

Volume 8, Issue 4 (Summer 2023)
Health in Emergencies and Disasters Quarterly 2023, 8(4): 301-312 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Badparva B, Maroufizadeh S, Eslami-Kenarsari H, Abdollahi S, Babakian P, Sayyad S et al . Nurses’ Perspectives on Nursing Management Performance in the COVID-19 Pandemic in Iran: A Cross-sectional Study. Health in Emergencies and Disasters Quarterly 2023; 8 (4) :301-312
URL: http://hdq.uswr.ac.ir/article-1-454-en.html
URL: http://hdq.uswr.ac.ir/article-1-454-en.html
Bita Badparva1 

 , Saman Maroufizadeh2 , Habib Eslami-Kenarsari3 , Sedigheh Abdollahi3 , Parvaneh Babakian3 , Shirin Sayyad3 , Negar Pourvakhshoori *4
, Saman Maroufizadeh2 , Habib Eslami-Kenarsari3 , Sedigheh Abdollahi3 , Parvaneh Babakian3 , Shirin Sayyad3 , Negar Pourvakhshoori *4
, Saman Maroufizadeh2 , Habib Eslami-Kenarsari3 , Sedigheh Abdollahi3 , Parvaneh Babakian3 , Shirin Sayyad3 , Negar Pourvakhshoori *4
1- Department of Internal Medicine, Inflammatory Lung Diseases Research Center, School of Medicine, Razi Hospital, Guilan University of Medical Sciences, Rasht, Iran., Nursing and Midwifery School of Shahid Dr. Beheshti, Hamidyan Shahrak, Shahid Dr. Beheshti Ave., Rasht, Guilan, IRAN
2- Department of Biostatistics, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran., Nursing and Midwifery School of Shahid Dr. Beheshti, Hamidyan Shahrak, Shahid Dr. Beheshti Ave., Rasht, Guilan, IRAN
3- Department of Internal Medicine, Inflammatory Lung Diseases Research Center, School of Medicine, Razi Hospital, Guilan University of Medical Sciences, Rasht, Iran., Inflammatory Lung Diseases Research Center, Department of Internal Medicine, Razi Hospital, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran
4- Department of Internal Medicine, Inflammatory Lung Diseases Research Center, School of Medicine, Razi Hospital, Guilan University of Medical Sciences, Rasht, Iran. ,nvakhshoori@gmail.com
2- Department of Biostatistics, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran., Nursing and Midwifery School of Shahid Dr. Beheshti, Hamidyan Shahrak, Shahid Dr. Beheshti Ave., Rasht, Guilan, IRAN
3- Department of Internal Medicine, Inflammatory Lung Diseases Research Center, School of Medicine, Razi Hospital, Guilan University of Medical Sciences, Rasht, Iran., Inflammatory Lung Diseases Research Center, Department of Internal Medicine, Razi Hospital, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran
4- Department of Internal Medicine, Inflammatory Lung Diseases Research Center, School of Medicine, Razi Hospital, Guilan University of Medical Sciences, Rasht, Iran. ,
Full-Text [PDF 524 kb]
(1185 Downloads)
| Abstract (HTML) (2979 Views)
Full-Text: (849 Views)
1. Introduction
Nurses are one of the main groups of health experts responsible for confronting and taking care of people when disasters happen [1]. Nurses play an important role during the COVID-19 pandemic like any other disaster. Taking care of patients has been challenging during disasters and had its special conditions, so taking care of patients suffering from COVID-19 is the same. In recent pandemic conditions, intensive care is taken in isolated units. Therefore, nurses will have to cope with the expanding workload and more different rotating shifts. One of the most important factors at this time is the nursing shortage. Therefore, it is necessary to consider the necessary arrangements like scheduling the rotating shifts well and effectively using human resources [2]. Nurses have been playing important roles in preventing and controlling infections and generally improving public health as was first raised by Florence Nightingale [3]. The conditions of disasters are very important and unique and need these special preparations and skills [4]. Providing healthcare during the COVID-19 pandemic is a unique condition, so it is important to know about its special features. Studies done at the time of the pandemic show that nurses experience conditions similar to those of previous pandemics. They have been worried about the health and safety of their families and themselves and needed to have connections with their families and the nursing team members. Since there are no certain treatments and effective antivirus medicine for the disease, managing patients suffering from COVID-19 has become a great problem in the work which is believed not to have an end. Moreover, managing these patients burdens healthcare providers, especially nurses, with difficulty or hard work. Currently, COVID-19 has caused anxiety in the public health and treatment community. That is why this virus is spreading all over the world and sharing a burden on low-income and developing countries [5, 6]. The COVID-19 pandemic is a major threat to public health all over the world. Therefore, a coordinated universal reaction is needed to prepare healthcare systems and confront this unprecedented challenge. Sound management of human resources can increase the efficiency and quality of the nurses’ care [7].
The COVID-19 pandemic has created fast changes in the structures of hospitals. Nurses of the ICU who take care of patients suffering from serious illnesses experience new challenges by delivering services in new units called the COVID-19 ICUs. The increased number of COVID-19 patients and the respiratory systems made the managers of the ICUs in Italy change the recovery and surgery units into COVID-19 ones because of the lack of empty beds in ICUs. The increase of patients with serious illnesses means sudden organizational changes which have been made by the hospital managers to make human resources give a quick response to the unprecedented disaster in delivering health care services. These conditions have provoked challenges and new opportunities for nursing management which are remarkable [8]. Nurses have faced a lot of challenges during the COVID-19 pandemic such as difficult and long-term shifts, and long-term uses of personal and protective supplies such as N95 masks which can cause skin disorders, an increase in burnout, dehydration, and an increase in medical errors. Therefore, managing these great challenges during the pandemic needs appropriate decisions at the level of management which make the nursing managers’ roles prominent [9]. Nurses have actively been doing their jobs of controlling infections and taking special care of patients at the forefront since the beginning of the pandemic [10].
