

Volume 4, Issue 4 (Summer 2019)
Health in Emergencies and Disasters Quarterly 2019, 4(4): 229-234 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ramezan Zadeh Z, Pashei Sabet F, Moosavi Arfa N, Abbasi M, Vahedian M. Assessment of the Incident Command System Preparedness of the Hospitals in Qom City, Iran. Health in Emergencies and Disasters Quarterly 2019; 4 (4) :229-234
URL: http://hdq.uswr.ac.ir/article-1-256-en.html
URL: http://hdq.uswr.ac.ir/article-1-256-en.html
Zahra Ramezan Zadeh1 

 , Fatemeh Pashei Sabet *2 , Nazila Moosavi Arfa3 , Mohammad Abbasi1 , Mostafa Vahedian4
, Fatemeh Pashei Sabet *2 , Nazila Moosavi Arfa3 , Mohammad Abbasi1 , Mostafa Vahedian4
, Fatemeh Pashei Sabet *2 , Nazila Moosavi Arfa3 , Mohammad Abbasi1 , Mostafa Vahedian4
1- Department of Nursing, Faculty of Nursing and Midwifery, Qom University of Medical Sciences, Qom, Iran.
2- Department of Community Health Nursing, School of Nursing & Midwifery, Iran University of Medical Sciences, Tehran, Iran. ,pashaii1392@gmail.com
3- Central Library and Archives, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
4- Neuroscience Research Center, Qom University of Medical Sciences, Qom, Iran.
2- Department of Community Health Nursing, School of Nursing & Midwifery, Iran University of Medical Sciences, Tehran, Iran. ,
3- Central Library and Archives, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
4- Neuroscience Research Center, Qom University of Medical Sciences, Qom, Iran.
Keywords: Disaster preparedness, Nursing personnel, Disasters, Hospital command system, Hospitals in Qom
Full-Text [PDF 520 kb]
(2709 Downloads)
| Abstract (HTML) (6990 Views)
Full-Text: (1502 Views)
1. Introduction
ach year, disasters, such as floods, earthquakes, terrorist attacks, fires, chemical and microbial attacks, industrial accidents, plane crashes and other types of unexpected events cause thousands of deaths, massive damage to property, displacement of people, and destroying thousands of businesses worldwide [1]. The incidence of disasters around the world has doubled in the last 30 years, and the number of affected people has tripled [2]. According to a global report, more than 400000 people were killed and 46 million affected by earthquakes and tsunamis between 1991 and 2005. It is estimated that in an earthquake in Tehran, about 590000 buildings will be severely damaged and it will result in about $220 million direct damage to the city. The frequent increase in catastrophic events has increased the need for public awareness [3].
One of the essential needs of people affected by natural disasters is health care. Therefore, addressing the diverse and widespread health problems of those affected by disasters is one of the biggest challenges for the health care providers and executives in all countries [1]. Health centers, especially hospitals, should be prepared to deal with natural disasters to avoid confusion and chaos [4]. One of the critical aspects of hospital preparedness for such incidents is the implementation of an early warning system [5]. The Hospital Incident Command System (HICS) is one of the most appropriate models for establishing a comprehensive plan to deal with any crisis in any dimension. HICS works by employing a rational management structure, outlining responsibilities, establishing transparent reporting channels, and also creating a standard, yet simple system for better coordination of hospitals with other agencies involved in disasters [6]. Establishing this system prepares the hospital disaster management committee for emergencies [7]. By assigning and describing the tasks related to the staff and also coordinating health centers to respond to disasters, HICS becomes a flexible approach to direct activities properly and achieve the desired outcome at the time of disasters [1].
Given the importance of hospital services and preparedness during natural disasters, this study aimed at assessing the readiness of the HICS in Qom City, Iran.
2. Materials and Methods
This descriptive-analytical study was conducted on all members of the disaster management committee and supervisors of hospitals in Qom, Iran. Using the census method, all subjects were enrolled in the study (n=120). The inclusion criteria included at least having a bachelor’s degree, having managerial responsibility in the hospital, and being familiar with the crisis management. The exclusion criteria were unwillingness to participate in the study and returning incomplete questionnaires.
