

Volume 8 - Special Issue
Health in Emergencies and Disasters Quarterly 2023, 8 - Special Issue: 279-288 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mirshafiee R, Akbari Sari A, Delshad V, Sayadnasiri M, Kolivand P, Takian A H. Comparing the Effectiveness of Motor Ambulances in Pre-hospital Emergency Medical Services Compared to Ambulances in Tehran City, Iran. Health in Emergencies and Disasters Quarterly 2023; 8 :279-288
URL: http://hdq.uswr.ac.ir/article-1-420-en.html
URL: http://hdq.uswr.ac.ir/article-1-420-en.html
Roohollah Mirshafiee1 

 , Ali Akbari Sari1 , Vahid Delshad2 , Mohammad Sayadnasiri3 , PirHossein Kolivand4 , Amir Hosein Takian 5
, Ali Akbari Sari1 , Vahid Delshad2 , Mohammad Sayadnasiri3 , PirHossein Kolivand4 , Amir Hosein Takian 5
, Ali Akbari Sari1 , Vahid Delshad2 , Mohammad Sayadnasiri3 , PirHossein Kolivand4 , Amir Hosein Takian 5
1- Department of Health Management, Policy & Economics, School of Public Health, TUMS, Tehran, Iran.
2- Health in Emergency and Disaster Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- School of Behavioral Sciences and Mental Health, Psychosis Research Center, Rofeideh Rehabilitation Hospital, Razi Educational and Therapeutic Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
4- School of Medicine, Immunoregulation Research Center, Shahed University, Tehran, Iran.
5- Department of Health Management, Policy & Economics, School of Public Health, TUMS, Tehran, Iran. , takian@tums.ac.ir
2- Health in Emergency and Disaster Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- School of Behavioral Sciences and Mental Health, Psychosis Research Center, Rofeideh Rehabilitation Hospital, Razi Educational and Therapeutic Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
4- School of Medicine, Immunoregulation Research Center, Shahed University, Tehran, Iran.
5- Department of Health Management, Policy & Economics, School of Public Health, TUMS, Tehran, Iran. , takian@tums.ac.ir
Full-Text [PDF 492 kb]
(231 Downloads)
| Abstract (HTML) (1161 Views)
Full-Text: (88 Views)
1. Introduction
Emergency Medical Services (EMS) are one of the most basic health services that play a vital role in saving people’s lives and reducing mortality [1]. World Health Organization (WHO) regards EMS systems as an integral part of any effective and functional health care system [2]. Quick and urgent action before the hospital, such as decisive decisions and interventions, has a decisive role in the recovery of patients with severe injuries and illnesses. Pre-hospital EMS is not only limited to clinical care but also equipment, skills, and scene management [3].
The medical emergency system is at the forefront of the health system service providers and is currently considered one of the crucial functions of the health system. The demand from the emergency system is to deal with urgent cases which, if not dealt with in time, may lead to irreparable physical and brain injuries of the patients [4].
Pre-hospital EMS has an effective role in the survival and prevention of serious injuries to patients and injured. During the last decade, the need to transfer patients through this system has increased progressively in the world, for example, in the decade (2002-2012) in Asian and Pacific countries, the annual growth rate of telephone calls was 5%-10%, which is increasing. But for all these calls and transfers, the ambulance and EMS system are not needed, and a large percentage of the calls were non-emergency. A study conducted in the United Kingdom and the United States shows that between 30%-50% of the responses given by EMS were for non-emergencies and non-life-threatening conditions [5].
Immediate intervention in patients where time is vital is one of the characteristics of the emergency system [6]. Survival after major trauma is considered highly time-dependent, and the efficiency of prehospital emergency with rapid transfer to medical centers is considered normal [3]. On the other hand, urban traffic and the increase in urban population as well as the increase in demand for a pre-hospital emergency are one of the problems that the emergency system is facing [5].
Tehran EMS has 216 stations, most of which have an ambulance and a motor ambulance. Also, a limited number of bases have two ambulances and an ambulance bus, which are used in accidents with mass casualties where air transport is not possible. Also, if the transfer of the injured person is required to the medical centers by EMS, after coordinating with the hospital, the transfer will be done. During the COVID-19 epidemic, the number of emergency calls increased from 355241 to 1589346 (a 380% increase) and the number of missions increased from 82282 to 99926 (a 20% increase) [7]. Also, in 2019, 14000 trauma patients were transported by the emergency system, 197 of whom died, and the most services provided included airway management (87.3%) and serum therapy (12.2%) [8].
The pre-hospital emergency system in our country is doubly vital because traffic accidents are the first cause of diseases and injuries to both genders of all ages [9]. Studies have shown that annually 1.2 million people in the world die due to road accidents and between 20 and 50 million people are injured or disabled [10]. Statistics show that Iran ranks first in the world in terms of accidents [11]. Iran’s road accident statistics are twenty times higher than the global average.
According to statistics presented in Iran, one person dies every 19 minutes due to traffic accidents. On the other hand, 50% of deaths in traffic accidents happen in the first hour of the accident. The results of a study on emergency patients show that the most errors in preventable cases include delay in primary care, insufficient care in patient transfer, and inappropriate communication [12]. Currently, according to the law, the time for an ambulance to arrive at a patient’s bedside in cities should be less than eight minutes [13]. In big cities, due to heavy traffic, the time to reach the bedside is more than eight minutes, which causes the loss of golden time to save patients. Traffic causes long-term complications in sick patients depending on time or their mortality, and these risks are aggravated after unprincipled movements. Also, in overcrowding and destruction of roads, or remote, mountainous, and inaccessible areas, it is not possible to reach the injured by common vehicles, and it becomes difficult or impossible to transport the injured from the accident site to medical centers. In these cases, light vehicles are needed that can overcome the obstacles and bring the medical personnel to the injured bedside. One of the proposed solutions to overcome these obstacles is to use a motorcycle [5].
The emergency motorcycle is the best method for quick response to patients in cities and public places [14] which is an objective, measurable, and understandable criterion for the public and policy-makers [15].
The concept of using an emergency motorcycle is not new, and its use in medical treatment and transportation dates back to the early 1900s and prominently in World War I, but the use of motorcycles in the EMS began when cities like Singapore, London, and Hong Kong used it as the first responder in the emergency system. Due to the success of this plan, other big cities were encouraged to research and evaluate its effectiveness in their emergency system [14].
In a study conducted in Iran, the average Response Time (RT) for an ambulance and a motor ambulance was reported as 16 minutes, 14 minutes, and 13 s, respectively. Ambulance and motor ambulance missions are reported with a frequency of 20% for weakness and malaise and 16% for heart problems, respectively. In 57% of ambulance missions and 71.5% of motor ambulance missions, patients refused to come to the hospital, and most cases leading to transfer related to traffic accidents were reported at 24% [5]. According to the available reports, a large number of missions are completed due to a lack of cooperation to transfer to the local hospital [15]. In a study conducted in Iran, it was found that about 30% to 50% of emergency calls were not urgent and life-threatening, in addition, 50% of those transferred to the hospital were discharged without any intervention, and about 29% of patients with internal problems did not need an immediate transfer [5]. The presence of motor ambulances is considered a strong point in terms of reducing costs for the EMS and preparing the ambulance for the next and more necessary missions, as well as preventing overcrowding in the emergency department of hospitals. It seems that due to the lower cost of the missions EMS with a motor ambulance compared to an ambulance (including the cost of equipment and fewer personnel), it is possible to avoid the waste of resources in the mentioned cases to some extent [5].
The time to reach the scene, i.e. RT, has been mentioned as one of the critical factors in the emergency system, which the use of a motorcycle can significantly reduce [16].
Also, Haji Nabi’s study showed that district 15 of Tehran municipality ranks first with about 9.5% of traffic accidents, and 13.5% of traffic accident victims in this area die at the scene of the accident, followed by districts 11 and 5 of Tehran municipality. In terms of having the highest statistics of accidents and deaths of the injured, they are in the next ranks. In this study, it was announced that RT has a statistically significant relationship with the mortality rate [17].