During the current pandemic, attention has been drawn to nurses working in the ICUs, and their important roles in taking long-term care of patients have been highlighted in recent months [11]. At the time confronting stressful conditions like the COVID-19 pandemic, it is so important for nursing managers to have enough capabilities to support in a good and appropriate way to come up against the hard days [12]. Nursing managers can be effective in the pandemic by identifying and improving appropriate strategies for taking care of patients suffering from COVID-19 [7]. Generally, in the studies, nurses reported their experience in seeing the patients’ agony and death. Moreover, the nursing managers enumerated extra responsibilities in managing human resources and supplies as their challenges during the pandemic [13-15]. The determined main strategies by World Health Organization (WHO) are as follows: Stopping the disease to be transmitted, recognizing, separating, and taking care of patients suffering from the virus, accelerating recognition, curing and vaccinating, performing activities about giving awareness to society and minimizing social and economic effects of the pandemic [1]. Nurses use their knowledge and skills to take the necessary care of patients at all levels of sickness to satisfy these approaches although there is a lack of the necessary supplies such as protective personal supplies with high quality. Society especially guides the most susceptible people and works considering the safety of the patients and the treatment team by following innovative strategies. Therefore, they face challenges that eventually make them stronger and learn valuable skills compared to the times when the pandemic has not started yet [16]. One of the ways to confront the COVID-19 pandemic is by increasing resilience which can give nursing managers a wider perspective on avoiding, preparing for, and answering the disaster [17]. The paradigm of resilience consists of seven main units including management commitments at senior levels, the culture of fallibility, the culture of learning, awareness, preparation, and transparency. Generally, resilience can prevent probable failures and losses in a disaster and the capability to give appropriate responses after a disaster [18]. Nursing managers are faced with a lot of daily challenges which need flexibility and great skills. The COVID-19 pandemic has put nursing managers under unprecedented pressure to make them update the resources, the staff, and the controlling infection strategies and revive connections with multidisciplinary teams. At the peak of the COVID-19 pandemic in the summer of 2020, a group of nursing managers dealt with producing resilience in the health system in the east of the Middle East to improve the emotional comfort and equilibrium between work and life to optimize and improve their management [19].
Most of the studies are about the resilience in the health care systems such as NHS based on the organizational disaster such as a lack of nurses, an increase in the workforce, and financial limitations. However, the nursing system can learn from the past to consider more stamina. Why resilience is important returns to the issue that when a saddening event such as the pandemic happens, resilience gives us the capability to resist the disorders with our natural performances by anticipating and preparing ourselves for the event. Also, we can have positive results such as a decrease in burnout and an increase in confrontational behavior by improving resilience strategies [16, 20]. The nursing managers’ decisions to manage the pandemic are important and should be made quickly and without wasting time. The performance referring to nursing managers’ appropriate decisions lead to better management during the COVID-19 pandemic. Therefore, the present study has been done to evaluate the nurse managers’ performance based on resilience during the COVID-19 pandemic from the nurses’ perspectives regarding the importance of this problem to take the necessary actions to improve the quality of the management and the nursing services by surveying the current conditions.
2. Materials and Methods
One hundred eighty-nine Iranian nurses working in the Corona center hospital in Guilan province participated in this cross-sectional study. This hospital is the main center of curing COVID-19 patients. Nurses who had at least one month experience of taking care of patients suffering from COVID-19 and were willing to participate in this study were considered. The data were collected by using a questionnaire consisting of demographic features and disaster-managing surveys based on seven engineering approaches at the hospitals by the enumeration sampling from June to October 2021. The first part of the questionnaire consisted of some information such as age, sex, level of education, experience in clinical work, and type of employment. The second part consisted of the survey of disaster management based on seven engineering resilience principles at hospitals which have been designed by Azadian et al. [21] and its validity and stability have been verified (Cronbach’s α 0.977 and the intragroup correlation coefficient 0.97). This questionnaire consisted of forty-four questions and seven subscales: Management commitment (9 questions), the culture of fallibility (6 questions), the culture of learning (4 questions), awareness (5 questions), preparation (3 questions), flexibility (5 questions), and transparency (2 questions). Senior management shows a commitment to recognizing the factors related to human performance. The management tries to recognize the human performances which lead to making errors and make the organization pay attention to the errors. Because at the time a disaster happens and the number of people going to hospitals increases, every single error which could be ignored in daily performances leads to unpredictable outcomes in the disaster and the necessary performances should be made to avoid the outcomes.
The culture of fallibility supports reporting cases with errors to the organization, meanwhile focusing on performance punishments and unsafe activities. A culture of learning pays attention to the organization’s answers to disasters by repairing and improving not by denying. It means how much the organization denies the disasters instead of repairing and modifying them in a real way. Awareness means how the data (about how the quality of human performance at the workplace, how the extent of the problem, and how the current defending conditions are against the disaster) is collected. Preparation is related to how the organization actively anticipates the problems and the preparations for them. Preparation means being ready for the problems in human performances in advance. Flexibility is the ability of the organization to conform itself to new problems in a way that makes it more able to solve problems. This needs the people to be able to make important decisions without waiting for the instructions of the organization. Transparency means that the organization knows the safe borders of work. The answers to the questions have been classified with five possible answers based on the Likert scale (very satisfied, satisfied, neutral, unsatisfied, very unsatisfied) on which the very satisfying answers get 5 scores and the very unsatisfied answer gets 1 score, respectively. The gained score is evaluated with the number of questions about the topic and the people’s answers. Thus, the total score for evaluating disaster management based on engineering approaches is gained by multiplying the total number of questions of the survey by the Likert scale of each question. The higher scores showed better performances. The limit of the gained score of the survey was 44 to 220. Eventually, the answers were classified and evaluated in three levels including low (44 to 100), medium (101 to 160), and high (161 to 220) [15, 21]. In this study, continuous variables were expressed as Mean±SD, and categorical variables as numbers (percentage). A one-sample t-test was conducted to determine whether the observed means of the performance are significantly different from the mid-point of the scale (i.e. 50). The relationships between demographic variables and scores of performances were examined by using an independent t-test and one-way ANOVA. Statistical analysis was done using SPSS software, version 16 for Windows (SPSS Inc., Chicago, IL, USA), and a P<0.05 was considered statistically significant.
