

Volume 5, Issue 1 (Autumn 2019)
Health in Emergencies and Disasters Quarterly 2019, 5(1): 37-44 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Shabanikiya H, Gholami-Fadihegi M, Khodashenas E, Sohrabizadeh S, Heidarian Miri H. Research Paper: A Model for Predicting Hospitalized Children Appropriate for Early Discharge During Disasters. Health in Emergencies and Disasters Quarterly 2019; 5 (1) :37-44
URL: http://hdq.uswr.ac.ir/article-1-264-en.html
URL: http://hdq.uswr.ac.ir/article-1-264-en.html
Hamidreza Shabanikiya1 

 , Mahdi Gholami-Fadihegi2 , Ezzat Khodashenas3 , Sanaz Sohrabizadeh4 , Hamid Heidarian Miri *5
, Mahdi Gholami-Fadihegi2 , Ezzat Khodashenas3 , Sanaz Sohrabizadeh4 , Hamid Heidarian Miri *5
, Mahdi Gholami-Fadihegi2 , Ezzat Khodashenas3 , Sanaz Sohrabizadeh4 , Hamid Heidarian Miri *5
1- Department of Health Economics & Management Sciences, Social Determinants of Health Research Center, Mashhad University of Medical Sciences, Mashhad, Iran., Faculty of Health, Daneshgah Ave. #18, Mashhad-Iran, Tel.: (+98 51) 31892503
2- Student Research Committee, School of Health, Mashhad University of Medical Sciences, Mashhad, Iran., Faculty of Health, Daneshgah Ave. #18, Mashhad-Iran, Tel.: (+98 51) 31892503
3- Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran., Faculty of Medicine, Azadi Square, Pardis campus, Mashhad-Iran Tel.: (+98 51) 38828888
4- Department of Health in Disasters and Emergencies, School of Health, Safety, and Environment, Shahid Beheshti University of Medical Sciences, Tehran, Iran., School of Health, ShahidBeheshtiUniversityof Medical Science, Daneshjoo Blvd, Evin Ave, Tehran, IR. IRAN Tel Number: 0098-21-22432040-41
5- Department of Epidemiology and Biostatistics, Social Determinants of Health Research Center, Mashhad University of Medical Sciences, Mashhad, Iran. ,heidarianh@mums.ac.ir
2- Student Research Committee, School of Health, Mashhad University of Medical Sciences, Mashhad, Iran., Faculty of Health, Daneshgah Ave. #18, Mashhad-Iran, Tel.: (+98 51) 31892503
3- Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran., Faculty of Medicine, Azadi Square, Pardis campus, Mashhad-Iran Tel.: (+98 51) 38828888
4- Department of Health in Disasters and Emergencies, School of Health, Safety, and Environment, Shahid Beheshti University of Medical Sciences, Tehran, Iran., School of Health, ShahidBeheshtiUniversityof Medical Science, Daneshjoo Blvd, Evin Ave, Tehran, IR. IRAN Tel Number: 0098-21-22432040-41
5- Department of Epidemiology and Biostatistics, Social Determinants of Health Research Center, Mashhad University of Medical Sciences, Mashhad, Iran. ,
Full-Text [PDF 591 kb]
(2046 Downloads)
| Abstract (HTML) (5015 Views)

Full-Text: (1266 Views)
1. Introduction
The proper response of health systems to disasters depends on provided healthcare services required by an increasing number of casualties rushing to the hospitals during disasters [1-3]. As hospitals in under-developed or developing countries are not capable of meeting healthcare demands in normal conditions, they definitely face serious challenges during disasters [4-6]. Early discharge or reverse triage is one of the best strategies to solve this challenge and increase the capacity of the hospitals during disasters [7-10]. However, the key issue in applying this strategy is recognizing patients appropriate for early discharge. In other words, those whose discharge from the hospital will not endanger their health for at least 72 h [11, 12].
Children are always affected by disasters and are one of the most vulnerable groups [13]. They have their own specific demands during disasters, which needs specific plans and approaches and are very different from those of adults [14, 15]. Nevertheless, the children’s needs and special conditions are usually ignored; for example, early discharge during disasters is frequently occurred in this age group [16]. Despite the significance of this issue, few studies have been conducted on identifying children appropriate for early discharge during disasters. Therefore, no tools or models to identify such children were found.