The data collection tool was the disaster preparedness questionnaire, which is a reliable and valid tool. It has four sections: the first section surveys demographic characteristics; the second section has 27 items measuring disaster knowledge of participants, scored by 1 (Yes) and 0 (No) with an overall score of 27; the third section with 20 items assesses the attitude towards disaster rated on a 4-point Likert scale (1= very low, 2= low, 3= high, and 4= very high) with a total score of 80; and the last section has 25 items evaluating disaster practice of participants, scored by 1 (Yes) and 0 (No) with the overall score of 25. 10 experts confirmed the validity of the questionnaire in the healthcare disaster response, and for testing its reliability, the Cronbach alpha was calculated and obtained 0.878. The Pearson correlation coefficient for the whole questionnaire was obtained as 0.867.
The introducing letter obtained from the university was provided to the hospitals, and the necessary permissions were received. The researcher then referred to the hospitals and informed the participants about the study objectives and method and obtained their consent. Afterward, the process of conducting committee meetings, disaster control measures, HICS activities, the role of each person, and how to be informed about the disaster were discussed through the structured interviews and numerous meetings. The content, documents and length of the sessions were then reviewed. The whole hospital was checked for entrance and exit routes, emergency doors, safe places, etc. In the next step, the checklist was completed by the participants. The collected data were analyzed in SPSS V.20 using descriptive statistics (mean and standard deviation) and statistical tests (independent t-test, Analysis of Variance (ANOVA) and chi-squared test).
3. Results
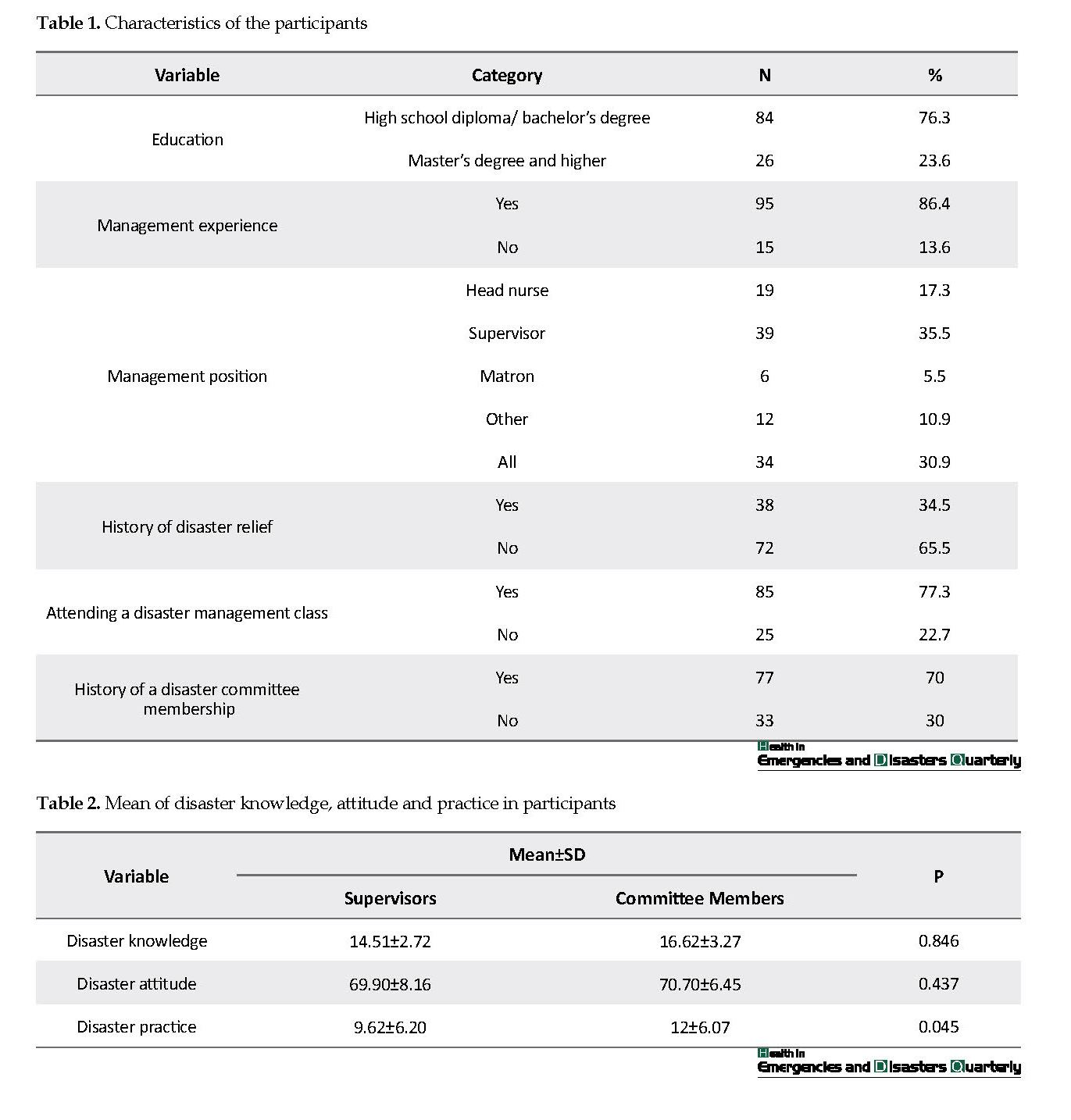
The participants had a management experience between 1 and 45 years (Mean±SD= 12.85±6.98) years and membership in the committee between 0 and 10 years (Mean±SD=3.06±3.24) year. Most of them (76.3%) had a high school diploma and bachelor’s degrees, and 86.4% of them had management experience. Regarding their management position, 35.5% were supervisor, 30.9% were supervisor/head nurse/matron/, and 10.9% had other positions. Only 34.5% of the subjects had a history of disaster relief. The majority of participants (77.3%) had attended a disaster management class, and 70% had a history of membership in the committee (Table 1).