3. Results
One hundred eighty-nine nurses took part in this study. Among the participants, 88.89% were females, 96.83% had a bachelor of science in nursing (BSN), 44.44% were under 30 years old, and 41.27% had more than 10 years of experience. The demographic characteristics of the participants have been announced in Table 1.

The mean total score of the survey of the nurses’ performance, ranges, and items have been shown in Tables 2 and 3 from the nurses’ perspectives.

.JPG)

.JPG)

According to the results of the study, the Mean±SD total score of the nursing managers’ performances equaled 44.4±14.8 from the nurses’ perspectives. The level of performance on a qualitative scale was as follows: Very unsatisfied 5.4%, unsatisfied 31.5%, neutral 49.5%, satisfied 13.0%, and very satisfied 0.5%. Generally, the highest score of the nursing managers’ performance respectively related to the ranges of the culture of learning and culture of fallibility, and the lowest score related to the flexibility range from the nurses’ perspectives.
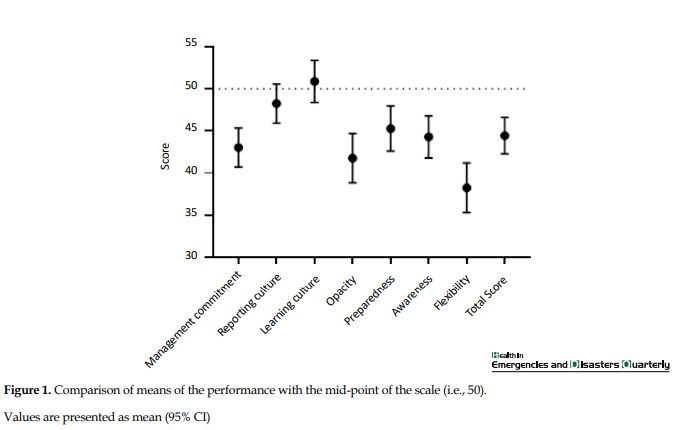
Comparison of performance scores with a midpoint of 50
According to the results of the sample t-test, the mean score of the nursing managers’ performance was meaningfully lower than the medium level (score of 50, P<0.001) from the nurses’ perspectives. The mean scores of performances in the ranges of management, transparency, preparation, and flexibility were meaningfully lower than the medium range (P<0.001), while there was not a meaningful statistical difference between the average scores of the performance in the ranges of the culture of fallibility (P=0.140), the culture of learning (P=0.488), and the medium-range (Figure 1). The Mean±SD scores of the resilience principles of the nursing managers’ performance separately included the senior management commitment 29.34±5.90), culture of fallibility 18.34±3.84), culture of learning 11.81±2.77), awareness 6.62±1.61), preparation 9.56±2.20), flexibility 48.42±10.31), and transparency 17.35±4.03).
Relationship of performance with nurses’ characteristics
As shown in Table 4, there is no meaningful statistical relationship between the scores of the nursing managers’ performance from the nurses’ perspectives and the nurses’ age (P=0.381). Also, there was no relationship between the scores of the nursing managers’ performance and their sex (P=0.467), level of education (P=0.771), working experience (P=0.761), and the nurses’ employment type (P=0.735).

4. Discussion
The results of the present study showed that most nurses believed the level of the nursing managers’ performance based on resilience during the COVID-19 pandemic was at a medium level. On the other hand, the highest and the lowest scores of the nursing managers’ performance were based on ‘workshops related to safety’. Also, there was a meaningful statistical difference between evaluating the nursing managers’ performance and the employment types. Generally, using resilience principles have been used as a strategy to evaluate the appropriate management in the health care systems in different countries during a disaster such as the COVID-19 pandemic [22]. The results of the study done by Alameddine et al. in 2021 which studied the nurses’ level of resilience during the pandemic showed that the nurses’ resilience levels were high which was different from the present study [17]. Another study which has been done by Lin et al in 2020 investigating the dispatched experts to Wuhan showed the nurses’ level of toleration was high [23]. Also, the studies done in China by Lin et al. and in South Korea by Huang et al. reported low levels of the working health staff’s level of toleration which disagreed with the present study [23, 24].
To explain this contradiction, we can refer to challenges like the lack of human resources, heavy movements, the unknown nature of the disease, and the confusion of the healthcare staff, especially at the beginning level of the disease because of the lack of certain treatments, and primary and hard cares. However, the conditions of taking care of patients suffering from COVID-19, the continuity of these problems, and the low levels of resilience in the management of the COVID-19 pandemic can lead to the healthcare staff’s burnout, especially nurses. However, the present study evaluated the level of the nursing managers’ performance based on the resilience principles during the COVID-19 pandemic from the nurses’ perspectives which was different from the compared studies. Although flexibility is a common feature of the present study and the compared ones, the studies were limited on this basis. Therefore, it has been recommended that future studies be done by focusing on the level of nursing managers’ performance based on resilience during the COVID-19 pandemic. Jo et al. showed that nurses perceiving high organizational support and also people taking part in improving the platforms and procedures of the departments and hospitals had higher scores of resilience in their study (P<0.01). Organizational support and nurses’ participation in improving policies can be considered important resilience factors [25]. In the present study, there is a meaningful statistical difference between evaluating the nursing managers’ performance by nurses and the employment type. While no meaningful relationship could be seen in the studies of Alameddine et al. and Lin and Huang. This difference can result from different factors such as the type of study tools, the culture, and the nature of the present study in comparison with the other studies [17, 23, 24].
In this study, the contracted nurses evaluated the level of the nursing managers more pleasantly in comparison with the registered nurses. This finding can result from different factors such as having less working experience and knowledge of this group concerning the nursing managers’ duties and responsibilities during the COVID-19 pandemic in comparison with administrative nurses. As other studies show the COVID-19 pandemic has pressed unprecedented pressure on the healthcare staff at international levels. An increase in the level of infections, not enough individual protective materials, and lack of availability of beds at hospitals lead to more hazards to the healthcare staff’s mental health which has unstable and brittle mental conditions. Those who have high resilience are less burnout and have a better performance in giving services to the patients [26].
