

Volume 8, Issue 2 (Winter 2023)
Health in Emergencies and Disasters Quarterly 2023, 8(2): 77-86 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Moslehi S, Dehghani A, Masoumi G, Barghi Shirazi F. Vulnerability Management of the Elderly During COVID-19 Pandemic: A Systematic Review. Health in Emergencies and Disasters Quarterly 2023; 8 (2) :77-86
URL: http://hdq.uswr.ac.ir/article-1-394-en.html
URL: http://hdq.uswr.ac.ir/article-1-394-en.html



1- Health Management and Economics Research Center, Health Management Research Institute, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Health in Disasters and Emergencies, School of public health and safety , shahid-beheshty University of Medical Sciences, Tehran, Iran.
3- Emergency Medicine, Emergency Management Research Center, Iran University of Medical Sciences, Tehran, Iran.
4- Department of Health in Disasters and Emergencies, School of Health Management and Information Sciences, Iran University of Medical Sciences, Tehran, Iran. , fshirazi63@gmail.com, barghishirazi.f@iums.ac.ir
2- Department of Health in Disasters and Emergencies, School of public health and safety , shahid-beheshty University of Medical Sciences, Tehran, Iran.
3- Emergency Medicine, Emergency Management Research Center, Iran University of Medical Sciences, Tehran, Iran.
4- Department of Health in Disasters and Emergencies, School of Health Management and Information Sciences, Iran University of Medical Sciences, Tehran, Iran. , fshirazi63@gmail.com, barghishirazi.f@iums.ac.ir
Full-Text [PDF 577 kb]
(398 Downloads)
| Abstract (HTML) (1739 Views)
Full-Text: (250 Views)
1. Introduction
Today, the population of the elderly has increased in developing societies because of the advancement of medical knowledge, control of infectious diseases, reduction of infant mortality, reduction of fertility level, economic, political, social, and welfare changes, technological progress, improvement of nutritional status, and higher life expectancy. According to the census of Iran’s statistical center in 2006, about 7.3% of the country’s population was over 60 years old and was considered elderly [1]. The elderly population is increasing from 800 million people worldwide to 2 billion by 2050, of which 23% live in developed countries and 9% live in developing countries [2]. In a report on Iran’s elderly population, the United Nations has predicted that the average age of the country’s population will increase by 10 years between 2006 and 2026 [3]. The results of another study showed that the fatality of the disease in people over the age of 60 with underlying disease (0.4%) is more than in subjects under 60 years old (9.0%) [4].
With the development of technology, medical science, and the improvement of health and nutrition, people’s life expectancy has increased and the number of deaths has decreased; however, because of the population policies, the changes in the fertility level have also affected the speed of aging. Aging and its biological and social processes disrupt the function of various body organs and result in a gradual inability to manage personal affairs and fulfill the social role of an elderly person. The effect of these inadequacies on the social aspect of the elderly’s life is more obvious so the limitation of the personal communication network can be considered the result of such factors. This is while the social dimension of life has a crucial impact on health in general and the quality of life in particular [5].
COVID-19 is a highly infectious acute respiratory syndrome that can be transmitted through human (and animal) interaction and is officially known as the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [6]. In recent months, the spread of COVID-19 in different parts of the world is considered a threat to the health of most people. The virus was first reported in Wuhan, China in early December 2019. Health officials declare that this virus is more dangerous for the elderly and about 80% of the related deaths are in the population who age over 65 years. This virus is usually spread between people through coughing and sneezing, personal contact with an infected person, or touching infected surfaces and then touching the mouth, nose, and eyes. Centers for Disease Control and Prevention has recommended the following hygiene practices: frequent hand washing, drinking fluids, coughing into the inside of the elbow or a tissue, and staying at home if one feels sick [7].
During the COVID-19 pandemic, an increase in psychological problems, including anxiety and depression, has been reported [8]. The unpredictability and high prevalence of this disease have caused panic in people, which sometimes leads to psychosocial disorders [9]. Vulnerable groups, including cardiovascular patients and individuals with pulmonary complications, along with the elderly are facing major risks. Emerging data indicate that COVID-19 is associated with a higher mortality rate in the elderly as its rate varies from 6.3% to 8.14% [10]. The elderly are at high risk of COVID-19 because of the low function of the immune system and having underlying diseases; therefore, these factors can cause anxiety among them [11].
The spread of COVID-19 has caused various problems in all aspects of human life and has seriously damaged the leisure time of the elderly, based on reports [12]. According to the urgent needs of the elderly for an active lifestyle, inattention to this problem causes fundamental changes in the lifestyle of the elderly and institutionalizes an inactive lifestyle in them. That is, the problems caused by this virus can harm the lifestyle of the elderly by damaging the cultural, social, health, economic and individual aspects in such a way that inactivity is institutionalized in them as a habit. Lack of due consideration for the sports leisure culture of the elderly following the spread of COVID-19 can have long-term cultural and social effects on societies, especially in Iran, considering the pathogenicity of this virus. The speed of its spread and the percentage of death caused by the virus may also endanger the mental health of people at different levels of society, from affected patients to healthcare workers, families, children, students, psychological patients, and even personnel of different jobs.
Accordingly, in the current high-risk situation, it is necessary to identify people prone to psychological disorders at different levels of society, whose mental health may be endangered, so that the mental health of these people can be maintained with appropriate psychological strategies and techniques [13].
In the response program for disasters and accidents and pandemics, people over 60 years of age, who are introduced as the elderly group, are one of the critically vulnerable groups in the priority of providing services to responsible organizations. According to the conducted studies, the person’s position in the life cycle has a significant effect on the resulting vulnerability, and the elderly are exposed to more damage because they need more care, and the lack of financial resources, poor health and treatment, and special psychological conditions after the disaster exposes this population to injury and the possibility of catching the disease more than others. In addition to mental and physical injuries, social injuries resulting from disasters and pandemics are also raised in the elderly group, including social isolation, social incompatibility, non-acceptance, and feeling of lack of social support. Given the COVID-19 pandemic and the special features and effects of this emerging disease, this study is conducted to investigate the effects of the virus on the elderly.