The results of Delshad’s study showed that the highest number of traffic accidents and falls from heights occurred in the north of Tehran City, stabbing and CO2 poisoning in the east, and burns in the west of Tehran City. Also, the mentioned study is useful for the use of epidemiological information to design preparation programs for EMS workers and community members [18].
Considering the importance of effectiveness studies, this study aims to examine the effects of a motor ambulance in terms of consequences and determine its advantages and disadvantages and compare the two options of the motor ambulance with ambulance versus ambulance alone to choose the best option with the method of effectiveness studies.
2. Materials and Methods
This study is a descriptive-analytical cross-sectional research conducted in the fall of 2020 (because the available data was the same and according to the opinion of the research team of one season and the most up-to-date data at the time of the study) to determine the effectiveness of motor ambulance with the ambulance. The research environment in the present study is the Tehran emergency center. Considering the characteristics of Tehran City as the capital of the country and the most populated city with the highest number of accidents and missions, the Tehran emergency center was chosen as the research environment of this study. The tool for collecting information is a checklist made by the researcher, some of the information using data recorded in the standard forms of the Tehran emergency, which is completed by the technician and stored in the data bank of the Tehran emergency center. Also, part of the data was obtained through specialized meetings with experts and a review of documents.
According to the research team, the effectiveness criterion was death at the scene. Considering that in this study, the primary data on the effectiveness of these two interventions is mortality, and according to previous studies, the mortality data should be converted into the prevented mortality and enter the analysis phase. In this study, since the mortality index is expressed as a percentage, the difference in the mortality index from 100 was estimated as the preventable mortality index and entered into the analysis. Since a unique code is assigned to each mission in EMS, a separate code was not registered in the system for the missions that sent both the motor and the ambulance. For this purpose, to compare these cases via SPSS software (version 21) and by linking different variables such as name, time, and address, this work was done, and finally, the data were separated into 3 groups.
After preparing the data for statistical analysis, descriptive analysis was performed first. For this purpose, data and variables were described using indicators, such as minimum and maximum value, average, and standard deviation. Tables and Figures were also used for a better description. This article is extracted from the master’s thesis in the field of health economics with an ethics license obtained from the Ethics Committee of the Faculty of Health and Paramedicine of Tehran University of Medical Sciences under the ID IR.TUMS.SPH.REC.1399.135.
3. Results
The findings of the study based on epidemiological information are stated below.
Gender
In this study, to investigate missions related to traffic accidents and trauma, the Tehran emergency center was included in the study in 3 months. Finally, the data from 9160 ambulance missions, 4147 motor ambulance missions, and 2042 simultaneous motorcycle and ambulance missions were analyzed. In terms of gender distribution, 82.1%, 83.4%, and 83% of all ambulance, motor ambulance, and joint missions (motor and ambulance) were men, respectively. In other words, the percentage of motor ambulance missions for men was higher than the other two groups. Although, this difference was not statistically significant (P=0.151) (Table 1, 2, 3 and 4).


Age
The mean age of people in ambulance missions, motor ambulance, and joint missions (motor and ambulance) were 33.4 (SD=14.6), 34.4 (SD=15.2), and 34.7 (SD=15.7) years, respectively (Figure 1, 2, 3 and 4).
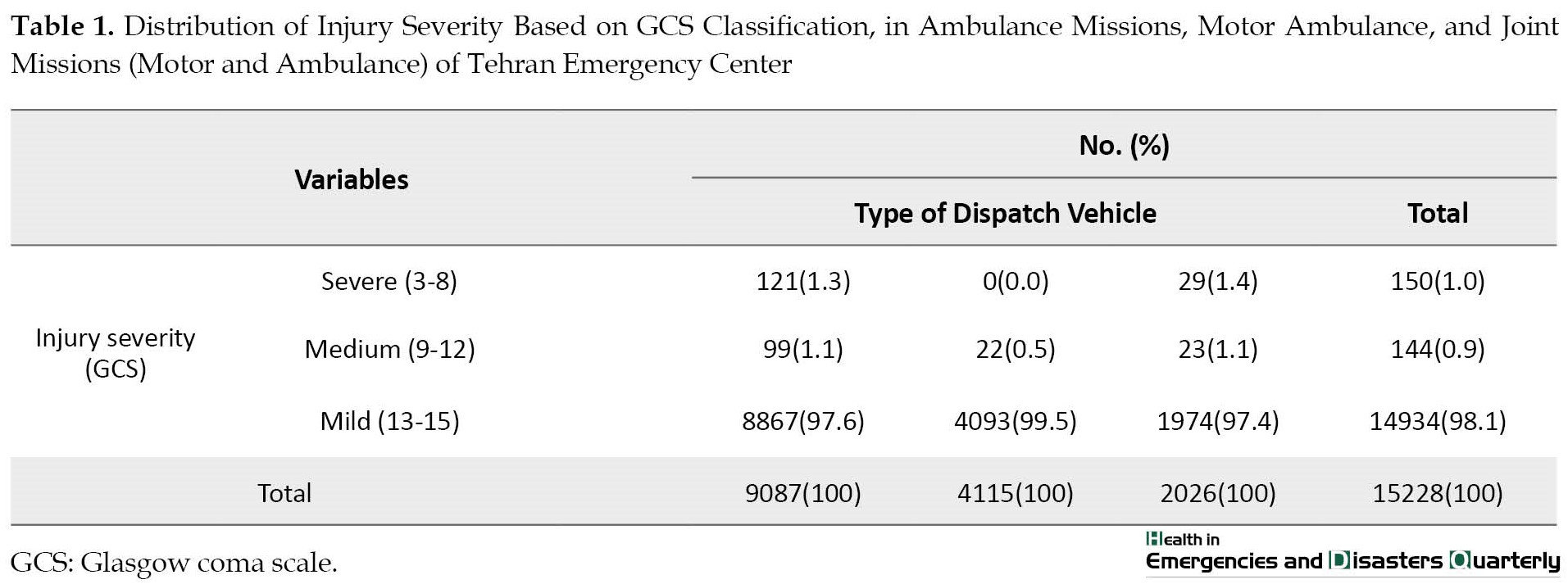
Distribution of Injury Severity Based on Glasgow Coma Scale (GCS) Classification
Based on the initial Glasgow Coma Scale (GCS), patients were divided into 3 groups, severe injury (GCS equal to 8 and less), moderate injury (GCS between 9 and 12), and mild injury (GCS equal to 13 to 15). Out of all the patients, 150 people (1%) had severe injuries and 0.9% and 98.1% of patients had moderate and mild injuries, respectively. In the group of patients who were sent by ambulance and motor at the same time, 1.4% had severe injuries, while this value was equal to zero and 1.3% for patients who were sent by motor ambulance and ambulance alone, respectively (Table 1). Statistically, a significant difference was observed between the severity of the injury and the means of dispatch (3 study groups) (P<0.001). Therefore, to eliminate the confounding effect of injury severity compared to outcomes in 3 study groups in terms of injury severity, and the outcomes studied separately, these classes were analyzed.
