

Volume 3, Issue 4 (Summer 2018 -- 2018)
Health in Emergencies and Disasters Quarterly 2018, 3(4): 221-233 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Khankeh H, Kolivand P H, Beyrami Jam M, Rajabi E. Kermanshah Health Care Services: A Lesson Learned From Iran’s Recent Earthquake. Health in Emergencies and Disasters Quarterly 2018; 3 (4) :221-233
URL: http://hdq.uswr.ac.ir/article-1-202-en.html
URL: http://hdq.uswr.ac.ir/article-1-202-en.html



1- Department of Clinical Science and Education, Karolinska Institute, Stockholm, Sweden.
2- Emergency Medical Services, Iran Ministry of Health and Medical Education, Tehran, Iran.
3- Health in Emergency and Disaster Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
4- Health in Emergency and Disaster Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. , rajabimw@gmail.com
2- Emergency Medical Services, Iran Ministry of Health and Medical Education, Tehran, Iran.
3- Health in Emergency and Disaster Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
4- Health in Emergency and Disaster Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. , rajabimw@gmail.com
Full-Text [PDF 746 kb]
(2119 Downloads)
| Abstract (HTML) (6928 Views)


Full-Text: (1777 Views)
1. Introduction
Health and treatment services have always been considered as the most important demands of the people in the event of incidents and disasters, because among their numerous consequences, the most important concern is injuries inflicted on people’s health and life [1]. Today, the incidence of disasters in large scale has led to injury and harm inflicted upon a great number of people and makes it imperative to use considerable amount of emergency health services [2]. Especially in an earthquake that is one of the most destructive natural disasters, a significant number of affected people may need health services. Furthermore, after the earthquake, health requirements should necessarily be provided within a limited time period [1].
Earthquakes have always been a serious threat to the health and properties of human beings and on average each year 16 earthquakes occur throughout the world that inflict many damages, especially economically and many injuries on human society [3]. Based on report by the World Health Organization, 564.4 million people were affected by natural disasters in 2016, of which two millions were affected by the earthquake and approximately 70000 persons lost their lives. One of the regions that report the highest number of earthquake fatalities is East Asia [4]. Iran because of its geographical position along the Alpine-Himalayan belt is also considered one of the earthquake prone areas of the world.
The seismicity of most regions of Iran has made it likely that disasters of this kind would occur and earthquake has always been one of the historical concerns of the people of Iran. According to official reports, each year on average one earthquake with magnitude of 6 on the Richter scale occurs in Iran and every ten years one earthquake occurs with magnitude of 7 on the Richter scale [5]. The 7.4 Richter scale magnitude earthquake in Rudbar and Manjil on June 21, 1990 and 6.6 magnitude earthquake on the Richter scale on December 26, 2003 in the city of Bam, that left 40000 and 30000 fatalities, respectively are considered two instances of the greatest earthquakes that took place in Iran in the past 30 years [6]. Recently, the earthquake in the province of Kermanshah on November 12, 2017 with magnitude of 7.3 Richter was another experience of this peril.
In particular in earthquakes, not only trauma and injury can put the survival of individuals at serious risk [1], damages incurred upon the health-treatment system and increase in demand, can also limit or make difficult access to emergency health services [7]. In other words, such peril can directly influence the affected population, and indirectly with disruption in supply of health services, lead to lack of access of large section of the population to emergency health services in the short period after the occurrence of earthquake and subsequently increase the magnitude of health injuries [8]. On the other hand, delivering health and treatment services in earthquake has significant differences with other situations [1]. This issue is very important that disruption in providing health services in an earthquake will lead to a great challenge in the life of vulnerable people, therefore, its occurrence in the current extensive scale requires earnest presence of health and treatment services on the scene of such events [2].
As such it is necessary that responsible organizations allocate their resources and time toward survival of individuals after such disasters, and in particular focus on supplying emergency health services and rescuing people from the disaster’s consequences. Without such valuable investment, the opportunity to learn lessons from experience for future events may be lost [9]. Apart from the fact that disasters could be natural or man-made, it is evident that for developing a plan for comprehensive disaster risk management approved by all international agreements from Yokohama to Sendai, it is necessary that services provided in all incidents should be examined carefully in the form of lessons learned and applied for developing risk management plans [10].
Provision of effective health services in disasters requires a vast and clear vision from different angles; because factors influencing the success of health care and services in disasters are not limited to the area of health, but interaction and close communication between different sections in disaster management should be established [1]. For example in Iran, 14 workgroups interact and cooperate with each other. In this regard, the workgroup of Ministry of Health with 9 committees under administration of the Minister of Health as the director and supervision of the director of Emergency Organization as the secretary embark on policymaking, planning and coordination between other crisis management workgroups in the country. In this way, they can act in the best manner and in the shortest time possible to respond to incidents and disasters.
It is important to understand that earthquake will happen again and the lessons learned from previous events can save the lives of many people in future incidents [9]. In order to develop health and treatment services and provide suitable response in disasters, it is necessary to have sufficient information from previous experiences. In other words, learning from previous information and experiences can be the basis for comprehensive planning of the risk management and rendering health and treatment services for later incidents [1].
Considering the role and importance of providing information and assessment of the activities (to identify the strong and weak points), the present study was conducted to investigate the performance of Health and Treatment workgroup in response to the 7.3 Richter earthquake in the province of Kermanshah so that grounds can be provided to benefit from the lessons learned and experiences acquired in order for advancement, preparation, and improvement in response and better decision making in the likely instances in future.
2. Materials and Methods
For conducting this case study, the triangulation method was used including interview, participatory observation, and expert panel in 3 emergency departments (State Emergency Organization), treatment centers (treatment deputy) and health centers (health deputy) to assess the performance of health and treatment workgroup during and after delivering the health services.
For this purpose, one of the researchers as an expert on rapid assessment of the incident went to the scene for 4 days and in addition to recording the information obtained from observation, reports related to the Emergency Operation Center and reports related to other rapid assessment experts (4 PhD candidate students in Health in Emergency and Disaster who were dispatched as representative of the Emergency Organization to the damaged areas) with regard to instances such as command and coordination, activation, EOC activation, dispatch of rapid assessment team, steps that have been taken by prehospital emergency, hospital and health and so on as well as the problems, weak and strong points in providing health services and incident management, were collected and assessed.
Health and treatment services have always been considered as the most important demands of the people in the event of incidents and disasters, because among their numerous consequences, the most important concern is injuries inflicted on people’s health and life [1]. Today, the incidence of disasters in large scale has led to injury and harm inflicted upon a great number of people and makes it imperative to use considerable amount of emergency health services [2]. Especially in an earthquake that is one of the most destructive natural disasters, a significant number of affected people may need health services. Furthermore, after the earthquake, health requirements should necessarily be provided within a limited time period [1].
Earthquakes have always been a serious threat to the health and properties of human beings and on average each year 16 earthquakes occur throughout the world that inflict many damages, especially economically and many injuries on human society [3]. Based on report by the World Health Organization, 564.4 million people were affected by natural disasters in 2016, of which two millions were affected by the earthquake and approximately 70000 persons lost their lives. One of the regions that report the highest number of earthquake fatalities is East Asia [4]. Iran because of its geographical position along the Alpine-Himalayan belt is also considered one of the earthquake prone areas of the world.
The seismicity of most regions of Iran has made it likely that disasters of this kind would occur and earthquake has always been one of the historical concerns of the people of Iran. According to official reports, each year on average one earthquake with magnitude of 6 on the Richter scale occurs in Iran and every ten years one earthquake occurs with magnitude of 7 on the Richter scale [5]. The 7.4 Richter scale magnitude earthquake in Rudbar and Manjil on June 21, 1990 and 6.6 magnitude earthquake on the Richter scale on December 26, 2003 in the city of Bam, that left 40000 and 30000 fatalities, respectively are considered two instances of the greatest earthquakes that took place in Iran in the past 30 years [6]. Recently, the earthquake in the province of Kermanshah on November 12, 2017 with magnitude of 7.3 Richter was another experience of this peril.
In particular in earthquakes, not only trauma and injury can put the survival of individuals at serious risk [1], damages incurred upon the health-treatment system and increase in demand, can also limit or make difficult access to emergency health services [7]. In other words, such peril can directly influence the affected population, and indirectly with disruption in supply of health services, lead to lack of access of large section of the population to emergency health services in the short period after the occurrence of earthquake and subsequently increase the magnitude of health injuries [8]. On the other hand, delivering health and treatment services in earthquake has significant differences with other situations [1]. This issue is very important that disruption in providing health services in an earthquake will lead to a great challenge in the life of vulnerable people, therefore, its occurrence in the current extensive scale requires earnest presence of health and treatment services on the scene of such events [2].
As such it is necessary that responsible organizations allocate their resources and time toward survival of individuals after such disasters, and in particular focus on supplying emergency health services and rescuing people from the disaster’s consequences. Without such valuable investment, the opportunity to learn lessons from experience for future events may be lost [9]. Apart from the fact that disasters could be natural or man-made, it is evident that for developing a plan for comprehensive disaster risk management approved by all international agreements from Yokohama to Sendai, it is necessary that services provided in all incidents should be examined carefully in the form of lessons learned and applied for developing risk management plans [10].
Provision of effective health services in disasters requires a vast and clear vision from different angles; because factors influencing the success of health care and services in disasters are not limited to the area of health, but interaction and close communication between different sections in disaster management should be established [1]. For example in Iran, 14 workgroups interact and cooperate with each other. In this regard, the workgroup of Ministry of Health with 9 committees under administration of the Minister of Health as the director and supervision of the director of Emergency Organization as the secretary embark on policymaking, planning and coordination between other crisis management workgroups in the country. In this way, they can act in the best manner and in the shortest time possible to respond to incidents and disasters.
It is important to understand that earthquake will happen again and the lessons learned from previous events can save the lives of many people in future incidents [9]. In order to develop health and treatment services and provide suitable response in disasters, it is necessary to have sufficient information from previous experiences. In other words, learning from previous information and experiences can be the basis for comprehensive planning of the risk management and rendering health and treatment services for later incidents [1].
