

Volume 11, Issue 2 (Winter 2026)
Health in Emergencies and Disasters Quarterly 2026, 11(2): 161-170 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rahmati R, Delam H, Keshtkaran Z, Shafiei M. Impact of COVID-19 on Women’s Psychological Well-Being: General Health, Anxiety, and Stress in Larestan, Iran. Health in Emergencies and Disasters Quarterly 2026; 11 (2) :161-170
URL: http://hdq.uswr.ac.ir/article-1-653-en.html
URL: http://hdq.uswr.ac.ir/article-1-653-en.html



1- Department of Midwifery, School of Nursing,Larestan University of Medical Sciences,Larestan, Iran.
2- Student Research Committee,Shiraz University of Medical Sciences,Shiraz, Iran.
3- Department of Nursing, Community-Based Psychiatric Care Research Center, School of Nursing and Midwifery,Shiraz University of Medical Sciences,Shiraz, Iran.
4- Department of Health in Disasters and Emergencies, School of Nursing,Larestan University of Medical Sciences, Larestan, Iran. ,jupiter782.782@gmail.com
2- Student Research Committee,Shiraz University of Medical Sciences,Shiraz, Iran.
3- Department of Nursing, Community-Based Psychiatric Care Research Center, School of Nursing and Midwifery,Shiraz University of Medical Sciences,Shiraz, Iran.
4- Department of Health in Disasters and Emergencies, School of Nursing,Larestan University of Medical Sciences, Larestan, Iran. ,
Full-Text [PDF 496 kb]
(649 Downloads)
| Abstract (HTML) (2007 Views)
References
Full-Text: (331 Views)
Introduction
Pandemics, as worldwide emergencies, significantly alter numerous aspects of human existence, with mental well-being emerging as a key area of concern. Women, often more susceptible due to their extensive social and family duties, caregiving obligations, and distinct physical and emotional traits, encounter intensified psychological difficulties during such crises. These factors collectively increase their risk for conditions, such as depression and anxiety [1, 2]. If not addressed, these conditions can profoundly impair individuals by diminishing their quality of life, straining personal connections, and increasing their predisposition to physical ailments. Moreover, persistent stress linked to these psychological states can compromise immune function, further intensifying their vulnerabilities [2].
Studies underscore the substantial effect of pandemics on women’s psychological health, driven largely by disruptions in everyday routines, including heightened societal and financial burdens, limitations on physical and social interactions, and changes in sleep and dietary habits [3, 4]. For instance, during the SARS epidemic, women faced heightened stress and depressive symptoms due to limited social interactions, mandatory isolation, evolving family dynamics, and greater demands from domestic and caregiving tasks [5]. Similarly, the Zika pandemic has raised severe mental health concerns among pregnant women, driven by fear of the potential adverse effects of the virus on the fetus. This anxiety not only impacts mothers’ mental health but also influences their decisions regarding pregnancy and medical care. [6].
Historical pandemics, such as the Spanish Flu and SARS have revealed similar patterns. Women, particularly pregnant women, were more vulnerable to depression and anxiety due to societal pressures, physical limitations, and changing gender roles [7, 8]. Evidence also suggests that women are more likely to experience post-traumatic stress disorder (PTSD) during such events; a SARS-era study, for instance, found that women were more predisposed to PTSD than men [9]. Additionally, during the H1N1 pandemic, pregnant women and young mothers faced an elevated risk of anxiety and depressive disorders [10].
The COVID-19 pandemic, as the latest global health crisis, has caused rapid increases in infections and deaths worldwide, including Iran, where its spread was confirmed on February 29, 2020 [11, 12]. This pandemic has significantly disrupted economies, politics, and societies globally, leading to increased mental health challenges across various population groups, including women, healthcare workers, children, students, and families [13, 14]. Psychological challenges, including anxiety, stress, and depression, have surged during this period. For example, research on patients admitted for COVID-19-related respiratory issues revealed markedly higher anxiety and depression levels compared to those with other respiratory conditions, like pneumonia [15].
Given the complex effects of pandemics on women’s mental health, identifying those at risk of psychological disorders and introducing suitable interventions to bolster their well-being is essential [16]. Maintaining mental health during crises is essential as individuals, including patients, healthcare workers, and family members, face stressors directly linked to the pandemic [17, 18]. Evidence highlights the importance of studying women’s mental health during such events, pinpointing risk and protective factors, and crafting effective strategies for prevention and support to lessen the psychological toll of these crises [18].
Given these vulnerabilities, it is essential to investigate the emotional effects of pandemics on women to identify potential risk elements, develop preventive strategies, and create targeted support measures. This research aimed to explore the relationship between overall health and the presence of depression, anxiety, and stress (DASS-21) in women utilizing healthcare services amid the COVID-19 outbreak. By addressing this urgent issue, our goal was to provide research-supported recommendations for policymakers and mental health professionals to mitigate the psychological impacts of such crises.
Materials and Methods
This study was designed as a descriptive-analytical inquiry within a cross-sectional framework and was conducted throughout 2021. It involved women who attended health facilities affiliated with the Larestan Faculty of Medical Sciences. The process began by assembling a detailed directory of these centers, with each facility’s name inscribed on a separate piece of paper. These were then sealed in individual envelopes, and ten were picked at random. The research team visited these designated sites, employing a practical sampling approach while ensuring alignment with specific inclusion and exclusion criteria.
To calculate the required number of participants, a statistical method based on the mean sample size was utilized. With a confidence level set at 95% and a margin of error of 0.09 standard deviation, the study aimed to recruit approximately 475 women. Eligibility required a voluntary agreement to participate, the ability to read and write, and possession of a digital device—such as a smartphone, tablet, or laptop—to access the online survey. Women were excluded if they submitted partially completed forms, opted out during the study, had a history of severe or persistent mental health issues, or had experienced significant emotional turmoil in the preceding six months, such as the loss of a family member, marital changes, or a diagnosis of a terminal condition.
Data collection was done using three tools: one to gather personal background details, another to assess overall well-being, and a third to measure emotional strain. Personal details included participants’ age, educational background, and marital status.
Research design
The investigation followed a cross-sectional, descriptive-analytical model and took place in 2021.
Study context
The focus was on women utilizing healthcare services at centers affiliated with the Larestan Faculty of Medical Sciences.
Timing and location
The fieldwork occurred in 2021 within health facilities governed by the Larestan Faculty of Medical Sciences.
Participants
The sample consisted of women who visited the chosen health centers during the research period.
Sample size determination
A mean-based calculation method was applied, factoring in a 95% confidence interval and a 0.09 standard deviation error margin, targeting a total of 475 participants.
Selection procedure
A complete inventory of health centers linked to the Larestan Faculty of Medical Sciences was first created, with each center’s name noted on individual slips of paper. These slips were placed into envelopes, and ten were randomly selected. Researchers then visited these locations, using an accessible sampling technique while adhering to predefined participation criteria.
Inclusion criteria
1) Willingness to take part voluntarily; 2) basic proficiency in reading and writing; 3) ownership of a device (e.g. smartphone, tablet, or computer) to complete the digital survey.
Exclusion criteria
1) Failure to fully complete the survey; 2) choosing to withdraw from the study before completion; 3) history of acute or ongoing psychiatric disorders; 4) recent significant emotional distress within the past six months (e.g. bereavement, divorce, marriage, or severe illness).