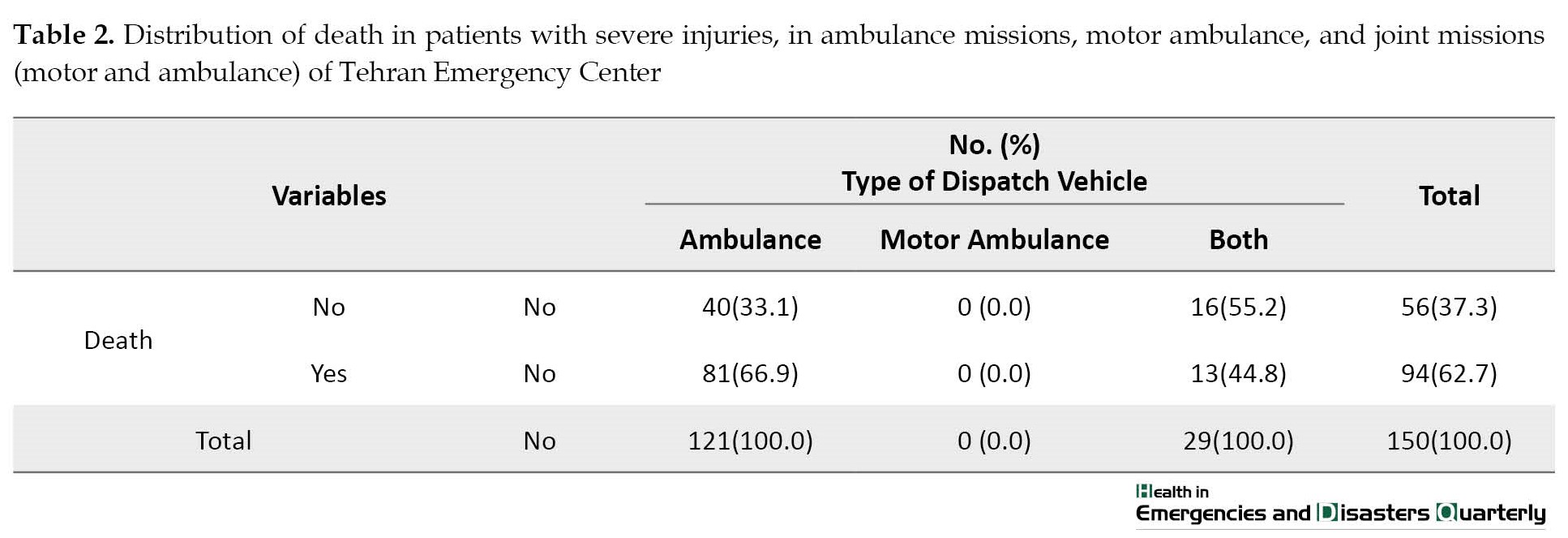
For none of the patients with severe injuries, the motor ambulance was dispatched alone. Death in patients with severe injuries in the ambulance group was more than the two groups of both dispatch vehicles (motor ambulance and ambulance). Totally, 66.9% of the patients in the ambulance group and 44.8% in the group of both devices had died, and this difference was statistically significant (P=0.027). In other words, in the group of patients with severe injuries, in cases where the motor was sent ahead of the ambulance or at the same time, compared to when the ambulance was sent alone, the death rate decreased (Table 2, 3 and 4).
Among patients with moderate and mild injury severity, a total of 15 deaths occurred among 15078 missions (9.9 deaths per 10 000 missions). In this group of patients, 13 cases of death occurred among the patients of the missions group of both dispatching vehicles and 2 cases of death occurred among the missions of the ambulance group. This difference was also statistically significant (P<0.001).
The Duration of Receiving the Mission Until Reaching the Emergency Response Time (RT)
The average duration of receiving the mission until reaching the emergency (RT) in motor ambulance missions was 9.12 minutes (SD=4.88) and this duration for ambulance missions was 12.94 minutes (SD=7.58). In the missions that were jointly dispatched by motor ambulance and ambulance, the average duration of receiving the mission to reach the emergency (RT) was 9.05 (SD=4.61) and 13.14 (SD=7.27) minutes, respectively. In other words, on average, the motor ambulance arrives at the emergency about 4 minutes earlier than the ambulance, and this difference was statistically significant (P<0.001).
Logistic Regression Results
Based on the results of univariate logistic regression for severe patients, although the chance of death was higher in female patients compared to male patients (OR=1.44), it was not statistically significant. Also, increasing age was a risk factor for death, although it was not statistically significant (P=0.200). On the other hand, changes in vital variables did not show a significant effect on the death of patients. Meanwhile, the chance of death in this group of patients (severe patients) was 2.49 times higher for cases where an ambulance was dispatched alone than when a motorcycle and an ambulance were dispatched.
In the multivariate analysis, after removing the confounding effect of age, the chance of death was 2.85 times higher for the cases in which the ambulance was sent alone than in the cases in which the motor and the ambulance were dispatched, and this relationship was also statistically significant (P=0.015). Therefore, dispatching a motor and an ambulance (both) in severe cases is a factor in preventing death. In other words, the chance of death for severe missions where the motor and ambulance (both) were dispatched is 0.351 times of the missions where the ambulance was dispatched alone.
4. Discussion
This study was conducted to investigate the effectiveness of a motor ambulance compared to an ambulance in the emergency department of Tehran in the fall of 2020.
The results indicate that in the first part of the study, by examining the outcome of death, the chance of death in the group of the motor ambulance with ambulance in severe level patients is 44.8% and in the group of ambulance alone is 66.9%. The probability of death in the two groups of the motor with ambulance and ambulance alone in mild and moderate patients is the opposite of severe patients. In the group of patients with mild and moderate injuries, the probability of death was estimated to be 0% in ambulance missions and 0.7% in the missions of the motor with an ambulance.
According to the results of the study, it was found that the use of a motor in Tehran’s EMS center reduces the RT in missions by 4 minutes, which is statistically and clinically significant. By examining the outcome of the study, which was death at the scene, it was found that the simultaneous dispatch of a motor and an ambulance led to a significant reduction in death from 66% to 44%. Previous studies consistent with our study show a reduction in RT using motors in missions. The results of the mentioned studies showed that the shortening of RT in the studies is different, and this difference can be due to the different traffic volumes in different countries and cities, as well as depending on the resources, existing infrastructure, and dispatch hours during the day and night in changing the effect of traffic. In some countries, emergency technicians with appropriate equipment are sent by motor ambulances as “pioneer” to the place of dispatch and provide medical measures. In the future, if more specialized services are needed, the necessary coordination for dispatching an ambulance will be done [5, 6, 19].
In the study of Soares-Oliveira et al, the number of 1972 phone calls to the emergency room was examined. The average time to reach the patient’s head was 4.4 ± 2.5 minutes. In 63% of cases, the motor ambulance arrived before other vehicles, and in 18% of cases, it was not required to transfer the patient to the hospital. As a result, in a wide range of clinical situations, the motor ambulance can intervene and guarantee a quick response. Additionally, in certain situations, motorcycles allow for better management of emergency vehicles safely and efficiently. This study suggests that the motorcycle be dispatched in these conditions, when the patient’s life is under serious threat and when the need for an ambulance is doubtful. Using the motor for two spectrums, with life-threatening conditions, makes life-saving interventions faster, and in mild cases with unknown conditions, it reduces the rate of transferring the patient to the hospital. In this study, it was found that for the injured with moderate injury, in some conditions and hours of the day and night, due to high demand for ambulances or heavy traffic, a motor ambulance was dispatched [19].
In 2019, Korakot Apiratwarakul et al., in a study conducted in Taiwan concluded that dispatching moor in emergency missions significantly reduces RT, and also the chance of survival significantly increases. The chance of survival in this study increased from 37.5% to 88% using motor dispatching as a pioneer, and the authors recommended the use of motor ambulance services in EMS services, especially in crowded cities [20].
In a study by van der Pols et al. which was conducted in the Netherlands, 1664 patients were investigated assisted by 468 operations by motorcycles and 1196 operations by ambulance. This study showed that the use of a motorcycle reduced the time to reach the patient by 54 s. The use of medical aid motorcycles in patients with milder emergency conditions reduced the rate of patient transfer to the hospital [21].
In a study conducted by Nakstad et al. in Norway, during a five-month research period on 703 medical aid motorcycles, it was found that the average driving time of the rescuers for the motorcycle is 30 s shorter than the ambulance car (6 minutes and 24 s versus 6 minutes and 54 s). Of course, this amount of time change has little importance clinically. In addition, when the need for a medical emergency and the condition of the patient is unknown, motorcycles have been used, which has reduced the unnecessary missions of the ambulance car. In this research, no motor ambulance accident was recorded. The lack of accidents may be due to extensive training for drivers and the fact that motorcycles only work during the day. The average total cost for each hour of working a motorcycle was about one-third of an ambulance. However, the ratio of benefit to real cost is smaller because the weather conditions make it impossible to use a motorcycle in winter [22].