Considering the role and importance of providing information and assessment of the activities (to identify the strong and weak points), the present study was conducted to investigate the performance of Health and Treatment workgroup in response to the 7.3 Richter earthquake in the province of Kermanshah so that grounds can be provided to benefit from the lessons learned and experiences acquired in order for advancement, preparation, and improvement in response and better decision making in the likely instances in future.
2. Materials and Methods
For conducting this case study, the triangulation method was used including interview, participatory observation, and expert panel in 3 emergency departments (State Emergency Organization), treatment centers (treatment deputy) and health centers (health deputy) to assess the performance of health and treatment workgroup during and after delivering the health services.
For this purpose, one of the researchers as an expert on rapid assessment of the incident went to the scene for 4 days and in addition to recording the information obtained from observation, reports related to the Emergency Operation Center and reports related to other rapid assessment experts (4 PhD candidate students in Health in Emergency and Disaster who were dispatched as representative of the Emergency Organization to the damaged areas) with regard to instances such as command and coordination, activation, EOC activation, dispatch of rapid assessment team, steps that have been taken by prehospital emergency, hospital and health and so on as well as the problems, weak and strong points in providing health services and incident management, were collected and assessed.
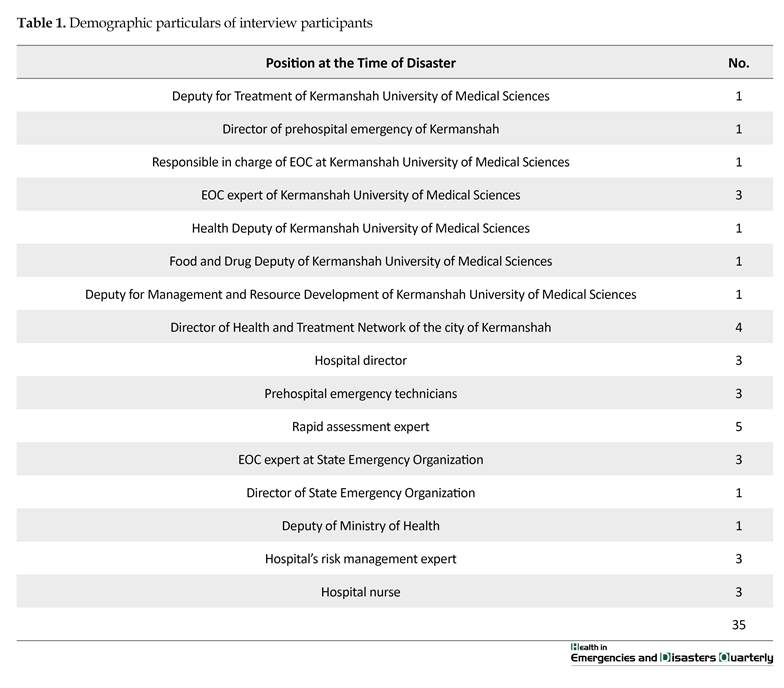
Also, interviews were conducted with responsible managers, commanders and experts at the field of incident including employees of EOC of Kermanshah University of Medical Sciences, a well as employees, field managers, commanders, and experts of incident management in different incident-stricken cities of the affected province (Kermanshah) and finally the experts and EOC specialists of the Ministry of Health in connection with the above mentioned circumstances (particulars and number of participants in the interview are mentioned in Table 1). Then, by organizing a panel of experts in incident management, supplementary information were collected and analyzed.
Study case: Kermanshah earthquake
This earthquake hit the Province of Kermanshah, with the magnitude of 7.3 on the Richter scale and lasted 30 seconds and at the depth of 11 km beneath the Earth’s surface, 5 km from the town of Ezgeleh in Kermanshah Province at 21:48 local time on November 12, 2017. Based on information derived from the Geophysics Institute and the National Seismological Center, this earthquake had 3 foreshocks the largest of which at 4.5 Richter magnitude was reported at 21:05 local time. Besides the western, northern and southwestern, central and northern regions of Iran, particularly Kermanshah, Ilam, Kurdistan, Western Azerbaijan and Khuzestan, this earthquake was also felt in the neighboring countries such as Iraq, Kuwait, and Bahrain.
During the days after the earthquake, more than 1000 aftershocks were recorded, the largest of which was an aftershock with a magnitude of 4.7 on the Richter scale that occurred at 7:57 local time and also at 16:46 local time on November 13. Number of fatalities in this earthquake was 625 persons and the number of injured was more than 15000. Regions affected by the earthquake encompassed a vast area in the west of the country including the cities of Dalahu, Javanrood, Gilan-e Gharb, Ghasreshirin, Eslam Abad-e Gharb, Sar-e pol-e Zahab, Salas-e Babajani, and parts of the city of Kermanshah with a population of 427000 people. Also 85 rural residential areas in the distance of 5 to 15 km from the epicenter sustained 80% destruction.
Study area
Area of health management in emergency and disaster, of the western side of the country that are responsible for health management in incidents and disasters in western provinces including Kermanshah (center), Kurdistan, Hamadan and Ilam were selected as field of the study because the recent earthquake occurred in this area.
3. Results
Activation of the Emergency Operation Center
After the 7.3 Richter earthquake hit the above mentioned areas at 21:48 local time, Emergency Operation Center (EOC) of the Ministry of Health, Treatment and Medical Education and the Incident Command System of that center immediately were activated and alert order was sent to all health-treatment centers and emergency bases in university centers in the west, southwest and northwest of the country as well as border headquarters in Mehran, Shalamcheh, and Chazabeh. The EOC in medical sciences universities of Kermanshah, Hamadan, Kurdistan, Urmia and Tabriz and also in Tehran were all placed on red alert for receiving the possible injured victims.
Medical sciences universities of support provinces such as Qum, Qazvin, Isfahan, Semnan, Mazandaran, Alborz, Zanjan, Khurramabad, and Arak were also placed at the orange alert (advisory) status in case their assistance may be needed. Also, considering the likelihood of national crisis, necessary coordination was made with relevant organizations such as workplace health center, center for disease control and prevention, the Red Crescent Society, the army, the guards’ corps, and the crisis management liaison. Communication was maintained at all times with the EOC on the scene of the incident and national EOC at the Ministry of the Interior.
Dispatch of Emergency Medical Technician teams
Immediately after the earthquake, 100 emergency medical technician teams were dispatched to the area. In the next stage, along with coordination with Kermanshah EOC, contact was made to bases at the scene of the incident through the cell phone number mentioned in the Integrated System of Iran’s Health Statistics and Information System, and considering the opinion announced by the shift personnel at bases of Emergency 115 in the affected areas, the initial map of the incident scene was obtained.
Then, by using the map of Kermanshah Province, the cities that were affected by the earthquake were investigated and the damaged areas were highlighted with white and red points. Based on information obtained by phone contacts with the area’s treatment centers and based on early data, the regions most affected, i.e. Dalahu, Javanrood, Gilan-e Gharb, Ghasreshirin, Salas-e Babajani, and Sar-e pol-e Zahab were identified and according to the information obtained at 1:00 AM, names of more than 97 deaths and 1200 injured were confirmed which showed the severity of the incident.
The supplementary information received by constant communication with emergency bases and treatment centers, indicated the serious increase in casualties and the injured. As such the level of the incident was determined as E3.
Employing military forces and other support organizations
Immediately after the earthquake, the highest official at the State Emergency Organization went to the scene and contacted the authorities in order to receive support and logistical services from colleague and support organizations. Consultations were made with commander of the ground forces of the army in order to transfer the injured by land or air transport and to use helicopters for covering medical emergency operations.
Consultations with Guard Corps commanders were also made to coordinate setting up field hospital, transfer the injured, and provide medical emergency services. Also by coordination with the director of civil defense organization, 2 air ambulances, 1 ambulance bus and 20 helicopters were dispatched for transport of large numbers of the injured. By coordination with the Red Crescent Society for the use of air emergency services, coordination was made with the food and drug administration to dispatch medicines and equipment; also coordination was made with blood transfusion organization for depot and sending blood and blood products. All these activities were carried out in the shortest time possible after the earthquake.
Establishing field hospital
The landing pad for the helicopter from Shohada Hospital was selected as the location for setting up field hospital and in the first hour after the earthquake, the first field hospital was established at that location. During the following days, provisions were made to use 6 field hospitals stationed in that region.
Dispatch of logistics and manpower to the region affected by the earthquake
Immediately after the earthquake, all facilities stationed at the border cities of Mehran, Shalamcheh and Chazabeh including 42 ambulances and 6 ambulance buses were sent to the scene of incident, and these measures continued by sending 48 ambulances, 13 ambulance buses and 2 mobile communications automobiles vehicles from other regions. In total, during the 17 days since the time the earthquake occurred until November 28, 2017, by taking into account the ambulances available in the city of Kermanshah, 120 ambulances, 20 ambulance buses and 2 operations communications vehicles
Study case: Kermanshah earthquake
This earthquake hit the Province of Kermanshah, with the magnitude of 7.3 on the Richter scale and lasted 30 seconds and at the depth of 11 km beneath the Earth’s surface, 5 km from the town of Ezgeleh in Kermanshah Province at 21:48 local time on November 12, 2017. Based on information derived from the Geophysics Institute and the National Seismological Center, this earthquake had 3 foreshocks the largest of which at 4.5 Richter magnitude was reported at 21:05 local time. Besides the western, northern and southwestern, central and northern regions of Iran, particularly Kermanshah, Ilam, Kurdistan, Western Azerbaijan and Khuzestan, this earthquake was also felt in the neighboring countries such as Iraq, Kuwait, and Bahrain.