5. Conclusion
This study showed that the level of the nursing managers’ performance based on resilience during the COVID-19 pandemic at the time of conducting the study was at a medium level. Since the pleasant performance of the nursing managers causes a decrease in burnout, an increase in working satisfaction, and ultimately a decrease in nurses’ levels from the nursing staff, designing and performing effective interventions to improve the nursing managers’ performance in the disaster is necessary. Actions based on how to create and improve flexibility in managers and service presenters at the front when facing patients suffering from the COVID-19 pandemic can be useful. These actions can be done by hospitals and other healthcare organizations to improve and keep mental and physical health in the long and short term. Also, hospitals can use these actions at the time of using and employing their experts so that more appropriate people are employed for the disaster in this job. It is also necessary for the managers to recognize and present strategies to create resilience among healthcare staff focusing on how resilience increases in nurses. It has been recommended that some studies should be done about designing interventions to create resilience to recognize the effects on the nurses’ resilience scores and the effects of their resilience on the nursing performances and the patients’ improvement. Moreover, organizational interventions should be investigated to consider the challenges of burnout effects on health care qualified presentation. COVID-19 has intensified the challenges in brittle healthcare systems. Nursing resilience is one of the intermediary factors between health systematics (such as extreme workloads, insufficient personnel, etc.) and burnout. Since the resilience between managers and health service presenters has been challenged during the pandemic, it is so important to design and experiment with strategies for improving resilience both at individual levels and healthcare system levels.
Nursing managers should create a long-term strategy to consider the nurses’ health during the disaster and after it. The trauma created by the COVID-19 pandemic has increased the managers’ responsibilities to create safe working environments and perform protective policies on nurses. These actions and strategies can be done at different levels. Interventions at primary levels are focused on creating flexibility through confrontational and relationship skills. Secondary interventions should consist of investigating levels of burnout and presenting support for those who are in danger of suffering from and gaining work experience. Ultimately, the third intervention should target the nurses who have gone forward more than their resilience level and need to be supported and improved to return safely to work. At the individual level, nursing managers can investigate their staff’s current emotional state in their units. Nursing managers should remind nurses about their permission to clearly express their feelings and their worries and ask for help to receive support related to mental health. Unwit resilience can be created when the nursing managers encourage cohesion among the interdisciplinary team members. Since we are hopeful that we move forward from the main level to the last one, the healthcare organizations and the managers should allow their staff to express their feelings. The health care organizations are needed to thank the staff and award them and also recognize the staff who show signals of stress after the event and give them the appropriate mental health resources.
Limitations and recommendations
One of the limitations of this study was the use of a questionnaire and receiving the opinions of nurses through self-reporting, which could have caused errors in answering. Also, the sample size was from a city in the north of Iran, which, although it had a very high morbidity rate, the findings of this study cannot be generalized to all hospitals in Iran. Furthermore, considering that this study was conducted with a quantitative approach, it is suggested to conduct additional studies using qualitative research methods to extract more and deeper experiences.
Ethical Considerations
Compliance with ethical guidelines
The ethical approval to conduct the study was obtained from the Institutional Review Board of Guilan University of Medical Sciences (Code: IR.GUMS.REC.1399.269). This study confirmed that all methods were carried out following relevant regulations and informed consent was obtained from all subjects.
Funding
This research was supported financially by Guilan University of Medical Sciences.
Authors' contributions
Study design and data collection: Negar Pourvakhshoori; Data analysis: Saman Maroufizadeh, Habib Eslami-Kenarsari and Saman Maroufizadeh; Supervision: Negar Pourvakhshoori, Sedigheh Abdollahi, Bita Badparva, Shirin Sayyad and Saman Maroufizadeh; Manuscript writing: Negar Pourvakhshoori and Bita Badparva; Critical revisions for important intellectual content: Negar Pourvakhshoori, Bita Badparva, Sedigheh Abdollahi, Parvaneh Babakian and Shirin Sayyad; Final approving: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors wish to express their gratitude to all nurses who participated in this study and also to the Guilan University of Medical Sciences for financial support.
References
Nurses are one of the main groups of health experts responsible for confronting and taking care of people when disasters happen [1]. Nurses play an important role during the COVID-19 pandemic like any other disaster. Taking care of patients has been challenging during disasters and had its special conditions, so taking care of patients suffering from COVID-19 is the same. In recent pandemic conditions, intensive care is taken in isolated units. Therefore, nurses will have to cope with the expanding workload and more different rotating shifts. One of the most important factors at this time is the nursing shortage. Therefore, it is necessary to consider the necessary arrangements like scheduling the rotating shifts well and effectively using human resources [2]. Nurses have been playing important roles in preventing and controlling infections and generally improving public health as was first raised by Florence Nightingale [3]. The conditions of disasters are very important and unique and need these special preparations and skills [4]. Providing healthcare during the COVID-19 pandemic is a unique condition, so it is important to know about its special features. Studies done at the time of the pandemic show that nurses experience conditions similar to those of previous pandemics. They have been worried about the health and safety of their families and themselves and needed to have connections with their families and the nursing team members. Since there are no certain treatments and effective antivirus medicine for the disease, managing patients suffering from COVID-19 has become a great problem in the work which is believed not to have an end. Moreover, managing these patients burdens healthcare providers, especially nurses, with difficulty or hard work. Currently, COVID-19 has caused anxiety in the public health and treatment community. That is why this virus is spreading all over the world and sharing a burden on low-income and developing countries [5, 6]. The COVID-19 pandemic is a major threat to public health all over the world. Therefore, a coordinated universal reaction is needed to prepare healthcare systems and confront this unprecedented challenge. Sound management of human resources can increase the efficiency and quality of the nurses’ care [7].