In the current study, the ratio of profit and cost was not calculated per operating hour but per completed mission, which can have an impact on the results. Of course, due to the difference between the climate of Norway and Iran, the seasonal and weather restrictions for the hours of motor operation in Tehran are less.
In a study conducted by Kiefe et al., the safety level of using medical aid motorcycles was investigated. According to the results, if motorcycles are equipped with an acceptable safety level, they can provide quick and effective relief in urban areas. Motorcycle riding training courses along with proper use of personal protective equipment can increase safety [23].
The rate of accidents in motor units compared to the ambulance is another influencing factor in the cost-effectiveness of using a motorcycle, which was not investigated in our study.
In a study conducted by Ramesh A et al. in India, an innovative system using a paramedic/nurse on a motorcycle as a pioneer has been introduced to rapidly identify and treat patients with acute ST-elevation myocardial infarction (STEMI) and perform standard protocols for acute management of cardiovascular problems and ultimately improving patient survival. The authors believe that this model can be integrated with existing processes in large Indian cities [24].
The ambulance service center of the University of Medical Sciences Ljubljana launched the emergency motorcycle service in 200 to reduce the time to access the service and perform first aid before the ambulance arrives and improve the quality of service. Five years after launching this system, its cost-effectiveness was evaluated. The result of this evaluation determined that the average RT using a motorcycle was reduced by 50%, which resulted in a 5-minute shorter RT for out-of-hospital cardiac arrest cases, and their long-term survival rate in these cases increased from 12% to 21%. The improvement of life chance in cases where a motorcycle was dispatched to the scene as the first responder in an emergency is consistent with the findings of our study and has shown the effectiveness of using a motorcycle in emergency cases [25].
Another study in Slovenia showed that the average RT of a motor ambulance is about half compared to an ambulance. The authors believe that although the access time in the motorcycle has been greatly reduced, motorcycle paramedics are highly exposed to traffic hazards and weather conditions. Evaluations have shown that the introduction of motorcycle paramedics in this country is a wise decision and is currently an essential part of the emergency system, which can be a logical reason for using ambulances to reduce RT and subsequently reduce the death rate [26].
Korakot Apiratwarak et al. by examining the motor ambulance missions in Thailand during the COVID-19 pandemic showed that the average RT of motor ambulances during the pandemic was shorter compared to normal conditions [27].
Korakot Apiratwarak et al. in 2020 by examining the motor ambulance missions in Thailand during the Corona pandemic showed that the average RT of motor ambulances during the pandemic was shorter compared to normal conditions [28].
On the other hand, in the second group that had mild and moderate injuries, based on the results of the obtained statistics, it seems that the use of a motor ambulance is not effective considering the outcome of death for this group. In other words, we should consider that according to previous studies and guidelines in EMS, motor dispatch is preferably recommended for critical and mild cases, and motor dispatch is not indicated for this group [28]. However, in situations where it is not possible to dispatch an ambulance due to some reasons such as the lack of an ambulance and heavy traffic, the motor is inevitably used, and the motor units are a way out, not an additional option. Definitely, in the case of not dispatching the motor units, all of these missions will be for the ambulance, which can, in turn, affect the time the ambulance arrives at the scene and even the outcome of critically ill patients. Therefore, to properly investigate and analyze the effectiveness of this group, another study should be designed to examine the outcome of patients in a system that uses a motor unit with a system without this possibility. Also, in mild cases, the cost-effectiveness criterion should be evaluated with the rate of not transferring to the hospital and treating patients at the scene, which will save additional costs for unnecessary transfers.
One of the other causes of effectiveness for this group can be due to the nature of injury and trauma, which is known in most trauma studies as a time-dependent problem [4] that sometimes at the time of contact, the patient may not have life-threatening conditions and according to the dispatcher’s judgment, only a motor unit should be dispatched, but over time, the conditions of the injured person will progress to critical conditions and a faster transfer to the centers that have definitive services for trauma is needed. The delay in dispatching an ambulance that has the possibility of transferring the injured person will lead to worse outcomes and even death. Therefore, the necessity of proper triage and more training for the nurses of the dispatch unit is very crucial to decide on the type of dispatching vehicle, and the developed protocols should consider all the necessary criteria for proper identification of the injured and triage.
According to the results of the study regarding secondary outcomes, which included physiological variables, it was found that dispatching the motor and ambulance at the same time improved the blood pressure and heart rate of the patient compared to the ambulance alone, which can be due to the faster interventions of the motor regarding the bleeding control and shock management in trauma victims. On the other hand, the amount of SPO2 in the motor ambulance group has decreased compared to the ambulance alone, which requires further research to determine the cause. Shock and airway management requires the intervention of two technicians, while these actions are performed simultaneously by the motorcycle technician, and this issue can affect the quality and effectiveness of some services, which can be investigated by designing simulated studies or evaluating this case on a larger scale. One of the other reasons may be due to the nature of the injury, especially in severe head injuries and traumas, which lead to secondary hypoxia requiring definitive and faster care. Sometimes, the blood oxygen level may decrease with a delay in dispatching an ambulance and transfer. Therefore, it is essential to use expert and special forces with higher skills for airway management, as well as the need to carry out periodical training to manage trauma victims in the conditions of performing one-person missions for the personnel of motor units.
Of course, the critical point is that a large part of the prevented deaths may be due to other factors, especially the severity of the disease and trauma. For example, for very severe patients, the ambulance may have been dispatched alone from the beginning, while in some cases, the operator’s inference of the disease may be milder and has doubts about the severity of the accident, and first, the motor ambulance was dispatched, and after the severity of the accident was determined, the ambulance was dispatched. This causes the RT in the ambulance to be longer and the difference in deaths can be caused by it. However, it seems that even if 1 death of these 22 deaths is prevented due to the shorter RT (9.05 minutes), dispatching the motor with the ambulance is still effective.
It should also be considered that the present study was conducted in Tehran City, one of the metropolises in the world with very high traffic and its high dependence on dispatch time, and the number of motor units is more than 170 units, which can be claimed as one of the largest motor rescue fleets in the world. Tehran emergency motor ambulances play a vital role in providing services to patients and injured people and are like an ambulance equipped with necessary valuable medical equipment, such as telemedicine, oxygen, ventilator, AED, etc., and are dispatched with an expert technician as a leader or alone based on the nature of the problem and based on the emergency medical dispatchers. If higher levels of treatment and transfer to the hospital are needed, an ambulance will be dispatched, otherwise, the mission will be terminated at the site after initial interventions. The use of an ambulance motor is necessary and vital due to the increase in Tehran’s population, high and heavy traffic leading to an increase in RT, and also an increase in the demand for EMS [29].
5. Conclusion
According to the results of the study, it was found that the use of a motor in Tehran EMS reduces the RT in missions. Examining the outcome of the study, which was death at the scene, it was found that dispatching a motor and an ambulance at the same time led to a significant reduction in the chance of death. In examining the effectiveness of the motor for the groups with severe injuries, it was also shown that the use of the motor ambulance is effective compared to the ambulance alone. Although in the mild and moderate groups, the results were less effective in contrast to the severe patients, these values do not reflect the ineffectiveness of the motor ambulance and the negative impact on the intended outcome.
Finally, the results of the present study showed that according to the considered outcome (death), the use of motor ambulance with ambulance was effective in severe group patients. Of course, this outcome alone is not the basis of correct judgment, and outcomes such as survival, Disability-Adjusted Life Years (DALY), and Quality-Adjusted Life Years (QALY) seem necessary for a more accurate evaluation.
Limitations of the study
The impossibility of leveling patients based on the severity of trauma with a valid criterion such as macaque genotype and phenotype resource and inevitably using the GCS scale.
The research environment is limited to Tehran, which lowers the generalizability of the study.
The lack of a suitable standard data recording system and manual recording of some variables by technicians and dispatchers, has reduced the quality and uniformity of the data.
The multiplicity of ambulance and motor ambulance models and the impossibility of separation for cost calculations.