ach year, disasters, such as floods, earthquakes, terrorist attacks, fires, chemical and microbial attacks, industrial accidents, plane crashes and other types of unexpected events cause thousands of deaths, massive damage to property, displacement of people, and destroying thousands of businesses worldwide [1]. The incidence of disasters around the world has doubled in the last 30 years, and the number of affected people has tripled [2]. According to a global report, more than 400000 people were killed and 46 million affected by earthquakes and tsunamis between 1991 and 2005. It is estimated that in an earthquake in Tehran, about 590000 buildings will be severely damaged and it will result in about $220 million direct damage to the city. The frequent increase in catastrophic events has increased the need for public awareness [3].
One of the essential needs of people affected by natural disasters is health care. Therefore, addressing the diverse and widespread health problems of those affected by disasters is one of the biggest challenges for the health care providers and executives in all countries [1]. Health centers, especially hospitals, should be prepared to deal with natural disasters to avoid confusion and chaos [4]. One of the critical aspects of hospital preparedness for such incidents is the implementation of an early warning system [5]. The Hospital Incident Command System (HICS) is one of the most appropriate models for establishing a comprehensive plan to deal with any crisis in any dimension. HICS works by employing a rational management structure, outlining responsibilities, establishing transparent reporting channels, and also creating a standard, yet simple system for better coordination of hospitals with other agencies involved in disasters [6]. Establishing this system prepares the hospital disaster management committee for emergencies [7]. By assigning and describing the tasks related to the staff and also coordinating health centers to respond to disasters, HICS becomes a flexible approach to direct activities properly and achieve the desired outcome at the time of disasters [1].
Given the importance of hospital services and preparedness during natural disasters, this study aimed at assessing the readiness of the HICS in Qom City, Iran.
2. Materials and Methods
This descriptive-analytical study was conducted on all members of the disaster management committee and supervisors of hospitals in Qom, Iran. Using the census method, all subjects were enrolled in the study (n=120). The inclusion criteria included at least having a bachelor’s degree, having managerial responsibility in the hospital, and being familiar with the crisis management. The exclusion criteria were unwillingness to participate in the study and returning incomplete questionnaires.