2. Materials and Methods
This is a systematic review conducted from March 2018 to June 2021 to investigate the vulnerability management of the elderly during the COVID-19 pandemic. For this purpose, the following keywords were used: “COVID-19,” “Coronavirus,” Vulnerable groups,” and “The elderly.” Persian and English articles available on PubMed, Google Scholar, Science Direct, MediLib, SID, and Magiran databases were searched from March 2019 to 2021 and the preferred reporting items for systematic reviews and meta-analyses (PRISMA) framework was employed to report the articles. All research steps, including the search strategy, article selection, quality evaluation, and data extraction were done by the two researchers, independently.
Search strategy
In the first step, the search strategy was designed using keywords and standard terms based on the medical subject heading (MeSH) method, including “health management,” “elderly,” “COVID-19,” and “vulnerability.”
Data sources
Both library databases and reference databases were considered the main sources of our data. Considering that Persian articles were very limited in the field of data source validation, all English articles that were published without a time limit until the end of June 2021 by searching the Web of Science, PubMed, Scopus, Cochrane Library, Science Direct, Google Scholar, and Embase were selected. Books, academic websites, authoritative documents, and reports of international organizations were also studied and reviewed based on the purpose of the study.
Inclusion criteria
According to the purpose of the research and the timeframe determined by the research team, all English studies that mentioned the vulnerability of the elderly, health management of the elderly, and the periods of the pandemic of COVID-19, and based on the quality assessment case, with minimum desirable quality, were included in the study.
Exclusion criteria
Studies that did not have the minimum score required for quality and inclusion in the review based on quality assessment were excluded. In addition, review studies, narratives, meta-analyses, and case reports that discussed the elderly but had no report during the COVID-19 pandemic were eliminated. Non-English studies were also excluded from our study.
Qualitative evaluation of studies
The quality of the studies was assessed using the strengthening of the reporting of observational studies in epidemiology (STROBE) checklist. This checklist has 22 sections, which are scored based on the importance of each section. The lowest score on this checklist is 15 and the highest is 33. In this study, the minimum acceptable score is 20.
Data extraction
At first, the articles were reviewed by the two researchers independently. They reviewed the title and the abstract, and then considered the inclusion and exclusion criteria. Then, the full text of the articles was reviewed by the two researchers. If both rejected an article, the reason was mentioned, and in case of disagreement, such studies were judged by a third researcher. Data extraction was done using a standard checklist.
Study selection
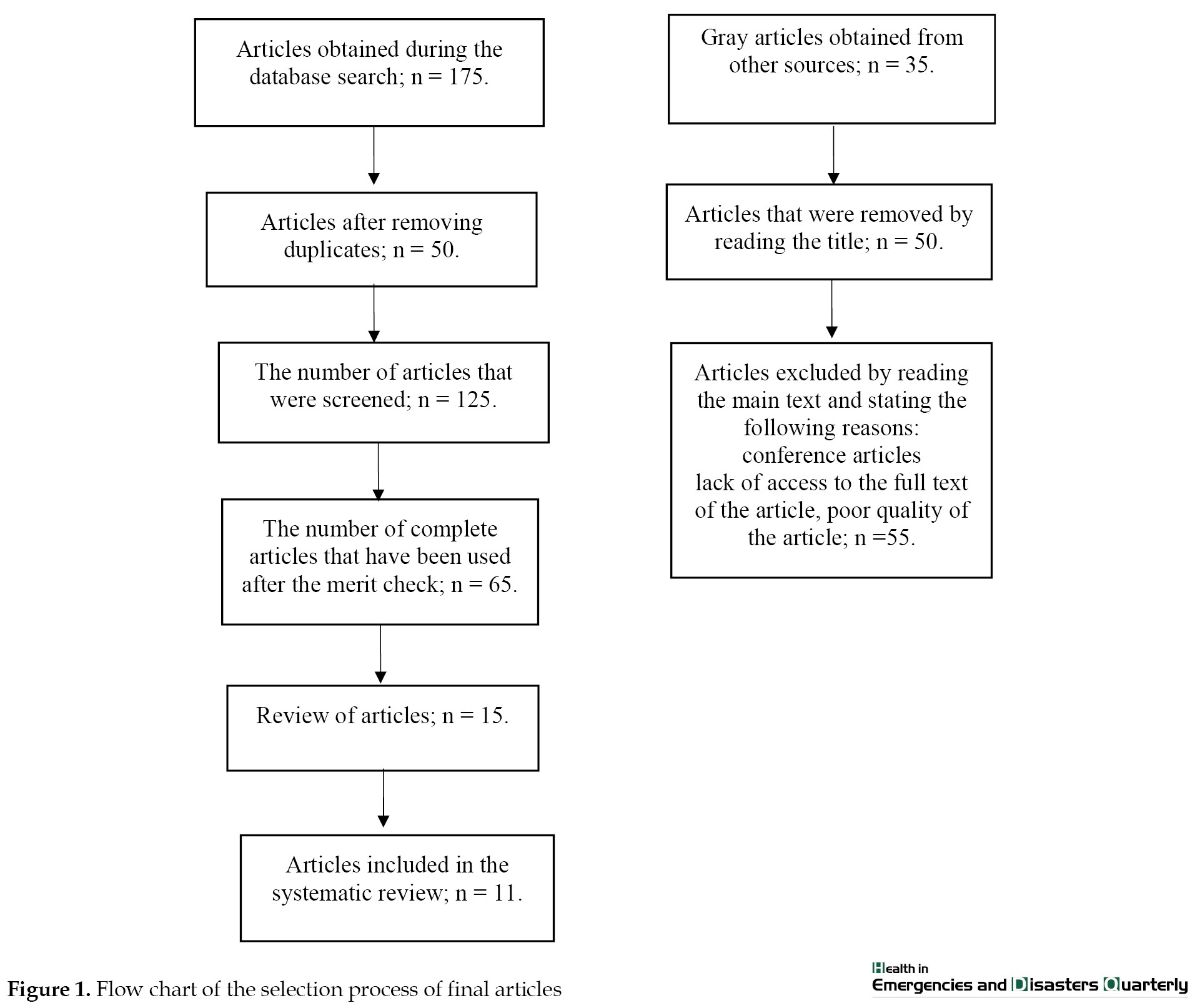
Articles, summaries, and documents related to the study were collected. The selection of keywords was based on the review of the texts and the opinions of experts. By searching for English articles in different databases, a total of 175 articles were obtained. Bibliographic information (title, author’s name, journal’s name, year of publication, period, and number) was entered in EndNote software, and duplicate articles were removed using “Find Duplicate.” After removing duplicate studies, 125 articles remained. The next step was the detailed study of the title and the abstract to identify eligible documents for inclusion in the study and remove irrelevant documents from the review. At this stage, the titles and abstracts of the articles were obtained and reviewed by the two experts to ensure their relevance to the study area. Subsequently, 65 articles were selected. The next step was to carefully read the full text of the articles to determine their relevance to the research objective. Therefore, 50 articles unrelated to the research objective and 4 duplicate articles were excluded. Finally, 11 articles were included in this review (Figure 1).