During the days after the earthquake, more than 1000 aftershocks were recorded, the largest of which was an aftershock with a magnitude of 4.7 on the Richter scale that occurred at 7:57 local time and also at 16:46 local time on November 13. Number of fatalities in this earthquake was 625 persons and the number of injured was more than 15000. Regions affected by the earthquake encompassed a vast area in the west of the country including the cities of Dalahu, Javanrood, Gilan-e Gharb, Ghasreshirin, Eslam Abad-e Gharb, Sar-e pol-e Zahab, Salas-e Babajani, and parts of the city of Kermanshah with a population of 427000 people. Also 85 rural residential areas in the distance of 5 to 15 km from the epicenter sustained 80% destruction.
Study area
Area of health management in emergency and disaster, of the western side of the country that are responsible for health management in incidents and disasters in western provinces including Kermanshah (center), Kurdistan, Hamadan and Ilam were selected as field of the study because the recent earthquake occurred in this area.
3. Results
Activation of the Emergency Operation Center
After the 7.3 Richter earthquake hit the above mentioned areas at 21:48 local time, Emergency Operation Center (EOC) of the Ministry of Health, Treatment and Medical Education and the Incident Command System of that center immediately were activated and alert order was sent to all health-treatment centers and emergency bases in university centers in the west, southwest and northwest of the country as well as border headquarters in Mehran, Shalamcheh, and Chazabeh. The EOC in medical sciences universities of Kermanshah, Hamadan, Kurdistan, Urmia and Tabriz and also in Tehran were all placed on red alert for receiving the possible injured victims.
Medical sciences universities of support provinces such as Qum, Qazvin, Isfahan, Semnan, Mazandaran, Alborz, Zanjan, Khurramabad, and Arak were also placed at the orange alert (advisory) status in case their assistance may be needed. Also, considering the likelihood of national crisis, necessary coordination was made with relevant organizations such as workplace health center, center for disease control and prevention, the Red Crescent Society, the army, the guards’ corps, and the crisis management liaison. Communication was maintained at all times with the EOC on the scene of the incident and national EOC at the Ministry of the Interior.
Dispatch of Emergency Medical Technician teams
Immediately after the earthquake, 100 emergency medical technician teams were dispatched to the area. In the next stage, along with coordination with Kermanshah EOC, contact was made to bases at the scene of the incident through the cell phone number mentioned in the Integrated System of Iran’s Health Statistics and Information System, and considering the opinion announced by the shift personnel at bases of Emergency 115 in the affected areas, the initial map of the incident scene was obtained.
Then, by using the map of Kermanshah Province, the cities that were affected by the earthquake were investigated and the damaged areas were highlighted with white and red points. Based on information obtained by phone contacts with the area’s treatment centers and based on early data, the regions most affected, i.e. Dalahu, Javanrood, Gilan-e Gharb, Ghasreshirin, Salas-e Babajani, and Sar-e pol-e Zahab were identified and according to the information obtained at 1:00 AM, names of more than 97 deaths and 1200 injured were confirmed which showed the severity of the incident.
The supplementary information received by constant communication with emergency bases and treatment centers, indicated the serious increase in casualties and the injured. As such the level of the incident was determined as E3.
Employing military forces and other support organizations
Immediately after the earthquake, the highest official at the State Emergency Organization went to the scene and contacted the authorities in order to receive support and logistical services from colleague and support organizations. Consultations were made with commander of the ground forces of the army in order to transfer the injured by land or air transport and to use helicopters for covering medical emergency operations.
Consultations with Guard Corps commanders were also made to coordinate setting up field hospital, transfer the injured, and provide medical emergency services. Also by coordination with the director of civil defense organization, 2 air ambulances, 1 ambulance bus and 20 helicopters were dispatched for transport of large numbers of the injured. By coordination with the Red Crescent Society for the use of air emergency services, coordination was made with the food and drug administration to dispatch medicines and equipment; also coordination was made with blood transfusion organization for depot and sending blood and blood products. All these activities were carried out in the shortest time possible after the earthquake.
Establishing field hospital
The landing pad for the helicopter from Shohada Hospital was selected as the location for setting up field hospital and in the first hour after the earthquake, the first field hospital was established at that location. During the following days, provisions were made to use 6 field hospitals stationed in that region.
Dispatch of logistics and manpower to the region affected by the earthquake
Immediately after the earthquake, all facilities stationed at the border cities of Mehran, Shalamcheh and Chazabeh including 42 ambulances and 6 ambulance buses were sent to the scene of incident, and these measures continued by sending 48 ambulances, 13 ambulance buses and 2 mobile communications automobiles vehicles from other regions. In total, during the 17 days since the time the earthquake occurred until November 28, 2017, by taking into account the ambulances available in the city of Kermanshah, 120 ambulances, 20 ambulance buses and 2 operations communications vehicles
covered the supply of medical emergency services for the victims of the earthquake.
Based on the information received from the base at Sar-e Pol-e Zahab, a safe location was determined for the landing of helicopters in the football field of Abuzar garrison (Army) in Sar-e Pol-e Zahab, and its geographic specifications were sent to all air emergency bases. Immediately after sunrise, all of the flight crew and medical personnel were summoned and prepared for dispatch to the affected areas. A total of 2 air ambulances and 20 helicopters were sent to the region for air transfer of the large numbers of the injured, and by cooperation of the army, the Guards, and the Red Crescent personnel, 4 airplanes were employed to send manpower and medical equipments to the affected areas and dispatch seriously injured victims from the scene of incident to treatment centers of the city of Kermanshah and other cities of the country.
The number of specialist forces and the amount of health and treatment equipments sent to the earthquake affected areas are presented in Table 2.
Surge capacity in the region and hospitals of other provinces
According to predetermined protocol, prompt action was taken to increase the hospitals capacity in terms of hospital beds. For this purpose, in addition to the transfer of facilities and equipments (which due to mass gathering of Arba`een religious ceremony were stationed at the border cities of Mehran, Chazabeh, and Shalamcheh), in the very early hours after the earthquake, the medical universities of Tehran, Alborz and Hamadan reported the capacity to receive the injured in each of the subsidiary centers and the status of specialist forces prepared for service in the hospitals associated with them.
Also, due to the logistical facilities provided in the region, during the first 20 hours, more than 7350 injured people were transferred to Kermanshah and other provinces using helicopters, airplanes, ambulances and ambulance buses to create more expeditious conditions for their treatment, and the potential to receive and treat other injured victims in Kermanshah hospitals. The status of the injured people referred to the treatment centers stationed in the earthquake- area and in treatment centers stationed in other provinces, as well as the number of hospitalizations and surgical procedures performed in these centers within the first 17 days after the earthquake are presented in Table 3.
Replacing damaged health units
During a quick and one-day inspection by a 3-person team, a list of construction needs, infrastructure repairs and use of conex were identified to replace the service provider units. Following the destruction of a number of health facilities, health and treatment centers and two hospitals in Kermanshah Province, necessary coordination was made to provide a number of conexes as temporary facilities for providing health services to the public.
Mental health measures
By establishing 10 mental health teams (20 psychologists) at Sar-e Pol-e Zahab, 4 mental health teams (8 psychologists) at the health centers of the region, and 2 mental health teams (4 psychologists) at Ghasr-e Shirin and Salas-e Babajani, provision of mental health
Based on the information received from the base at Sar-e Pol-e Zahab, a safe location was determined for the landing of helicopters in the football field of Abuzar garrison (Army) in Sar-e Pol-e Zahab, and its geographic specifications were sent to all air emergency bases. Immediately after sunrise, all of the flight crew and medical personnel were summoned and prepared for dispatch to the affected areas. A total of 2 air ambulances and 20 helicopters were sent to the region for air transfer of the large numbers of the injured, and by cooperation of the army, the Guards, and the Red Crescent personnel, 4 airplanes were employed to send manpower and medical equipments to the affected areas and dispatch seriously injured victims from the scene of incident to treatment centers of the city of Kermanshah and other cities of the country.
The number of specialist forces and the amount of health and treatment equipments sent to the earthquake affected areas are presented in Table 2.
Surge capacity in the region and hospitals of other provinces
According to predetermined protocol, prompt action was taken to increase the hospitals capacity in terms of hospital beds. For this purpose, in addition to the transfer of facilities and equipments (which due to mass gathering of Arba`een religious ceremony were stationed at the border cities of Mehran, Chazabeh, and Shalamcheh), in the very early hours after the earthquake, the medical universities of Tehran, Alborz and Hamadan reported the capacity to receive the injured in each of the subsidiary centers and the status of specialist forces prepared for service in the hospitals associated with them.
Also, due to the logistical facilities provided in the region, during the first 20 hours, more than 7350 injured people were transferred to Kermanshah and other provinces using helicopters, airplanes, ambulances and ambulance buses to create more expeditious conditions for their treatment, and the potential to receive and treat other injured victims in Kermanshah hospitals. The status of the injured people referred to the treatment centers stationed in the earthquake- area and in treatment centers stationed in other provinces, as well as the number of hospitalizations and surgical procedures performed in these centers within the first 17 days after the earthquake are presented in Table 3.
Replacing damaged health units
During a quick and one-day inspection by a 3-person team, a list of construction needs, infrastructure repairs and use of conex were identified to replace the service provider units. Following the destruction of a number of health facilities, health and treatment centers and two hospitals in Kermanshah Province, necessary coordination was made to provide a number of conexes as temporary facilities for providing health services to the public.
Mental health measures
By establishing 10 mental health teams (20 psychologists) at Sar-e Pol-e Zahab, 4 mental health teams (8 psychologists) at the health centers of the region, and 2 mental health teams (4 psychologists) at Ghasr-e Shirin and Salas-e Babajani, provision of mental health
services for the earthquake victims began since the first days after the earthquake. Planning and coordination for screening the injured people, planning and coordination for the constant presence of mental health teams, placing on alert of up to 30 mental health teams and sending training packages related to mental and social consideration in disasters, were among the activities in mental health area in Kermanshah earthquake.
Also, in order to provide mental health services to the injured and their companions who were transferred to the treatment centers of Tehran, Alborz and Hamadan, 30 teams with 60 psychologists began their activities at these centers.