Given the limitations of the study, it is suggested that a clinical trial study should be conducted with the possibility of following up with the patients after the hospital which requires receiving data from the hospital’s information system during hospitalization and follow-up after discharge.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the TUMS (Code:IR.TUMS.SPH.REC.1399.135).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
References
Emergency Medical Services (EMS) are one of the most basic health services that play a vital role in saving people’s lives and reducing mortality [1]. World Health Organization (WHO) regards EMS systems as an integral part of any effective and functional health care system [2]. Quick and urgent action before the hospital, such as decisive decisions and interventions, has a decisive role in the recovery of patients with severe injuries and illnesses. Pre-hospital EMS is not only limited to clinical care but also equipment, skills, and scene management [3].
The medical emergency system is at the forefront of the health system service providers and is currently considered one of the crucial functions of the health system. The demand from the emergency system is to deal with urgent cases which, if not dealt with in time, may lead to irreparable physical and brain injuries of the patients [4].
Pre-hospital EMS has an effective role in the survival and prevention of serious injuries to patients and injured. During the last decade, the need to transfer patients through this system has increased progressively in the world, for example, in the decade (2002-2012) in Asian and Pacific countries, the annual growth rate of telephone calls was 5%-10%, which is increasing. But for all these calls and transfers, the ambulance and EMS system are not needed, and a large percentage of the calls were non-emergency. A study conducted in the United Kingdom and the United States shows that between 30%-50% of the responses given by EMS were for non-emergencies and non-life-threatening conditions [5].
Immediate intervention in patients where time is vital is one of the characteristics of the emergency system [6]. Survival after major trauma is considered highly time-dependent, and the efficiency of prehospital emergency with rapid transfer to medical centers is considered normal [3]. On the other hand, urban traffic and the increase in urban population as well as the increase in demand for a pre-hospital emergency are one of the problems that the emergency system is facing [5].
Tehran EMS has 216 stations, most of which have an ambulance and a motor ambulance. Also, a limited number of bases have two ambulances and an ambulance bus, which are used in accidents with mass casualties where air transport is not possible. Also, if the transfer of the injured person is required to the medical centers by EMS, after coordinating with the hospital, the transfer will be done. During the COVID-19 epidemic, the number of emergency calls increased from 355241 to 1589346 (a 380% increase) and the number of missions increased from 82282 to 99926 (a 20% increase) [7]. Also, in 2019, 14000 trauma patients were transported by the emergency system, 197 of whom died, and the most services provided included airway management (87.3%) and serum therapy (12.2%) [8].
The pre-hospital emergency system in our country is doubly vital because traffic accidents are the first cause of diseases and injuries to both genders of all ages [9]. Studies have shown that annually 1.2 million people in the world die due to road accidents and between 20 and 50 million people are injured or disabled [10]. Statistics show that Iran ranks first in the world in terms of accidents [11]. Iran’s road accident statistics are twenty times higher than the global average.
According to statistics presented in Iran, one person dies every 19 minutes due to traffic accidents. On the other hand, 50% of deaths in traffic accidents happen in the first hour of the accident. The results of a study on emergency patients show that the most errors in preventable cases include delay in primary care, insufficient care in patient transfer, and inappropriate communication [12]. Currently, according to the law, the time for an ambulance to arrive at a patient’s bedside in cities should be less than eight minutes [13]. In big cities, due to heavy traffic, the time to reach the bedside is more than eight minutes, which causes the loss of golden time to save patients. Traffic causes long-term complications in sick patients depending on time or their mortality, and these risks are aggravated after unprincipled movements. Also, in overcrowding and destruction of roads, or remote, mountainous, and inaccessible areas, it is not possible to reach the injured by common vehicles, and it becomes difficult or impossible to transport the injured from the accident site to medical centers. In these cases, light vehicles are needed that can overcome the obstacles and bring the medical personnel to the injured bedside. One of the proposed solutions to overcome these obstacles is to use a motorcycle [5].
The emergency motorcycle is the best method for quick response to patients in cities and public places [14] which is an objective, measurable, and understandable criterion for the public and policy-makers [15].
The concept of using an emergency motorcycle is not new, and its use in medical treatment and transportation dates back to the early 1900s and prominently in World War I, but the use of motorcycles in the EMS began when cities like Singapore, London, and Hong Kong used it as the first responder in the emergency system. Due to the success of this plan, other big cities were encouraged to research and evaluate its effectiveness in their emergency system [14].
In a study conducted in Iran, the average Response Time (RT) for an ambulance and a motor ambulance was reported as 16 minutes, 14 minutes, and 13 s, respectively. Ambulance and motor ambulance missions are reported with a frequency of 20% for weakness and malaise and 16% for heart problems, respectively. In 57% of ambulance missions and 71.5% of motor ambulance missions, patients refused to come to the hospital, and most cases leading to transfer related to traffic accidents were reported at 24% [5]. According to the available reports, a large number of missions are completed due to a lack of cooperation to transfer to the local hospital [15]. In a study conducted in Iran, it was found that about 30% to 50% of emergency calls were not urgent and life-threatening, in addition, 50% of those transferred to the hospital were discharged without any intervention, and about 29% of patients with internal problems did not need an immediate transfer [5]. The presence of motor ambulances is considered a strong point in terms of reducing costs for the EMS and preparing the ambulance for the next and more necessary missions, as well as preventing overcrowding in the emergency department of hospitals. It seems that due to the lower cost of the missions EMS with a motor ambulance compared to an ambulance (including the cost of equipment and fewer personnel), it is possible to avoid the waste of resources in the mentioned cases to some extent [5].
The time to reach the scene, i.e. RT, has been mentioned as one of the critical factors in the emergency system, which the use of a motorcycle can significantly reduce [16].
Also, Haji Nabi’s study showed that district 15 of Tehran municipality ranks first with about 9.5% of traffic accidents, and 13.5% of traffic accident victims in this area die at the scene of the accident, followed by districts 11 and 5 of Tehran municipality. In terms of having the highest statistics of accidents and deaths of the injured, they are in the next ranks. In this study, it was announced that RT has a statistically significant relationship with the mortality rate [17].
The results of Delshad’s study showed that the highest number of traffic accidents and falls from heights occurred in the north of Tehran City, stabbing and CO2 poisoning in the east, and burns in the west of Tehran City. Also, the mentioned study is useful for the use of epidemiological information to design preparation programs for EMS workers and community members [18].
Considering the importance of effectiveness studies, this study aims to examine the effects of a motor ambulance in terms of consequences and determine its advantages and disadvantages and compare the two options of the motor ambulance with ambulance versus ambulance alone to choose the best option with the method of effectiveness studies.
2. Materials and Methods
This study is a descriptive-analytical cross-sectional research conducted in the fall of 2020 (because the available data was the same and according to the opinion of the research team of one season and the most up-to-date data at the time of the study) to determine the effectiveness of motor ambulance with the ambulance. The research environment in the present study is the Tehran emergency center. Considering the characteristics of Tehran City as the capital of the country and the most populated city with the highest number of accidents and missions, the Tehran emergency center was chosen as the research environment of this study. The tool for collecting information is a checklist made by the researcher, some of the information using data recorded in the standard forms of the Tehran emergency, which is completed by the technician and stored in the data bank of the Tehran emergency center. Also, part of the data was obtained through specialized meetings with experts and a review of documents.
According to the research team, the effectiveness criterion was death at the scene. Considering that in this study, the primary data on the effectiveness of these two interventions is mortality, and according to previous studies, the mortality data should be converted into the prevented mortality and enter the analysis phase. In this study, since the mortality index is expressed as a percentage, the difference in the mortality index from 100 was estimated as the preventable mortality index and entered into the analysis. Since a unique code is assigned to each mission in EMS, a separate code was not registered in the system for the missions that sent both the motor and the ambulance. For this purpose, to compare these cases via SPSS software (version 21) and by linking different variables such as name, time, and address, this work was done, and finally, the data were separated into 3 groups.
After preparing the data for statistical analysis, descriptive analysis was performed first. For this purpose, data and variables were described using indicators, such as minimum and maximum value, average, and standard deviation. Tables and Figures were also used for a better description. This article is extracted from the master’s thesis in the field of health economics with an ethics license obtained from the Ethics Committee of the Faculty of Health and Paramedicine of Tehran University of Medical Sciences under the ID IR.TUMS.SPH.REC.1399.135.
