

Volume 4, Issue 3 (Spring 2019)
Health in Emergencies and Disasters Quarterly 2019, 4(3): 127-134 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Saeid M, Khankeh H, Habibisoola A, Mohammadali M, Hamidkolg G, Dadkhah B. Investigating Hospital Preparedness in Ardabil Province Against Unexpected Accidents. Health in Emergencies and Disasters Quarterly 2019; 4 (3) :127-134
URL: http://hdq.uswr.ac.ir/article-1-230-en.html
URL: http://hdq.uswr.ac.ir/article-1-230-en.html
Mehri Saeid1 

 , Hamidreza Khankeh2 , Aghil Habibisoola1 , Mohammadi Mohammadali *3 , Gholamreza Hamidkolg4 , Behrouz Dadkhah4
, Hamidreza Khankeh2 , Aghil Habibisoola1 , Mohammadi Mohammadali *3 , Gholamreza Hamidkolg4 , Behrouz Dadkhah4
, Hamidreza Khankeh2 , Aghil Habibisoola1 , Mohammadi Mohammadali *3 , Gholamreza Hamidkolg4 , Behrouz Dadkhah4
1- Department of Nursing, School of Nursing and Midwifery,, Ardabil University of Medical Sciences, Ardabil, Iran.
2- Department of Nursing, University of Social Welfare & Rehabilitation Sciences, Tehran, Iran.
3- Department of Nursing, School of Nursing and Midwifery, Ardabil University of Medical Sciences, Ardabil, Iran. ,habibiarums@gmail.com
4- Department of Nursing, School of Nursing and Midwifery, Ardabil University of Medical Sciences, Ardabil, Iran.
2- Department of Nursing, University of Social Welfare & Rehabilitation Sciences, Tehran, Iran.
3- Department of Nursing, School of Nursing and Midwifery, Ardabil University of Medical Sciences, Ardabil, Iran. ,
4- Department of Nursing, School of Nursing and Midwifery, Ardabil University of Medical Sciences, Ardabil, Iran.
Full-Text [PDF 566 kb]
(2238 Downloads)
| Abstract (HTML) (6001 Views)
Full-Text: (1981 Views)
1. Introduction
Natural (earthquakes, floods, storms, etc.) and human-made (war, nuclear explosions, etc.) disasters affect human life and environment and because of their large scale disrupt the socioeconomic performance of the affected areas [1, 2]. The severity of disasters is rising in the world and resulted in many deaths, diseases, and economic losses [3, 4]. TheA Islamic Republic of Iran, as a developing country with a particular political and geographical situation, is always affected by natural and human-made disasters and is one of the most vulnerable countries in terms of accidents in the world [5]. Ardebil Province is no exception to this issue and is always exposed to unexpected events such as floods, earthquakes, snow, blizzards, droughts, frost, and so on. Based on the earthquake hazard zonation in Iran, Ardabil Province is located in a high to a medium risk area, where the vast earthquakes in the past years causes many deaths and injuries [6].
Vahedparast et al. reported that their study hospitals were not prepared for disasters [7]. While Amerion et al. stated that the surveyed hospitals’ preparedness in response to the crisis was equal to 78.23% in the 11 studied dimensions. This result indicates that the level of readiness of hospitals was desirable in most dimensions [8]. Likewise, Lee et al. reported that 85% of the studied hospitals had emergency plans, 93% a command center and personnel for hospital preparation, and 53% a drug storage control program. Physicians in 80% of hospitals had up-to-date information about their hospital preparedness program, and 94.5% had a regular training program for personnel and maneuvering. However, the overall research data from this study indicate that hospital preparedness plans for disasters in China are at an early stage of development [9].
The most critical issue in disaster management is the health management of the affected-community since disasters always have a significant impact on hygiene, general health, and wellbeing of the stricken community. Hospitals play the most important role in the health system, as they are the basic units to provide healthcare services [10]. Hospitals should have a crisis response program because of their function and front line position in managing the victims of accidents. They have to continue and even increase their activities and perform strong teamwork at the time of accidents [5, 11, 12].
Preparedness is one of the essential stages of the crisis management cycle in pre-disaster and includes all the measures, programs, and activities that enable every organization to respond quickly and effectively in critical situations [10]. Hospital preparedness program, like all other programs, requires an initial survey to determine the strong and weak points of the system. There are studies on the level of preparedness of hospitals in accidents and disasters in other provinces of the country [7, 8, 13]. However, these studies overlooked the level of preparedness of hospitals in Ardabil Province. Thus, the current study assessed the level of preparedness of hospitals in Ardabil Province, Iran, in response to accidents and disasters.
2. Materials and Methods
This research was a descriptive and cross-sectional study. The research setting consisted of all hospitals in Ardabil Province that were selected and studied by total enumeration method. To determine the preparedness of hospitals, the national tool for assessing hospital preparedness in disasters was used. This tool estimates the readiness of a hospital, based on the World Health Organization (WHO) standardized assessment checklist [14] (the customized version for Iran). It was designed to provide an adequate response to medical emergencies and incidents, with an all-hazards approach.