Health measures undertaken in the earthquake-stricken areas
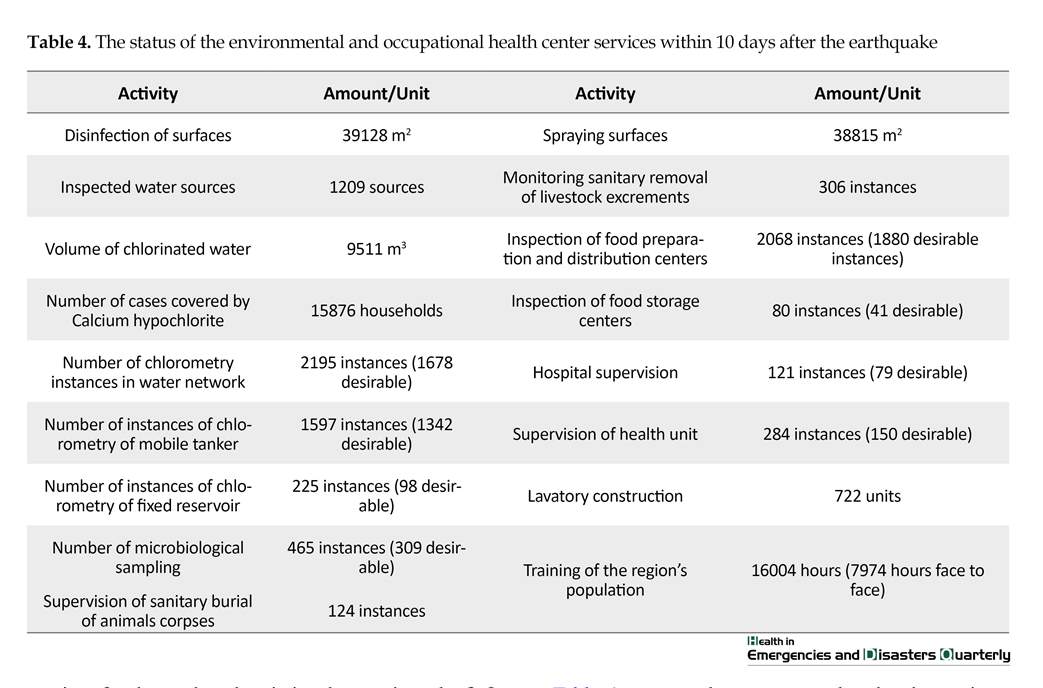
A total of 860 villages were covered by environmental health, and occupational teams in this field who performed activities such as burying corpses, controlling water and food materials, monitoring waste management and taking steps to fight pediculosis in households. Other environmental health activities in these regions were visiting 1046 water sources, 4114 instances of chlorometry, chlorination of 9324350 liters of drinking water, 387 sampling of drinking water, disinfection of 38398 square meters of surfaces, and visiting 1736 food materials preparation and distribution centers.
Table 4 presents the measures taken by the environmental and occupational health center of the Ministry of Health within 10 days after the earthquake.
Activities of Iran Blood Transfusion Organization
Within the first hour after the earthquake, coordination was made with the neighboring provinces to send the necessary blood and the crisis committee was formed at the headquarters of the Blood Transfusion Organization of Iran. Also general offices of blood transfusion, especially in support provinces, were ordered to be alert conforming to the National Blood Donation Network. With the capacity of mass media, public call was issued upon donation of negative type blood groups, especially O negative, and a fleet equipped with cold chain facility for blood transport to general offices of blood transfusion in the affected provinces was established. It is worth noting that blood donation reported during the first week after the earthquake was 58262 mL, with more than 10% the O negative blood group.
Strong points
Sending the Emergency Medical Technicians (EMT)
Dispatch of 100 rapid reaction teams to the area affected by the earthquake at the first hours after the earthquake allowed the immediate assessment of the severity of the incident, identifying the likely challenges and problems ahead, as well as the possibility of determining the magnitude of the disaster.
Activation of the center for directing Emergency Operations Center (EOC)
Immediately after the occurrence of the earthquake, the EOC of the Ministry of Health, Treatment, and Medical Education was activated and the Incident Command System (ICS) was set in place with the presence of the high ranking official of the Ministry and deputies. At the same time, the Emergency Organization took the central authority and activate and direct the operations at the affiliated universities of medical sciences and announcing red and orange status in accordance with the need and position of each of the satellite centers.
Prompt coordination to benefit from the logistical and operational potential of parallel and support organizations
Availability of senior directors of the Ministry of Health and the presence of a majority of the Ministry’s officials at the Operations Command Center help in necessary coordination for support and follow-up operations from the very early moments. The immediate response by military forces and other similar and support organizations played an effective role in the success of health and treatment services.
Coherence and coordination between the affiliated sectors of the Health and Treatment Workgroup
The existence of a center for crisis management command at the central headquarters and having unified management at this center, having an incident command system, the existence of an incident command system at each satellite area of the Ministry of Health, had an important role in the coherence of health and treatment workgroup and the adoption of appropriate measures in response to the earthquake. It is noteworthy that the presence of the 24-hour successor director in the Crisis Management Center, the coordination and interaction between the members stationed at the incident command system and use of previous members’ experiences are among the strong points that can be used in any probable future events.
Immediate meeting of the workgroup secretariat
The secretariat of the workgroup was promptly formed at the Ministry of Health, Treatment and Medical Education and while preparing the agenda in an orderly fashion and inviting the members to attend the meetings, the secretariat proceeded to follow up the implementations of each meeting’s approvals to obtain results. Indeed, the presence of experienced personnel in the management team stationed at the crisis management centers of the country’s medical universities and their affiliated hospitals and the high industriousness of the crisis experts had an effective role in execution of commands issued from the Incident Command Post (ICP) and the implementation of notified approvals.
Formation of the Patient Guidance Headquarters
This worthy step was taken to facilitate the transfer, hospitalization, identification of patients, and prevent the confusion of the injured and their families. Obviously, the existence of the crisis management center throughout the country and the training of officials and staff of these centers provided a suitable ground for the proper functioning of said headquarters and the management of the transfer and guidance of the injured.
Dispersal of Emergency Bases across the country
This dispersal led to an increase in the organization’s response ability for triage and eviction of the injured from the area. The scattering of the facilities of the Emergency Organization in the cities, as well as their close communication with the Central Emergency Department in Tehran to triage the injured and the removal and eviction of the injured from the scene of incident to hospitals, and especially the strong ability of the Emergency Operations team, contributed to its success.
Multiplicity and dispersion of mobilized treatment centers
Regarding the treatment of the injured, state-run hospitals became available as front line service providers. On the other hand, more than 750 private and charity hospitals announced their readiness to provide services, and private-sector forces were placed on standby. Dispersion of hospitals and health and treatment centers in the country was another factor effective in providing proper response to this incident.
Sufficient expert human resources
Emergency medicine specialists, general surgery, neurosurgery and orthopedics, and nursing’s different specialties, in sufficient numbers were ready to respond adequately to the needs of the affected area and the injured population. Furthermore, planning for the use of volunteers and nursing and paramedical students and medics added to the number of qualified specialist forces.
Depot of considerable equipment and medicines was provided by the Food and Drug Administration
The supply of treatment equipments and drugs and the ability to coordinate the provision of such resources in suitable time, were among other important and effective factors in the field of treatment.
Possibility of using all health facilities in disaster situations
Having a health team including the environment specialists, fighting disease experts, mental illness specialists and so on after the initial response phase, was effective in providing environmental health, controlling infectious diseases and helping to improve mental health and well-being in the first days after the earthquake.
Learning and practicing before facing disasters
Performing multiple table top drills and readiness of the operational forces, testing the ICS system in drills, using lessons learned from table top exercises and operations for similar situations, were effective in carrying out the above measures. Besides, assessing the points of strength and weakness in previous disasters were effective on how to response to the recent earthquake.
Weak points
Despite the many points of strengths mentioned, response operations had deficiencies and weaknesses in the areas of crisis management and command, rapid assessment, patient tracing, patient transfer, capacity building, and documentation.
Rapid assessment challenges
Although the Emergency Medical Technician teams were quickly deployed to the area for initial assessment of the incident, they were short of a specific structure and protocol for rapid assessment. In this regard, the standard tools are necessary for taking report from the incident site in the early days and weeks after the earthquake, as well as the possibility of reviewing and training the existing quick assessment tools. Furthermore, it is obligatory to form rapid assessment teams at local, regional and national levels accompanied with special instructions about the personal and professional equipment, cover waistcoats, and identification cards.
Challenges for the management and incident command
Despite description and position of the incident management and command system in the area of public health at the local, regional, and national level, the manner of incident management and command in the colleague and support organizations had the following weaknesses as follows:
1. Weakness in the position and status of EOC in the crisis management organizational system that challenged the necessary power and authority for calling and commanding representatives of various units in EOC;
2. Weaknesses in the EOC operations of Kermanshah Province based on the standards defined for this department including deficiency in the incidence management system activity and the absence of the main personnel with the identification cover and tags in the positions defined in the system and also the lack of appointing the successors.