The COVID-19 pandemic has created fast changes in the structures of hospitals. Nurses of the ICU who take care of patients suffering from serious illnesses experience new challenges by delivering services in new units called the COVID-19 ICUs. The increased number of COVID-19 patients and the respiratory systems made the managers of the ICUs in Italy change the recovery and surgery units into COVID-19 ones because of the lack of empty beds in ICUs. The increase of patients with serious illnesses means sudden organizational changes which have been made by the hospital managers to make human resources give a quick response to the unprecedented disaster in delivering health care services. These conditions have provoked challenges and new opportunities for nursing management which are remarkable [8]. Nurses have faced a lot of challenges during the COVID-19 pandemic such as difficult and long-term shifts, and long-term uses of personal and protective supplies such as N95 masks which can cause skin disorders, an increase in burnout, dehydration, and an increase in medical errors. Therefore, managing these great challenges during the pandemic needs appropriate decisions at the level of management which make the nursing managers’ roles prominent [9]. Nurses have actively been doing their jobs of controlling infections and taking special care of patients at the forefront since the beginning of the pandemic [10].
During the current pandemic, attention has been drawn to nurses working in the ICUs, and their important roles in taking long-term care of patients have been highlighted in recent months [11]. At the time confronting stressful conditions like the COVID-19 pandemic, it is so important for nursing managers to have enough capabilities to support in a good and appropriate way to come up against the hard days [12]. Nursing managers can be effective in the pandemic by identifying and improving appropriate strategies for taking care of patients suffering from COVID-19 [7]. Generally, in the studies, nurses reported their experience in seeing the patients’ agony and death. Moreover, the nursing managers enumerated extra responsibilities in managing human resources and supplies as their challenges during the pandemic [13-15]. The determined main strategies by World Health Organization (WHO) are as follows: Stopping the disease to be transmitted, recognizing, separating, and taking care of patients suffering from the virus, accelerating recognition, curing and vaccinating, performing activities about giving awareness to society and minimizing social and economic effects of the pandemic [1]. Nurses use their knowledge and skills to take the necessary care of patients at all levels of sickness to satisfy these approaches although there is a lack of the necessary supplies such as protective personal supplies with high quality. Society especially guides the most susceptible people and works considering the safety of the patients and the treatment team by following innovative strategies. Therefore, they face challenges that eventually make them stronger and learn valuable skills compared to the times when the pandemic has not started yet [16]. One of the ways to confront the COVID-19 pandemic is by increasing resilience which can give nursing managers a wider perspective on avoiding, preparing for, and answering the disaster [17]. The paradigm of resilience consists of seven main units including management commitments at senior levels, the culture of fallibility, the culture of learning, awareness, preparation, and transparency. Generally, resilience can prevent probable failures and losses in a disaster and the capability to give appropriate responses after a disaster [18]. Nursing managers are faced with a lot of daily challenges which need flexibility and great skills. The COVID-19 pandemic has put nursing managers under unprecedented pressure to make them update the resources, the staff, and the controlling infection strategies and revive connections with multidisciplinary teams. At the peak of the COVID-19 pandemic in the summer of 2020, a group of nursing managers dealt with producing resilience in the health system in the east of the Middle East to improve the emotional comfort and equilibrium between work and life to optimize and improve their management [19].
Most of the studies are about the resilience in the health care systems such as NHS based on the organizational disaster such as a lack of nurses, an increase in the workforce, and financial limitations. However, the nursing system can learn from the past to consider more stamina. Why resilience is important returns to the issue that when a saddening event such as the pandemic happens, resilience gives us the capability to resist the disorders with our natural performances by anticipating and preparing ourselves for the event. Also, we can have positive results such as a decrease in burnout and an increase in confrontational behavior by improving resilience strategies [16, 20]. The nursing managers’ decisions to manage the pandemic are important and should be made quickly and without wasting time. The performance referring to nursing managers’ appropriate decisions lead to better management during the COVID-19 pandemic. Therefore, the present study has been done to evaluate the nurse managers’ performance based on resilience during the COVID-19 pandemic from the nurses’ perspectives regarding the importance of this problem to take the necessary actions to improve the quality of the management and the nursing services by surveying the current conditions.
2. Materials and Methods
One hundred eighty-nine Iranian nurses working in the Corona center hospital in Guilan province participated in this cross-sectional study. This hospital is the main center of curing COVID-19 patients. Nurses who had at least one month experience of taking care of patients suffering from COVID-19 and were willing to participate in this study were considered. The data were collected by using a questionnaire consisting of demographic features and disaster-managing surveys based on seven engineering approaches at the hospitals by the enumeration sampling from June to October 2021. The first part of the questionnaire consisted of some information such as age, sex, level of education, experience in clinical work, and type of employment. The second part consisted of the survey of disaster management based on seven engineering resilience principles at hospitals which have been designed by Azadian et al. [21] and its validity and stability have been verified (Cronbach’s α 0.977 and the intragroup correlation coefficient 0.97). This questionnaire consisted of forty-four questions and seven subscales: Management commitment (9 questions), the culture of fallibility (6 questions), the culture of learning (4 questions), awareness (5 questions), preparation (3 questions), flexibility (5 questions), and transparency (2 questions). Senior management shows a commitment to recognizing the factors related to human performance. The management tries to recognize the human performances which lead to making errors and make the organization pay attention to the errors. Because at the time a disaster happens and the number of people going to hospitals increases, every single error which could be ignored in daily performances leads to unpredictable outcomes in the disaster and the necessary performances should be made to avoid the outcomes.