3. Results
The findings of the study based on epidemiological information are stated below.
Gender
In this study, to investigate missions related to traffic accidents and trauma, the Tehran emergency center was included in the study in 3 months. Finally, the data from 9160 ambulance missions, 4147 motor ambulance missions, and 2042 simultaneous motorcycle and ambulance missions were analyzed. In terms of gender distribution, 82.1%, 83.4%, and 83% of all ambulance, motor ambulance, and joint missions (motor and ambulance) were men, respectively. In other words, the percentage of motor ambulance missions for men was higher than the other two groups. Although, this difference was not statistically significant (P=0.151) (Table 1, 2, 3 and 4).
Age
The mean age of people in ambulance missions, motor ambulance, and joint missions (motor and ambulance) were 33.4 (SD=14.6), 34.4 (SD=15.2), and 34.7 (SD=15.7) years, respectively (Figure 1, 2, 3 and 4).
Distribution of Injury Severity Based on Glasgow Coma Scale (GCS) Classification
Based on the initial Glasgow Coma Scale (GCS), patients were divided into 3 groups, severe injury (GCS equal to 8 and less), moderate injury (GCS between 9 and 12), and mild injury (GCS equal to 13 to 15). Out of all the patients, 150 people (1%) had severe injuries and 0.9% and 98.1% of patients had moderate and mild injuries, respectively. In the group of patients who were sent by ambulance and motor at the same time, 1.4% had severe injuries, while this value was equal to zero and 1.3% for patients who were sent by motor ambulance and ambulance alone, respectively (Table 1). Statistically, a significant difference was observed between the severity of the injury and the means of dispatch (3 study groups) (P<0.001). Therefore, to eliminate the confounding effect of injury severity compared to outcomes in 3 study groups in terms of injury severity, and the outcomes studied separately, these classes were analyzed.
For none of the patients with severe injuries, the motor ambulance was dispatched alone. Death in patients with severe injuries in the ambulance group was more than the two groups of both dispatch vehicles (motor ambulance and ambulance). Totally, 66.9% of the patients in the ambulance group and 44.8% in the group of both devices had died, and this difference was statistically significant (P=0.027). In other words, in the group of patients with severe injuries, in cases where the motor was sent ahead of the ambulance or at the same time, compared to when the ambulance was sent alone, the death rate decreased (Table 2, 3 and 4).
Among patients with moderate and mild injury severity, a total of 15 deaths occurred among 15078 missions (9.9 deaths per 10 000 missions). In this group of patients, 13 cases of death occurred among the patients of the missions group of both dispatching vehicles and 2 cases of death occurred among the missions of the ambulance group. This difference was also statistically significant (P<0.001).
The Duration of Receiving the Mission Until Reaching the Emergency Response Time (RT)
The average duration of receiving the mission until reaching the emergency (RT) in motor ambulance missions was 9.12 minutes (SD=4.88) and this duration for ambulance missions was 12.94 minutes (SD=7.58). In the missions that were jointly dispatched by motor ambulance and ambulance, the average duration of receiving the mission to reach the emergency (RT) was 9.05 (SD=4.61) and 13.14 (SD=7.27) minutes, respectively. In other words, on average, the motor ambulance arrives at the emergency about 4 minutes earlier than the ambulance, and this difference was statistically significant (P<0.001).
Logistic Regression Results
Based on the results of univariate logistic regression for severe patients, although the chance of death was higher in female patients compared to male patients (OR=1.44), it was not statistically significant. Also, increasing age was a risk factor for death, although it was not statistically significant (P=0.200). On the other hand, changes in vital variables did not show a significant effect on the death of patients. Meanwhile, the chance of death in this group of patients (severe patients) was 2.49 times higher for cases where an ambulance was dispatched alone than when a motorcycle and an ambulance were dispatched.
In the multivariate analysis, after removing the confounding effect of age, the chance of death was 2.85 times higher for the cases in which the ambulance was sent alone than in the cases in which the motor and the ambulance were dispatched, and this relationship was also statistically significant (P=0.015). Therefore, dispatching a motor and an ambulance (both) in severe cases is a factor in preventing death. In other words, the chance of death for severe missions where the motor and ambulance (both) were dispatched is 0.351 times of the missions where the ambulance was dispatched alone.
4. Discussion
This study was conducted to investigate the effectiveness of a motor ambulance compared to an ambulance in the emergency department of Tehran in the fall of 2020.
The results indicate that in the first part of the study, by examining the outcome of death, the chance of death in the group of the motor ambulance with ambulance in severe level patients is 44.8% and in the group of ambulance alone is 66.9%. The probability of death in the two groups of the motor with ambulance and ambulance alone in mild and moderate patients is the opposite of severe patients. In the group of patients with mild and moderate injuries, the probability of death was estimated to be 0% in ambulance missions and 0.7% in the missions of the motor with an ambulance.
According to the results of the study, it was found that the use of a motor in Tehran’s EMS center reduces the RT in missions by 4 minutes, which is statistically and clinically significant. By examining the outcome of the study, which was death at the scene, it was found that the simultaneous dispatch of a motor and an ambulance led to a significant reduction in death from 66% to 44%. Previous studies consistent with our study show a reduction in RT using motors in missions. The results of the mentioned studies showed that the shortening of RT in the studies is different, and this difference can be due to the different traffic volumes in different countries and cities, as well as depending on the resources, existing infrastructure, and dispatch hours during the day and night in changing the effect of traffic. In some countries, emergency technicians with appropriate equipment are sent by motor ambulances as “pioneer” to the place of dispatch and provide medical measures. In the future, if more specialized services are needed, the necessary coordination for dispatching an ambulance will be done [5, 6, 19].
In the study of Soares-Oliveira et al, the number of 1972 phone calls to the emergency room was examined. The average time to reach the patient’s head was 4.4 ± 2.5 minutes. In 63% of cases, the motor ambulance arrived before other vehicles, and in 18% of cases, it was not required to transfer the patient to the hospital. As a result, in a wide range of clinical situations, the motor ambulance can intervene and guarantee a quick response. Additionally, in certain situations, motorcycles allow for better management of emergency vehicles safely and efficiently. This study suggests that the motorcycle be dispatched in these conditions, when the patient’s life is under serious threat and when the need for an ambulance is doubtful. Using the motor for two spectrums, with life-threatening conditions, makes life-saving interventions faster, and in mild cases with unknown conditions, it reduces the rate of transferring the patient to the hospital. In this study, it was found that for the injured with moderate injury, in some conditions and hours of the day and night, due to high demand for ambulances or heavy traffic, a motor ambulance was dispatched [19].
In 2019, Korakot Apiratwarakul et al., in a study conducted in Taiwan concluded that dispatching moor in emergency missions significantly reduces RT, and also the chance of survival significantly increases. The chance of survival in this study increased from 37.5% to 88% using motor dispatching as a pioneer, and the authors recommended the use of motor ambulance services in EMS services, especially in crowded cities [20].
In a study by van der Pols et al. which was conducted in the Netherlands, 1664 patients were investigated assisted by 468 operations by motorcycles and 1196 operations by ambulance. This study showed that the use of a motorcycle reduced the time to reach the patient by 54 s. The use of medical aid motorcycles in patients with milder emergency conditions reduced the rate of patient transfer to the hospital [21].
In a study conducted by Nakstad et al. in Norway, during a five-month research period on 703 medical aid motorcycles, it was found that the average driving time of the rescuers for the motorcycle is 30 s shorter than the ambulance car (6 minutes and 24 s versus 6 minutes and 54 s). Of course, this amount of time change has little importance clinically. In addition, when the need for a medical emergency and the condition of the patient is unknown, motorcycles have been used, which has reduced the unnecessary missions of the ambulance car. In this research, no motor ambulance accident was recorded. The lack of accidents may be due to extensive training for drivers and the fact that motorcycles only work during the day. The average total cost for each hour of working a motorcycle was about one-third of an ambulance. However, the ratio of benefit to real cost is smaller because the weather conditions make it impossible to use a motorcycle in winter [22].