3. Undue bustle and huddling of crowds in Kermanshah City, as well as the presence of VIPs and their interference in decision making, disrupted the managerial functions of this unit. This problem was due to the lack of a specific protocol for sending VIPs to the site of the incident;
4. Deficiencies in the proper organization of human resources in colleague and support organizations in incident management, including the inappropriate calling and distribution of relief forces in the incident areas due to the absence of a registering system for personnel entering the incident site as well as absence of a specified protocol for need assessment as well as calling and organizing volunteer forces;
5. Lack of identification and differentiation between individuals as well as professional and specialized teams in the field of incident due to lack of identification code or a suitable and identifiable cover waistcoats (high visibility clothing) especially for women, and the presence of individuals and specialist teams disregarding the characteristics of self-sufficiency;
6. Absence of task description protocol for support provinces.
7. Lack of proper communication between support and colleague organizations and the EOC of the university and hospitals and treatment centers;
8. Disorder in primary health services because of serious damage to health area infrastructures in damaged towns and villages, such as hospitals, health centers, rural and urban health and treatment centers due to structural and non-structural lack of safety;
9. Weakness in the need assessment and provision of social and psychosocial health services to those affected by the incident and the health staff attending the incident field due to the absence of a national protocol on post-incident social and psychosocial health services;
10. Absence of a specific program for patient tracing and hospital coordination systems.
Surge capacity
Deployed field hospitals, although provided a proper treatment capacity, were not all affiliated to one organization but rather to different organizations with different instructions and equipments. It seems that a unified management of field hospitals following the same standards and protocol in running the operations is needed. In addition, due to the lack of specifying a proper location for the stationing of these hospitals, a considerable time was lost for selecting the appropriate location. Therefore, the country’s health system should provide for arrangements to station field hospitals at minimum time by taking into account the complementary infrastructures such as helicopter pads and provision of security. The dependence and lack of self-sufficiency of these hospitals was another weakness of some of these hospitals in a way that some of them could not operate without the use of infrastructures such as water, electricity, and fuel.
Patient tracing
Despite the establishments of patients’ guidance headquarters, the weakness in recording, follow up and tracing of the patients and casualties from the field to the treatment centers was another weakness in the area of health in the recent earthquake. In many hospitals and treatment centers there were deficiencies in the complete registration of patients admitted there and the patients sent to other treatment centers.
Apparently recording profiles and taking report with a unified and standard form sheet is necessary. In general, registration of the injured and patients’ characteristics at the incident site, during the transfer and dispatch of patients and admission to treatment centers was defective due to the lack of unified protocol for patient tracing. Shortcomings in registration of the profile of some patients sent by air ambulance, as well as deficiencies in registering patients’ profile in field hospitals, were among other problems of the health system. Furthermore, the absence of a clear protocol to supply information to the public about patients and injured people who were admitted to hospitals, or were dispatched to, or released from treatment centers, had created concerns and problems for some companions and family members. In general, the information and reporting process and the statistics had many weaknesses that should be taken into account in future incidents.
Prehospital Emergency Services
Despite the timely and extensive presence of prehospital emergency services by mobilizing all the capabilities of this sector, this critical area needs to be developed in terms of structure, resources, manpower and especially aeronautical assistance with night vision which is one of the priorities of this field.
Weakness in provision of safety for the responders
The lack of attention to physical and mental health and briefing of personnel and service providers were among other neglected instances. Most medical emergency technicians worked for hours and were fatigued, and it is required that the rotating work system be implemented more efficiently. In addition to the aforementioned weaknesses, the lack of organized and national assessment teams, national disaster and incidents response program, and an unclear process in documenting the incident and activities, were other weaknesses associated with the performance of the crisis management organization which are realized in this earthquake.
4. Discussion
Based on the study results, the difference between the performance of the health system response in the recent earthquake (Kermanshah earthquake) and similar incidents in the past is prominent. One of the distinct points was the rapid start and the coherence of the health and treatment workgroup in response operations at the central headquarters and Kermanshah Province, as well as preparation of adjacent and assistant provinces.
This important measure was developed due to the existence of crisis management centers at the central headquarters and affiliated universities, the immediate formation of the health and treatment workgroup secretariat, the existence of an incident command system in each of the satellite areas of the Ministry of Health, and the use of qualified personnel in the management team stationed at these centers.
Also, the presence of the head of organization from the early hours of the incident at the site accelerated the process of coordination and provision of health services. This point is not agreed upon by all experts in this area, but in the Kermanshah incident, it led to coherence of command and management and facilitated the provision of resources. This capacity led to the rapid activation of EOCs at national, regional and local levels proportionate to the level of the incident and issuing an alert massage in the initial hours after the earthquake. In other words, it had a significant role in improving the performance of the workgroup in response to the recent earthquake.
A review of related experiences shows that our country lacks such an integrated managerial structure and coherence in the health system, and creating an integrated and coherent structure for managing hospitals in disasters and incidents was identified as one of the basic needs in the Bam earthquake [11]. Rapid assessment of the incident and injury is one of the key components of disaster management that affects the success or failure of response operations [12]. Therefore, rapid mapping of damaged areas and prompt estimate of the damages which resulted from extensive dispersal capacity of prehospital emergency bases in the region, use of SinaSa system, and sending 100 rapid assessment teams to the region, were other strong points in response to this earthquake indicating the ever increasing readiness of the health system to use national, regional and local capacities in the process of rapid assessment of damage in incident affected areas by using standard local tools.
Conforming to the findings of this study, using capacity of different organizations for rapid assessment has also been experienced elsewhere in the world. For example, after the hurricane Katrina, more than 95000 assessments of residential properties were carried out by local authorities and contractors of FEMA (Federal Emergency Management Agency) [13]. Apart from these strong points, lack of a clear protocol and national standard tools for rapid assessment, were a major challenge in this regard. According to the findings of our study, this problem was also present in the Azerbaijan earthquake [14] and it is advisable to examine this problem deeply in future incidents.
Studies have shown that coordination has always been one of the main challenges among individuals, groups and organizations responding to disasters in our country and around the world [14-17]. However, immediate and high inter-sectorial coordination in using logistical and operational capacities of the support and colleague organizations including the military and law enforcement forces (the Army and the Guard Corps), the Civil Defense organization, the Red Crescent Society, the Food and Drug Administration and the Blood Transfusion Organization, in rapid transfer of the injured and also the provision of pharmaceutical and blood products are among positive activities of the health and treatment workgroup in response to Kermanshah earthquake.
The extensive presence of high ranking officials of the health workgroup in the earthquake-stricken areas, as well as the use of individual capacities to communicate effectively with the authorities of colleague and support organizations had a positive impact on this coordination.
In the first 20 hours after the earthquake, nearly 7350 injured were transferred from the stricken areas to the treatment centers in the provinces of Kermanshah, Hamadan, Tehran and Alborz using the capabilities of patient guidance headquarters and the emergency prehospital fleet and logistical and transportation equipment of the colleague and support organizations present in the region. This indicates the high capability of the prehospital emergency operation team and high coordination with colleague and support organizations. Addition of helicopters and air ambulances in recent years to the prehospital emergency fleet has created a high capacity and recent experience has shown that the use of air ambulances in this earthquake (20 helicopters) was much more than the Azerbaijan earthquake (3 helicopters) [18].
Despite the sufficiency in composition, the quantity and quality of the human resources participating in incident management, the poor organization of calling and the distribution of specialist individuals and specialized teams, absence of a process in identifying the forces and their self-sufficiency were among the problems of manpower management in this earthquake. According to the findings of this study, these problems also were reported in the Bam earthquake [19, 20].
Considering the findings of the study, overlooking the physical and mental health of health service providers as well as the lack of a specific program for replacing the personnel were among other problems that the participants in the study acknowledged. Attention to the physical and mental health of health service providers in similar disasters and incidents is an important issue to which previous studies have pointed out [21].
Preparedness is one of the four main components of disaster risk management cycle and the readiness of organizations has a significant role in reducing the damages caused by disasters and incidents. Studies show that insufficient preparation is one of the main challenges of health area management in responding to incidents in our country [20, 22].
The rapid increase in the capacity to transfer and admission of the victims of the incident was one of the achievements in response to the Kermanshah earthquake. This achievement was the result of prehospital and hospital emergency preparedness, and in general, the preparedness of the health field of the western part of our country in connection with Arba`een religious ceremony in a way that in the aftermath of the earthquake, the capacities prepared to manage the possible incidents in Arba`een were quickly used for the injured of the Kermanshah earthquake. This lesson learned is the result of practical experience of the role and importance of preparedness for effective risk management in disasters and incidents.
Performing extensive treatment procedures including 1930 operations was another strong point of the response by the health and treatment workgroup after the earthquake indicating the high power and capacity of the specialist manpower and facilities for surgical operations in our country.
Regarding the incident management and command system, the weak status of the EOC in the structure of the workgroup and the crisis management organization, the weakness in observing the EOC functional standards, poor activation of the incident command system at EOC centers and colleague and support organizations, were among the problems reported in the said sector.
In this regard, since Bam earthquake, which was a turning point in creation of the structure and initial format of health and treatment workgroup of the healthcare team, significant efforts have been made to institutionalize this structure in health and treatment risk management of our country [17]; however, the experiences of this earthquake showed that conducting structural reforms in the status of EOC as well as training the managerial and command structure of the health and treatment workgroup based on the national response framework to subordinate units are inevitable.
Weakness in patient tracing, reporting and information on the condition of patients, resulting from the absence of a specific protocol and operational program in this regard, were among the main challenges reported on the response by the health field in this event. In the study by Tavakoli et al. (2017) the said problem was also one of the main findings of the study and it is necessary to address this problem in order to cope with future incidents [23].
5. Conclusion
Strong points of the health area response in Kermanshah earthquake were the result of the positive measures and steps taken by the secretariat of the health and treatment workgroup in recent years, promoting the status of prehospital emergency to a national organization, formulating numerous national guidelines and protocols such as the Disaster Hospital Preparedness National Plan, the nation’s health risk assessment tools, health safety assessment tools, health system response national plan and framework, and so on. However, based on the findings of this study, there are challenges that should be addressed by the health systems in order to improve the provision of health services in incidents and disasters.
The results of the present study can be used as lessons learned in effective management of incidents and disasters in our country and elsewhere in the world. Development of the Emergency Organization, especially the development of the Air Emergency, promoting the status of our country’s crisis management organization, accurate and careful planning for relief services such as temporary sheltering, provision of sanitation and bathrooms, development of mobile hospitals under unified management according to the findings of this study, are recommended.
Ethical Considerations
Compliance with ethical guidelines
There is no ethical principal to be considered doing this research.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interest
The Authors declare no conflict of interest.
Acknowledgments
The researchers hereby express their gratitude for the sincere cooperation of all directors and colleagues of the National Emergency Organization and the Ministry of Health, Treatment and Medical Education, and the personnel of Incident Management Center of Kermanshah University of Medical Sciences. We also would like to thank all colleagues, stakeholders and staffs that kindly cooperate to conduct this study.