The data collection tool was the disaster preparedness questionnaire, which is a reliable and valid tool. It has four sections: the first section surveys demographic characteristics; the second section has 27 items measuring disaster knowledge of participants, scored by 1 (Yes) and 0 (No) with an overall score of 27; the third section with 20 items assesses the attitude towards disaster rated on a 4-point Likert scale (1= very low, 2= low, 3= high, and 4= very high) with a total score of 80; and the last section has 25 items evaluating disaster practice of participants, scored by 1 (Yes) and 0 (No) with the overall score of 25. 10 experts confirmed the validity of the questionnaire in the healthcare disaster response, and for testing its reliability, the Cronbach alpha was calculated and obtained 0.878. The Pearson correlation coefficient for the whole questionnaire was obtained as 0.867.
The introducing letter obtained from the university was provided to the hospitals, and the necessary permissions were received. The researcher then referred to the hospitals and informed the participants about the study objectives and method and obtained their consent. Afterward, the process of conducting committee meetings, disaster control measures, HICS activities, the role of each person, and how to be informed about the disaster were discussed through the structured interviews and numerous meetings. The content, documents and length of the sessions were then reviewed. The whole hospital was checked for entrance and exit routes, emergency doors, safe places, etc. In the next step, the checklist was completed by the participants. The collected data were analyzed in SPSS V.20 using descriptive statistics (mean and standard deviation) and statistical tests (independent t-test, Analysis of Variance (ANOVA) and chi-squared test).
3. Results
The participants had a management experience between 1 and 45 years (Mean±SD= 12.85±6.98) years and membership in the committee between 0 and 10 years (Mean±SD=3.06±3.24) year. Most of them (76.3%) had a high school diploma and bachelor’s degrees, and 86.4% of them had management experience. Regarding their management position, 35.5% were supervisor, 30.9% were supervisor/head nurse/matron/, and 10.9% had other positions. Only 34.5% of the subjects had a history of disaster relief. The majority of participants (77.3%) had attended a disaster management class, and 70% had a history of membership in the committee (Table 1).
According to the results in Table 2, there was no significant difference between the mean knowledge (P=0.846) and attitude (P=0.437) of the members of the Disaster Management Committee and supervisors of hospitals regarding disaster and emergency preparedness. However, the results showed a significant difference between the mean practice of them regarding disaster preparedness (P=0.045), as the committee members had a higher mean practice score compared with the supervisors.
4. Discussion
According to the findings, the studied hospitals had no approved operational plan and predetermined guidelines regarding disaster preparedness, and they were arranging meetings based on events that had already occurred or were likely to occur. This finding is consistent with the results of Malekshahi and Mardani [8] study, who mentioned the absence of a pre-defined and comprehensive operational plan in the studied hospitals and also the results of Mastaneh and Mouseli [9] study, who reported that only in some cases, such as continuing education programs, hospitals had approved operating plans and executive instructions. Therefore, given the importance and role of the Disaster Management Committee in responding to disasters before, during, and after its occurrence, the HICS of hospitals need to be more active. Based on the findings of the research, most hospitals had old and worn-out construction. Results of a study on 100 Hospitals in Ecuador also indicated that 16 hospitals did not have suitable structural conditions and needed to participate in reconstruction programs, and their vulnerability should also be reduced [9].
According to the findings, there was no significant relationship between knowledge, attitude, and practice of the individuals towards disaster preparedness and their history of membership in the Disaster Management Committee. This finding agrees with the results of Amiri et al. [10] and Mohammadi et al. [11] studies, in which hospital readiness had a significant relationship with management experience and educational level of managers. On the contrary, the results of Imani et al. [12] showed a significant correlation between the level of education and experience in crisis maneuvering and membership in the Crisis Committee and also people’s knowledge of crisis management.
5. Conclusion
Some members of the Disaster Management Committee did not have enough information about this committee, their job descriptions, functions, etc., and they were only a member of the committee. Therefore, it is suggested that the duties of the committee members be specified. All members should be fully aware of the subject of the meetings and participate actively in the meetings.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article.
Funding
The present paper was extracted from the MSc. thesis of the first author Zahra Ramadanzadeh Department of Nursing, Faculty of Nursing and Midwifery, Qom University of Medical Sciences, Qom, and with the guidance of Dr. Fatemeh Pashaei and other colleagues of the research team.
Authors' contributions
All authors contributed in preparing this article.