 3. Results
3. Results
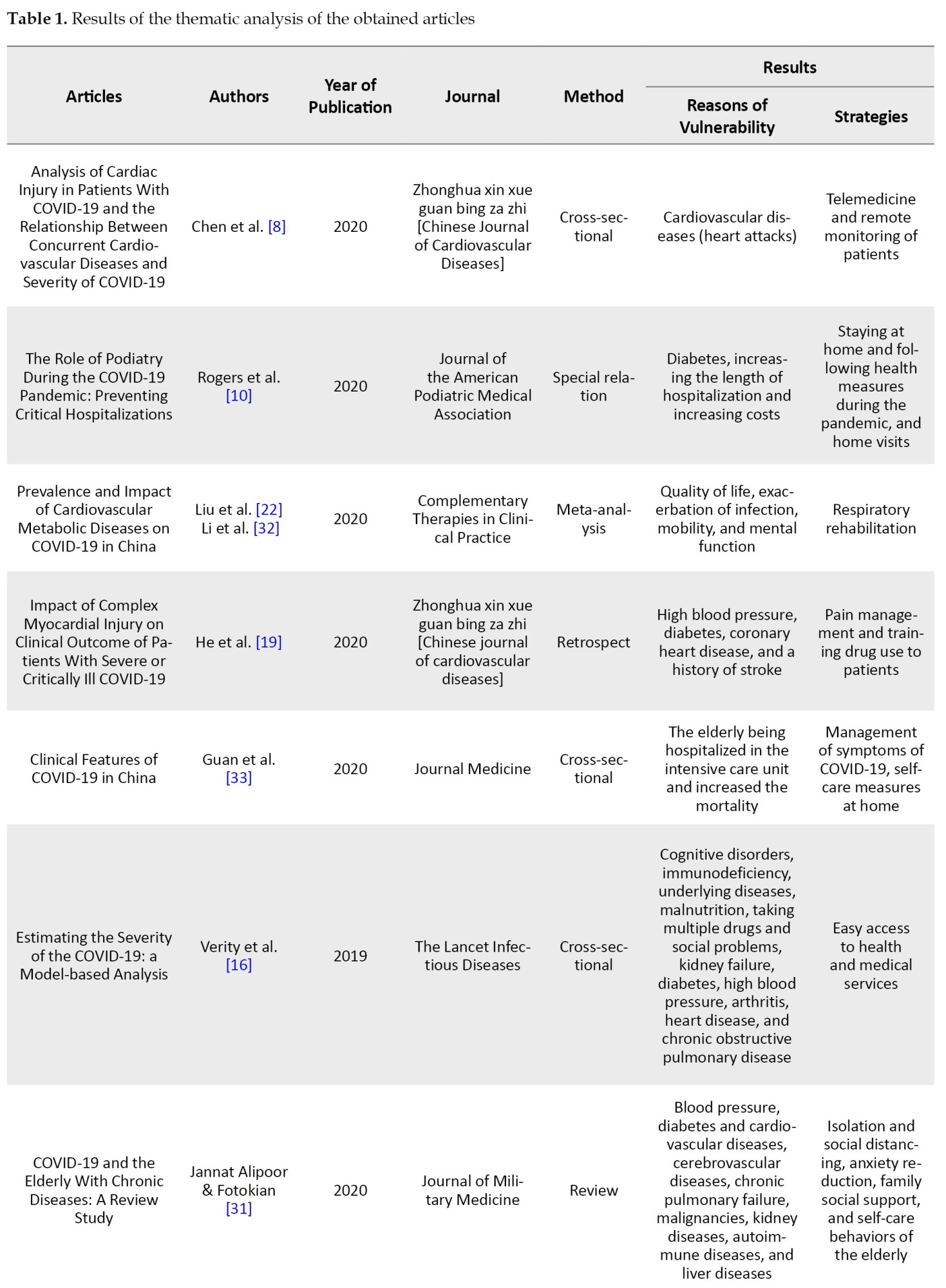
From the total of 175 reviewed studies, 11 articles were eligible and related to our purpose and were analyzed. The PRISMA framework was used to report the articles (Figure 1, Table 1).

The purpose of this study was to manage the vulnerability of the elderly during the COVID-19 pandemic. Given the special needs of the elderly during the COVID-19 pandemic and being sensitive to their vulnerability, the results can help them in this difficult situation.
During the outbreak of this disease, publishing new and correct information is essential. Much of this information is published online; however, the elderly may have limited access to new technologies. Therefore, information must be available to them through the media, newspapers, and magazines. Many of the elderly may not be familiar with the complex medical terms and statistics of the disease but it is their right to be informed of important information. For this reason, information should be provided to them in simple and understandable language [14].
According to the primary statistical data from China, the mortality rate in patients over 60 years old is much higher than the overall mortality rate. Accordingly, this rate is 14.8% in patients over 80 years old, 8% in patients aged 70-79 years, and 3.6% in patients aged 60-69. The share of deaths over the age of 60 is 81% of all deaths at the national level, which shows that the elderly are more vulnerable to SARS-CoV-2 [15]. The results of a study [16] showed that the lethality of the disease in people older than 60 years old with underlying disease (4.5%) is higher than in people younger than 60 years (1.4%). However, the reason why the elderly with underlying diseases is more susceptible to the disease is still unknown. Accordingly, various assumptions are raised, including in the lung where COVID-19 settles, changes in the physical characteristics of the lung tissue, or the aging of the immune system (immune senescence) increase the susceptibility of the elderly to the disease. The lung causes an immune response with cough reactions, mucus production, and airway clearance [17]. These responses have a vital role in expelling the virus from the airways and reducing the spread of the disease. While such responses decrease with increasing age in the body and the risk of COVID-19 increases in the elderly [18], after being infected with this virus, they appear “off” or have non-specific symptoms, such as decreased activity, sleepiness, lack of desire for food, indifference, confusion, delirium, loss of awareness of the surrounding environment, speech disorder, urinary incontinence, fall following the loss of balance and faint [19].