References
Also, in order to provide mental health services to the injured and their companions who were transferred to the treatment centers of Tehran, Alborz and Hamadan, 30 teams with 60 psychologists began their activities at these centers.
Health measures undertaken in the earthquake-stricken areas
A total of 860 villages were covered by environmental health, and occupational teams in this field who performed activities such as burying corpses, controlling water and food materials, monitoring waste management and taking steps to fight pediculosis in households. Other environmental health activities in these regions were visiting 1046 water sources, 4114 instances of chlorometry, chlorination of 9324350 liters of drinking water, 387 sampling of drinking water, disinfection of 38398 square meters of surfaces, and visiting 1736 food materials preparation and distribution centers.
Table 4 presents the measures taken by the environmental and occupational health center of the Ministry of Health within 10 days after the earthquake.
Activities of Iran Blood Transfusion Organization
Within the first hour after the earthquake, coordination was made with the neighboring provinces to send the necessary blood and the crisis committee was formed at the headquarters of the Blood Transfusion Organization of Iran. Also general offices of blood transfusion, especially in support provinces, were ordered to be alert conforming to the National Blood Donation Network. With the capacity of mass media, public call was issued upon donation of negative type blood groups, especially O negative, and a fleet equipped with cold chain facility for blood transport to general offices of blood transfusion in the affected provinces was established. It is worth noting that blood donation reported during the first week after the earthquake was 58262 mL, with more than 10% the O negative blood group.
Strong points
Sending the Emergency Medical Technicians (EMT)
Dispatch of 100 rapid reaction teams to the area affected by the earthquake at the first hours after the earthquake allowed the immediate assessment of the severity of the incident, identifying the likely challenges and problems ahead, as well as the possibility of determining the magnitude of the disaster.
Activation of the center for directing Emergency Operations Center (EOC)
Immediately after the occurrence of the earthquake, the EOC of the Ministry of Health, Treatment, and Medical Education was activated and the Incident Command System (ICS) was set in place with the presence of the high ranking official of the Ministry and deputies. At the same time, the Emergency Organization took the central authority and activate and direct the operations at the affiliated universities of medical sciences and announcing red and orange status in accordance with the need and position of each of the satellite centers.
Prompt coordination to benefit from the logistical and operational potential of parallel and support organizations
Availability of senior directors of the Ministry of Health and the presence of a majority of the Ministry’s officials at the Operations Command Center help in necessary coordination for support and follow-up operations from the very early moments. The immediate response by military forces and other similar and support organizations played an effective role in the success of health and treatment services.
Coherence and coordination between the affiliated sectors of the Health and Treatment Workgroup
The existence of a center for crisis management command at the central headquarters and having unified management at this center, having an incident command system, the existence of an incident command system at each satellite area of the Ministry of Health, had an important role in the coherence of health and treatment workgroup and the adoption of appropriate measures in response to the earthquake. It is noteworthy that the presence of the 24-hour successor director in the Crisis Management Center, the coordination and interaction between the members stationed at the incident command system and use of previous members’ experiences are among the strong points that can be used in any probable future events.
Immediate meeting of the workgroup secretariat
The secretariat of the workgroup was promptly formed at the Ministry of Health, Treatment and Medical Education and while preparing the agenda in an orderly fashion and inviting the members to attend the meetings, the secretariat proceeded to follow up the implementations of each meeting’s approvals to obtain results. Indeed, the presence of experienced personnel in the management team stationed at the crisis management centers of the country’s medical universities and their affiliated hospitals and the high industriousness of the crisis experts had an effective role in execution of commands issued from the Incident Command Post (ICP) and the implementation of notified approvals.
Formation of the Patient Guidance Headquarters
This worthy step was taken to facilitate the transfer, hospitalization, identification of patients, and prevent the confusion of the injured and their families. Obviously, the existence of the crisis management center throughout the country and the training of officials and staff of these centers provided a suitable ground for the proper functioning of said headquarters and the management of the transfer and guidance of the injured.
Dispersal of Emergency Bases across the country
This dispersal led to an increase in the organization’s response ability for triage and eviction of the injured from the area. The scattering of the facilities of the Emergency Organization in the cities, as well as their close communication with the Central Emergency Department in Tehran to triage the injured and the removal and eviction of the injured from the scene of incident to hospitals, and especially the strong ability of the Emergency Operations team, contributed to its success.
Multiplicity and dispersion of mobilized treatment centers
Regarding the treatment of the injured, state-run hospitals became available as front line service providers. On the other hand, more than 750 private and charity hospitals announced their readiness to provide services, and private-sector forces were placed on standby. Dispersion of hospitals and health and treatment centers in the country was another factor effective in providing proper response to this incident.
Sufficient expert human resources
Emergency medicine specialists, general surgery, neurosurgery and orthopedics, and nursing’s different specialties, in sufficient numbers were ready to respond adequately to the needs of the affected area and the injured population. Furthermore, planning for the use of volunteers and nursing and paramedical students and medics added to the number of qualified specialist forces.
Depot of considerable equipment and medicines was provided by the Food and Drug Administration
The supply of treatment equipments and drugs and the ability to coordinate the provision of such resources in suitable time, were among other important and effective factors in the field of treatment.
Possibility of using all health facilities in disaster situations
Having a health team including the environment specialists, fighting disease experts, mental illness specialists and so on after the initial response phase, was effective in providing environmental health, controlling infectious diseases and helping to improve mental health and well-being in the first days after the earthquake.
Learning and practicing before facing disasters
Performing multiple table top drills and readiness of the operational forces, testing the ICS system in drills, using lessons learned from table top exercises and operations for similar situations, were effective in carrying out the above measures. Besides, assessing the points of strength and weakness in previous disasters were effective on how to response to the recent earthquake.
Weak points
Despite the many points of strengths mentioned, response operations had deficiencies and weaknesses in the areas of crisis management and command, rapid assessment, patient tracing, patient transfer, capacity building, and documentation.
Rapid assessment challenges
Although the Emergency Medical Technician teams were quickly deployed to the area for initial assessment of the incident, they were short of a specific structure and protocol for rapid assessment. In this regard, the standard tools are necessary for taking report from the incident site in the early days and weeks after the earthquake, as well as the possibility of reviewing and training the existing quick assessment tools. Furthermore, it is obligatory to form rapid assessment teams at local, regional and national levels accompanied with special instructions about the personal and professional equipment, cover waistcoats, and identification cards.
Challenges for the management and incident command
Despite description and position of the incident management and command system in the area of public health at the local, regional, and national level, the manner of incident management and command in the colleague and support organizations had the following weaknesses as follows:
1. Weakness in the position and status of EOC in the crisis management organizational system that challenged the necessary power and authority for calling and commanding representatives of various units in EOC;
2. Weaknesses in the EOC operations of Kermanshah Province based on the standards defined for this department including deficiency in the incidence management system activity and the absence of the main personnel with the identification cover and tags in the positions defined in the system and also the lack of appointing the successors.
3. Undue bustle and huddling of crowds in Kermanshah City, as well as the presence of VIPs and their interference in decision making, disrupted the managerial functions of this unit. This problem was due to the lack of a specific protocol for sending VIPs to the site of the incident;
4. Deficiencies in the proper organization of human resources in colleague and support organizations in incident management, including the inappropriate calling and distribution of relief forces in the incident areas due to the absence of a registering system for personnel entering the incident site as well as absence of a specified protocol for need assessment as well as calling and organizing volunteer forces;
5. Lack of identification and differentiation between individuals as well as professional and specialized teams in the field of incident due to lack of identification code or a suitable and identifiable cover waistcoats (high visibility clothing) especially for women, and the presence of individuals and specialist teams disregarding the characteristics of self-sufficiency;
6. Absence of task description protocol for support provinces.
7. Lack of proper communication between support and colleague organizations and the EOC of the university and hospitals and treatment centers;
8. Disorder in primary health services because of serious damage to health area infrastructures in damaged towns and villages, such as hospitals, health centers, rural and urban health and treatment centers due to structural and non-structural lack of safety;
9. Weakness in the need assessment and provision of social and psychosocial health services to those affected by the incident and the health staff attending the incident field due to the absence of a national protocol on post-incident social and psychosocial health services;
10. Absence of a specific program for patient tracing and hospital coordination systems.
Surge capacity
Deployed field hospitals, although provided a proper treatment capacity, were not all affiliated to one organization but rather to different organizations with different instructions and equipments. It seems that a unified management of field hospitals following the same standards and protocol in running the operations is needed. In addition, due to the lack of specifying a proper location for the stationing of these hospitals, a considerable time was lost for selecting the appropriate location. Therefore, the country’s health system should provide for arrangements to station field hospitals at minimum time by taking into account the complementary infrastructures such as helicopter pads and provision of security. The dependence and lack of self-sufficiency of these hospitals was another weakness of some of these hospitals in a way that some of them could not operate without the use of infrastructures such as water, electricity, and fuel.
Patient tracing
Despite the establishments of patients’ guidance headquarters, the weakness in recording, follow up and tracing of the patients and casualties from the field to the treatment centers was another weakness in the area of health in the recent earthquake. In many hospitals and treatment centers there were deficiencies in the complete registration of patients admitted there and the patients sent to other treatment centers.
Apparently recording profiles and taking report with a unified and standard form sheet is necessary. In general, registration of the injured and patients’ characteristics at the incident site, during the transfer and dispatch of patients and admission to treatment centers was defective due to the lack of unified protocol for patient tracing. Shortcomings in registration of the profile of some patients sent by air ambulance, as well as deficiencies in registering patients’ profile in field hospitals, were among other problems of the health system. Furthermore, the absence of a clear protocol to supply information to the public about patients and injured people who were admitted to hospitals, or were dispatched to, or released from treatment centers, had created concerns and problems for some companions and family members. In general, the information and reporting process and the statistics had many weaknesses that should be taken into account in future incidents.