The culture of fallibility supports reporting cases with errors to the organization, meanwhile focusing on performance punishments and unsafe activities. A culture of learning pays attention to the organization’s answers to disasters by repairing and improving not by denying. It means how much the organization denies the disasters instead of repairing and modifying them in a real way. Awareness means how the data (about how the quality of human performance at the workplace, how the extent of the problem, and how the current defending conditions are against the disaster) is collected. Preparation is related to how the organization actively anticipates the problems and the preparations for them. Preparation means being ready for the problems in human performances in advance. Flexibility is the ability of the organization to conform itself to new problems in a way that makes it more able to solve problems. This needs the people to be able to make important decisions without waiting for the instructions of the organization. Transparency means that the organization knows the safe borders of work. The answers to the questions have been classified with five possible answers based on the Likert scale (very satisfied, satisfied, neutral, unsatisfied, very unsatisfied) on which the very satisfying answers get 5 scores and the very unsatisfied answer gets 1 score, respectively. The gained score is evaluated with the number of questions about the topic and the people’s answers. Thus, the total score for evaluating disaster management based on engineering approaches is gained by multiplying the total number of questions of the survey by the Likert scale of each question. The higher scores showed better performances. The limit of the gained score of the survey was 44 to 220. Eventually, the answers were classified and evaluated in three levels including low (44 to 100), medium (101 to 160), and high (161 to 220) [15, 21]. In this study, continuous variables were expressed as Mean±SD, and categorical variables as numbers (percentage). A one-sample t-test was conducted to determine whether the observed means of the performance are significantly different from the mid-point of the scale (i.e. 50). The relationships between demographic variables and scores of performances were examined by using an independent t-test and one-way ANOVA. Statistical analysis was done using SPSS software, version 16 for Windows (SPSS Inc., Chicago, IL, USA), and a P<0.05 was considered statistically significant.
3. Results
One hundred eighty-nine nurses took part in this study. Among the participants, 88.89% were females, 96.83% had a bachelor of science in nursing (BSN), 44.44% were under 30 years old, and 41.27% had more than 10 years of experience. The demographic characteristics of the participants have been announced in Table 1.
The mean total score of the survey of the nurses’ performance, ranges, and items have been shown in Tables 2 and 3 from the nurses’ perspectives.
According to the results of the study, the Mean±SD total score of the nursing managers’ performances equaled 44.4±14.8 from the nurses’ perspectives. The level of performance on a qualitative scale was as follows: Very unsatisfied 5.4%, unsatisfied 31.5%, neutral 49.5%, satisfied 13.0%, and very satisfied 0.5%. Generally, the highest score of the nursing managers’ performance respectively related to the ranges of the culture of learning and culture of fallibility, and the lowest score related to the flexibility range from the nurses’ perspectives.
Comparison of performance scores with a midpoint of 50
According to the results of the sample t-test, the mean score of the nursing managers’ performance was meaningfully lower than the medium level (score of 50, P<0.001) from the nurses’ perspectives. The mean scores of performances in the ranges of management, transparency, preparation, and flexibility were meaningfully lower than the medium range (P<0.001), while there was not a meaningful statistical difference between the average scores of the performance in the ranges of the culture of fallibility (P=0.140), the culture of learning (P=0.488), and the medium-range (Figure 1). The Mean±SD scores of the resilience principles of the nursing managers’ performance separately included the senior management commitment 29.34±5.90), culture of fallibility 18.34±3.84), culture of learning 11.81±2.77), awareness 6.62±1.61), preparation 9.56±2.20), flexibility 48.42±10.31), and transparency 17.35±4.03).
Relationship of performance with nurses’ characteristics
As shown in Table 4, there is no meaningful statistical relationship between the scores of the nursing managers’ performance from the nurses’ perspectives and the nurses’ age (P=0.381). Also, there was no relationship between the scores of the nursing managers’ performance and their sex (P=0.467), level of education (P=0.771), working experience (P=0.761), and the nurses’ employment type (P=0.735).
4. Discussion
The results of the present study showed that most nurses believed the level of the nursing managers’ performance based on resilience during the COVID-19 pandemic was at a medium level. On the other hand, the highest and the lowest scores of the nursing managers’ performance were based on ‘workshops related to safety’. Also, there was a meaningful statistical difference between evaluating the nursing managers’ performance and the employment types. Generally, using resilience principles have been used as a strategy to evaluate the appropriate management in the health care systems in different countries during a disaster such as the COVID-19 pandemic [22]. The results of the study done by Alameddine et al. in 2021 which studied the nurses’ level of resilience during the pandemic showed that the nurses’ resilience levels were high which was different from the present study [17]. Another study which has been done by Lin et al in 2020 investigating the dispatched experts to Wuhan showed the nurses’ level of toleration was high [23]. Also, the studies done in China by Lin et al. and in South Korea by Huang et al. reported low levels of the working health staff’s level of toleration which disagreed with the present study [23, 24].
To explain this contradiction, we can refer to challenges like the lack of human resources, heavy movements, the unknown nature of the disease, and the confusion of the healthcare staff, especially at the beginning level of the disease because of the lack of certain treatments, and primary and hard cares. However, the conditions of taking care of patients suffering from COVID-19, the continuity of these problems, and the low levels of resilience in the management of the COVID-19 pandemic can lead to the healthcare staff’s burnout, especially nurses. However, the present study evaluated the level of the nursing managers’ performance based on the resilience principles during the COVID-19 pandemic from the nurses’ perspectives which was different from the compared studies. Although flexibility is a common feature of the present study and the compared ones, the studies were limited on this basis. Therefore, it has been recommended that future studies be done by focusing on the level of nursing managers’ performance based on resilience during the COVID-19 pandemic. Jo et al. showed that nurses perceiving high organizational support and also people taking part in improving the platforms and procedures of the departments and hospitals had higher scores of resilience in their study (P<0.01). Organizational support and nurses’ participation in improving policies can be considered important resilience factors [25]. In the present study, there is a meaningful statistical difference between evaluating the nursing managers’ performance by nurses and the employment type. While no meaningful relationship could be seen in the studies of Alameddine et al. and Lin and Huang. This difference can result from different factors such as the type of study tools, the culture, and the nature of the present study in comparison with the other studies [17, 23, 24].