In addition, the results of other studies indicate that more than one-third of deaths among the elderly are caused by infectious diseases. Resistant viral infections may stimulate the expression of monoclonal T cells. While by increasing age, memory T cells have poor diversity, and for this reason, immune responses are activated later in the elderly than in children or young people. Therefore, in the face of pandemics, such as COVID-19, the elderly are among the sensitive and vulnerable groups [20].
During a study on the elderly conducted in China during the COVID-19 pandemic, it was shown that the emotional response of elderly women is higher than men so elderly women experience more anxiety and depression [20]. During the COVID-19 pandemic, the reduction of daily activities and the reduction of physical performance have significantly reduced the quality of life of the elderly [22]. Appropriate guidelines on COVID-19 and care of the elderly have been published by the World Health Organization, the Center for Disease Control and Prevention of the United States, and so on. These resources can be used to guide the elderly and care for them. Isolation and quarantine of the elderly at home may aggravate their psychological problems. For this reason, they should always be supported psychologically and emotionally and their relationship with family and relatives should be maintained, not necessarily physically, but with frequent voice and video calls [23].
In another study [24], the authors have also specified that to improve leisure time activities, it is necessary to form social interactions to reduce concerns about COVID-19. It seems that communication factors, by reducing the worries of the elderly following the spread of COVID-19, as well as informing about sports leisure programs during the spread of COVID-19 and the post-COVID-19 era can create the primary platform for the persistence of the culture of sports leisure time for the elderly after the spread of COVID-19. In other words, economic and communication factors improve the sustainability of the leisure time of sports culture in the elderly after the spread of COVID-19 by facilitating the sports leisure activities of the elderly and making them available [25].
Also, research [26] has shown that during the outbreak of COVID-19, with an increased level of perceived social support, the level of anxiety decreases significantly. Perceived social support should be considered a determinant of anxiety during the COVID-19 pandemic.
Based on the results obtained from a study [27], the causal model of the relationship between perceived stress, sense of coherence, perceived social support, and COVID-19 anxiety in the elderly according to various indicators of the confirmed fit of perceived stress, the sense of coherence and perceived social support have a direct effect on COVID-19 anxiety of the elderly. Also, perceived stress and a sense of cohesion through perceived social support have an indirect effect on COVID-19 anxiety in the elderly (P < 0.05). Therefore, during the COVID-19 pandemic, it is possible to reduce the anxiety of COVID-19 in the elderly by awareness and applying measures to empower this population in the field of perceived stress, sense of cohesion, and perceived social support.
The elderly are more susceptible to the disease than the younger groups [28]. Recently, research has shown that the high rate of COVID-19 in the elderly is because of cognitive disorders, immune deficiency, underlying diseases, malnutrition, taking multiple medications, and social problems. Background diseases, such as kidney failure, diabetes, high blood pressure, arthritis, heart diseases, and chronic obstructive pulmonary disease are more common in the elderly. For this reason, in developing countries, the number of elderly people suffering and dying from COVID-19 is more compared to other age groups [16, 29]. The presence of underlying diseases in the elderly as well as the changes caused by the aging process in various body systems, including the immunity system can affect the nature and severity of the clinical symptoms of the disease in the elderly [30]. The report of the Center for Disease Control and Prevention indicates that the rate of hospitalization, admission to the intensive care unit, and death because of COVID-19 in the elderly is more than other age groups [31].
Investigations on the elderly with COVID-19 showed that most of this population (60.7%) were suffering from underlying diseases and about one-third of them were suffering from two or more underlying diseases. The most common underlying disease in the elderly with COVID-19 was blood pressure (40.8%), diabetes (16%), and cardiovascular diseases (14.2%). Other underlying diseases with lower frequency include cerebrovascular diseases (6.2%), chronic pulmonary insufficiency (6.2%), malignancies (4.4%), kidney diseases (3.8%), autoimmune diseases (1.5%), and liver diseases (1.6%) [32].
According to studies and reviews [33], the mortality rate in patients over 60 is much higher than the overall mortality rate. This rate is 14.8% in patients over 80 years old, 8% in patients with 70 to 79 years of age, and 3.6% in patients aged 60 to 69. The share of deaths over 60 years is 81% of all deaths at the national level, which indicates that the elderly is more vulnerable to SARS-CoV-2.
4. Conclusion
According to the results obtained from a population of elderly who have stayed at home for a long time, problems with accessing their daily needs have been reported and they have been exposed to the risk of social isolation, abuse, and age discrimination. To control the negative consequences of this disease in the elderly, government officials, people, and families should consider methods and laws to minimize the possibility of misbehavior and age discrimination and provide equal opportunities to all individuals. Families should also be aware of the increase in social isolation among the elderly and maintain their relationship with them. Considering that the elderly may not have much access to the internet and new technologies, public media, radio, and television, can play a vital role in informing about COVID-19. These media outlets should provide the elderly with necessary information about COVID-19 by avoiding rumors and fear. Paying attention to social support as an economic and cheap resource to deal with anxiety and depression and improve the quality of life and mental well-being of the elderly has particular importance. Given that now the elderly should spend most of their time at home and their physical and sports activities and social interactions have decreased, virtual communication technologies can help to maintain and improve the health and positive mental well-being of the elderly. Also, by maintaining or creating virtual interpersonal relationships, such technologies can maintain and improve the social solidarity of the elderly. Compared to formal social activities and individual activities, informal social activities, such as communication with friends and relatives, have a greater effect on positive mental well-being in the elderly during the spread of COVID-19. Considering the importance of infrastructural factors in improving the sustainability of the culture of sport leisure times of the elderly following the outbreak of COVID-19, it is suggested to promote and improve the sustainability of the culture of sports leisure times for the elderly following the spread of the COVID-19 by creating camps for sports leisure times for the elderly and installing special sports places for this population in the post-COVID-19 era. It should be noted that intervention measures, such as self-care training can help prevent disease and improve the health of these people. In this regard, the importance of social distancing should be taught and managed.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgments
We thank all the professors who helped enrich the present material with their valuable comments.