The tool has 91 three-option questions and developed based on 9 key components, as follows: 1. command and control (6 questions); 2. triage (10 questions); 3. human resources (15 questions); 4. communication (9 questions); 5. capacity increase (13 questions); 6. support/logistics management (10 questions); 7. safety and security (11 questions); 8. critical service continuation (8 questions); 9. Post-disaster recovery (9 questions). Score 1 is allocated for the option of under review, score 2 for the option of under performance, and score 3 for the option of completed. In addition to this tool, the general profile of the hospitals was obtained from the general information form of hospitals, which included the hospital name, type, and organizational affiliation, address, telephone, fax, and website, as well as the number of active beds, and hospital occupancy rate.
The applied tool evaluated hospital preparation in 9 key components, each containing a list of necessary measures to assist hospital managers and emergency planners. It includes the following components: 1. Command and control: a decision-making system, which is responsible for activating, coordinating, implementing, and terminating a predetermined program. The desirable performance of the command and control system is essential for the effective management of hospital accidents and emergencies; 2. Communications: clear, accurate, and timely communications are needed to ensure sound decision-making, effective collaboration, public awareness, and public confidence; 3. Safety and security: safety and advanced security mechanisms are essential for an effective response during medical emergencies and incidents; 4. Triage: running patients’ triage operations is required based on the predetermined protocol for the desirable functioning of personnel in the face of high patients’ admission, their management, and care; 5. Increasing capacity: the ability of healthcare facilities to raise their routine capacity to respond to increasing demand for clinical care, which is an essential factor in the planning process of a hospital; 6. Continuation of vital services: An incident should not disturb daily services for essential and surgical services (e.g. emergency care and maternal and child care) that are provided in normal conditions; 7. Human resources: it is necessary to ensure sufficient staff capacity and continuity of efficiency in any incident that increases the need for human resources; 8. Support management: continuity of hospital supplies and supply chains is often underestimated as a challenge during a crisis which requires precise contingency planning and response; 9. Disaster recovery: post-incident recovery planning should be initiated at the same time as responding to the disaster. Quick implementation of the recovery program can help to reduce the long-term impact of a catastrophe on the hospital’s function [15].
Tool scoring
Each of the tool questions has three options; under review, under performance, and completed. It is scored according to the opinions of experts as follows: the option under review: score 1. the option in progress; score 2. The option completed; score 3. Calculating of the level of preparedness in each component is as follows: initially, the scores of options are separately summed up; then, by subtracting the sum of the score of the first option (under review) from the sum of the score of the third option (completed), the preparedness range for each component is obtained. Then, the mentioned range is divided into three sections to determine hospital readiness levels in each component (weak, moderate, and good levels). For example, for the first component (command and control) which has 6 questions, if the sum of the first option answers is 6, the sum of the second option answers is 12, and the sum of the third option answers is 18, then the range of the preparedness for this component is obtained by deducting number 6 (sum of the first options) from 18 (the sum of the third options) which is equal to 12. Next, we divide this range into three parts (equal to 4) to calculate the distance between levels. Therefore, the level of weak preparation of the first component is 6-10, the moderate level of preparation of the first component is 11-14, and the good preparation level of the first component is 18-14.
Also, the total obtainable score of the questionnaire is 273. To assess the overall hospital preparedness, the score ranges from poor preparedness (91-136) to moderate preparedness (137-182), then good preparedness (183-228), and finally to excellent preparedness (229-273). The validity and reliability of the National Assessment Tool for Hospital Preparedness in Accidents and Disasters have been approved in Karimian et al. research. Based on their study, the instrument validity was obtained by content validity method (0.86), and its reliability was calculated using the Cronbach α coefficient (0.83) [14].
After approval of the research project by the Research Council of Ardabil University of Medical Sciences, the researchers referred to the health centers and collected the required information. After providing explanations and obtaining the approval of hospital managers, hospital preparedness was measured using the tools mentioned above. The questionnaire was completed by a crisis management expert of each hospital in the presence of the researcher, and the required supervision was carried out. Eventually, the data collected from the questionnaires were analyzed using descriptive statistics.