Assessment tools
Three instruments were employed:
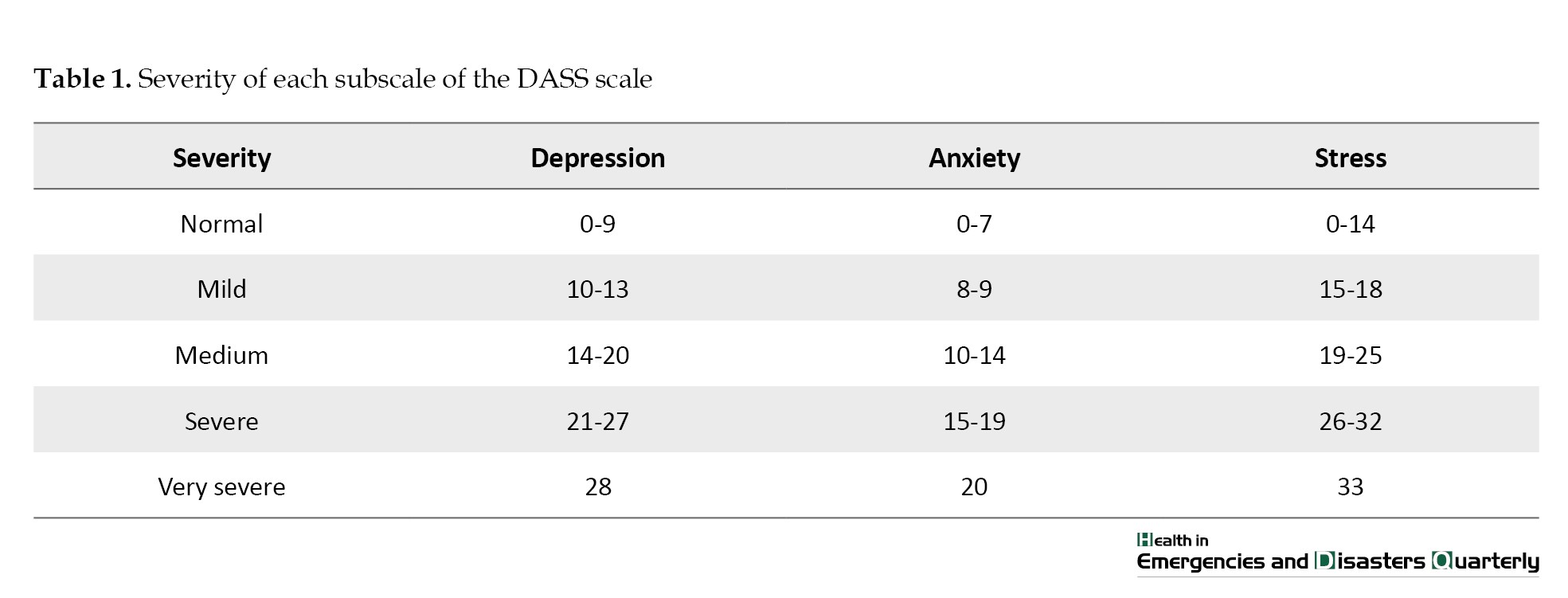
1) Personal information form: This recorded details, such as age, education level, and marital status; 2) General health questionnaire–28 (GHQ-28): This tool was developed by Goldberg in 1978 [19]. It has 28 questions grouped into four categories, each containing eight items. Participants rated each question on a four-point scale, with scores ranging from 0 to 3 based on a Likert system. The total score was calculated by adding the results from all four categories, where lower scores indicated better well-being and higher scores suggested greater impairment. The categories cover physical complaints (items 1-7), anxiety and sleep disturbances (items 8-14), social challenges (items 15-21), and depressive tendencies (items 22-28), with a maximum possible score of 84. Its reliability was validated by Ebrahimi et al. with a consistency coefficient of 0.88 [20]. 2) physical Complaints Category: Scores of 0-9 reflect robust physical health despite psychosomatic issues, 10-15 suggest moderate well-being, and 16-21 indicate pronounced psychosomatic symptoms. 3) anxiety and sleep category: Scores of 0-9 signify a calm and controlled state, 10-15 imply occasional anxiety, and 16-21 point to intense anxiety in various contexts. 4) social Challenges Category: Scores of 0-9 denote strong interpersonal and workplace functioning, 10-15 reflect moderate social health, and 16-21 indicate persistent relational or work-related struggles. 5) depression category: Scores of 0-9 suggest vitality and positivity in daily life, 10-15 indicate occasional low mood, and 16-21 signal a probable depressive state. 6) total score interpretation: A range of 0-21 reflects excellent mental well-being, 22-42 suggests some areas of concern, 43-63 indicates repeated mental health difficulties, and 64-84 points to a severe condition. 7) Emotional strain assessment (DASS-21): This tool consists of 21 questions divided into three sets of seven, each targeting a distinct emotional domain. Scores are derived by summing responses within each set, with ratings from 0 (not relevant to me) to 3 (highly relevant). As a condensed version of the original 42-item tool, each set’s score is doubled, and severity is evaluated using established thresholds (Table 1).
Its suitability for Iranian contexts was confirmed by Afzali et al. with reliability scores of 0.81 for depression, 0.73 for anxiety, and 0.81 for stress [21].
The tools were hosted on Google Forms, and access links were shared with qualifying participants via SMS and WhatsApp. The collected data were organized and encoded by the research team and then analyzed using SPSS software, version 25. Statistical methods included the independent t-test, chi-square test, and analysis of variance (ANOVA), adjusted for data normality, with a significance threshold of 5%. The DASS-21 measures three emotional dimensions: Depression (items 3, 5, 10, 13, 16, 17, and 21), anxiety (items 2, 4, 9, 15, 19, and 20), and stress (items 1, 6, 8, 11, 12, 14, and 18), drawing from validated frameworks [22].
Results
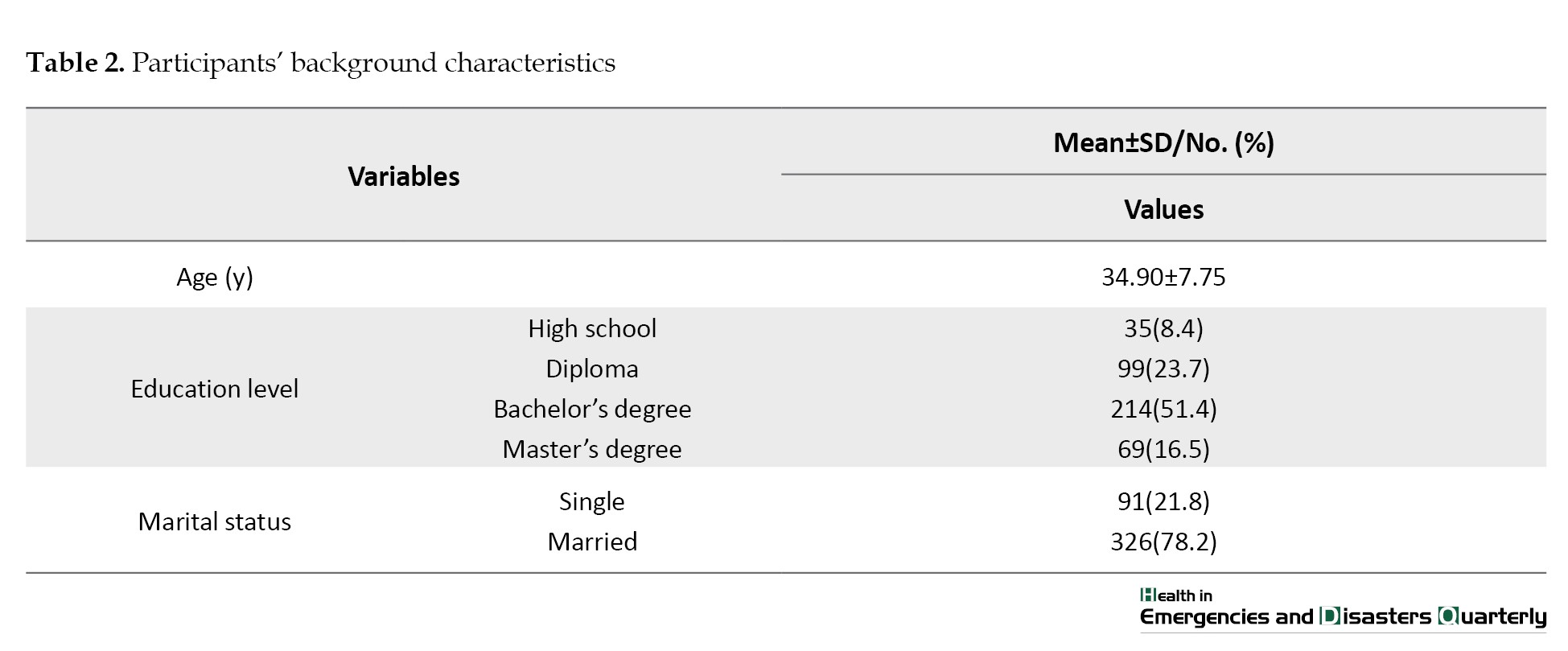
Out of 475 women invited to join the study, 417 submitted fully completed surveys, achieving a participation rate of 87.78%. The average age among these respondents was 34.90 years, with a standard deviation of 7.75 years, ranging from a 16-year-old girl as the youngest to a 57-year-old woman as the oldest. A considerable number of participants held advanced educational qualifications, and 78.2% were in marital relationships. These background details are summarized in Table 2.
