and electronic signatures), legal considerations (legal guidelines, rules and regulations related to health) and standardization infrastructure (information exchange standards, vocabulary, security, and system architecture).
Other studies also emphasized these obstacles in the implementation of telemedicine due to specific environments. In one study in India declared the role of ICT and the context of Indian society for implementing telemedicine. They noted the importance of telecommunication infrastructure along with economic and sociocultural infrastructure [15].
The vulnerability assessment of the equipment and facilities of the telemedicine infrastructure is very important. Reliable and persistent communication along with well-established devices in both side of telemedicine technology is mandatory. There are many automated solutions to help us control our telemedicine environment better [16].
5. Conclusion
In this research, due to the nature of the future and the novelty of the subject, the Delphi method was used to identify the key themes and subthemes of telemedicine implementation in Iran during an earthquake disaster. We believe that our model of telemedicine implementation is an appropriate model for Iran. We suggest that the results of this study be implemented as a theoretical model, or in the pilot study, in a region of the country. Then, the outcomes are investigated regarding the amount of mortality reduction. We also recommend that a comparative study is done for using telemedicine in other types of disasters.
Ethical Considerations
Compliance with ethical guidelines
There was no ethical considerations to be considered in this research.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. Farhad Fatehi received financial support from the Queensland Government through an Advance Queensland Research Fellowship.
Authors' contributions
All authors contributed in preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The present paper has been extracted from a part of Master’s dissertation of the first author at Faculty of Medical Engineering, Amirkabir University of Technology.
References
4. Discussion
In this study, we tried to create an applicable model of telemedicine in disasters for Iran, with the focus on earthquake. Given that earthquake is one of the most important natural disasters in our country, and about 93% of Iran are at risk of the earthquake [11], we need new technologies such as telemedicine to provide health services in the affected areas. Because of the rapid development of telecommunication industry in Iran with the improvement of communication all over the country, there is a good chance for using telemedicine [12].
There are many successful implementations of remote health services in the world from the beginning of their usage since the mid-1980s. Past experiences allow scientists to extrapolate how telemedicine will evolve to meet future needs in disasters [8]. From the first usage of telecommunication technology in Mexico City earthquake in 1985 to remote surgery in recent years, telemedicine has developed unbelievably. In recent years with the development of cellular phones, counseling and medical diagnostic interventions are available. Surgeons can do complicated operations with the help of reliable communication technology, such as long-term evolution [13].
In our study, the experts categorized key elements of a telemedicine application in 6 themes. Our study results indicated that having the appropriate telecommunication tools along with financing for the proper maintenance of the equipment is very important. The importance of these cases in other studies shows clearly the telemedicine conceptual framework. Innovation in Information and Communication Technology (ICT) with considerable investments in the field of healthcare informatics, resulted in improving and extending medical services in remote, unprivileged areas with important social and economic benefits [14].
To implement telemedicine in Iran, it is first necessary to identify the principle and partner organizations with a clear task description. Then the essential infrastructure should be developed according to specific goals. The most important infrastructures are the technical and telecommunication infrastructure (including telemedicine equipment, strong and efficient communications and the development of platforms, increased bandwidth and access to intranets and the Internet), social and cultural infrastructure (public education, special education for users, specialist physicians, medical and paramedical students and emergency aid staff), security infrastructure (coordination with network police, security information centers and electronic signatures), legal considerations (legal guidelines, rules and regulations related to health) and standardization infrastructure (information exchange standards, vocabulary, security, and system architecture).
Other studies also emphasized these obstacles in the implementation of telemedicine due to specific environments. In one study in India declared the role of ICT and the context of Indian society for implementing telemedicine. They noted the importance of telecommunication infrastructure along with economic and sociocultural infrastructure [15].
The vulnerability assessment of the equipment and facilities of the telemedicine infrastructure is very important. Reliable and persistent communication along with well-established devices in both side of telemedicine technology is mandatory. There are many automated solutions to help us control our telemedicine environment better [16].
5. Conclusion
In this research, due to the nature of the future and the novelty of the subject, the Delphi method was used to identify the key themes and subthemes of telemedicine implementation in Iran during an earthquake disaster. We believe that our model of telemedicine implementation is an appropriate model for Iran. We suggest that the results of this study be implemented as a theoretical model, or in the pilot study, in a region of the country. Then, the outcomes are investigated regarding the amount of mortality reduction. We also recommend that a comparative study is done for using telemedicine in other types of disasters.
Ethical Considerations
Compliance with ethical guidelines
There was no ethical considerations to be considered in this research.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. Farhad Fatehi received financial support from the Queensland Government through an Advance Queensland Research Fellowship.
Authors' contributions
All authors contributed in preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The present paper has been extracted from a part of Master’s dissertation of the first author at Faculty of Medical Engineering, Amirkabir University of Technology.
References
- Bashshur RL, Shannon GW, Sanders JH. Telemedicine: Theory and practice. Springfield: Charles C. Thomas; 1997.