Kelen et al. offered a 5-level classification for the risk level of health-threatening events caused by early discharge of a pediatric patient [17]. However, they did not present any criterion, indicator or variable to consider a child in any class. In fact, this study only calculated and classified the acceptable risk level of the early discharge of pediatric patients, approved by a group of pediatricians.
In normal conditions, the attending physician is best person to decide about the discharge of a patient. He/she can make the best decision about the early discharge of their patients based on a range of clinical and non-clinical variables during disasters [18]. In other words, consulting the attending physician is one of the ways to recognize patients appropriate for early discharge. However, finding an attending physician could be restricted in disasters.
Therefore, regarding the knowledge gap in this area, and also the significance of early discharge as an effective strategy to increase hospital capacity, the current study aimed at estimating a model for predicting pediatric patients appropriate for early discharge, based on the attending physician’s opinion. This model not only assist the hospital clinical staff to discharge patients during disasters in the absence of the attending physician but also can be used as a tool to assess the capability of an early discharge during normal conditions to plan for the hospital surge capacity and improve hospital disaster preparedness.
2. Materials and Methods
This cross-sectional study was conducted on 210 pediatric patients (younger than 14 years) hospitalized in the emergency and pediatrics wards of Imam Reza, Ghaem, Shahid Hasheminejad, and Doctor Sheikh hospitals covered by Mashhad University of Medical Sciences (MUMS). Sampling was conducted through census method because the sampling could not be achieved in the studied hospitals in one day. It was started at the time of data collection until the required subjects were achieved (three days of three weeks). The exclusion criterion was the due date of discharge at data collection day.
A trained clinician visited the hospitals and asked the patient’s attending physician to fill the first part of the questionnaire. Subsequently, he filled the second part of the questionnaire after obtaining consent from the patient’s parents.
Data collection was done through a researcher-made questionnaire. After conducting an extensive literature review, the research team developed the initial questionnaire, which consisted of 29 questions in two parts. Content Validity Ratio (CVR) was used to assess the validity of the initial questionnaire. Accordingly, a group of experts including 20 pediatricians was asked for their opinion about 29 questions. The calculated CVRs are presented in Table 1. The validity of 10 out of the 28 questions of the second part, and the only question of the first part were approved (Table 1). As the patient’s conditions and consequently, the physician’s opinion could change at any moment, the reliability was not considered.
Therefore, the final questionnaire consisted of two parts. The second part consisted of 10 questions (to measure the independent variables), whereas the first part included one question to assess the dependent variable. In this stage, the first early discharge during disasters was defined briefly, and then the patient’s attending physician was provided with a short scenario about a disaster taking place near the studied hospital along with some assumptions. Based on the presented scenario and assumptions, the patient’s attending physician was asked to give his opinion on the early discharge or not for his/her patient in the form of a yes/no question.
Data analysis was done by STATA v14.1. To investigate the relationship between each independent variable and the dependent variable, the Chi-squared test was used for qualitative independent variables and the T-test was employed for quantitative independent variables. Subsequently, variables with a P-value of less than or equal to 0.2 (P≤0.2) entered the final logistic regression model.
3. Results
The results of validity of the initial questionnaire (the calculated CVRs) are presented in Table 1. As shown in Table 1, 11 questions (38%) of the initial questionnaire were approved by the experts. Regarding gender, 107 cases (51.7%)were male and 100 cases (48.3%) were female with an average age of 4.42±3.77 years. According to the attending physicians’ opinions, 56.5% (n=117) of the patients were appropriate for an early discharge.