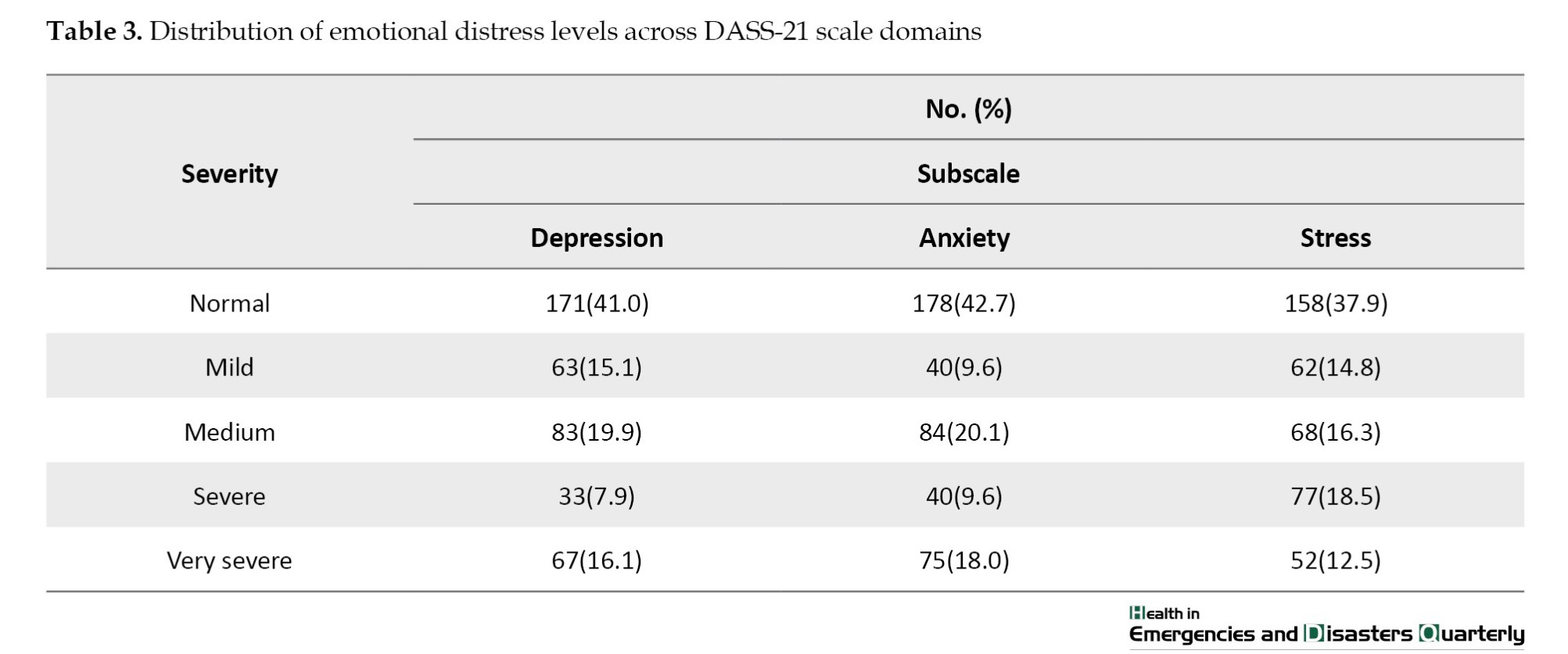
Evaluation of the DASS-21 responses revealed that around 41% of the women maintained emotional equilibrium in terms of depression, while the remainder showed varying levels of depressive symptoms. On the anxiety measure, approximately 18% experienced extremely elevated levels, and on the stress dimension, 31% reported levels ranging from severe to very severe. These findings are detailed in Table 3.
Further statistical exploration using ANOVA indicated no substantial association between age and depression (P=0.750), anxiety (P=0.541), or stress (P=0.418). Additionally, chi-square analyses showed no significant relationships between educational level or marital status and these psychological indicators. Further statistical exploration using ANOVA indicated no substantial link between age and the emotional domains of depression (P=0.750), anxiety (P=0.541), or stress (P=0.418). Additionally, the chi-square test showed no notable associations between educational attainment or marital status and these psychological indicators.
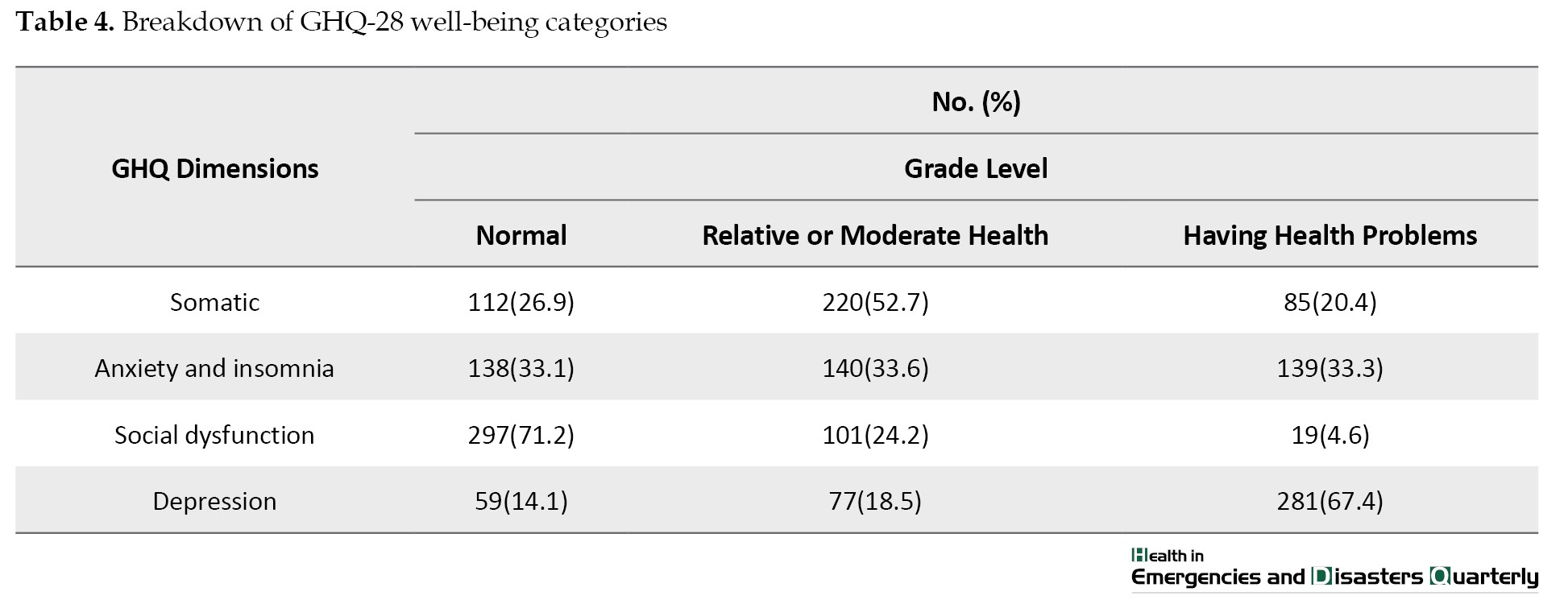
The GHQ-28 yielded an overall Mean±SD of 47.68±12.07, pointing to repeated disruptions in the mental well-being of the participants. Specifically, 20.4% of the women reported bodily discomforts, 33.3% faced challenges with sleep and anxiety, while a mere 4.6% encountered persistent difficulties in social or occupational interactions. In stark contrast, 67.4% showed signs of depressive tendencies (Table 4).