- Crane PW, Wiegand TJ, Kamali M, Reif M, Wratni R, Montante R, et al. Telemedicine Delivery and Successful Reimbursement in Toxicology. Journal of Medical Toxicology. 2018; 14(3):242-7. [DOI:10.1007/s13181-018-0665-5] [PMID][PMCID]
- Nicogossian AE, Doarn CR. Armenia 1988 earthquake and telemedicine: lessons learned and forgotten. Telemedicine and e-Health. 2011; 17(9):741-5. [DOI:10.1089/tmj.2011.0118][PMID]
- Dullet NW, Geraghty EM, Kaufman T, Kissee JL, King J, Dharmar M, et al. Impact of a university-based outpatient telemedicine program on time savings, travel costs, and environmental pollutants. Value in Health. 2017; 20(4):542-6. [DOI:10.1016/j.jval.2017.01.014] [PMID]
- Helsel BC, Williams JE, Lawson K, Liang J, Markowitz J. Telemedicine and mobile health technology are effective in the management of digestive diseases: A systematic review. Digestive Diseases and Sciences. 2018; 63(6):1392-408. [DOI:10.1007/s10620-018-5054-z] [PMID]
- Strode SW, Gustke S, Allen A. Technical and clinical progress in telemedicine. Jama. 1999; 281(12):1066-8. [DOI:10.1001/jama.281.12.1066] [PMID]
- Østbye T, Hurlen P. The electronic house call: consequences of telemedicine consultations for physicians, patients, and society. Archives of Family Medicine. 1997; 6(3):266-77. [DOI:10.1001/archfami.6.3.266] [PMID]
- Garshnek V, Burkle FM. Applications of telemedicine and telecommunications to disaster medicine: Historical and future perspectives. Journal of the American Medical Informatics Association. 1999; 6(1):26-37. [DOI:10.1136/jamia.1999.0060026] [PMID] [PMCID]
- International Institute of Earthquake Engineering and Seismology. Preliminary Earthquake Reconnaissance Report on the June 22, 2002 Changureh (Avaj), Iran Earthquake. [Internet]. 2002 [Updated 2010 March 25] Availabe from: http://www.iiees.ac.ir/en/preliminary-report-of-iiees-reconnaissance-team-the-changureh-avaj-earthquake-of-june-22-2002-mw64/
- Ghomian Z, Yousefian S. Natural Disasters in the Middle-East and North Africa With a Focus on Iran: 1900 to 2015. HDQ. 2017; 2(2):53-62. [DOI:10.18869/nrip.hdq.2.2.53]
- Latifi R, Tilley EH. Telemedicine for disaster management: can it transform chaos into an organized, structured care from the distance. American Journal of Disaster Medicine. 2014; 9(1):25-37. [DOI:10.5055/ajdm.2014.0139] [PMID]
- Nekoueizadeh S, Esmaeili S. A study of the impact of TQM on organizational performance of the telecommunication Industry in Iran. European Online Journal of Natural and Social Sciences. 2013; 2(3):968-78.
- Lynn M. Telemedicine to manage sudden Mass casualty incidents remotely. In: Lynn M, Lieberman H, Lynn L, Pust GD, Stahl K, Yeh DD, et al. editors. Disasters and Mass Casualty Incidents. Cham: Springer; 2019. [DOI:10.1007/978-3-319-97361-6_17]
- Vizitiu C. TeleMedicine-theoretical framework. In: Vizitiu C, editor. Systems Engineering and Organizational Assessment Solutions Ensuring Sustainability within Telemedicine Context. Wiesbaden: Springer Gabler; 2019. [DOI:10.1007/978-3-658-23538-3_4]
- Ahmed SS, Sandhya M, Shankar S. ICT’s role in building and understanding indian telemedicine environment: A study. In: Fong S, Akashe S, Mahalle P, editors. Information and Communication Technology for Competitive Strategies. Downtown Core: Springer; 2019. [DOI:10.1007/978-981-13-0586-3_39]
- Nikoloudakis Y, Pallis E, Mastorakis G, Mavromoustakis CX, Skianis C, Markakis EK. Vulnerability assessment as a service for fog-centric ICT ecosystems: A healthcare use case. Peer-to-Peer Networking and Applications. 2019; 2019:1-9. [DOI:10.1007/s12083-019-0716-y]
- Handschu R, Littmann R, Reulbach U, Gaul C, Heckmann JG, Neundörfer B, et al. Telemedicine in emergency evaluation of acute stroke: Interrater agreement in remote video examination with a novel multimedia system. Stroke. 2004; 34(12):2842-6. [DOI:10.1161/01.STR.0000102043.70312.E9] [PMID]
- Lambrecht CJ. Emergency physicians’ roles in a clinical telemedicine network. Annals of emergency medicine. 1997; 30(5):670-4. [DOI:10.1016/S0196-0644(97)70087-8]
- Czaplik M, Bergrath S, Rossaint R, Thelen S, Brodziak T, Valentin B, et al. Employment of telemedicine in emergency medicine. clinical requirement analysis, system development and first-test results. Methods of Information in Medicine. 2014; 53(2):99-107. [DOI:10.3414/ME13-01-0022] [PMID]
Type of Study: Research |
Subject:
Special
Received: 2019/05/11 | Accepted: 2019/06/12 | Published: 2019/07/23
Received: 2019/05/11 | Accepted: 2019/06/12 | Published: 2019/07/23
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Health in Emergencies and Disasters Quarterly
Health in Emergencies & Disasters Research Center, University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave, Tehran, Iran.
Journal Tel: +9821 71732816 (2816)
Publisher Tel: +9821 4535 5555 - 4535 5000