References
Today, the population of the elderly has increased in developing societies because of the advancement of medical knowledge, control of infectious diseases, reduction of infant mortality, reduction of fertility level, economic, political, social, and welfare changes, technological progress, improvement of nutritional status, and higher life expectancy. According to the census of Iran’s statistical center in 2006, about 7.3% of the country’s population was over 60 years old and was considered elderly [1]. The elderly population is increasing from 800 million people worldwide to 2 billion by 2050, of which 23% live in developed countries and 9% live in developing countries [2]. In a report on Iran’s elderly population, the United Nations has predicted that the average age of the country’s population will increase by 10 years between 2006 and 2026 [3]. The results of another study showed that the fatality of the disease in people over the age of 60 with underlying disease (0.4%) is more than in subjects under 60 years old (9.0%) [4].
With the development of technology, medical science, and the improvement of health and nutrition, people’s life expectancy has increased and the number of deaths has decreased; however, because of the population policies, the changes in the fertility level have also affected the speed of aging. Aging and its biological and social processes disrupt the function of various body organs and result in a gradual inability to manage personal affairs and fulfill the social role of an elderly person. The effect of these inadequacies on the social aspect of the elderly’s life is more obvious so the limitation of the personal communication network can be considered the result of such factors. This is while the social dimension of life has a crucial impact on health in general and the quality of life in particular [5].
COVID-19 is a highly infectious acute respiratory syndrome that can be transmitted through human (and animal) interaction and is officially known as the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [6]. In recent months, the spread of COVID-19 in different parts of the world is considered a threat to the health of most people. The virus was first reported in Wuhan, China in early December 2019. Health officials declare that this virus is more dangerous for the elderly and about 80% of the related deaths are in the population who age over 65 years. This virus is usually spread between people through coughing and sneezing, personal contact with an infected person, or touching infected surfaces and then touching the mouth, nose, and eyes. Centers for Disease Control and Prevention has recommended the following hygiene practices: frequent hand washing, drinking fluids, coughing into the inside of the elbow or a tissue, and staying at home if one feels sick [7].
During the COVID-19 pandemic, an increase in psychological problems, including anxiety and depression, has been reported [8]. The unpredictability and high prevalence of this disease have caused panic in people, which sometimes leads to psychosocial disorders [9]. Vulnerable groups, including cardiovascular patients and individuals with pulmonary complications, along with the elderly are facing major risks. Emerging data indicate that COVID-19 is associated with a higher mortality rate in the elderly as its rate varies from 6.3% to 8.14% [10]. The elderly are at high risk of COVID-19 because of the low function of the immune system and having underlying diseases; therefore, these factors can cause anxiety among them [11].
The spread of COVID-19 has caused various problems in all aspects of human life and has seriously damaged the leisure time of the elderly, based on reports [12]. According to the urgent needs of the elderly for an active lifestyle, inattention to this problem causes fundamental changes in the lifestyle of the elderly and institutionalizes an inactive lifestyle in them. That is, the problems caused by this virus can harm the lifestyle of the elderly by damaging the cultural, social, health, economic and individual aspects in such a way that inactivity is institutionalized in them as a habit. Lack of due consideration for the sports leisure culture of the elderly following the spread of COVID-19 can have long-term cultural and social effects on societies, especially in Iran, considering the pathogenicity of this virus. The speed of its spread and the percentage of death caused by the virus may also endanger the mental health of people at different levels of society, from affected patients to healthcare workers, families, children, students, psychological patients, and even personnel of different jobs.
Accordingly, in the current high-risk situation, it is necessary to identify people prone to psychological disorders at different levels of society, whose mental health may be endangered, so that the mental health of these people can be maintained with appropriate psychological strategies and techniques [13].
In the response program for disasters and accidents and pandemics, people over 60 years of age, who are introduced as the elderly group, are one of the critically vulnerable groups in the priority of providing services to responsible organizations. According to the conducted studies, the person’s position in the life cycle has a significant effect on the resulting vulnerability, and the elderly are exposed to more damage because they need more care, and the lack of financial resources, poor health and treatment, and special psychological conditions after the disaster exposes this population to injury and the possibility of catching the disease more than others. In addition to mental and physical injuries, social injuries resulting from disasters and pandemics are also raised in the elderly group, including social isolation, social incompatibility, non-acceptance, and feeling of lack of social support. Given the COVID-19 pandemic and the special features and effects of this emerging disease, this study is conducted to investigate the effects of the virus on the elderly.
2. Materials and Methods
This is a systematic review conducted from March 2018 to June 2021 to investigate the vulnerability management of the elderly during the COVID-19 pandemic. For this purpose, the following keywords were used: “COVID-19,” “Coronavirus,” Vulnerable groups,” and “The elderly.” Persian and English articles available on PubMed, Google Scholar, Science Direct, MediLib, SID, and Magiran databases were searched from March 2019 to 2021 and the preferred reporting items for systematic reviews and meta-analyses (PRISMA) framework was employed to report the articles. All research steps, including the search strategy, article selection, quality evaluation, and data extraction were done by the two researchers, independently.
Search strategy
In the first step, the search strategy was designed using keywords and standard terms based on the medical subject heading (MeSH) method, including “health management,” “elderly,” “COVID-19,” and “vulnerability.”
Data sources
Both library databases and reference databases were considered the main sources of our data. Considering that Persian articles were very limited in the field of data source validation, all English articles that were published without a time limit until the end of June 2021 by searching the Web of Science, PubMed, Scopus, Cochrane Library, Science Direct, Google Scholar, and Embase were selected. Books, academic websites, authoritative documents, and reports of international organizations were also studied and reviewed based on the purpose of the study.
Inclusion criteria
According to the purpose of the research and the timeframe determined by the research team, all English studies that mentioned the vulnerability of the elderly, health management of the elderly, and the periods of the pandemic of COVID-19, and based on the quality assessment case, with minimum desirable quality, were included in the study.
Exclusion criteria
Studies that did not have the minimum score required for quality and inclusion in the review based on quality assessment were excluded. In addition, review studies, narratives, meta-analyses, and case reports that discussed the elderly but had no report during the COVID-19 pandemic were eliminated. Non-English studies were also excluded from our study.
Qualitative evaluation of studies
The quality of the studies was assessed using the strengthening of the reporting of observational studies in epidemiology (STROBE) checklist. This checklist has 22 sections, which are scored based on the importance of each section. The lowest score on this checklist is 15 and the highest is 33. In this study, the minimum acceptable score is 20.
Data extraction
At first, the articles were reviewed by the two researchers independently. They reviewed the title and the abstract, and then considered the inclusion and exclusion criteria. Then, the full text of the articles was reviewed by the two researchers. If both rejected an article, the reason was mentioned, and in case of disagreement, such studies were judged by a third researcher. Data extraction was done using a standard checklist.