In the current study, the ratio of profit and cost was not calculated per operating hour but per completed mission, which can have an impact on the results. Of course, due to the difference between the climate of Norway and Iran, the seasonal and weather restrictions for the hours of motor operation in Tehran are less.
In a study conducted by Kiefe et al., the safety level of using medical aid motorcycles was investigated. According to the results, if motorcycles are equipped with an acceptable safety level, they can provide quick and effective relief in urban areas. Motorcycle riding training courses along with proper use of personal protective equipment can increase safety [23].
The rate of accidents in motor units compared to the ambulance is another influencing factor in the cost-effectiveness of using a motorcycle, which was not investigated in our study.
In a study conducted by Ramesh A et al. in India, an innovative system using a paramedic/nurse on a motorcycle as a pioneer has been introduced to rapidly identify and treat patients with acute ST-elevation myocardial infarction (STEMI) and perform standard protocols for acute management of cardiovascular problems and ultimately improving patient survival. The authors believe that this model can be integrated with existing processes in large Indian cities [24].
The ambulance service center of the University of Medical Sciences Ljubljana launched the emergency motorcycle service in 200 to reduce the time to access the service and perform first aid before the ambulance arrives and improve the quality of service. Five years after launching this system, its cost-effectiveness was evaluated. The result of this evaluation determined that the average RT using a motorcycle was reduced by 50%, which resulted in a 5-minute shorter RT for out-of-hospital cardiac arrest cases, and their long-term survival rate in these cases increased from 12% to 21%. The improvement of life chance in cases where a motorcycle was dispatched to the scene as the first responder in an emergency is consistent with the findings of our study and has shown the effectiveness of using a motorcycle in emergency cases [25].
Another study in Slovenia showed that the average RT of a motor ambulance is about half compared to an ambulance. The authors believe that although the access time in the motorcycle has been greatly reduced, motorcycle paramedics are highly exposed to traffic hazards and weather conditions. Evaluations have shown that the introduction of motorcycle paramedics in this country is a wise decision and is currently an essential part of the emergency system, which can be a logical reason for using ambulances to reduce RT and subsequently reduce the death rate [26].
Korakot Apiratwarak et al. by examining the motor ambulance missions in Thailand during the COVID-19 pandemic showed that the average RT of motor ambulances during the pandemic was shorter compared to normal conditions [27].
Korakot Apiratwarak et al. in 2020 by examining the motor ambulance missions in Thailand during the Corona pandemic showed that the average RT of motor ambulances during the pandemic was shorter compared to normal conditions [28].
On the other hand, in the second group that had mild and moderate injuries, based on the results of the obtained statistics, it seems that the use of a motor ambulance is not effective considering the outcome of death for this group. In other words, we should consider that according to previous studies and guidelines in EMS, motor dispatch is preferably recommended for critical and mild cases, and motor dispatch is not indicated for this group [28]. However, in situations where it is not possible to dispatch an ambulance due to some reasons such as the lack of an ambulance and heavy traffic, the motor is inevitably used, and the motor units are a way out, not an additional option. Definitely, in the case of not dispatching the motor units, all of these missions will be for the ambulance, which can, in turn, affect the time the ambulance arrives at the scene and even the outcome of critically ill patients. Therefore, to properly investigate and analyze the effectiveness of this group, another study should be designed to examine the outcome of patients in a system that uses a motor unit with a system without this possibility. Also, in mild cases, the cost-effectiveness criterion should be evaluated with the rate of not transferring to the hospital and treating patients at the scene, which will save additional costs for unnecessary transfers.
One of the other causes of effectiveness for this group can be due to the nature of injury and trauma, which is known in most trauma studies as a time-dependent problem [4] that sometimes at the time of contact, the patient may not have life-threatening conditions and according to the dispatcher’s judgment, only a motor unit should be dispatched, but over time, the conditions of the injured person will progress to critical conditions and a faster transfer to the centers that have definitive services for trauma is needed. The delay in dispatching an ambulance that has the possibility of transferring the injured person will lead to worse outcomes and even death. Therefore, the necessity of proper triage and more training for the nurses of the dispatch unit is very crucial to decide on the type of dispatching vehicle, and the developed protocols should consider all the necessary criteria for proper identification of the injured and triage.
According to the results of the study regarding secondary outcomes, which included physiological variables, it was found that dispatching the motor and ambulance at the same time improved the blood pressure and heart rate of the patient compared to the ambulance alone, which can be due to the faster interventions of the motor regarding the bleeding control and shock management in trauma victims. On the other hand, the amount of SPO2 in the motor ambulance group has decreased compared to the ambulance alone, which requires further research to determine the cause. Shock and airway management requires the intervention of two technicians, while these actions are performed simultaneously by the motorcycle technician, and this issue can affect the quality and effectiveness of some services, which can be investigated by designing simulated studies or evaluating this case on a larger scale. One of the other reasons may be due to the nature of the injury, especially in severe head injuries and traumas, which lead to secondary hypoxia requiring definitive and faster care. Sometimes, the blood oxygen level may decrease with a delay in dispatching an ambulance and transfer. Therefore, it is essential to use expert and special forces with higher skills for airway management, as well as the need to carry out periodical training to manage trauma victims in the conditions of performing one-person missions for the personnel of motor units.
Of course, the critical point is that a large part of the prevented deaths may be due to other factors, especially the severity of the disease and trauma. For example, for very severe patients, the ambulance may have been dispatched alone from the beginning, while in some cases, the operator’s inference of the disease may be milder and has doubts about the severity of the accident, and first, the motor ambulance was dispatched, and after the severity of the accident was determined, the ambulance was dispatched. This causes the RT in the ambulance to be longer and the difference in deaths can be caused by it. However, it seems that even if 1 death of these 22 deaths is prevented due to the shorter RT (9.05 minutes), dispatching the motor with the ambulance is still effective.
It should also be considered that the present study was conducted in Tehran City, one of the metropolises in the world with very high traffic and its high dependence on dispatch time, and the number of motor units is more than 170 units, which can be claimed as one of the largest motor rescue fleets in the world. Tehran emergency motor ambulances play a vital role in providing services to patients and injured people and are like an ambulance equipped with necessary valuable medical equipment, such as telemedicine, oxygen, ventilator, AED, etc., and are dispatched with an expert technician as a leader or alone based on the nature of the problem and based on the emergency medical dispatchers. If higher levels of treatment and transfer to the hospital are needed, an ambulance will be dispatched, otherwise, the mission will be terminated at the site after initial interventions. The use of an ambulance motor is necessary and vital due to the increase in Tehran’s population, high and heavy traffic leading to an increase in RT, and also an increase in the demand for EMS [29].
5. Conclusion
According to the results of the study, it was found that the use of a motor in Tehran EMS reduces the RT in missions. Examining the outcome of the study, which was death at the scene, it was found that dispatching a motor and an ambulance at the same time led to a significant reduction in the chance of death. In examining the effectiveness of the motor for the groups with severe injuries, it was also shown that the use of the motor ambulance is effective compared to the ambulance alone. Although in the mild and moderate groups, the results were less effective in contrast to the severe patients, these values do not reflect the ineffectiveness of the motor ambulance and the negative impact on the intended outcome.
Finally, the results of the present study showed that according to the considered outcome (death), the use of motor ambulance with ambulance was effective in severe group patients. Of course, this outcome alone is not the basis of correct judgment, and outcomes such as survival, Disability-Adjusted Life Years (DALY), and Quality-Adjusted Life Years (QALY) seem necessary for a more accurate evaluation.
Limitations of the study
The impossibility of leveling patients based on the severity of trauma with a valid criterion such as macaque genotype and phenotype resource and inevitably using the GCS scale.
The research environment is limited to Tehran, which lowers the generalizability of the study.
The lack of a suitable standard data recording system and manual recording of some variables by technicians and dispatchers, has reduced the quality and uniformity of the data.
The multiplicity of ambulance and motor ambulance models and the impossibility of separation for cost calculations.