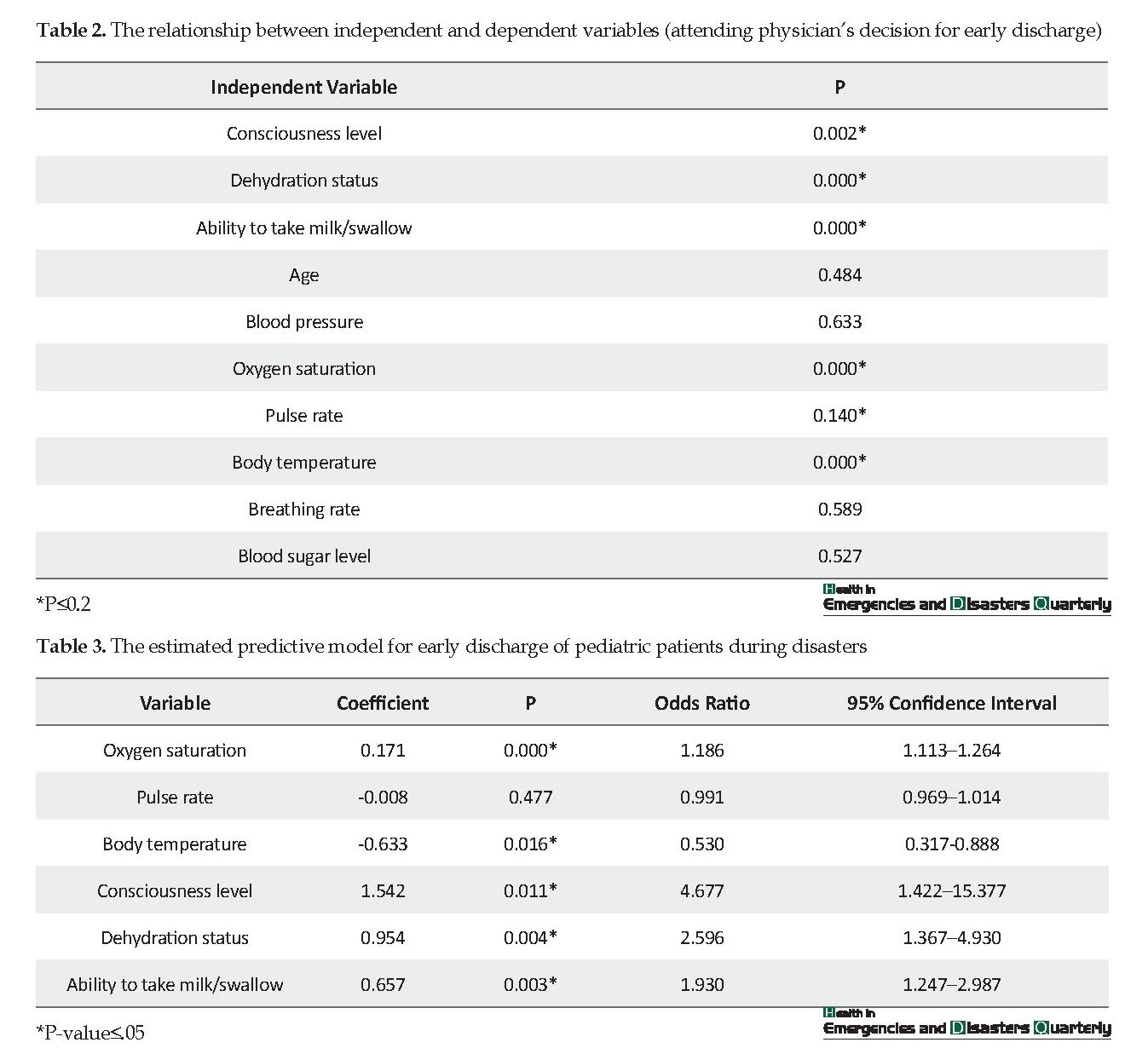
Table 2 indicates the results of the Pearson chi-squared test and t-test conducted to assess the relationship between each independent variables and the dependent variable of the study (early discharge). Table 2 indicates that there was a significant relationship between the five independent variables, such as consciousness level, dehydration status, ability to take milk/swallow, blood oxygen saturation level, and body temperature and the dependent variable (P≤0.05). The effect of these variables and also the pulse rate were calculated simultaneously using the logistic regression method. The estimated model and its coefficients are represented in Table 3.
As shown in Table 3, all variables with a significant relationship with early discharge. Only pulse rate showed no significant effect on the dependent variable in this regression model. Based on the Table 3, for each unit increase in the oxygen saturation level, the chance of early discharge of the pediatric patient by the attending physician increased by 1.186%, whereas it decreased by .530% with each unit increase in the body temperature. The Table 3 indicates that the chance of early discharge was 4.677 times higher in conscious patients compared with the other patients and 2.596 higher in patients with no dehydration than those with certain degrees of dehydration. The chance of early discharge in children who had the ability to take milk/swallow was almost twice as much as those with inability to take milk/swallow (1.930 times higher).