3. Results
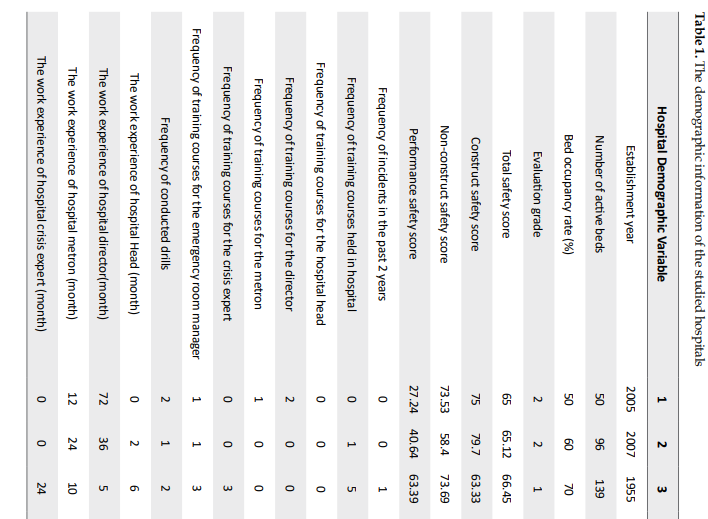
Of 15 hospitals studied, there were two private hospitals, three hospitals affiliated with nongovernmental organizations, and 10 government hospitals affiliated with Ardabil University of Medical Sciences. The latest evaluation grade of the surveyed hospitals was as follows: 4 hospitals were ranked as second-grade, and 11 hospitals were ranked as first-grade. The hospitals were 28.47 years old on average, and Fatemi Hospital, with 94 years old had the most former constructed building. The total number of beds in the surveyed hospitals was 1844, with an average occupancy rate of 67.13% per year.
Over the past two years, only 6 crises have been reported in all of the studied hospitals. They were food poisoning, water supply disconnection, hospital fuse box fire, and electrical wiring fire at the hospital pharmacy, which occurred in 4 of the investigated hospitals. The training courses and drills held included crisis management, fire extinction, table top drill, hazard management, triage, bioterrorism, aircraft crash, the emergency landing of helicopter.
The average records of Head of hospitals, hospital directors, metrons, and crisis experts were 62.77, 85, 62, and 43.37 months, respectively, in this study. Tables 1 and 2 present other information and findings of the present study. It should be noted that numbers 1 to 15 are used instead of hospital names.



According to Table 2, the mean scores of preparedness of hospitals are as follows: good command and control (15 out of 18), moderate communication (17.5 out of 27), moderate security and safety (21.4 out of 33), weak triage (17 out of 30), moderate capacity increase (23.9 out of 39), moderate critical service continuation (14.6 out of 24), weak human resources (24.7 out of 45), moderate support and logistics (17.7 out of 30), and weak recovery after an event (14.4 out of 27). In general, of 15 hospitals examined, by considering the total score of hospital preparedness assessment in 9 studied aspects, 3 hospitals were rated as weak (127, 135, 136 out of 273), 8 as moderate (153, 151, 178, 156, 179, 164, 175, 160 out of 273) and 4 as good (205, 198, 202, 185 out of 273).
4. Discussion
Currently, the crisis response plan is vital for every organization with any activity. Many studies emphasize the importance of having disaster preparedness plans for every individual, society, organization, health center, and in particular for every hospital. Moreover, response programs are more vital for hospitals because of their function and priority in the admission of victims of accidents.
In the present study, according to the obtained mean score in the command and control aspect, the preparedness of studied hospitals was good. The existence of a hospital-based command headquarters, the appointment of a person responsible for each of the 9 components of the hospital’s preparation, registration and keeping all documentation, familiarity with job descriptions for managers and staff, and adequate training in this field were among the reasons for obtaining a high score in this field. This finding of the present study is inconsistent with the results of Ojaghi et al. who rated the preparedness of hospitals in Kermanshah City as weak; the absence of an incident command center may be the reason for their result [16]. Furthermore, Hojjat et al. and Karimian et al. evaluated their studied hospitals moderate with regard to this component that could be due to specific attention to command and control elements [14, 17].
The second most crucial aspect was communication. In the current research, the studied hospitals scored at a moderate level. In this regard, the lack of a person as an interlocutor and spokesperson, lack of drafting of incidents for patients and the public, and inappropriate methods for collecting and analyzing data were among the weak points in communication component. The findings are consistent with the study findings of Daneshmand et al. as well as Karimian et al. [14, 18].
In our research, the investigated hospitals were scored moderate in the area of safety and security. The strong points were the existence of a hospital safety team and the identification of potential hospital vulnerabilities. However the weak points were the lack of required rules for the presence of people at hospital during disasters and accidents; an unreliable method for identifying personnel, patients and visitors; inappropriate methods for coordinating hospital and military rules; and the lack of suitable location for the sterilization of radioactive, biological, and chemical substances and their isolation. This finding is consistent with the research finding by Karimian et al. but is inconsistent with Amrillon et al. [8, 14] findings.
With regard to the triage component, the average score obtained indicated the weakness of studied hospitals in this area. In 4 hospitals, the triage unit was not active at all. Other reasons for weakness in this aspect were the absence of alternative sites for massive triage, no guidelines for admitted injuries, and the lack of a simple mechanism that can trigger an emergency response from an emergency or triage disaster unit, as well as the failure to determine a specific waiting room for patients who are able to walk. This finding is inconsistent with the results of Karimian et al. and Hasanpour et al. studies [14, 19].