Prehospital Emergency Services
Despite the timely and extensive presence of prehospital emergency services by mobilizing all the capabilities of this sector, this critical area needs to be developed in terms of structure, resources, manpower and especially aeronautical assistance with night vision which is one of the priorities of this field.
Weakness in provision of safety for the responders
The lack of attention to physical and mental health and briefing of personnel and service providers were among other neglected instances. Most medical emergency technicians worked for hours and were fatigued, and it is required that the rotating work system be implemented more efficiently. In addition to the aforementioned weaknesses, the lack of organized and national assessment teams, national disaster and incidents response program, and an unclear process in documenting the incident and activities, were other weaknesses associated with the performance of the crisis management organization which are realized in this earthquake.
4. Discussion
Based on the study results, the difference between the performance of the health system response in the recent earthquake (Kermanshah earthquake) and similar incidents in the past is prominent. One of the distinct points was the rapid start and the coherence of the health and treatment workgroup in response operations at the central headquarters and Kermanshah Province, as well as preparation of adjacent and assistant provinces.
This important measure was developed due to the existence of crisis management centers at the central headquarters and affiliated universities, the immediate formation of the health and treatment workgroup secretariat, the existence of an incident command system in each of the satellite areas of the Ministry of Health, and the use of qualified personnel in the management team stationed at these centers.
Also, the presence of the head of organization from the early hours of the incident at the site accelerated the process of coordination and provision of health services. This point is not agreed upon by all experts in this area, but in the Kermanshah incident, it led to coherence of command and management and facilitated the provision of resources. This capacity led to the rapid activation of EOCs at national, regional and local levels proportionate to the level of the incident and issuing an alert massage in the initial hours after the earthquake. In other words, it had a significant role in improving the performance of the workgroup in response to the recent earthquake.
A review of related experiences shows that our country lacks such an integrated managerial structure and coherence in the health system, and creating an integrated and coherent structure for managing hospitals in disasters and incidents was identified as one of the basic needs in the Bam earthquake [11]. Rapid assessment of the incident and injury is one of the key components of disaster management that affects the success or failure of response operations [12]. Therefore, rapid mapping of damaged areas and prompt estimate of the damages which resulted from extensive dispersal capacity of prehospital emergency bases in the region, use of SinaSa system, and sending 100 rapid assessment teams to the region, were other strong points in response to this earthquake indicating the ever increasing readiness of the health system to use national, regional and local capacities in the process of rapid assessment of damage in incident affected areas by using standard local tools.
Conforming to the findings of this study, using capacity of different organizations for rapid assessment has also been experienced elsewhere in the world. For example, after the hurricane Katrina, more than 95000 assessments of residential properties were carried out by local authorities and contractors of FEMA (Federal Emergency Management Agency) [13]. Apart from these strong points, lack of a clear protocol and national standard tools for rapid assessment, were a major challenge in this regard. According to the findings of our study, this problem was also present in the Azerbaijan earthquake [14] and it is advisable to examine this problem deeply in future incidents.
Studies have shown that coordination has always been one of the main challenges among individuals, groups and organizations responding to disasters in our country and around the world [14-17]. However, immediate and high inter-sectorial coordination in using logistical and operational capacities of the support and colleague organizations including the military and law enforcement forces (the Army and the Guard Corps), the Civil Defense organization, the Red Crescent Society, the Food and Drug Administration and the Blood Transfusion Organization, in rapid transfer of the injured and also the provision of pharmaceutical and blood products are among positive activities of the health and treatment workgroup in response to Kermanshah earthquake.
The extensive presence of high ranking officials of the health workgroup in the earthquake-stricken areas, as well as the use of individual capacities to communicate effectively with the authorities of colleague and support organizations had a positive impact on this coordination.
In the first 20 hours after the earthquake, nearly 7350 injured were transferred from the stricken areas to the treatment centers in the provinces of Kermanshah, Hamadan, Tehran and Alborz using the capabilities of patient guidance headquarters and the emergency prehospital fleet and logistical and transportation equipment of the colleague and support organizations present in the region. This indicates the high capability of the prehospital emergency operation team and high coordination with colleague and support organizations. Addition of helicopters and air ambulances in recent years to the prehospital emergency fleet has created a high capacity and recent experience has shown that the use of air ambulances in this earthquake (20 helicopters) was much more than the Azerbaijan earthquake (3 helicopters) [18].
Despite the sufficiency in composition, the quantity and quality of the human resources participating in incident management, the poor organization of calling and the distribution of specialist individuals and specialized teams, absence of a process in identifying the forces and their self-sufficiency were among the problems of manpower management in this earthquake. According to the findings of this study, these problems also were reported in the Bam earthquake [19, 20].
Considering the findings of the study, overlooking the physical and mental health of health service providers as well as the lack of a specific program for replacing the personnel were among other problems that the participants in the study acknowledged. Attention to the physical and mental health of health service providers in similar disasters and incidents is an important issue to which previous studies have pointed out [21].
Preparedness is one of the four main components of disaster risk management cycle and the readiness of organizations has a significant role in reducing the damages caused by disasters and incidents. Studies show that insufficient preparation is one of the main challenges of health area management in responding to incidents in our country [20, 22].
The rapid increase in the capacity to transfer and admission of the victims of the incident was one of the achievements in response to the Kermanshah earthquake. This achievement was the result of prehospital and hospital emergency preparedness, and in general, the preparedness of the health field of the western part of our country in connection with Arba`een religious ceremony in a way that in the aftermath of the earthquake, the capacities prepared to manage the possible incidents in Arba`een were quickly used for the injured of the Kermanshah earthquake. This lesson learned is the result of practical experience of the role and importance of preparedness for effective risk management in disasters and incidents.
Performing extensive treatment procedures including 1930 operations was another strong point of the response by the health and treatment workgroup after the earthquake indicating the high power and capacity of the specialist manpower and facilities for surgical operations in our country.
Regarding the incident management and command system, the weak status of the EOC in the structure of the workgroup and the crisis management organization, the weakness in observing the EOC functional standards, poor activation of the incident command system at EOC centers and colleague and support organizations, were among the problems reported in the said sector.
In this regard, since Bam earthquake, which was a turning point in creation of the structure and initial format of health and treatment workgroup of the healthcare team, significant efforts have been made to institutionalize this structure in health and treatment risk management of our country [17]; however, the experiences of this earthquake showed that conducting structural reforms in the status of EOC as well as training the managerial and command structure of the health and treatment workgroup based on the national response framework to subordinate units are inevitable.
Weakness in patient tracing, reporting and information on the condition of patients, resulting from the absence of a specific protocol and operational program in this regard, were among the main challenges reported on the response by the health field in this event. In the study by Tavakoli et al. (2017) the said problem was also one of the main findings of the study and it is necessary to address this problem in order to cope with future incidents [23].
5. Conclusion
Strong points of the health area response in Kermanshah earthquake were the result of the positive measures and steps taken by the secretariat of the health and treatment workgroup in recent years, promoting the status of prehospital emergency to a national organization, formulating numerous national guidelines and protocols such as the Disaster Hospital Preparedness National Plan, the nation’s health risk assessment tools, health safety assessment tools, health system response national plan and framework, and so on. However, based on the findings of this study, there are challenges that should be addressed by the health systems in order to improve the provision of health services in incidents and disasters.
The results of the present study can be used as lessons learned in effective management of incidents and disasters in our country and elsewhere in the world. Development of the Emergency Organization, especially the development of the Air Emergency, promoting the status of our country’s crisis management organization, accurate and careful planning for relief services such as temporary sheltering, provision of sanitation and bathrooms, development of mobile hospitals under unified management according to the findings of this study, are recommended.
Ethical Considerations
Compliance with ethical guidelines
There is no ethical principal to be considered doing this research.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interest
The Authors declare no conflict of interest.
Acknowledgments
The researchers hereby express their gratitude for the sincere cooperation of all directors and colleagues of the National Emergency Organization and the Ministry of Health, Treatment and Medical Education, and the personnel of Incident Management Center of Kermanshah University of Medical Sciences. We also would like to thank all colleagues, stakeholders and staffs that kindly cooperate to conduct this study.
References
- Pourhosseini SS, Ardalan A, Mehrolhassani MH. Key aspects of providing healthcare services in disaster response Stage. Iranian Journal of Public Health. 2015; 44(1):111-8. [PMID] [PMCID]
- Wilson JA, McKenzie LK, McLeod WT, Darsey DA, Craig J. Improving disaster response efforts through the development of a disaster health care response system. Disaster Medicine and Public Health Preparedness. 2017; 11(5):600-4. [DOI:10.1017/dmp.2016.192] [PMID]
- Koenig KL, Schultz CH. Koenig and Schultz’s: Disaster medicine: Comprehensive principles and practices. New York: Cambridge University Press; 2010.
- Guha-Sapir D, Hoyois P, Wallemacq P, Below R. Annual disaster statistical review 2016: The numbers and trends brussels. Brussels: CRED; 2016.
- Ardalan A. [Text book of Health in Emergency and Disaster (Persian)]. Tehran: Mehravash; 2016.
- Amini-Hosseini K, Hosseinioon S, Pooyan Z. An investigation into the socioeconomic aspects of two major earthquakes in Iran. Disasters. 2013; 37(3):516-35. [DOI:10.1111/disa.12001]
- Fitter DL, Delson DB, Guillaume FD, Schaad AW, Moffett DB, Poncelet JL, et al. Applying a new framework for public health systems recovery following emergencies and disasters: the example of Haiti following a major earthquake and cholera outbreak. The American Journal of Tropical Medicine and Hygiene. 2017; 97(4_Suppl):4-11. [DOI:10.4269/ajtmh.16-0862] [PMID] [PMCID]
- World Health Organization. Disaster risk management for health: Overview. Geneva: World Health Organization; 2011.