Given the limitations of the study, it is suggested that a clinical trial study should be conducted with the possibility of following up with the patients after the hospital which requires receiving data from the hospital’s information system during hospitalization and follow-up after discharge.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the TUMS (Code:IR.TUMS.SPH.REC.1399.135).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
References
- Aringhieri R, Bruni ME, Khodaparasti S, van Essen JT. Emergency medical services and beyond: Addressing new challenges through a wide literature review. Computers & Operations Research. 2017; 78:349-68. [DOI:10.1016/j.cor.2016.09.016]
- Al-Shaqsi S. Models of international emergency medical service (EMS) systems. Oman medical journal. 2010; 25(4):320-23. [Link]
- Wilson MH, Habig K, Wright C, Hughes A, Davies G, Imray CHE. Pre-hospital emergency medicine. Lancet. 2015; 386(10012):2526-34. [DOI:10.1016/S0140-6736(15)00985-X] [PMID]
- Delshad V, Shemshadi H, Moradian MJ, Ahmadi S, Malkyan L, Sabzalizadeh S. The effect of applying global positioning system in ambulances on response time of Tehran Emergency Medical Service. Heal Emergencies Disasters Q. 2016;1(3):125-8. [DOI:10.15412/J.HDQ.09010302]
- Jafari M, Shakeri K, Mahmoudian P, Bathaei SA. Innovation in the use of motor ambulance for prehospital emergency care. Journal of Education and Health Promotion. 2019; 8. [DOI:10.4103/jehp.jehp_249_18]
- Lin CS, Chang H, Shyu KG, Liu CY, Lin CC, Hung CR, Chen PH. A method to reduce response times in prehospital care: the motorcycle experience. The American Journal of Emergency Medicine. 1998; 16(7):711-3. [DOI:10.1016/S0735-6757(98)90185-1] [PMID]
- Saberian P, Conovaloff JL, Vahidi E, Hasani-Sharamin P, Kolivand PH. How the COVID-19 epidemic affected prehospital emergency medical services in Tehran, Iran. Western Journal of Emergency Medicine. 2020; 21(6):110-6. [DOI:10.5811/westjem.2020.8.48679] [PMID] [PMCID]
- Kolivand PH, Mahshidfar B, Saberian P, Tavakoli N, Hasani-Sharamin P, Abdollahi A. Audit on in-hospital mortality of trauma patients: EMS Management and Mismanagement. Trauma Monthly. 2020; 25(5):200-6. [Link]
- Akbari ME, Naghavi M, Soori H. Epidemiology of deaths from injuries in the Islamic Republic of Iran. EMHJ-Eastern Mediterranean Health Journal. 2006;12(3-4):382-90. [Link]
- Naghavi M, Jafar N, Alaeddini F, Akbari M. Epidemiology of external causes of injuries in IR Iran. Tehran, Iran: Ministry of Health And Medical Education; 2004. [Link]
- Sankaran-Kutty M, Bener A, Muralikuttan KP, Sebastian M. Road traffic accident admissions in the United Arab Emirates. Annals of Saudi Medicine. 1998; 18(4):349-51. [DOI:10.5144/0256-4947.1998.349] [PMID]
- Bahadori MK. Prioritization of determinants influencing preparedness of Iranian Pre-hospital Emergency Services. 2011. [Link]
- Pons PT, Haukoos JS, Bludworth W, Cribley T, Pons KA, Markovchick VJ. Paramedic response time: does it affect patient survival? Annals of Saudi Medicine. 2005; 12(7):594-600. [DOI:10.1197/j.aem.2005.02.013] [PMID]
- Maslanka M. Rescue on two wheels. Journal of Emergency Nursing. 2014; 40(3):276-8. [DOI:10.1016/j.jen.2014.02.008] [PMID]
- Al-Shaqsi SZ. Response time as a sole performance indicator in EMS: Pitfalls and solutions. Open access emergency medicine: OAEM. 2010; 2:1. [DOI:10.2147/OAEM.S8510] [PMID]
- Peyravi MR, Toubaei F, Pourmohammadi K. The efficiency of motorlance in comparison with ambulance in Shiraz, southern Iran. Iranian Red Crescent Medical Journal. 2009; 11(3):330-3. [Link]
- Hajinabi K, Riahi L, Gholipour Varki H. The relationship between prehospital time indices and on-scene death rate in traffic accidents in the 22 regions of Tehran. Health Information Management. 2014; 11(3):353-61. [Link]
- Delshad V, Sabzalizadeh S, Moradian MJ, Safarpour H, Malekyan L, Shemshadi H, et al. Epidemiology of accidents in Tehran emergency medical service during 2012 to 2013. Trauma Monthly. 2018; 23(1). [DOI:10.5812/traumamon.61871]
- Soares-Oliveira M, Egipto P, Costa I, Cunha-Ribeiro LM. Emergency motorcycle: has it a place in a medical emergency system? American Journal of Emergency Medicine. 2007; 25(6):620-2. [DOI:10.1016/j.ajem.2006.11.030] [PMID]
- Apiratwarakul K, Ienghong K, Mitsungnern T, Kotruchin P, Phungoen P, Bhudhisawasdi V. Use of a motorlance to deliver emergency medical services; a prospective cross sectional study. Archives of Academic Emergency Medicine. 2019; 7(1):e48. [PMCID] [PMID]
- Van Der Pols H, Mencl F, De Vos R. The impact of an emergency motorcycle response vehicle on prehospital care in an urban area. European Journal of Emergency Medicine. 2011; 18(6):328-33. [DOI:10.1097/MEJ.0b013e32834624e8] [PMID]
- Nakstad AR, Bjelland B, Sandberg M. Medical emergency motorcycle-is it useful in a Scandinavian Emergency Medical Service? Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine. 2009; 17(1):1-4. [DOI:10.1186/1757-7241-17-9] [PMID] [PMCID]
- Kiefe CC, Soares-Oliveira M. Medical emergency motorcycles: are they safe? European Journal of Emergency Medicine. 2008; 15(1):40-2. [DOI:10.1097/MEJ.0b013e3282861d2f] [PMID]
- Ramesh A, Vanden Hoek TL, LaBresh K, Campbell T, Murthy K, Shetty N. Development of an emergency nurse-paramedic motorcycle response system for acute STEMI and sudden cardiac arrest care in India. Glob J Emerg Med. 2018; 1(2):1008. [Link]
- Fink A, Andoljšek D. 143: Cost-benefit of medical emergency motorcycle system. Annals of Emergency Medicine. 2008; 51(4):514-5. [DOI:10.1016/j.annemergmed.2008.01.111]
- Ho AFW, Chew D, Wong TH, Ng YY, Pek PP, Lim SH, et al. Prehospital trauma care in Singapore. Prehospital Emerg care. 2015; 19(3):409-15. [DOI:10.3109/10903127.2014.980477] [PMID]
- Apiratwarakul K, Ienghong K, Bhudhisawasdi V, Gaysonsiri D, Tiamkao S. Response Times of Motorcycle Ambulances during the COVID-19 Pandemic. Open Access Macedonian Journal of Medical Sciences. 2020; 8(T1):526-9. [DOI:10.3889/oamjms.2020.5527]
- Mehshidfar B, Hosni Shramin P. [Step-by-step in communication and dispatch of pre-hospital emergencies (Persian)]. Tehran: Sepid Berg, Emergency Organization of the country, Yek-Panj; 2018. [Link]
- Saberian P, Sharamin PH, Dadashi F. Emergency medical service concepts in Tehran, Iran. Journal of Orthopedic and Spine Trauma. 2017. [DOI:10.5812/jost.80778]
Type of Study: Applicable |
Subject:
Special
Received: 2022/02/28 | Accepted: 2022/05/29 | Published: 2023/04/18
Received: 2022/02/28 | Accepted: 2022/05/29 | Published: 2023/04/18
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Health in Emergencies and Disasters Quarterly
Health in Emergencies & Disasters Research Center, University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave, Tehran, Iran.
Journal Tel: +9821 71732816 (2816)
Publisher Tel: +9821 4535 5555 - 4535 5000