In this study, the contracted nurses evaluated the level of the nursing managers more pleasantly in comparison with the registered nurses. This finding can result from different factors such as having less working experience and knowledge of this group concerning the nursing managers’ duties and responsibilities during the COVID-19 pandemic in comparison with administrative nurses. As other studies show the COVID-19 pandemic has pressed unprecedented pressure on the healthcare staff at international levels. An increase in the level of infections, not enough individual protective materials, and lack of availability of beds at hospitals lead to more hazards to the healthcare staff’s mental health which has unstable and brittle mental conditions. Those who have high resilience are less burnout and have a better performance in giving services to the patients [26].
5. Conclusion
This study showed that the level of the nursing managers’ performance based on resilience during the COVID-19 pandemic at the time of conducting the study was at a medium level. Since the pleasant performance of the nursing managers causes a decrease in burnout, an increase in working satisfaction, and ultimately a decrease in nurses’ levels from the nursing staff, designing and performing effective interventions to improve the nursing managers’ performance in the disaster is necessary. Actions based on how to create and improve flexibility in managers and service presenters at the front when facing patients suffering from the COVID-19 pandemic can be useful. These actions can be done by hospitals and other healthcare organizations to improve and keep mental and physical health in the long and short term. Also, hospitals can use these actions at the time of using and employing their experts so that more appropriate people are employed for the disaster in this job. It is also necessary for the managers to recognize and present strategies to create resilience among healthcare staff focusing on how resilience increases in nurses. It has been recommended that some studies should be done about designing interventions to create resilience to recognize the effects on the nurses’ resilience scores and the effects of their resilience on the nursing performances and the patients’ improvement. Moreover, organizational interventions should be investigated to consider the challenges of burnout effects on health care qualified presentation. COVID-19 has intensified the challenges in brittle healthcare systems. Nursing resilience is one of the intermediary factors between health systematics (such as extreme workloads, insufficient personnel, etc.) and burnout. Since the resilience between managers and health service presenters has been challenged during the pandemic, it is so important to design and experiment with strategies for improving resilience both at individual levels and healthcare system levels.
Nursing managers should create a long-term strategy to consider the nurses’ health during the disaster and after it. The trauma created by the COVID-19 pandemic has increased the managers’ responsibilities to create safe working environments and perform protective policies on nurses. These actions and strategies can be done at different levels. Interventions at primary levels are focused on creating flexibility through confrontational and relationship skills. Secondary interventions should consist of investigating levels of burnout and presenting support for those who are in danger of suffering from and gaining work experience. Ultimately, the third intervention should target the nurses who have gone forward more than their resilience level and need to be supported and improved to return safely to work. At the individual level, nursing managers can investigate their staff’s current emotional state in their units. Nursing managers should remind nurses about their permission to clearly express their feelings and their worries and ask for help to receive support related to mental health. Unwit resilience can be created when the nursing managers encourage cohesion among the interdisciplinary team members. Since we are hopeful that we move forward from the main level to the last one, the healthcare organizations and the managers should allow their staff to express their feelings. The health care organizations are needed to thank the staff and award them and also recognize the staff who show signals of stress after the event and give them the appropriate mental health resources.
Limitations and recommendations
One of the limitations of this study was the use of a questionnaire and receiving the opinions of nurses through self-reporting, which could have caused errors in answering. Also, the sample size was from a city in the north of Iran, which, although it had a very high morbidity rate, the findings of this study cannot be generalized to all hospitals in Iran. Furthermore, considering that this study was conducted with a quantitative approach, it is suggested to conduct additional studies using qualitative research methods to extract more and deeper experiences.
Ethical Considerations
Compliance with ethical guidelines
The ethical approval to conduct the study was obtained from the Institutional Review Board of Guilan University of Medical Sciences (Code: IR.GUMS.REC.1399.269). This study confirmed that all methods were carried out following relevant regulations and informed consent was obtained from all subjects.
Funding
This research was supported financially by Guilan University of Medical Sciences.
Authors' contributions
Study design and data collection: Negar Pourvakhshoori; Data analysis: Saman Maroufizadeh, Habib Eslami-Kenarsari and Saman Maroufizadeh; Supervision: Negar Pourvakhshoori, Sedigheh Abdollahi, Bita Badparva, Shirin Sayyad and Saman Maroufizadeh; Manuscript writing: Negar Pourvakhshoori and Bita Badparva; Critical revisions for important intellectual content: Negar Pourvakhshoori, Bita Badparva, Sedigheh Abdollahi, Parvaneh Babakian and Shirin Sayyad; Final approving: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors wish to express their gratitude to all nurses who participated in this study and also to the Guilan University of Medical Sciences for financial support.