- Naghii MR. Public health impact and medical consequences of earthquakes. Revista Panamericana de Salud Pública. 2005; 180(3):216-21. [DOI:10.1590/S1020-49892005000800013]
- Ciottone G, Anderson PD, Heide EAD, Darling RG, Jacoby I, Noji E, et al. Disaster Medicine. Philadelphia: Mosby; 2006.
- World Health Organization. Health sector response to the Bam earthquake: lessons learnt. Geneva: World Health Organization; 2005.
- McEntire DA. Coordinating multi-organisational responses to disaster: Lessons from the March 28, 2000, fort worth tornado. Disaster Prevention and Management: An International Journal. 2002; 11(5):369-79. [DOI:10.1108/09653560210453416]
- Pistrika AK, Jonkman SN. Damage to residential buildings due to flooding of New Orleans after hurricane Katrina. Natural Hazards. 2010; 54(2):413-34. [DOI:10.1007/s11069-009-9476-y]
- Babaie J, Moslehi S, Ardalan A. Rapid health needs assessment experience in 11 August 2012 East Azerbaijan Earthquakes: A Qualitative Study. PLoS Currents Disasters. 2013; 6.
- Dynes RR. Community emergency planning: False assumption and inappropriate analogies. International Journal of Mass Emergencies and Disasters. 1994; 12(2):141-58.
- Achour N, Pascale F, Price AD, Polverino F, Aciksari K, Miyajima M, et al. Learning lessons from the 2011 Van Earthquake to enhance healthcare surge capacity in Turkey. Environmental Hazards. 2016; 15(1):74-94. [DOI:10.1080/17477891.2016.1139539]
- Khankeh HR, Khorasani-Zavareh D, Johanson E, Mohammadi R, Ahmadi F, Mohammadi R. Disaster health-related challenges and requirements: A grounded theory study in Iran. Prehospital and Disaster Medicine. 2011; 26(3):151-8. [DOI:10.1017/S1049023X11006200] [PMID]
- World Health Organization. Islamic Republic of Iran earthquake. [Internet] 2012 [Updated 2012 August 12]. Available from: http://www.who.int/hac/crises/irn/iran_sitrep_12august2012.pdf
- Sadeghi-Bazargani H, Azami-Aghdash S, Kazemi A, Ziapour B. Crisis management aspects of bam catastrophic earthquake. Health Promotion Perspectives. 2015; 5(1):3-13. [DOI:10.15171/hpp.2015.002] [PMID] [PMCID]
- Moosazadeh M, Zolala F, Sheikhzadeh K, Safiri S, Amiresmaili M. Response to the Bam earthquake: A qualitative study on the experiences of the top and middle level health managers in Kerman, Iran. Prehospital and Disaster Medicine. 2014; 29(4):388-91. [DOI:10.1017/S1049023X14000727] [PMID]
- Bilal MS, Rana MH, Rahim S, Ali S. Psychological trauma in a relief worker—A case report from earthquake-struck areas of north Pakistan. Prehospital and Disaster Medicine. 2007; 22(5):458-61. [PMID]
- Pouraghaei M, Jannati A, Moharamzadeh P, Ghaffarzad A, Far MH, Babaie J. Challenges of hospital response to the twin earthquakes of August 21, 2012, in East Azerbaijan, Iran. Disaster Medicine and Public Health Preparedness. 2017; 11(4):422-30. [DOI:10.1017/dmp.2016.153]
- Tavakoli N, Yarmohammadian MH, Safdari R, Keyvanara M. Patient tracking in earthquake emergency response in Iran: A qualitative study. World Journal of Emergency Medicine. 2017; 8(2):91-8. [PMID] [PMCID]
Type of Study: Research |
Subject:
Special
Received: 2018/02/23 | Accepted: 2018/05/15 | Published: 2018/07/1
Received: 2018/02/23 | Accepted: 2018/05/15 | Published: 2018/07/1
References
1. Pourhosseini SS, Ardalan A, Mehrolhassani MH. Key aspects of providing healthcare services in disaster response Stage. Iranian Journal of Public Health. 2015; 44(1):111-8. [PMID] [PMCID] [PMID] [PMCID]
2. Wilson JA, McKenzie LK, McLeod WT, Darsey DA, Craig J. Improving disaster response efforts through the development of a disaster health care response system. Disaster Medicine and Public Health Preparedness. 2017; 11(5):600-4. [DOI:10.1017/dmp.2016.192] [PMID] [DOI:10.1017/dmp.2016.192]
3. Koenig KL, Schultz CH. Koenig and Schultz's: Disaster medicine: Comprehensive principles and practices. New York: Cambridge University Press; 2010.
4. Guha-Sapir D, Hoyois P, Wallemacq P, Below R. Annual disaster statistical review 2016: The numbers and trends brussels. Brussels: CRED; 2016.
5. Ardalan A. [Text book of Health in Emergency and Disaster (Persian)]. Tehran: Mehravash; 2016.
6. Amini-Hosseini K, Hosseinioon S, Pooyan Z. An investigation into the socioeconomic aspects of two major earthquakes in Iran. Disasters. 2013; 37(3):516-35. [DOI:10.1111/disa.12001] [DOI:10.1111/disa.12001]
7. Fitter DL, Delson DB, Guillaume FD, Schaad AW, Moffett DB, Poncelet JL, et al. Applying a new framework for public health systems recovery following emergencies and disasters: the example of Haiti following a major earthquake and cholera outbreak. The American Journal of Tropical Medicine and Hygiene. 2017; 97(4_Suppl):4-11. [DOI:10.4269/ajtmh.16-0862] [PMID] [PMCID] [DOI:10.4269/ajtmh.16-0862]
8. World Health Organization. Disaster risk management for health: Overview. Geneva: World Health Organization; 2011.
9. Naghii MR. Public health impact and medical consequences of earthquakes. Revista Panamericana de Salud Pública. 2005; 180(3):216-21. [DOI:10.1590/S1020-49892005000800013] [DOI:10.1590/S1020-49892005000800013]
10. Ciottone G, Anderson PD, Heide EAD, Darling RG, Jacoby I, Noji E, et al. Disaster Medicine. Philadelphia: Mosby; 2006.
11. World Health Organization. Health sector response to the Bam earthquake: lessons learnt. Geneva: World Health Organization; 2005.
12. McEntire DA. Coordinating multi-organisational responses to disaster: Lessons from the March 28, 2000, fort worth tornado. Disaster Prevention and Management: An International Journal. 2002; 11(5):369-79. [DOI:10.1108/09653560210453416] [DOI:10.1108/09653560210453416]
13. Pistrika AK, Jonkman SN. Damage to residential buildings due to flooding of New Orleans after hurricane Katrina. Natural Hazards. 2010; 54(2):413-34. [DOI:10.1007/s11069-009-9476-y] [DOI:10.1007/s11069-009-9476-y]
14. Babaie J, Moslehi S, Ardalan A. Rapid health needs assessment experience in 11 August 2012 East Azerbaijan Earthquakes: A Qualitative Study. PLoS Currents Disasters. 2013; 6.
15. Dynes RR. Community emergency planning: False assumption and inappropriate analogies. International Journal of Mass Emergencies and Disasters. 1994; 12(2):141-58.
16. Achour N, Pascale F, Price AD, Polverino F, Aciksari K, Miyajima M, et al. Learning lessons from the 2011 Van Earthquake to enhance healthcare surge capacity in Turkey. Environmental Hazards. 2016; 15(1):74-94. [DOI:10.1080/17477891.2016.1139539] [DOI:10.1080/17477891.2016.1139539]
17. Khankeh HR, Khorasani-Zavareh D, Johanson E, Mohammadi R, Ahmadi F, Mohammadi R. Disaster health-related challenges and requirements: A grounded theory study in Iran. Prehospital and Disaster Medicine. 2011; 26(3):151-8. [DOI:10.1017/S1049023X11006200] [PMID] [DOI:10.1017/S1049023X11006200]
18. World Health Organization. Islamic Republic of Iran earthquake. [Internet] 2012 [Updated 2012 August 12]. Available from: http://www.who.int/hac/crises/irn/iran_sitrep_12august2012.pdf
19. Sadeghi-Bazargani H, Azami-Aghdash S, Kazemi A, Ziapour B. Crisis management aspects of bam catastrophic earthquake. Health Promotion Perspectives. 2015; 5(1):3-13. [DOI:10.15171/hpp.2015.002] [PMID] [PMCID] [DOI:10.15171/hpp.2015.002]
20. Moosazadeh M, Zolala F, Sheikhzadeh K, Safiri S, Amiresmaili M. Response to the Bam earthquake: A qualitative study on the experiences of the top and middle level health managers in Kerman, Iran. Prehospital and Disaster Medicine. 2014; 29(4):388-91. [DOI:10.1017/S1049023X14000727] [PMID] [DOI:10.1017/S1049023X14000727]
21. Bilal MS, Rana MH, Rahim S, Ali S. Psychological trauma in a relief worker—A case report from earthquake-struck areas of north Pakistan. Prehospital and Disaster Medicine. 2007; 22(5):458-61. [PMID] [DOI:10.1017/S1049023X00005215] [PMID]
22. Pouraghaei M, Jannati A, Moharamzadeh P, Ghaffarzad A, Far MH, Babaie J. Challenges of hospital response to the twin earthquakes of August 21, 2012, in East Azerbaijan, Iran. Disaster Medicine and Public Health Preparedness. 2017; 11(4):422-30. [DOI:10.1017/dmp.2016.153] [DOI:10.1017/dmp.2016.153]
23. Tavakoli N, Yarmohammadian MH, Safdari R, Keyvanara M. Patient tracking in earthquake emergency response in Iran: A qualitative study. World Journal of Emergency Medicine. 2017; 8(2):91-8. [PMID] [PMCID] [DOI:10.5847/wjem.j.1920-8642.2017.02.002] [PMID] [PMCID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Health in Emergencies and Disasters Quarterly
Health in Emergencies & Disasters Research Center, University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave, Tehran, Iran.
Journal Tel: +9821 71732816 (2816)
Publisher Tel: +9821 4535 5555 - 4535 5000