Conflict of interest
The authors declared no conflict of interests.
References
Hussmann B, Lendemans S. Pre-hospital and early in-hospital management of severe injuries: Changes and trends. Injury. 2014; 45(Suppl 3):S39-42. [DOI:10.1016/j.injury.2014.08.016] [PMID]
Ghabari V, Maddah SBS, Khankeh HR, Karimlu M, Ardalan A. Impact of disaster preparedness plan on nursing staff readiness for responding to potential natural disasters. Iranian Journal of Nursing. 2011; 24(73):72-80.
Amanat, Nasir, Khankeh HR, Hoseini AM, Mohammadi R, et al. The effect of seismic coping training on high school male students on households’ preparedness in Eshtehard City in 2010-2011. Journal of Rescue and Rescue. 2013; 5(3):27-39 .
Paul JA, Batta R. Models for hospital location and capacity allocation for an area prone to natural disasters. International Journal of Operational Research. 2007; 3(5):473. [DOI:10.1504/IJOR.2008.019170]
Delshad V, Borhani F, Khankeh H, Abbaszadeh A, Sabzalizadeh S, Moradian MJ, et al. The effect of activating early warning system on motahari hospital preparedness. Health in Emergencies and Disasters Quarterly. 2015; 1(1):3-8. [DOI:10.15412/J.HDQ.09010302]
Akhavanmoghadam, Adibnejad, Soheil, Nayini M. Familiarity with the crisis management and hospital management system in unhealthy accidents (HEICS) and how it is executed. Journal of Medicine. 2005; 7(2):167-75.
Khankeh HR, Lotfolahbeygi M, Dalvandi A, Amanat N. Effects hospital incident command system establishment on disaster preparedness of tehran hospitals affiliated to law enforcement staff under simulated conditions. Health in Emergencies and Disasters Quarterly. 2018; 3(4):207-14. [DOI:10.32598/hdq.3.4.207]
Malekshahi F, Mardani M. Abilities and limitations of crisis management in Shohadaye Ashayer and Social Security hospitals of Khorramabad in 1385. Journal of Critical Care Nursing. 2009; 1(1):29-34.
Mastaneh Z, Mouseli L. Capabilities and limitations of crisis management in the teaching hospitals of Hormozgan University of Medical Sciences, 2010. Scientific Research and Essays. 2013; 8(26):1196-202.
Amiri M, Raee M, Nasrollahpur Shirvani Sd, Mohahhadi Gh, Afkar A, Aghayan Sh, et al. Assessing the readiness of hospitals in north of Iran for dealing with disasters in 2011. Hospital Magazine. 2012; 12(1):19-28.
Amiri M, Mohammadi G, Khosravi A, Chaman R, Arabi M, Sadeghi E, et al. Hospital preparedness of Semnan province to deal with disasters. 2011; 6(3):44-50.
E Imani, Hoseini Tashnizi S, Tafrihi M, Alavi A, Jafari A, Badri Sh.. Nurses Knowledge about Crisis Management and its Related Factors. J Health Care. 2012; 13(4):10-8.
4. Discussion
According to the findings, the studied hospitals had no approved operational plan and predetermined guidelines regarding disaster preparedness, and they were arranging meetings based on events that had already occurred or were likely to occur. This finding is consistent with the results of Malekshahi and Mardani [8] study, who mentioned the absence of a pre-defined and comprehensive operational plan in the studied hospitals and also the results of Mastaneh and Mouseli [9] study, who reported that only in some cases, such as continuing education programs, hospitals had approved operating plans and executive instructions. Therefore, given the importance and role of the Disaster Management Committee in responding to disasters before, during, and after its occurrence, the HICS of hospitals need to be more active. Based on the findings of the research, most hospitals had old and worn-out construction. Results of a study on 100 Hospitals in Ecuador also indicated that 16 hospitals did not have suitable structural conditions and needed to participate in reconstruction programs, and their vulnerability should also be reduced [9].