In the aspect of increasing the capacity of the hospital during a crisis, the obtained mean score was indicative of the moderate preparedness of the studied hospitals. In this study, the weak points in this area comprised the failure to calculate the required capacity surge and the increase in demand for hospital services in critical situations based on essential resources and manpower and the lack of identification of methods to increase the capacity of hospitalization and no program contracts with other institutions to provide post-mortality care as well as the absence of a contract with places like stadiums and nearby hotels. The existence of a plan to prioritize interventions and the cancellation of non-essential services were the strengths of studied hospitals in this research. These findings are consistent with investigations by Karimian et al. and Kaji and Gravandi [14, 20, 21].
In this research, the studied hospitals achieved a moderate score in the continuation of vital services. The lack of a regular plan for the continuation of essential services, especially for vulnerable groups (children, elderly and disabled individuals); failure to study the impact of accidents on hospital facilities, like water and food; overlooking the availability of essential items; and no coordination with the neighbor hospitals and private physicians to ensure the continuity of essential services were the weak points of this component. Listing and prioritizing the services of the hospital and compiling the essential services were of the strong points of this preparedness component, which is inconsistent with the research findings of Karimian et al. but agree with the findings of Hoseinin Shokooh and Amiri [14, 10, 22].
In addition, in the efficient human resources management, the studied hospitals obtained a weak score. Ignoring the needs of employees and their families during the crisis and inappropriate programs to recruit volunteers and their training and the lack of a multi-task team for the psychological support of the family of staff and patients were the weaknesses of studied hospitals. Possessing a complete list of staff and their information, continuous monitoring of attendance and absenteeism of employees, providing training to staff in the most demanding wards, and considering the vaccination of employees were their strong points. This finding is consistent with the research findings by Karimian and Salari [14, 23].
Moreover, in the research by Amerion the investigated hospitals were influential in terms of human resources [8]. Considering that human resources always play an essential role in the management of hospital services, using skilled and trained staff should be considered as a fundamental principle in each department of the hospital.
The mean obtained score of the studied hospitals in terms of the continuation of procurement and provision of hospital supplies was moderate. In the present study, the hospitals had an appropriate list of their equipment; however, they were weak in assessing the consumption of essential and medicinal resources, coordinating with the authorities to ensure the continuous provision of medicines and essential hospital supplies, as well as signing cooperation agreements with retailers to ensure the supply and immediate delivery of equipment in times of shortages and disasters. This finding is not consistent with Karimian, Hosseini Shokouh and Arab et al. findings [10, 14, 24].
In the post-disaster recovery aspect, according to the obtained average score, the hospitals were evaluated as weak. Failure to appoint a responsible person to monitor post-disaster recovery operations, and the lack of setting the necessary criteria for retrieving the team, and absence of a team to check the hospital’s post-accident inventory, the lack of personnel appointment to help post-disaster recovery, no staff’s job description, and overlooking volunteers and other staff in crisis were the main weak points of the studied hospitals. This finding is consistent with Karimian as well as Hasanpour et al. results [14, 19].
Eventually, according to the overall evaluation of all studied hospitals and based on the data presented in Table 2, three hospitals scored below 136, which is considered as a weak overall assessment. Eight hospitals scored less than 182 and more than 136, which indicates a moderate level in their overall assessment. Finally, only 4 hospitals scored above 183, which indicates their good preparedness to cope with unexpected accidents. This finding is also consistent with some studies but inconsistent with some others [8, 10, 14, 20, 21, 24]. The reason for this discrepancies is that this study evaluated all hospitals in the province of Ardabil, but most of the mentioned studies evaluated only a few hospitals.
5. Conclusion
In this study, the preparedness of Ardabil hospitals in disaster response was assessed using a national and standardized tool. The obtained results indicated that the preparedness level of the hospitals in Ardebil in response to unexpected events is moderate. Considering these findings, the high odds of incidents in this province, and the vital role of hospitals in controlling and managing accidents, it seems necessary to take measures like organizing a plan for disaster preparedness, holding regular training courses for crisis management for employees, hiring specialized forces, and other similar actions.
Ethical Considerations
Compliance with ethical guidelines
This article was result of a research project approved by Ardabil University of Medical Sciences and Health Services (Ethical code: IR.ARUMS.REC.1395.130).
Funding
This article was approved by Ardabil University of Medical Sciences and Health Services.
Authors' contributions
All authors contributed in preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all the officials of the Hospitals in Ardebil Province who contributed to the implementation of this project.
References
The most critical issue in disaster management is the health management of the affected-community since disasters always have a significant impact on hygiene, general health, and wellbeing of the stricken community. Hospitals play the most important role in the health system, as they are the basic units to provide healthcare services [10]. Hospitals should have a crisis response program because of their function and front line position in managing the victims of accidents. They have to continue and even increase their activities and perform strong teamwork at the time of accidents [5, 11, 12].
Preparedness is one of the essential stages of the crisis management cycle in pre-disaster and includes all the measures, programs, and activities that enable every organization to respond quickly and effectively in critical situations [10]. Hospital preparedness program, like all other programs, requires an initial survey to determine the strong and weak points of the system. There are studies on the level of preparedness of hospitals in accidents and disasters in other provinces of the country [7, 8, 13]. However, these studies overlooked the level of preparedness of hospitals in Ardabil Province. Thus, the current study assessed the level of preparedness of hospitals in Ardabil Province, Iran, in response to accidents and disasters.