Study selection
Articles, summaries, and documents related to the study were collected. The selection of keywords was based on the review of the texts and the opinions of experts. By searching for English articles in different databases, a total of 175 articles were obtained. Bibliographic information (title, author’s name, journal’s name, year of publication, period, and number) was entered in EndNote software, and duplicate articles were removed using “Find Duplicate.” After removing duplicate studies, 125 articles remained. The next step was the detailed study of the title and the abstract to identify eligible documents for inclusion in the study and remove irrelevant documents from the review. At this stage, the titles and abstracts of the articles were obtained and reviewed by the two experts to ensure their relevance to the study area. Subsequently, 65 articles were selected. The next step was to carefully read the full text of the articles to determine their relevance to the research objective. Therefore, 50 articles unrelated to the research objective and 4 duplicate articles were excluded. Finally, 11 articles were included in this review (Figure 1).
From the total of 175 reviewed studies, 11 articles were eligible and related to our purpose and were analyzed. The PRISMA framework was used to report the articles (Figure 1, Table 1).
The purpose of this study was to manage the vulnerability of the elderly during the COVID-19 pandemic. Given the special needs of the elderly during the COVID-19 pandemic and being sensitive to their vulnerability, the results can help them in this difficult situation.
During the outbreak of this disease, publishing new and correct information is essential. Much of this information is published online; however, the elderly may have limited access to new technologies. Therefore, information must be available to them through the media, newspapers, and magazines. Many of the elderly may not be familiar with the complex medical terms and statistics of the disease but it is their right to be informed of important information. For this reason, information should be provided to them in simple and understandable language [14].
According to the primary statistical data from China, the mortality rate in patients over 60 years old is much higher than the overall mortality rate. Accordingly, this rate is 14.8% in patients over 80 years old, 8% in patients aged 70-79 years, and 3.6% in patients aged 60-69. The share of deaths over the age of 60 is 81% of all deaths at the national level, which shows that the elderly are more vulnerable to SARS-CoV-2 [15]. The results of a study [16] showed that the lethality of the disease in people older than 60 years old with underlying disease (4.5%) is higher than in people younger than 60 years (1.4%). However, the reason why the elderly with underlying diseases is more susceptible to the disease is still unknown. Accordingly, various assumptions are raised, including in the lung where COVID-19 settles, changes in the physical characteristics of the lung tissue, or the aging of the immune system (immune senescence) increase the susceptibility of the elderly to the disease. The lung causes an immune response with cough reactions, mucus production, and airway clearance [17]. These responses have a vital role in expelling the virus from the airways and reducing the spread of the disease. While such responses decrease with increasing age in the body and the risk of COVID-19 increases in the elderly [18], after being infected with this virus, they appear “off” or have non-specific symptoms, such as decreased activity, sleepiness, lack of desire for food, indifference, confusion, delirium, loss of awareness of the surrounding environment, speech disorder, urinary incontinence, fall following the loss of balance and faint [19].
In addition, the results of other studies indicate that more than one-third of deaths among the elderly are caused by infectious diseases. Resistant viral infections may stimulate the expression of monoclonal T cells. While by increasing age, memory T cells have poor diversity, and for this reason, immune responses are activated later in the elderly than in children or young people. Therefore, in the face of pandemics, such as COVID-19, the elderly are among the sensitive and vulnerable groups [20].
During a study on the elderly conducted in China during the COVID-19 pandemic, it was shown that the emotional response of elderly women is higher than men so elderly women experience more anxiety and depression [20]. During the COVID-19 pandemic, the reduction of daily activities and the reduction of physical performance have significantly reduced the quality of life of the elderly [22]. Appropriate guidelines on COVID-19 and care of the elderly have been published by the World Health Organization, the Center for Disease Control and Prevention of the United States, and so on. These resources can be used to guide the elderly and care for them. Isolation and quarantine of the elderly at home may aggravate their psychological problems. For this reason, they should always be supported psychologically and emotionally and their relationship with family and relatives should be maintained, not necessarily physically, but with frequent voice and video calls [23].
In another study [24], the authors have also specified that to improve leisure time activities, it is necessary to form social interactions to reduce concerns about COVID-19. It seems that communication factors, by reducing the worries of the elderly following the spread of COVID-19, as well as informing about sports leisure programs during the spread of COVID-19 and the post-COVID-19 era can create the primary platform for the persistence of the culture of sports leisure time for the elderly after the spread of COVID-19. In other words, economic and communication factors improve the sustainability of the leisure time of sports culture in the elderly after the spread of COVID-19 by facilitating the sports leisure activities of the elderly and making them available [25].
Also, research [26] has shown that during the outbreak of COVID-19, with an increased level of perceived social support, the level of anxiety decreases significantly. Perceived social support should be considered a determinant of anxiety during the COVID-19 pandemic.
Based on the results obtained from a study [27], the causal model of the relationship between perceived stress, sense of coherence, perceived social support, and COVID-19 anxiety in the elderly according to various indicators of the confirmed fit of perceived stress, the sense of coherence and perceived social support have a direct effect on COVID-19 anxiety of the elderly. Also, perceived stress and a sense of cohesion through perceived social support have an indirect effect on COVID-19 anxiety in the elderly (P < 0.05). Therefore, during the COVID-19 pandemic, it is possible to reduce the anxiety of COVID-19 in the elderly by awareness and applying measures to empower this population in the field of perceived stress, sense of cohesion, and perceived social support.
The elderly are more susceptible to the disease than the younger groups [28]. Recently, research has shown that the high rate of COVID-19 in the elderly is because of cognitive disorders, immune deficiency, underlying diseases, malnutrition, taking multiple medications, and social problems. Background diseases, such as kidney failure, diabetes, high blood pressure, arthritis, heart diseases, and chronic obstructive pulmonary disease are more common in the elderly. For this reason, in developing countries, the number of elderly people suffering and dying from COVID-19 is more compared to other age groups [16, 29]. The presence of underlying diseases in the elderly as well as the changes caused by the aging process in various body systems, including the immunity system can affect the nature and severity of the clinical symptoms of the disease in the elderly [30]. The report of the Center for Disease Control and Prevention indicates that the rate of hospitalization, admission to the intensive care unit, and death because of COVID-19 in the elderly is more than other age groups [31].