According to the findings, there was no significant relationship between knowledge, attitude, and practice of the individuals towards disaster preparedness and their history of membership in the Disaster Management Committee. This finding agrees with the results of Amiri et al. [10] and Mohammadi et al. [11] studies, in which hospital readiness had a significant relationship with management experience and educational level of managers. On the contrary, the results of Imani et al. [12] showed a significant correlation between the level of education and experience in crisis maneuvering and membership in the Crisis Committee and also people’s knowledge of crisis management.
5. Conclusion
Some members of the Disaster Management Committee did not have enough information about this committee, their job descriptions, functions, etc., and they were only a member of the committee. Therefore, it is suggested that the duties of the committee members be specified. All members should be fully aware of the subject of the meetings and participate actively in the meetings.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article.
Funding
The present paper was extracted from the MSc. thesis of the first author Zahra Ramadanzadeh Department of Nursing, Faculty of Nursing and Midwifery, Qom University of Medical Sciences, Qom, and with the guidance of Dr. Fatemeh Pashaei and other colleagues of the research team.
Authors' contributions
All authors contributed in preparing this article.
Conflict of interest
The authors declared no conflict of interests.
References
Hussmann B, Lendemans S. Pre-hospital and early in-hospital management of severe injuries: Changes and trends. Injury. 2014; 45(Suppl 3):S39-42. [DOI:10.1016/j.injury.2014.08.016] [PMID]
Ghabari V, Maddah SBS, Khankeh HR, Karimlu M, Ardalan A. Impact of disaster preparedness plan on nursing staff readiness for responding to potential natural disasters. Iranian Journal of Nursing. 2011; 24(73):72-80.
Amanat, Nasir, Khankeh HR, Hoseini AM, Mohammadi R, et al. The effect of seismic coping training on high school male students on households’ preparedness in Eshtehard City in 2010-2011. Journal of Rescue and Rescue. 2013; 5(3):27-39 .
Paul JA, Batta R. Models for hospital location and capacity allocation for an area prone to natural disasters. International Journal of Operational Research. 2007; 3(5):473. [DOI:10.1504/IJOR.2008.019170]
Delshad V, Borhani F, Khankeh H, Abbaszadeh A, Sabzalizadeh S, Moradian MJ, et al. The effect of activating early warning system on motahari hospital preparedness. Health in Emergencies and Disasters Quarterly. 2015; 1(1):3-8. [DOI:10.15412/J.HDQ.09010302]
Akhavanmoghadam, Adibnejad, Soheil, Nayini M. Familiarity with the crisis management and hospital management system in unhealthy accidents (HEICS) and how it is executed. Journal of Medicine. 2005; 7(2):167-75.
Khankeh HR, Lotfolahbeygi M, Dalvandi A, Amanat N. Effects hospital incident command system establishment on disaster preparedness of tehran hospitals affiliated to law enforcement staff under simulated conditions. Health in Emergencies and Disasters Quarterly. 2018; 3(4):207-14. [DOI:10.32598/hdq.3.4.207]
Malekshahi F, Mardani M. Abilities and limitations of crisis management in Shohadaye Ashayer and Social Security hospitals of Khorramabad in 1385. Journal of Critical Care Nursing. 2009; 1(1):29-34.
Mastaneh Z, Mouseli L. Capabilities and limitations of crisis management in the teaching hospitals of Hormozgan University of Medical Sciences, 2010. Scientific Research and Essays. 2013; 8(26):1196-202.
Amiri M, Raee M, Nasrollahpur Shirvani Sd, Mohahhadi Gh, Afkar A, Aghayan Sh, et al. Assessing the readiness of hospitals in north of Iran for dealing with disasters in 2011. Hospital Magazine. 2012; 12(1):19-28.
Amiri M, Mohammadi G, Khosravi A, Chaman R, Arabi M, Sadeghi E, et al. Hospital preparedness of Semnan province to deal with disasters. 2011; 6(3):44-50.
E Imani, Hoseini Tashnizi S, Tafrihi M, Alavi A, Jafari A, Badri Sh.. Nurses Knowledge about Crisis Management and its Related Factors. J Health Care. 2012; 13(4):10-8.
Type of article: Research |
Subject:
General
Received: 2019/05/7 | Accepted: 2019/09/23 | Published: 2020/01/27
Received: 2019/05/7 | Accepted: 2019/09/23 | Published: 2020/01/27
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