2. Materials and Methods
This research was a descriptive and cross-sectional study. The research setting consisted of all hospitals in Ardabil Province that were selected and studied by total enumeration method. To determine the preparedness of hospitals, the national tool for assessing hospital preparedness in disasters was used. This tool estimates the readiness of a hospital, based on the World Health Organization (WHO) standardized assessment checklist [14] (the customized version for Iran). It was designed to provide an adequate response to medical emergencies and incidents, with an all-hazards approach.
The tool has 91 three-option questions and developed based on 9 key components, as follows: 1. command and control (6 questions); 2. triage (10 questions); 3. human resources (15 questions); 4. communication (9 questions); 5. capacity increase (13 questions); 6. support/logistics management (10 questions); 7. safety and security (11 questions); 8. critical service continuation (8 questions); 9. Post-disaster recovery (9 questions). Score 1 is allocated for the option of under review, score 2 for the option of under performance, and score 3 for the option of completed. In addition to this tool, the general profile of the hospitals was obtained from the general information form of hospitals, which included the hospital name, type, and organizational affiliation, address, telephone, fax, and website, as well as the number of active beds, and hospital occupancy rate.
The applied tool evaluated hospital preparation in 9 key components, each containing a list of necessary measures to assist hospital managers and emergency planners. It includes the following components: 1. Command and control: a decision-making system, which is responsible for activating, coordinating, implementing, and terminating a predetermined program. The desirable performance of the command and control system is essential for the effective management of hospital accidents and emergencies; 2. Communications: clear, accurate, and timely communications are needed to ensure sound decision-making, effective collaboration, public awareness, and public confidence; 3. Safety and security: safety and advanced security mechanisms are essential for an effective response during medical emergencies and incidents; 4. Triage: running patients’ triage operations is required based on the predetermined protocol for the desirable functioning of personnel in the face of high patients’ admission, their management, and care; 5. Increasing capacity: the ability of healthcare facilities to raise their routine capacity to respond to increasing demand for clinical care, which is an essential factor in the planning process of a hospital; 6. Continuation of vital services: An incident should not disturb daily services for essential and surgical services (e.g. emergency care and maternal and child care) that are provided in normal conditions; 7. Human resources: it is necessary to ensure sufficient staff capacity and continuity of efficiency in any incident that increases the need for human resources; 8. Support management: continuity of hospital supplies and supply chains is often underestimated as a challenge during a crisis which requires precise contingency planning and response; 9. Disaster recovery: post-incident recovery planning should be initiated at the same time as responding to the disaster. Quick implementation of the recovery program can help to reduce the long-term impact of a catastrophe on the hospital’s function [15].
Tool scoring
Each of the tool questions has three options; under review, under performance, and completed. It is scored according to the opinions of experts as follows: the option under review: score 1. the option in progress; score 2. The option completed; score 3. Calculating of the level of preparedness in each component is as follows: initially, the scores of options are separately summed up; then, by subtracting the sum of the score of the first option (under review) from the sum of the score of the third option (completed), the preparedness range for each component is obtained. Then, the mentioned range is divided into three sections to determine hospital readiness levels in each component (weak, moderate, and good levels). For example, for the first component (command and control) which has 6 questions, if the sum of the first option answers is 6, the sum of the second option answers is 12, and the sum of the third option answers is 18, then the range of the preparedness for this component is obtained by deducting number 6 (sum of the first options) from 18 (the sum of the third options) which is equal to 12. Next, we divide this range into three parts (equal to 4) to calculate the distance between levels. Therefore, the level of weak preparation of the first component is 6-10, the moderate level of preparation of the first component is 11-14, and the good preparation level of the first component is 18-14.
Also, the total obtainable score of the questionnaire is 273. To assess the overall hospital preparedness, the score ranges from poor preparedness (91-136) to moderate preparedness (137-182), then good preparedness (183-228), and finally to excellent preparedness (229-273). The validity and reliability of the National Assessment Tool for Hospital Preparedness in Accidents and Disasters have been approved in Karimian et al. research. Based on their study, the instrument validity was obtained by content validity method (0.86), and its reliability was calculated using the Cronbach α coefficient (0.83) [14].
After approval of the research project by the Research Council of Ardabil University of Medical Sciences, the researchers referred to the health centers and collected the required information. After providing explanations and obtaining the approval of hospital managers, hospital preparedness was measured using the tools mentioned above. The questionnaire was completed by a crisis management expert of each hospital in the presence of the researcher, and the required supervision was carried out. Eventually, the data collected from the questionnaires were analyzed using descriptive statistics.
3. Results
Of 15 hospitals studied, there were two private hospitals, three hospitals affiliated with nongovernmental organizations, and 10 government hospitals affiliated with Ardabil University of Medical Sciences. The latest evaluation grade of the surveyed hospitals was as follows: 4 hospitals were ranked as second-grade, and 11 hospitals were ranked as first-grade. The hospitals were 28.47 years old on average, and Fatemi Hospital, with 94 years old had the most former constructed building. The total number of beds in the surveyed hospitals was 1844, with an average occupancy rate of 67.13% per year.