Investigations on the elderly with COVID-19 showed that most of this population (60.7%) were suffering from underlying diseases and about one-third of them were suffering from two or more underlying diseases. The most common underlying disease in the elderly with COVID-19 was blood pressure (40.8%), diabetes (16%), and cardiovascular diseases (14.2%). Other underlying diseases with lower frequency include cerebrovascular diseases (6.2%), chronic pulmonary insufficiency (6.2%), malignancies (4.4%), kidney diseases (3.8%), autoimmune diseases (1.5%), and liver diseases (1.6%) [32].
According to studies and reviews [33], the mortality rate in patients over 60 is much higher than the overall mortality rate. This rate is 14.8% in patients over 80 years old, 8% in patients with 70 to 79 years of age, and 3.6% in patients aged 60 to 69. The share of deaths over 60 years is 81% of all deaths at the national level, which indicates that the elderly is more vulnerable to SARS-CoV-2.
4. Conclusion
According to the results obtained from a population of elderly who have stayed at home for a long time, problems with accessing their daily needs have been reported and they have been exposed to the risk of social isolation, abuse, and age discrimination. To control the negative consequences of this disease in the elderly, government officials, people, and families should consider methods and laws to minimize the possibility of misbehavior and age discrimination and provide equal opportunities to all individuals. Families should also be aware of the increase in social isolation among the elderly and maintain their relationship with them. Considering that the elderly may not have much access to the internet and new technologies, public media, radio, and television, can play a vital role in informing about COVID-19. These media outlets should provide the elderly with necessary information about COVID-19 by avoiding rumors and fear. Paying attention to social support as an economic and cheap resource to deal with anxiety and depression and improve the quality of life and mental well-being of the elderly has particular importance. Given that now the elderly should spend most of their time at home and their physical and sports activities and social interactions have decreased, virtual communication technologies can help to maintain and improve the health and positive mental well-being of the elderly. Also, by maintaining or creating virtual interpersonal relationships, such technologies can maintain and improve the social solidarity of the elderly. Compared to formal social activities and individual activities, informal social activities, such as communication with friends and relatives, have a greater effect on positive mental well-being in the elderly during the spread of COVID-19. Considering the importance of infrastructural factors in improving the sustainability of the culture of sport leisure times of the elderly following the outbreak of COVID-19, it is suggested to promote and improve the sustainability of the culture of sports leisure times for the elderly following the spread of the COVID-19 by creating camps for sports leisure times for the elderly and installing special sports places for this population in the post-COVID-19 era. It should be noted that intervention measures, such as self-care training can help prevent disease and improve the health of these people. In this regard, the importance of social distancing should be taught and managed.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgments
We thank all the professors who helped enrich the present material with their valuable comments.
References
- Ghannadi M, Mohebbi MR. [A 2006 survey of drinking water microbial quality in rural areas in Iran (limitations, challenges, and opportunities) (Persian)]. Journal of Water and Wastewater Ab va Fazilab. 2008; 19(1):23-9. [DOI:10.1353/imp.2008.0004]
- Benksim A, Addi RA, Cherkaoui M. Vulnerability and fragility expose older adults to the potential dangers of COVID-19 pandemic. Iranian Journal of Public Health. 2020; 49(Suppl 1):122. [DOI:10.18502/ijph.v49iS1.3682]
- Chen J. Rapid urbanization in China: A real challenge to soil protection and food security. Catena. 2007; 69(1):1-15. [DOI:10.1016/S0341-8162(01)00176-X]
- Noroozian M. The elderly population in iran: An ever growing concern in the health system. Iranian Journal of Psychiatry and Behavioral Sciences. 2012; 6(2):1-6. [PMID] [PMCID]
- Chen Y, Liu Q, Guo D. Emerging coronaviruses: Genome structure, replication, and pathogenesis [published correction appears in J Med Virol. 2020 Oct;92(10):2249]. Journal of Medical Virology. 2020; 92(4):418-23. [DOI:10.1002/jmv.25681] [PMID] [PMCID]
- Wang P, Lu J, Jin Y, Zhu M, Wang L, Chen S. Epidemiological characteristics of 1212 COVID-19 patients in Henan, China. medRxiv. Preprint Manuscript. 2020; 1-11. [DOI:10.1101/2020.02.21.20026112]
- Santesmasses D, Castro JP, Zenin AA, Shindyapina AV, Gerashchenko MV, Zhang B, et al. COVID‐19 is an emergent disease of aging. Aging Cell. 2020; 19(10):e13230. [DOI:10.1111/acel.13230] [PMID] [PMCID]
- Chen C, Chen C, Yan JT, Zhou N, Zhao JP, Wang DW. Analysis of myocardial injury and underlying cardiovascular diseases in critically ill patients with novel coronavirus pneumonia [J]. Chinese Journal of Cardiovascular Diseases (Zhonghua Xin Xue Guan Bing Za Zhi). 2020; 48(7):567-71. [DOI:10.3760/cma.j.cn112148-20200225-00123] [PMID]
- Hammami A, Harrabi B, Mohr M, Krustrup P. Physical activity and coronavirus disease 2019 (COVID-19): Specific recommendations for home-based physical training. Managing Sport and Leisure. 2020:1-6. [DOI:10.1080/23750472.2020.1757494]
- Rogers LC, Lavery LA, Joseph WS, Armstrong DG. All feet on deck-the role of podiatry during the COVID-19 pandemic: Preventing hospitalizations in an overburdened healthcare system, reducing amputation and death in people with diabetes. Journal of the American Podiatric Medical Association. 2020; 10.7547/20-051. [DOI:10.7547/20-051] [PMID]