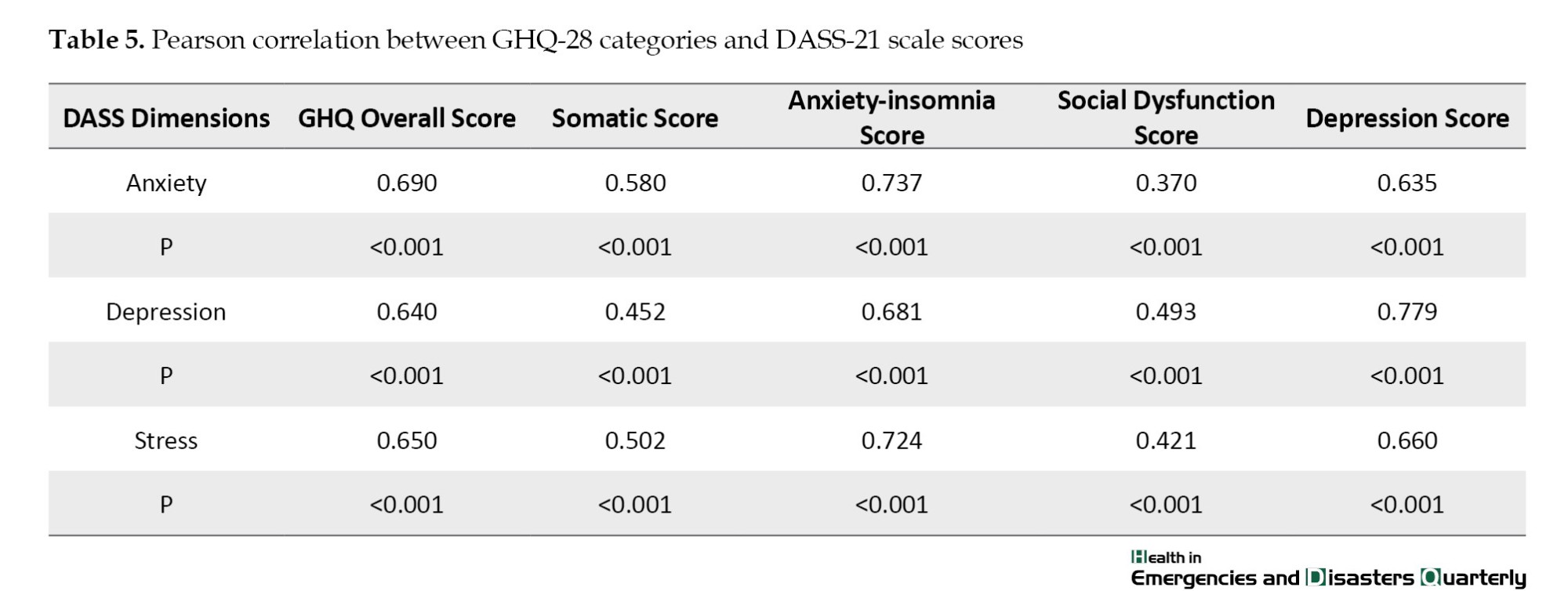
Pearson’s correlation analysis uncovered a strong connection (P<0.001) between the total GHQ-28 score and the emotional distress measures of anxiety, depression, and stress. Notably, a one-unit increase in the GHQ-28 average corresponded to a 0.690-unit rise in anxiety levels. A comparable association was evident with depression, marked by a correlation coefficient of 0.640. Across all evaluated aspects, a direct and statistically robust relationship emerged between the GHQ-28 subscale scores and the DASS-21 indicators of emotional strain, as detailed in Table 5.
Discussion
This study explored the association between overall health and the degrees of DASS-21 experienced by women attending health centers during the COVID-19 outbreak. Our results indicated that 41% of the participants exhibited normal depression levels, whereas 18% reported extremely severe anxiety, and 31% experienced stress ranging from severe to very severe. In a study conducted by Verma and Mishra (2020) among an Indian cohort, they observed that 25% of individuals displayed moderate to severe depression, 28% had anxiety, and 18.6% faced stress, underscoring the urgent need to bolster mental health support systems [23]. Similarly, a systematic review and meta-analysis by Salari et al. (2020) reported prevalence rates of 31.9% for anxiety and 33.7% for depression. Although our study—focused solely on women visiting healthcare centers—did not reveal a statistically significant relationship between demographic characteristics and psychological distress, some studies conducted on both genders have shown mixed results. For instance, Montano et al. did not find significant differences between women’s and men’s distress levels, a discrepancy that may be attributed to cultural variations in gender roles and caregiving responsibilities [24]. In contrast to some prior research, our study did not establish a statistically significant relationship between demographic characteristics (age, education, and marital status) and psychological distress. Elbay et al. (2020) found no substantial differences between men’s and women’s psychological distress levels during the pandemic, a discrepancy that may be attributed to cultural and social variations in caregiving responsibilities [25]. Othman’s research identified female gender as a key independent factor contributing to elevated DASS-21 levels [26].
A trend supported by Alamri et al. (2020), who noted greater distress among women, younger individuals, and those single or unemployed [27]. Additionally, another study by Othman reinforced the role of the female sex in predicting elevated psychological distress [26]. However, in our research, where most participants were married, no meaningful connections emerged between demographic factors and emotional distress, diverging from these earlier findings [27]. Our average well-being score of 47.68 indicated that 20.4% of women experienced physical ailments alongside prevalent sleep and anxiety issues. A robust, statistically significant link (P<0.001) was evident between overall wellness and emotional challenges, though no such associations appeared with demographic variables. Comparatively, Varma et al. (2021) found that younger age groups are more susceptible to emotional turmoil, with disrupted sleep, reduced adaptability, youth, and isolation intensifying the relationships between stress, depression, and anxiety [28]. Consistent with their work, we noted sleep difficulties among participants, with the strong association between insomnia and anxiety likely stemming from ongoing tension due to pandemic uncertainties. Such sleep disturbances amplify emotional struggles, creating a harmful cycle that diminishes overall health. The heightened prevalence of anxiety and stress in our sample underscores the profound psychological impact of the COVID-19 outbreak on women, potentially exacerbated by disrupted routines, financial pressures, and increased caregiving responsibilities. Furthermore, our finding that women with lower wellness scores reported greater emotional distress corroborates prior evidence of a reciprocal relationship between physical and mental health [15]. A notable constraint of this study is its exclusive focus on women at health centers, limiting gender comparisons, coupled with a sample size that may not fully represent broader trends. The lack of demographic correlations suggests the need for context-specific interpretations of these psychological patterns.