References
- Pourvakhshoori N, Norouzi K, Ahmadi F, Hosseini M, Khankeh H. Nurse in limbo: A qualitative study of nursing in disasters in Iranian context. PLoS One, 2017; 12(7):e0181314. [DOI:10.1371/journal.pone.0181314] [PMID] [PMCID]
- Gao X, Jiang L, Hu Y, Li L, Hou L. Nurses' experiences regarding shift patterns in isolation wards during the COVID-19 pandemic in China: A qualitative study. Journal of Clinical Nursing. 2020; 29(21-22):4270-80. [DOI:10.1111/jocn.15464] [PMID] [PMCID]
- Smith GD, Ng F, Ho Cheung Li W. COVID-19: Emerging compassion, courage and resilience in the face of misinformation and adversity. Journal of Clinical Nursing. 2020; 29(9-10):1425-8. [DOI:10.1111/jocn.15231] [PMID] [PMCID]
- Pourvakhshoori N, Norouzi K, Ahmadi F, Hosseini M, Khankeh H. Nursing in disasters: A review of existing models. International Emergency Nursing. 2017; 31:58-63. [DOI:10.1016/j.ienj.2016.06.004] [PMID]
- Jamaati H, Dastan F, Tabarsi P, Marjani M, Saffaei A, Hashemian SM. A fourteen-day experience with coronavirus disease 2019 (COVID-19) induced Acute Respiratory Distress Syndrome (ARDS): An Iranian Treatment Protocol. Iranian Journal of Pharmaceutical Research. 2020; 19(1):31-6. [DOI:10.22037/ijpr.2020.113337.14239] [PMID]
- Khankeh H, Farrokhi M, Roudini J, Pourvakhshoori N, Ahmadi S, Abbasabadi-Arab M, et al. Challenges to manage pandemic of coronavirus disease (COVID-19) in Iran with a special situation: A qualitative multi-method study. BMC Public Health. 2021; 21(1):1919. [DOI:10.1186/s12889-021-11973-5] [PMID] [PMCID]
- Poortaghi S, Shahmari M, Ghobadi A. Exploring nursing managers' perceptions of nursing workforce management during the outbreak of COVID-19: A content analysis study. BMC Nursing. 2021; 20(1):27. [DOI:10.1186/s12912-021-00546-x] [PMID] [PMCID]
- Catania G, Zanini M, Hayter M, Timmins F, Dasso N, Ottonello G, et al. Lessons from Italian front-line nurses' experiences during the COVID-19 pandemic: A qualitative descriptive study. Journal of Nursing Management. 2021; 29(3):404-11. [DOI:10.1111/jonm.13194] [PMID]
- Sharma SK, Nuttall C, Kalyani V; Hemlata. Clinical nursing care guidance for management of patient with COVID-19. The Journal of the Pakistan Medical Association. 2020; 70(Suppl 3)(5):S118-23. [PMID]
- Muz G, Erdoğan Yüce G. Experiences of nurses caring for patients with COVID-19 in Turkey: A phenomenological enquiry. Journal of Nursing Management, 2021; 29(5):1026-35. [DOI:10.1111/jonm.13240] [PMID]
- Resnick B. What have we learned about nursing from the Coronavirus Pandemic? Journal of the American Medical Directors Association. 2020; 21(7):997-8. [DOI:10.1016/j.jamda.2020.06.011] [PMID] [PMCID]
- Gab Allah AR. Challenges facing nurse managers during and beyond COVID-19 pandemic in relation to perceived organizational support. Nursing Forum. 2021; 56(3):539-49. [DOI:10.1111/nuf.12578] [PMID] [PMCID]
- Sun Q, Qiu H, Huang M, Yang Y. Lower mortality of COVID-19 by early recognition and intervention: Experience from Jiangsu Province. Annals of Intensive Care. 2020; 10(1):33. [DOI:10.1186/s13613-020-00650-2] [PMID] [PMCID]
- Galehdar N, Toulabi T, Kamran A, Heydari H. Exploring nurses' perception of taking care of patients with coronavirus disease (COVID-19): A qualitative study. Nursing Open. 2021; 8(1):171-9. [DOI:10.1002/nop2.616] [PMID] [PMCID]
- White JH. A phenomenological study of nurse managers' and assistant nurse managers' experiences during the covid-19 pandemic in the United States. Journal of Nursing Management. 2021; 29(6):1525-34. [DOI:10.1111/jonm.13304] [PMID] [PMCID]
- Odom-Forren J. Nursing resilience in the world of COVID-19. Journal of Perianesthesia Nursing. 2020; 35(6):555-6. [DOI:10.1016/j.jopan.2020.10.005] [PMID] [PMCID]
- Alameddine M, Bou-Karroum K, Ghalayini W, Abiad F. Resilience of nurses at the epicenter of the COVID-19 pandemic in Lebanon. International Journal of Nursing Sciences. 2021; 8(4):432-8. [DOI:10.1016/j.ijnss.2021.08.002] [PMID] [PMCID]
- Jeffcott SA, Ibrahim JE, Cameron PA. Resilience in healthcare and clinical handover. Quality & Safety in Health Care. 2009; 18(4):256-60. [DOI:10.1136/qshc.2008.030163] [PMID]
- Carter M, Turner KM. Enhancing nurse manager resilience in a pandemic. Nurse Leader. 2021; 19(6):622-4. [DOI:10.1016/j.mnl.2021.07.007] [PMID] [PMCID]
- Bazyar J, Alimoradi S, Seydi M, Pourvakhshoori N, Sadeghifar J. Coronavirus disease-2019 risk management using strengths, weaknesses, opportunities, threats analysis approach in the health system: A qualitative multimethod study. Journal of Education and Health Promotion. 2021; 10:453. [PMID] [PMCID]
- Azadian S, Shirali G, Saki A. [Evaluation reliability and validity a questionnaire to assess crisis management based on seven principles of resilience engineering approach in hospitals (Persian)]. Jundishapur Journal of Health Sciences. 2016; 13(1):15-26. [Link]
- Woods DD. Four concepts for resilience and the implications for the future of resilience engineering. Reliability Engineering & System Safety. 2015; 141:5-9. [DOI:10.1016/j.ress.2015.03.018]
- Lin J, Ren YH, Gan HJ, Chen Y, Huang YF, You XM. Factors associated with resilience among non-local medical workers sent to Wuhan, China during the COVID-19 outbreak. BMC Psychiatry. 2020; 20(1):417. [DOI:10.1186/s12888-020-02821-8] [PMID] [PMCID]
- Huang L, Wang Y, Liu J, Ye P, Cheng B, Xu H, et al. Factors associated with resilience among medical staff in radiology departments during the outbreak of 2019 novel coronavirus disease (COVID-19): A cross-sectional study. Medical Science Monitor. 2020; 26:e925669. [DOI:10.12659/MSM.925669]
- Jo S, Kurt S, Bennett JA, Mayer K, Pituch KA, Simpson V, et al. Nurses' resilience in the face of coronavirus (COVID-19): An international view. Nursing & Health Sciences. 2021; 23(3):646-57. [DOI:10.1111/nhs.12863] [PMID] [PMCID]
- Baskin RG, Bartlett R. Healthcare worker resilience during the COVID-19 pandemic: An integrative review. Journal of Nursing Management. 2021; 29(8):2329-42. [DOI:10.1111/jonm.13395] [PMID] [PMCID]
Type of article: Research |
Subject:
Special
Received: 2022/08/4 | Accepted: 2023/02/24 | Published: 2023/07/24
Received: 2022/08/4 | Accepted: 2023/02/24 | Published: 2023/07/24
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