- Corres IS, Rego FM, Canton EP. [8. Marcadors Immunològics (Catalan)]. Iniciativa ACCLC COVID-19. 2020; 1-6. [Link]
- Kim Y-J, Cho J-H. Correlation between preventive health behaviors and psycho-social health based on the leisure activities of South Koreans in the COVID-19 crisis. International Journal of Environmental Research and Public Health. 2020; 17(11):4066. [DOI:10.3390/ijerph17114066] [PMID] [PMCID]
- Nikolich-Zugich J, Knox KS, Rios CT, Natt B, Bhattacharya D, Fain MJ. SARS-CoV-2 and COVID-19 in older adults: What we may expect regarding pathogenesis, immune responses, and outcomes. Geroscience. 2020; 42(2):505-14. [DOI:10.1007/s11357-020-00186-0] [PMID] [PMCID]
- Petretto DR, Pili R. Ageing and COVID-19: What is the role for elderly people? Geriatrics. 2020; 5(2):25. Published 2020 Apr 26. [DOI:10.3390/geriatrics5020025] [PMID] [PMCID]
- Hase R, Kurita T, Muranaka E, Sasazawa H, Mito H, Yano Y. A case of imported COVID-19 diagnosed by PCR-positive lower respiratory specimen but with PCR-negative throat swabs. Infectious Diseases. 2020; 52(6):423-6. [DOI:10.1080/23744235.2020.1744711] [PMID] [PMCID]
- Verity R, Okell LC, Dorigatti I, Winskill P, Whittaker C, Imai N, et al. Estimates of the severity of coronavirus disease 2019: A model-based analysis. The Lancet Infectious Diseases. 2020; 20(6):669-77. [DOI:10.1016/S1473-3099(20)30243-7] [PMID]
- Moslehi S, Masoumi G, Rostamian M, Shirazi FB. Prevention, control and safety of health care providers during COVID-19: A review study. Research Square. 2020. Preprint (Version 1) available at: [DOI:10.21203/rs.3.rs-108680/v1]
- Santesmasses D, Castro J, Zenin A, Shindyapina A, Gerashchenko M, Zhang B, et al. COVID-19 is an emergent disease of aging. GERO Aging Therapeutics Project. 2020. [DOI:10.1111/acel.13230]
- He XW, Lai JS, Cheng J, Wang M, Liu Y, Xiao Z, et al. [Impact of complicated myocardial injury on the clinical outcome of severe or critically ill COVID-19 patients (Chinese)]. Zhonghua Xin Xue Guan Bing Za Zhi. 2020; 48(6):456-60. [DOI:10.3760/cma.j.cn112148-20200228-00137] [PMID]
- Kline KA, Bowdish DM. Infection in an aging population. Current Opinion in Microbiology. 2016; 29:63-7. [DOI:10.1016/j.mib.2015.11.003] [PMID]
- Meng H, Xu Y, Dai J, Zhang Y, Liu B, Yang H. Analyze the psychological impact of COVID-19 among the elderly population in China and make corresponding suggestions. Psychiatry Research. 2020; 289:112983. [DOI:10.1016/j.psychres.2020.112983] [PMID] [PMCID]
- Liu K, Zhang W, Yang Y, Zhang J, Li Y, Chen Y. Respiratory rehabilitation in elderly patients with COVID-19: A randomized controlled study. Complementary therapies in clinical practice. 2020; 39:101166. [DOI:10.1016/j.ctcp.2020.101166] [PMID] [PMCID]
- Riccioni L, Bertolini G, Giannini A, Vergano M, Gristina G, Livigni S, et al. Clinical ethics recommendations for the allocation of intensive care treatments, in exceptional, resource-limited circumstances. Recenti Progressi in Medicina. 2020; 111(4):207-11. [DOI:10.1701/3347.33183] [PMID]
- Son JS, Nimrod G, West ST, Janke MC, Liechty T, Naar JJ. Promoting older adults’ physical activity and social well-being during COVID-19. Leisure Sciences. 2021; 43(1-2):287-94. [DOI:10.1080/01490400.2020.1774015]
- Farnoosh G, Ghanei M, Khorramdelazad H, Alishiri G, Farahani AJ, Shahriary A, et al. Are Iranian sulfur mustard gas-exposed survivors more vulnerable to SARS-CoV-2? Some similarity in their pathogenesis. Disaster Medicine and Public Health Preparedness. 2020; 14(6):826-32. [DOI:10.1017/dmp.2020.156] [PMID] [PMCID]
- Özmete E, Pak M. The relationship between anxiety levels and perceived social support during the pandemic of COVID-19 in Turkey. Social Work in Public Health. 2020; 35(7):603-16. [DOI:10.1080/19371918.2020.1808144] [PMID]
- Hashemi Z, Eyni S. Perceived stress in the elderly: The role of spiritual intelligence, self-compassion, and psychological hardiness. Aging Psychology. 2020; 5(4):289-99. [Link]
- Larijani HA, Shirazi FB, Moslehi S. Responding to coronavirus (COVID-19) and providing reproductive health services in humanitarian settings. Journal of Disaster and Emergency Research. 2021. [Link]
- Nouri M, Ostadtaghizadeh A, Hosseinzadeh-Attar MJ, Fallah-Aliabadi S, Bagheri S, AlJasem M, et al. A systematic review of the nutritional consequences of the earthquake in East Azerbaijan earthquake, 2012. Journal of Nutrition, Fasting and Health. 2021. [Link]
- Cao B, Wang Y, Wen D, Liu W, Wang J, Fan G, et al. A trial of lopinavir-ritonavir in adults hospitalized with severe COVID-19. New England Journal of Medicine. 2020; 382(19):1-13. [Link]
- Jannat Alipoor Z, Fotokian Z. COVID-19 and the Elderly with Chronic diseases: Narrative Review. Journal of Military Medicine. 2020; 22(6):632-40. [Link]
- Li B, Yang J, Zhao F, Zhi L, Wang X, Liu L, et al. Prevalence and impact of cardiovascular metabolic diseases on COVID-19 in China. Clinical Research in Cardiology. 2020; 109(5):531-8. [DOI:10.1007/s00392-020-01626-9] [PMID] [PMCID]
- Guan W-j, Ni Z-y, Hu Y, Liang W-h, Ou C-q, He J-x, et al. Clinical characteristics of coronavirus disease 2019 in China. New England Journal of Medicine. 2020; 382(18):1708-20. [DOI:10.1056/NEJMoa2002032] [PMID] [PMCID]
- Singh AK, Gupta R, Ghosh A, Misra A. Diabetes in COVID-19: Prevalence, pathophysiology, prognosis and practical considerations. Diabetes & Metabolic Syndrome: Clinical Research & Reviews. 2020; 14(4):303-10. [DOI:10.1016/j.dsx.2020.04.004] [PMID] [PMCID]
Type of Study: Review |
Subject:
General
Received: 2021/10/7 | Accepted: 2022/03/8 | Published: 2023/01/1
Received: 2021/10/7 | Accepted: 2022/03/8 | Published: 2023/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Health in Emergencies and Disasters Quarterly
Health in Emergencies & Disasters Research Center, University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave, Tehran, Iran.
Journal Tel: +9821 71732816 (2816)
Publisher Tel: +9821 4535 5555 - 4535 5000