Conclusion
This study highlights the significant toll that global disruptions, such as pandemics, take on women’s psychological well-being, showing that a large share of women attending health facilities faced heightened levels of anxiety, stress, and depressive symptoms. A meaningful connection was uncovered between overall wellness and these emotional struggles, with those registering higher wellness scores also noting increased psychological distress. By focusing on women during the COVID-19 outbreak, this work highlights their particular vulnerability to mental health difficulties. The application of trusted tools, such as the GHQ-28 and DASS-21, reinforces the trustworthiness of the results, laying a strong numerical foundation. Conducting this research amid a pandemic offers timely insights, stressing the critical need for personalized mental health assistance. The pronounced link between general wellness and emotional difficulties, like anxiety and depression, points to essential areas for targeted action, providing a detailed perspective on the psychological hardships women encounter during turbulent times.
These findings underline the pressing need to focus on women’s mental wellness, especially in the face of worldwide emergencies. Pinpointing those at risk of psychological issues across diverse societal segments is key to preserving and boosting mental resilience through effective strategies and methods. Leaders and mental health specialists should craft and implement specific measures to avert and ease the emotional consequences of such events. Moreover, enhancing community awareness of anxiety, stress, and depression while promoting practical coping skills could uplift women’s psychological health and diminish the adverse effects of global crises. Integrating mental health priorities into emergency planning and public health systems may reduce the lasting emotional burden on at-risk groups, cultivating greater strength for future trials.
Although this study offers valuable perspectives on women’s mental health during the COVID-19 crisis, its reach is tempered by certain drawbacks. Its one-time, cross-sectional nature captures only a momentary glimpse, hindering the ability to determine causal ties. Additionally, the sample was limited to women using healthcare services in a single locale, which may not mirror the wider female populace. Differences in economic circumstances, cultural backgrounds, and access to care might affect how widely these results apply to other regions or communities.
Even with these limitations on broader relevance, the study’s core ideas and primary findings—such as the connection between wellness and emotional distress—provide a stepping stone for similar investigations elsewhere. A key aim was to evaluate the local setting and the social-cultural factors shaping women’s mental health in Larestan, deepening insight into its specific challenges and supporting more customized healthcare approaches. This work builds a firm foundation for exploring how general and psychological health intertwine during crises. It emphasizes the importance of integrating mental health support into everyday care settings, particularly for groups like women who are more exposed to risk. Moving forward, studies with a long-term focus and wider participant diversity are advised to enhance applicability and investigate the persistent psychological impacts of global upheavals.
Limitation
This investigation faces certain limitations. Its snapshot methodology captures only a single instance in time, which restricts the ability to determine causal links. Consequently, the outcomes may not be widely applicable to all individuals. Furthermore, the reliance on participants’ self-provided answers opens the door to potential biases, such as a tendency to give socially acceptable responses, which might affect the accuracy of the findings.
Suggestions
1) Health systems should implement targeted mental health programs specifically aimed at women during crises. These interventions could include counseling, stress management workshops, and psychoeducation to mitigate anxiety, depression, and stress; 2) strengthening community networks and peer support systems could help women cope with increased caregiving burdens and isolation during pandemics, thereby reducing their mental health risks; 3) mental health screenings and services should be integrated into routine healthcare visits, especially during global health emergencies, to identify and support at-risk women early; 4) increasing awareness of mental health, reducing stigma, and promoting healthy coping mechanisms through public campaigns would empower women to seek help when needed; 5) additional long-term studies are encouraged to explore the enduring emotional impacts of worldwide emergencies on women while also identifying further elements that either increase vulnerability or enhance psychological strength.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Larestan Medical University, Lar, Iran (Code: IR.LARUMS.REC.1399.015). All participants completed the survey voluntarily, without any obligation.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and methodology: Mohammadreza Shafiei and Zahra Keshtkaran; Software, visualization, project administration and writing the original draft: Mohammadreza Shafiei; Validation and resources: Zahra Keshtkaran; Formal Analysis: Mohammadreza Shafiei and Hamed Delam; Investigation: Raziyeh Rahmati and Mohammadreza Shafiei; Data collection: Raziyeh Rahmati and Hamed Delam; Supervision: Zahra Keshtkaran; Review & editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to express their gratitude to all participants who voluntarily took part in this study and generously shared their time and experiences.
Pandemics, as worldwide emergencies, significantly alter numerous aspects of human existence, with mental well-being emerging as a key area of concern. Women, often more susceptible due to their extensive social and family duties, caregiving obligations, and distinct physical and emotional traits, encounter intensified psychological difficulties during such crises. These factors collectively increase their risk for conditions, such as depression and anxiety [1, 2]. If not addressed, these conditions can profoundly impair individuals by diminishing their quality of life, straining personal connections, and increasing their predisposition to physical ailments. Moreover, persistent stress linked to these psychological states can compromise immune function, further intensifying their vulnerabilities [2].
Studies underscore the substantial effect of pandemics on women’s psychological health, driven largely by disruptions in everyday routines, including heightened societal and financial burdens, limitations on physical and social interactions, and changes in sleep and dietary habits [3, 4]. For instance, during the SARS epidemic, women faced heightened stress and depressive symptoms due to limited social interactions, mandatory isolation, evolving family dynamics, and greater demands from domestic and caregiving tasks [5]. Similarly, the Zika pandemic has raised severe mental health concerns among pregnant women, driven by fear of the potential adverse effects of the virus on the fetus. This anxiety not only impacts mothers’ mental health but also influences their decisions regarding pregnancy and medical care. [6].
Historical pandemics, such as the Spanish Flu and SARS have revealed similar patterns. Women, particularly pregnant women, were more vulnerable to depression and anxiety due to societal pressures, physical limitations, and changing gender roles [7, 8]. Evidence also suggests that women are more likely to experience post-traumatic stress disorder (PTSD) during such events; a SARS-era study, for instance, found that women were more predisposed to PTSD than men [9]. Additionally, during the H1N1 pandemic, pregnant women and young mothers faced an elevated risk of anxiety and depressive disorders [10].
The COVID-19 pandemic, as the latest global health crisis, has caused rapid increases in infections and deaths worldwide, including Iran, where its spread was confirmed on February 29, 2020 [11, 12]. This pandemic has significantly disrupted economies, politics, and societies globally, leading to increased mental health challenges across various population groups, including women, healthcare workers, children, students, and families [13, 14]. Psychological challenges, including anxiety, stress, and depression, have surged during this period. For example, research on patients admitted for COVID-19-related respiratory issues revealed markedly higher anxiety and depression levels compared to those with other respiratory conditions, like pneumonia [15].
Given the complex effects of pandemics on women’s mental health, identifying those at risk of psychological disorders and introducing suitable interventions to bolster their well-being is essential [16]. Maintaining mental health during crises is essential as individuals, including patients, healthcare workers, and family members, face stressors directly linked to the pandemic [17, 18]. Evidence highlights the importance of studying women’s mental health during such events, pinpointing risk and protective factors, and crafting effective strategies for prevention and support to lessen the psychological toll of these crises [18].