Over the past two years, only 6 crises have been reported in all of the studied hospitals. They were food poisoning, water supply disconnection, hospital fuse box fire, and electrical wiring fire at the hospital pharmacy, which occurred in 4 of the investigated hospitals. The training courses and drills held included crisis management, fire extinction, table top drill, hazard management, triage, bioterrorism, aircraft crash, the emergency landing of helicopter.
The average records of Head of hospitals, hospital directors, metrons, and crisis experts were 62.77, 85, 62, and 43.37 months, respectively, in this study. Tables 1 and 2 present other information and findings of the present study. It should be noted that numbers 1 to 15 are used instead of hospital names.
According to Table 2, the mean scores of preparedness of hospitals are as follows: good command and control (15 out of 18), moderate communication (17.5 out of 27), moderate security and safety (21.4 out of 33), weak triage (17 out of 30), moderate capacity increase (23.9 out of 39), moderate critical service continuation (14.6 out of 24), weak human resources (24.7 out of 45), moderate support and logistics (17.7 out of 30), and weak recovery after an event (14.4 out of 27). In general, of 15 hospitals examined, by considering the total score of hospital preparedness assessment in 9 studied aspects, 3 hospitals were rated as weak (127, 135, 136 out of 273), 8 as moderate (153, 151, 178, 156, 179, 164, 175, 160 out of 273) and 4 as good (205, 198, 202, 185 out of 273).
4. Discussion
Currently, the crisis response plan is vital for every organization with any activity. Many studies emphasize the importance of having disaster preparedness plans for every individual, society, organization, health center, and in particular for every hospital. Moreover, response programs are more vital for hospitals because of their function and priority in the admission of victims of accidents.
In the present study, according to the obtained mean score in the command and control aspect, the preparedness of studied hospitals was good. The existence of a hospital-based command headquarters, the appointment of a person responsible for each of the 9 components of the hospital’s preparation, registration and keeping all documentation, familiarity with job descriptions for managers and staff, and adequate training in this field were among the reasons for obtaining a high score in this field. This finding of the present study is inconsistent with the results of Ojaghi et al. who rated the preparedness of hospitals in Kermanshah City as weak; the absence of an incident command center may be the reason for their result [16]. Furthermore, Hojjat et al. and Karimian et al. evaluated their studied hospitals moderate with regard to this component that could be due to specific attention to command and control elements [14, 17].
The second most crucial aspect was communication. In the current research, the studied hospitals scored at a moderate level. In this regard, the lack of a person as an interlocutor and spokesperson, lack of drafting of incidents for patients and the public, and inappropriate methods for collecting and analyzing data were among the weak points in communication component. The findings are consistent with the study findings of Daneshmand et al. as well as Karimian et al. [14, 18].
In our research, the investigated hospitals were scored moderate in the area of safety and security. The strong points were the existence of a hospital safety team and the identification of potential hospital vulnerabilities. However the weak points were the lack of required rules for the presence of people at hospital during disasters and accidents; an unreliable method for identifying personnel, patients and visitors; inappropriate methods for coordinating hospital and military rules; and the lack of suitable location for the sterilization of radioactive, biological, and chemical substances and their isolation. This finding is consistent with the research finding by Karimian et al. but is inconsistent with Amrillon et al. [8, 14] findings.
With regard to the triage component, the average score obtained indicated the weakness of studied hospitals in this area. In 4 hospitals, the triage unit was not active at all. Other reasons for weakness in this aspect were the absence of alternative sites for massive triage, no guidelines for admitted injuries, and the lack of a simple mechanism that can trigger an emergency response from an emergency or triage disaster unit, as well as the failure to determine a specific waiting room for patients who are able to walk. This finding is inconsistent with the results of Karimian et al. and Hasanpour et al. studies [14, 19].
In the aspect of increasing the capacity of the hospital during a crisis, the obtained mean score was indicative of the moderate preparedness of the studied hospitals. In this study, the weak points in this area comprised the failure to calculate the required capacity surge and the increase in demand for hospital services in critical situations based on essential resources and manpower and the lack of identification of methods to increase the capacity of hospitalization and no program contracts with other institutions to provide post-mortality care as well as the absence of a contract with places like stadiums and nearby hotels. The existence of a plan to prioritize interventions and the cancellation of non-essential services were the strengths of studied hospitals in this research. These findings are consistent with investigations by Karimian et al. and Kaji and Gravandi [14, 20, 21].
In this research, the studied hospitals achieved a moderate score in the continuation of vital services. The lack of a regular plan for the continuation of essential services, especially for vulnerable groups (children, elderly and disabled individuals); failure to study the impact of accidents on hospital facilities, like water and food; overlooking the availability of essential items; and no coordination with the neighbor hospitals and private physicians to ensure the continuity of essential services were the weak points of this component. Listing and prioritizing the services of the hospital and compiling the essential services were of the strong points of this preparedness component, which is inconsistent with the research findings of Karimian et al. but agree with the findings of Hoseinin Shokooh and Amiri [14, 10, 22].