Given these vulnerabilities, it is essential to investigate the emotional effects of pandemics on women to identify potential risk elements, develop preventive strategies, and create targeted support measures. This research aimed to explore the relationship between overall health and the presence of depression, anxiety, and stress (DASS-21) in women utilizing healthcare services amid the COVID-19 outbreak. By addressing this urgent issue, our goal was to provide research-supported recommendations for policymakers and mental health professionals to mitigate the psychological impacts of such crises.
Materials and Methods
This study was designed as a descriptive-analytical inquiry within a cross-sectional framework and was conducted throughout 2021. It involved women who attended health facilities affiliated with the Larestan Faculty of Medical Sciences. The process began by assembling a detailed directory of these centers, with each facility’s name inscribed on a separate piece of paper. These were then sealed in individual envelopes, and ten were picked at random. The research team visited these designated sites, employing a practical sampling approach while ensuring alignment with specific inclusion and exclusion criteria.
To calculate the required number of participants, a statistical method based on the mean sample size was utilized. With a confidence level set at 95% and a margin of error of 0.09 standard deviation, the study aimed to recruit approximately 475 women. Eligibility required a voluntary agreement to participate, the ability to read and write, and possession of a digital device—such as a smartphone, tablet, or laptop—to access the online survey. Women were excluded if they submitted partially completed forms, opted out during the study, had a history of severe or persistent mental health issues, or had experienced significant emotional turmoil in the preceding six months, such as the loss of a family member, marital changes, or a diagnosis of a terminal condition.
Data collection was done using three tools: one to gather personal background details, another to assess overall well-being, and a third to measure emotional strain. Personal details included participants’ age, educational background, and marital status.
Research design
The investigation followed a cross-sectional, descriptive-analytical model and took place in 2021.
Study context
The focus was on women utilizing healthcare services at centers affiliated with the Larestan Faculty of Medical Sciences.
Timing and location
The fieldwork occurred in 2021 within health facilities governed by the Larestan Faculty of Medical Sciences.
Participants
The sample consisted of women who visited the chosen health centers during the research period.
Sample size determination
A mean-based calculation method was applied, factoring in a 95% confidence interval and a 0.09 standard deviation error margin, targeting a total of 475 participants.
Selection procedure
A complete inventory of health centers linked to the Larestan Faculty of Medical Sciences was first created, with each center’s name noted on individual slips of paper. These slips were placed into envelopes, and ten were randomly selected. Researchers then visited these locations, using an accessible sampling technique while adhering to predefined participation criteria.
Inclusion criteria
1) Willingness to take part voluntarily; 2) basic proficiency in reading and writing; 3) ownership of a device (e.g. smartphone, tablet, or computer) to complete the digital survey.
Exclusion criteria
1) Failure to fully complete the survey; 2) choosing to withdraw from the study before completion; 3) history of acute or ongoing psychiatric disorders; 4) recent significant emotional distress within the past six months (e.g. bereavement, divorce, marriage, or severe illness).
Assessment tools
Three instruments were employed:
1) Personal information form: This recorded details, such as age, education level, and marital status; 2) General health questionnaire–28 (GHQ-28): This tool was developed by Goldberg in 1978 [19]. It has 28 questions grouped into four categories, each containing eight items. Participants rated each question on a four-point scale, with scores ranging from 0 to 3 based on a Likert system. The total score was calculated by adding the results from all four categories, where lower scores indicated better well-being and higher scores suggested greater impairment. The categories cover physical complaints (items 1-7), anxiety and sleep disturbances (items 8-14), social challenges (items 15-21), and depressive tendencies (items 22-28), with a maximum possible score of 84. Its reliability was validated by Ebrahimi et al. with a consistency coefficient of 0.88 [20]. 2) physical Complaints Category: Scores of 0-9 reflect robust physical health despite psychosomatic issues, 10-15 suggest moderate well-being, and 16-21 indicate pronounced psychosomatic symptoms. 3) anxiety and sleep category: Scores of 0-9 signify a calm and controlled state, 10-15 imply occasional anxiety, and 16-21 point to intense anxiety in various contexts. 4) social Challenges Category: Scores of 0-9 denote strong interpersonal and workplace functioning, 10-15 reflect moderate social health, and 16-21 indicate persistent relational or work-related struggles. 5) depression category: Scores of 0-9 suggest vitality and positivity in daily life, 10-15 indicate occasional low mood, and 16-21 signal a probable depressive state. 6) total score interpretation: A range of 0-21 reflects excellent mental well-being, 22-42 suggests some areas of concern, 43-63 indicates repeated mental health difficulties, and 64-84 points to a severe condition. 7) Emotional strain assessment (DASS-21): This tool consists of 21 questions divided into three sets of seven, each targeting a distinct emotional domain. Scores are derived by summing responses within each set, with ratings from 0 (not relevant to me) to 3 (highly relevant). As a condensed version of the original 42-item tool, each set’s score is doubled, and severity is evaluated using established thresholds (Table 1).
Its suitability for Iranian contexts was confirmed by Afzali et al. with reliability scores of 0.81 for depression, 0.73 for anxiety, and 0.81 for stress [21].
The tools were hosted on Google Forms, and access links were shared with qualifying participants via SMS and WhatsApp. The collected data were organized and encoded by the research team and then analyzed using SPSS software, version 25. Statistical methods included the independent t-test, chi-square test, and analysis of variance (ANOVA), adjusted for data normality, with a significance threshold of 5%. The DASS-21 measures three emotional dimensions: Depression (items 3, 5, 10, 13, 16, 17, and 21), anxiety (items 2, 4, 9, 15, 19, and 20), and stress (items 1, 6, 8, 11, 12, 14, and 18), drawing from validated frameworks [22].
Results
Out of 475 women invited to join the study, 417 submitted fully completed surveys, achieving a participation rate of 87.78%. The average age among these respondents was 34.90 years, with a standard deviation of 7.75 years, ranging from a 16-year-old girl as the youngest to a 57-year-old woman as the oldest. A considerable number of participants held advanced educational qualifications, and 78.2% were in marital relationships. These background details are summarized in Table 2.
Evaluation of the DASS-21 responses revealed that around 41% of the women maintained emotional equilibrium in terms of depression, while the remainder showed varying levels of depressive symptoms. On the anxiety measure, approximately 18% experienced extremely elevated levels, and on the stress dimension, 31% reported levels ranging from severe to very severe. These findings are detailed in Table 3.
Further statistical exploration using ANOVA indicated no substantial association between age and depression (P=0.750), anxiety (P=0.541), or stress (P=0.418). Additionally, chi-square analyses showed no significant relationships between educational level or marital status and these psychological indicators. Further statistical exploration using ANOVA indicated no substantial link between age and the emotional domains of depression (P=0.750), anxiety (P=0.541), or stress (P=0.418). Additionally, the chi-square test showed no notable associations between educational attainment or marital status and these psychological indicators.
The GHQ-28 yielded an overall Mean±SD of 47.68±12.07, pointing to repeated disruptions in the mental well-being of the participants. Specifically, 20.4% of the women reported bodily discomforts, 33.3% faced challenges with sleep and anxiety, while a mere 4.6% encountered persistent difficulties in social or occupational interactions. In stark contrast, 67.4% showed signs of depressive tendencies (Table 4).
Pearson’s correlation analysis uncovered a strong connection (P<0.001) between the total GHQ-28 score and the emotional distress measures of anxiety, depression, and stress. Notably, a one-unit increase in the GHQ-28 average corresponded to a 0.690-unit rise in anxiety levels. A comparable association was evident with depression, marked by a correlation coefficient of 0.640. Across all evaluated aspects, a direct and statistically robust relationship emerged between the GHQ-28 subscale scores and the DASS-21 indicators of emotional strain, as detailed in Table 5.
Discussion
This study explored the association between overall health and the degrees of DASS-21 experienced by women attending health centers during the COVID-19 outbreak. Our results indicated that 41% of the participants exhibited normal depression levels, whereas 18% reported extremely severe anxiety, and 31% experienced stress ranging from severe to very severe. In a study conducted by Verma and Mishra (2020) among an Indian cohort, they observed that 25% of individuals displayed moderate to severe depression, 28% had anxiety, and 18.6% faced stress, underscoring the urgent need to bolster mental health support systems [23]. Similarly, a systematic review and meta-analysis by Salari et al. (2020) reported prevalence rates of 31.9% for anxiety and 33.7% for depression. Although our study—focused solely on women visiting healthcare centers—did not reveal a statistically significant relationship between demographic characteristics and psychological distress, some studies conducted on both genders have shown mixed results. For instance, Montano et al. did not find significant differences between women’s and men’s distress levels, a discrepancy that may be attributed to cultural variations in gender roles and caregiving responsibilities [24]. In contrast to some prior research, our study did not establish a statistically significant relationship between demographic characteristics (age, education, and marital status) and psychological distress. Elbay et al. (2020) found no substantial differences between men’s and women’s psychological distress levels during the pandemic, a discrepancy that may be attributed to cultural and social variations in caregiving responsibilities [25]. Othman’s research identified female gender as a key independent factor contributing to elevated DASS-21 levels [26].
A trend supported by Alamri et al. (2020), who noted greater distress among women, younger individuals, and those single or unemployed [27]. Additionally, another study by Othman reinforced the role of the female sex in predicting elevated psychological distress [26]. However, in our research, where most participants were married, no meaningful connections emerged between demographic factors and emotional distress, diverging from these earlier findings [27]. Our average well-being score of 47.68 indicated that 20.4% of women experienced physical ailments alongside prevalent sleep and anxiety issues. A robust, statistically significant link (P<0.001) was evident between overall wellness and emotional challenges, though no such associations appeared with demographic variables. Comparatively, Varma et al. (2021) found that younger age groups are more susceptible to emotional turmoil, with disrupted sleep, reduced adaptability, youth, and isolation intensifying the relationships between stress, depression, and anxiety [28]. Consistent with their work, we noted sleep difficulties among participants, with the strong association between insomnia and anxiety likely stemming from ongoing tension due to pandemic uncertainties. Such sleep disturbances amplify emotional struggles, creating a harmful cycle that diminishes overall health. The heightened prevalence of anxiety and stress in our sample underscores the profound psychological impact of the COVID-19 outbreak on women, potentially exacerbated by disrupted routines, financial pressures, and increased caregiving responsibilities. Furthermore, our finding that women with lower wellness scores reported greater emotional distress corroborates prior evidence of a reciprocal relationship between physical and mental health [15]. A notable constraint of this study is its exclusive focus on women at health centers, limiting gender comparisons, coupled with a sample size that may not fully represent broader trends. The lack of demographic correlations suggests the need for context-specific interpretations of these psychological patterns.
Conclusion
This study highlights the significant toll that global disruptions, such as pandemics, take on women’s psychological well-being, showing that a large share of women attending health facilities faced heightened levels of anxiety, stress, and depressive symptoms. A meaningful connection was uncovered between overall wellness and these emotional struggles, with those registering higher wellness scores also noting increased psychological distress. By focusing on women during the COVID-19 outbreak, this work highlights their particular vulnerability to mental health difficulties. The application of trusted tools, such as the GHQ-28 and DASS-21, reinforces the trustworthiness of the results, laying a strong numerical foundation. Conducting this research amid a pandemic offers timely insights, stressing the critical need for personalized mental health assistance. The pronounced link between general wellness and emotional difficulties, like anxiety and depression, points to essential areas for targeted action, providing a detailed perspective on the psychological hardships women encounter during turbulent times.
These findings underline the pressing need to focus on women’s mental wellness, especially in the face of worldwide emergencies. Pinpointing those at risk of psychological issues across diverse societal segments is key to preserving and boosting mental resilience through effective strategies and methods. Leaders and mental health specialists should craft and implement specific measures to avert and ease the emotional consequences of such events. Moreover, enhancing community awareness of anxiety, stress, and depression while promoting practical coping skills could uplift women’s psychological health and diminish the adverse effects of global crises. Integrating mental health priorities into emergency planning and public health systems may reduce the lasting emotional burden on at-risk groups, cultivating greater strength for future trials.
Although this study offers valuable perspectives on women’s mental health during the COVID-19 crisis, its reach is tempered by certain drawbacks. Its one-time, cross-sectional nature captures only a momentary glimpse, hindering the ability to determine causal ties. Additionally, the sample was limited to women using healthcare services in a single locale, which may not mirror the wider female populace. Differences in economic circumstances, cultural backgrounds, and access to care might affect how widely these results apply to other regions or communities.
Even with these limitations on broader relevance, the study’s core ideas and primary findings—such as the connection between wellness and emotional distress—provide a stepping stone for similar investigations elsewhere. A key aim was to evaluate the local setting and the social-cultural factors shaping women’s mental health in Larestan, deepening insight into its specific challenges and supporting more customized healthcare approaches. This work builds a firm foundation for exploring how general and psychological health intertwine during crises. It emphasizes the importance of integrating mental health support into everyday care settings, particularly for groups like women who are more exposed to risk. Moving forward, studies with a long-term focus and wider participant diversity are advised to enhance applicability and investigate the persistent psychological impacts of global upheavals.
Limitation
This investigation faces certain limitations. Its snapshot methodology captures only a single instance in time, which restricts the ability to determine causal links. Consequently, the outcomes may not be widely applicable to all individuals. Furthermore, the reliance on participants’ self-provided answers opens the door to potential biases, such as a tendency to give socially acceptable responses, which might affect the accuracy of the findings.
Suggestions
1) Health systems should implement targeted mental health programs specifically aimed at women during crises. These interventions could include counseling, stress management workshops, and psychoeducation to mitigate anxiety, depression, and stress; 2) strengthening community networks and peer support systems could help women cope with increased caregiving burdens and isolation during pandemics, thereby reducing their mental health risks; 3) mental health screenings and services should be integrated into routine healthcare visits, especially during global health emergencies, to identify and support at-risk women early; 4) increasing awareness of mental health, reducing stigma, and promoting healthy coping mechanisms through public campaigns would empower women to seek help when needed; 5) additional long-term studies are encouraged to explore the enduring emotional impacts of worldwide emergencies on women while also identifying further elements that either increase vulnerability or enhance psychological strength.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Larestan Medical University, Lar, Iran (Code: IR.LARUMS.REC.1399.015). All participants completed the survey voluntarily, without any obligation.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and methodology: Mohammadreza Shafiei and Zahra Keshtkaran; Software, visualization, project administration and writing the original draft: Mohammadreza Shafiei; Validation and resources: Zahra Keshtkaran; Formal Analysis: Mohammadreza Shafiei and Hamed Delam; Investigation: Raziyeh Rahmati and Mohammadreza Shafiei; Data collection: Raziyeh Rahmati and Hamed Delam; Supervision: Zahra Keshtkaran; Review & editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to express their gratitude to all participants who voluntarily took part in this study and generously shared their time and experiences.