In addition, in the efficient human resources management, the studied hospitals obtained a weak score. Ignoring the needs of employees and their families during the crisis and inappropriate programs to recruit volunteers and their training and the lack of a multi-task team for the psychological support of the family of staff and patients were the weaknesses of studied hospitals. Possessing a complete list of staff and their information, continuous monitoring of attendance and absenteeism of employees, providing training to staff in the most demanding wards, and considering the vaccination of employees were their strong points. This finding is consistent with the research findings by Karimian and Salari [14, 23].
Moreover, in the research by Amerion the investigated hospitals were influential in terms of human resources [8]. Considering that human resources always play an essential role in the management of hospital services, using skilled and trained staff should be considered as a fundamental principle in each department of the hospital.
The mean obtained score of the studied hospitals in terms of the continuation of procurement and provision of hospital supplies was moderate. In the present study, the hospitals had an appropriate list of their equipment; however, they were weak in assessing the consumption of essential and medicinal resources, coordinating with the authorities to ensure the continuous provision of medicines and essential hospital supplies, as well as signing cooperation agreements with retailers to ensure the supply and immediate delivery of equipment in times of shortages and disasters. This finding is not consistent with Karimian, Hosseini Shokouh and Arab et al. findings [10, 14, 24].
In the post-disaster recovery aspect, according to the obtained average score, the hospitals were evaluated as weak. Failure to appoint a responsible person to monitor post-disaster recovery operations, and the lack of setting the necessary criteria for retrieving the team, and absence of a team to check the hospital’s post-accident inventory, the lack of personnel appointment to help post-disaster recovery, no staff’s job description, and overlooking volunteers and other staff in crisis were the main weak points of the studied hospitals. This finding is consistent with Karimian as well as Hasanpour et al. results [14, 19].
Eventually, according to the overall evaluation of all studied hospitals and based on the data presented in Table 2, three hospitals scored below 136, which is considered as a weak overall assessment. Eight hospitals scored less than 182 and more than 136, which indicates a moderate level in their overall assessment. Finally, only 4 hospitals scored above 183, which indicates their good preparedness to cope with unexpected accidents. This finding is also consistent with some studies but inconsistent with some others [8, 10, 14, 20, 21, 24]. The reason for this discrepancies is that this study evaluated all hospitals in the province of Ardabil, but most of the mentioned studies evaluated only a few hospitals.
5. Conclusion
In this study, the preparedness of Ardabil hospitals in disaster response was assessed using a national and standardized tool. The obtained results indicated that the preparedness level of the hospitals in Ardebil in response to unexpected events is moderate. Considering these findings, the high odds of incidents in this province, and the vital role of hospitals in controlling and managing accidents, it seems necessary to take measures like organizing a plan for disaster preparedness, holding regular training courses for crisis management for employees, hiring specialized forces, and other similar actions.
Ethical Considerations
Compliance with ethical guidelines
This article was result of a research project approved by Ardabil University of Medical Sciences and Health Services (Ethical code: IR.ARUMS.REC.1395.130).
Funding
This article was approved by Ardabil University of Medical Sciences and Health Services.
Authors' contributions
All authors contributed in preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all the officials of the Hospitals in Ardebil Province who contributed to the implementation of this project.
References
- Becker JS, Paton D, Johnston DM, Ronan KR. Salient beliefs about earthquake hazards and household preparedness. Risk Analysis. 2013; 33(9):1710-27. [DOI:10.1111/risa.12014] [PMID]
- Yellman TW, Murray TM. Vulnerability and resilience. Risk Analysis. 2013; 33(5):753. [DOI:10.1111/risa.12026] [PMID]
- Williams J, Nocera M, Casteel C. The effectiveness of disaster training for health care workers: A systematic review. Annals of Emergency Medicine. 2008; 52(3):211-22. [DOI:10.1016/j.annemergmed.2007.09.030] [PMID]
- Habte A, Addisie A, Azazh A. Assessment of knowledge, attitude and practice of disaster preparedness among Tikur Anbessa specialized hospital health care workers, Addis Ababa, Ethiopia. American Journal of Nursing Science. 2018; 7(1):39-48. [DOI:10.11648/j.ajns.20180701.15]
- Abbasi Sh, Shooshtari Sh, Tofighi Sh. Developing a conceptual model of the Hospital Incident Command System (HICS) via quality improvement models in Iran. Journal of Research in Medical and Dental Science. 2018; 6(2):257-68. [DOI: 10.5455/jrmds.20186240]
- Tavakoli HR, Farajzadeh D, Joneidi N. [Check the status of procurement, storage and distribution of foodstuffs in Bam earthquake (Persian)]. Military Medicine. 2008; 10(1):11-20.
- Vahedparast H, Ravanipour M, Hajinezhad F, Kamali F, Gharibi T, Bagherzadeh R. [Assessing hospital disaster preparedness of Bushehr Province (Persian)]. Iranian Journal of War and Public Health. 2013; 16(1):69-76.
- Amerion A, Delavari AR, Teymourzadeh E. [Rate of preparedness in confronting crisis in three selected border hospitals (Persian)]. Iranian Journal of Military Medicine. 2010; 12(1):19-22.
- Li X, Huang J, Zhang H. An analysis of hospital preparedness capacity for public health emergency in four regions of China: Beijing, Shandong, Guangxi, and Hainan. BMC Public Health. 2008; 8(1):319-30. [DOI:10.1186/1471-2458-8-319] [PMID] [PMCID]
- Hosseini Shokouh SM, Arab M, Rahimi A, Rashidian A, Sadr Momtaz N. [Preparedness of the Iran University of Medical Sciences hospitals against earthquake (Persian)]. Journal of School of Public Health and Institute of Public Health Research. 2009; 6(3-4):61-77.
- Zaboli R, Sh T, Amerion A, Moghaddasi H. [Survey of Tehran City hospitals disaster preparedness for disaster (Persian)]. Journal Millitary Medicine. 2006; 8(2):103-11.
- Varjoshani NJ, Hosseini MA, Khankeh HR, Ahmadi F. Tumultuous atmosphere (physical, mental): The main barrier to emergency department inter-professional communication. Global Journal of Health Science. 2015; 7(1):144-53. [DOI:10.5539/gjhs.v7n1p144] [PMID] [PMCID]
- Ghafari S KHR, Ghanbari V, Ranjbar M. [The study of affiliated hospitals preparedness to University of Welfare and Rehabilitation Sciences for unexpected disasters in 2011 (Persian)]. Quarterly Scientific Journal of Rescue & Relief. 2012; 4(3):21-34.
- Karimiyan A, Khankeh HR, Dalvandi A, Farzin Nia B. The effect of teaching principles of hospital preparedness according to the national program on preparedness of Shahid Motahari burns hospital of Tehran in response to disasters. Health in Emergencies and Disasters Quarterly. 2016; 2(1):25-32. [DOI:10.18869/nrip.hdq.2.1.25]
- Khankeh HR. [Hospital preparedness in disasters and emergencies (national program) (Persian)]. Tehran: University of Social Welfare and Rehabilitation Sciences; 2011.
- Ojaghi SH, Nourizadeh S, Mahboubi M, Khazaei AAR, Najafi GhA. [Disaster crisis handling preparedness level of hospitals in Kermanshah (Persian)]. Journal of Kermanshah University of Medical Sciences (Behbood). 2009; 13(3):267-74.
- Hojat M, Sirati N, Khaghanizadeh M, Karimi ZM. [A survey of hospital disaster management in medical science universities (Persian)]. Daneshvar Medicine. 2008; 15(74):1-10.
- Daneshmandi M, Amiri H, Vahedi M, Farshi M, Saghafi A, Zigheymat F. Assessing the level of preparedness for confronting crisis such as flood, earthquake, fire, and storm in some selected hospitals of Iran. Journal of Military Medicine. 2010; 12(3):167-71.
- Hassanpoor E, Zahmatkesh E, Nazari M, Abbas Imani Z, Mahmodi H, Arabzozani M. [Hospital emergency response of Iran’s hospitals against disasters: A case study in Karaj (Persian)]. Journal of Hospital. 2015; 14(4):67-74.
- Kaji AH, Lewis RJ. Hospital disaster preparedness in Los Angeles County. Academic Emergency Medicine. 2006; 13(11):1198-203. [DOI:10.1197/j.aem.2006.05.007] [PMID]
- Geravandi S, Soltani F, Mohammadi M, Salmanzadeh S, Shirali S, Shahriari A, et al. [The effects of increasing the capacity of admission in emergency ward in increasing the rate of patient acceptance at the time of crisis (Persian)]. Armaghane-e-Danesh. 2016; 20(12):1057-69.
- Amiri M, Mohammadi G, Khosravani A, Chaman R, Arabi M, Sadeghi E, et al. Hospital preparedness of Semnan Province to deal with disasters. Knowledge & Health. 2011; 6(3):44-9.
- Salari H, Heidari A, Julaee H, Rahimi S, Shafaghat T. Shiraz hospitals (public & private) preparedness in dealing with disasters. Scientific Journal of Rescue & Relief. 2010; 2(4):1-11.
- Arab M, Zeraati H, Akbari Haghighi F, Ravangard R. [A study on the executive managers’ knowledge and performance, and their hospitals preparedness against earthquake events and their relationships at public hospitals (affiliated by Tehran University of Medical Sciences (TUMS) 2005-2006) (Persian)]. Journal of Health Administration. 2009; 11(34):7-14.
Type of article: Research |
Subject:
Special
Received: 2018/09/26 | Accepted: 2019/02/20 | Published: 2019/07/23
Received: 2018/09/26 | Accepted: 2019/02/20 | Published: 2019/07/23
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