References
- Damian AC, Ciobanu AM, Anghele C, Papacocea IR, Manea MC, Iliuță FP, et al. Caregiving for dementia patients during the coronavirus pandemic. Journal of Clinical Medicine. 2023; 12(7):2616. [DOI:10.3390/jcm12072616] [PMID]
- Bahall M, Bailey H. The impact of chronic disease and accompanying bio-psycho-social factors on health-related quality of life. Journal of Family Medicine and Primary Care. 2022; 11(8):4694-704. [DOI:10.4103/jfmpc.jfmpc_2399_21] [PMID]
- do Carmo SG, Oliveira JPT, Aragão BdA, Botelho PB. Impact of final phase social isolation and the Covid-19 pandemic on eating behavior, sleep quality, and anxiety level. Nutrients. 2023; 15(9):2148. [DOI:10.3390/nu15092148] [PMID]
- Foroughi N, Hay P, Mannan H. Community women’s lifestyle and eating disorders in the era of COVID-19 pandemic: A 15-year follow-up study. Nutrients. 2023; 15(7):1676. [DOI:10.3390/nu15071676] [PMID]
- Almeida M, Shrestha AD, Stojanac D, Miller LJ. The impact of the COVID-19 pandemic on women’s mental health. Archives of Women’s Mental Health. 2020; 23(6):741-8.[DOI:10.1007/s00737-020-01092-2] [PMID]
- Ceulemans M, Foulon V, Ngo E, Panchaud A, Winterfeld U, Pomar L, et al. Mental health status of pregnant and breastfeeding women during the COVID‐19 pandemic-A multinational cross‐sectional study. Acta Obstetricia et Gynecologica Scandinavica. 2021; 100(7):1219-29. [DOI:10.1111/aogs.14092] [PMID]
- Zilver S, Broekman B, Hendrix Y, De Leeuw R, Mentzel S, Van Pampus M, et al. Stress, anxiety and depression in 1466 pregnant women during and before the COVID-19 pandemic: A Dutch cohort study. Journal of Psychosomatic Obstetrics & Gynecology. 2021; 42(2):108-14. [DOI:10.1080/0167482X.2021.1907338] [PMID]
- Xiong J, Lipsitz O, Nasri F, Lui LM, Gill H, Phan L, et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. Journal of Affective Disorders. 2020; 277:55-64. [DOI:10.1016/j.jad.2020.08.001] [PMID]
- Kaugars AS, Zemlak J, Oswald DL. Impact of the COVID-19 pandemic on US women’s mental health. Journal of Women’s Health. 2023; 32(11):1166-73. [DOI:10.1089/jwh.2023.0253] [PMID]
- Ahmad M, Vismara L. The psychological impact of COVID-19 pandemic on women’s mental health during pregnancy: A rapid evidence review. International Journal of Environmental Research and Public Health. 2021; 18(13):7112. [DOI:10.3390/ijerph18137112] [PMID]
- Zhigaleva OgN, Ermolaev I, Mardanly S, Gashenko TY. Analysis of the domestic market for COVID-19 diagnostic kits by real-time reverse-transcription polymerase chain reaction. Klinicheskaia Laboratornaia Diagnostika. 2022; 67(11):672-7. [DOI:10.51620/0869-2084-2022-67-11-672-677] [PMID]
- Mazaherifar S, Solhjoo K, Abdoli A. Outbreak of cutaneous leishmaniasis before and during the COVID-19 pandemic in Jahrom, an endemic region in the southwest of Iran. Emerging Microbes & Infections. 2022; 11(1):2218-21. [DOI:10.1080/22221751.2022.2117099] [PMID]
- Bao Y, Sun Y, Meng S, Shi J, Lu L. 2019-nCoV epidemic: Address mental health care to empower society. The lancet. 2020; 395(10224):e37-e8. [DOI:10.1016/S0140-6736(20)30309-3] [PMID]
- Chen Q, Liang M, Li Y, Guo J, Fei D, Wang L, et al. Mental health care for medical staff in China during the COVID-19 outbreak. The Lancet Psychiatry. 2020; 7(4):e15-e6. [DOI:10.1016/S2215-0366(20)30078-X] [PMID]
- Yang L, Wu D, Hou Y, Wang X, Dai N, Wang G, et al. Analysis of psychological state and clinical psychological intervention model of patients with COVID-19. MedRxiv. 2020:2020.03 [Unpublished]. [DOI:10.1101/2020.03.22.20040899]
- Ryff CD, Singer B. The contours of positive human health. Psychological Inquiry. 1998; 9(1):1-28. [DOI:10.1207/s15327965pli0901_1]
- Shahyad S, Mohammadi MT. [Psychological impacts of Covid-19 outbreak on mental health status of society individuals: A narrative review (Persian)]. Journal of Military Medicine. 2020; 22(2):184-92. [DOI:10.30491/JMM.22.2.184]
- Wang L, Nabi G, Zuo L, Wu Y, Li D. Impacts of the COVID-19 pandemic on mental health and potential solutions in different members in an ordinary family unit. Frontiers in Psychiatry. 2022; 12:735653. [DOI:10.3389/fpsyt.2021.735653] [PMID]
- Goldberg P. The detection of psychiatric illness by questionnaire. Oxford: Oxford University Press; 1972. [Link]
- Ebrahimi A, Molavi H, Mossavi G, Bornamanesh A, Yaghobi M. [Psychometric properties and factor structure of General Health Questionnaire 28 (GHQ-28) in Iranian psychiatric patients (Persian)]. Journal of Research in Behavioural Sciences. 2007; 5(1):5-12. [Link]
- Afzali A, Delavar A, Borjali A, Mirzamani M. [Psychometric properties of DASS-42 as assessed in a sample of Kermanshah High School students (Persian)]. Journal of Research in Behavioural Sciences. 2007; 5(2):81-92. [Link]
- Sharifi A, Fallahi-Khoshknab M, Mohammadi S, Zeraati M, Jamshidi Z, Aghabeygi-Arani M, et al. Depression, anxiety, and stress among Iranian nurses in COVID-19 care wards. BMC Psychology. 2022; 10(1):205. [DOI:10.1186/s40359-022-00911-8]
- Verma S, Mishra A. Depression, anxiety, and stress and socio-demographic correlates among general Indian public during COVID-19. International Journal of Social Psychiatry. 2020; 66(8):756-62. [DOI:10.1177/0020764020934508] [PMID]
- Salari N, Hosseinian-Far A, Jalali R, Vaisi-Raygani A, Rasoulpoor S, Mohammadi M, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Globalization and Health. 2020; 16(1):57. [DOI:10.20525/ijrbs.v9i4.773]
- Elbay RY, Kurtulmuş A, Arpacıoğlu S, Karadere E. Depression, anxiety, stress levels of physicians and associated factors in Covid-19 pandemics. Psychiatry Research. 2020; 290:113130. [DOI:10.1016/j.psychres.2020.113130] [PMID]
- Othman N. Depression, anxiety, and stress in the time of COVID-19 pandemic in Kurdistan region, Iraq. Kurdistan Journal of Applied Research. 2020. 5(3):37-44. [DOI:10.24017/covid.5]
- Alamri HS, Algarni A, Shehata SF, Al Bshabshe A, Alshehri NN, ALAsiri AM, et al. Prevalence of depression, anxiety, and stress among the general population in Saudi Arabia during Covid-19 pandemic. International Journal of Environmental Research and Public Health. 2020; 17(24):9183. [DOI:10.3390/ijerph17249183] [PMID]
- Varma P, Junge M, Meaklim H, Jackson ML. Younger people are more vulnerable to stress, anxiety and depression during COVID-19 pandemic: A global cross-sectional survey. Progress in Neuro-Psychopharmacology and Biological Psychiatry. 2021; 109:110236. [DOI:10.1016/j.pnpbp.2020.110236] [PMID]
Type of article: Research |
Subject:
General
Received: 2024/09/5 | Accepted: 2025/04/5 | Published: 2026/01/29
Received: 2024/09/5 | Accepted: 2025/04/5 | Published: 2026/01/29
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