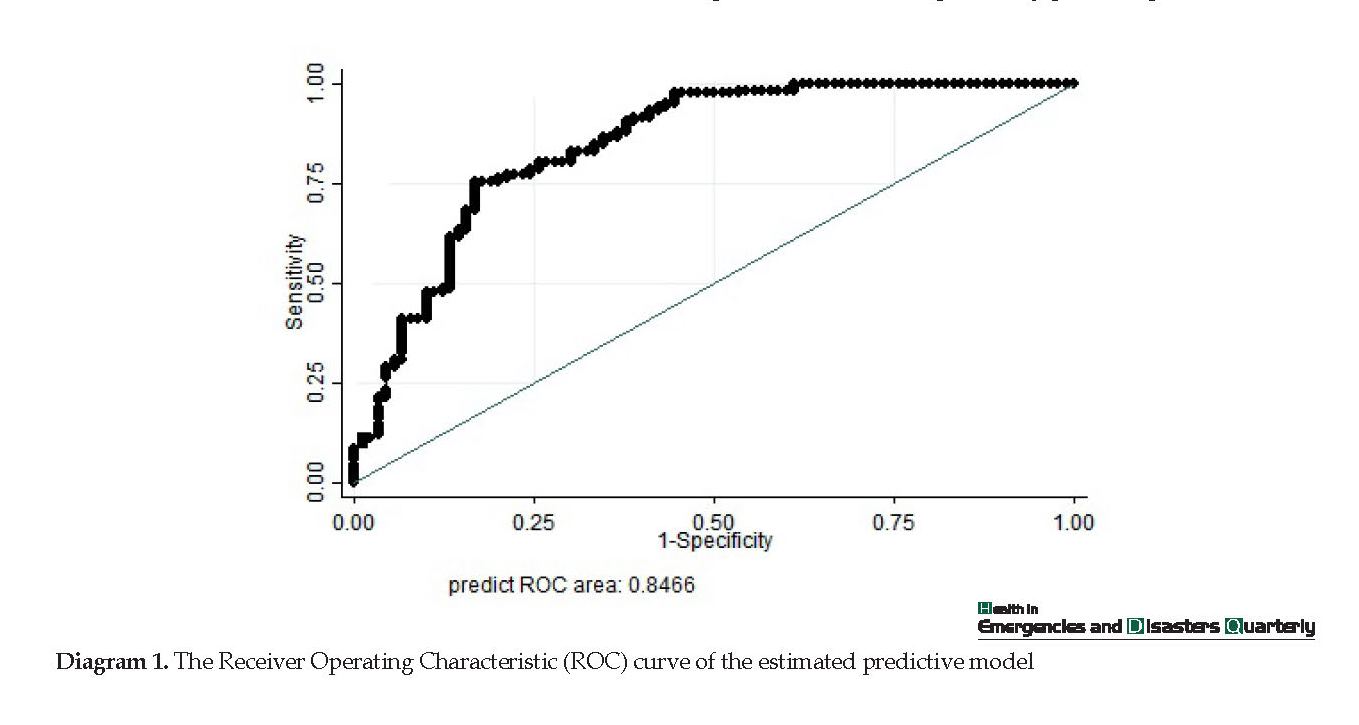
Diagram 1 represents the ROC curve to predict the estimated regression model. Diagram 1 indicates the area under the curve of .846 with a standard error of .028, which was significant (P-value ≤.05). The area under the curve was within the 95% confidence interval of between 0.791 and 0.901. Due to the area under the curve of between 0.8 and 0.9, this model had a good curve fit.
4. Discussion
Five variables of oxygen saturation, body temperature, consciousness level, dehydration status, and ability to take milk/swallow were entered the estimated model and determined as the predictors for pediatric patients appropriate for early discharge. No relevant study has been conducted to provide a model to predict which pediatric patients can be considered for early discharge during disasters. However, the findings of this study can be compared with “triage” and “reverse triage” models or models evaluating the patients’ conditions, specifically pediatric patients.
The proper response of health systems to disasters depends on provided healthcare services required by an increasing number of casualties rushing to the hospitals during disasters [1-3]. As hospitals in under-developed or developing countries are not capable of meeting healthcare demands in normal conditions, they definitely face serious challenges during disasters [4-6]. Early discharge or reverse triage is one of the best strategies to solve this challenge and increase the capacity of the hospitals during disasters [7-10]. However, the key issue in applying this strategy is recognizing patients appropriate for early discharge. In other words, those whose discharge from the hospital will not endanger their health for at least 72 h [11, 12].
Children are always affected by disasters and are one of the most vulnerable groups [13]. They have their own specific demands during disasters, which needs specific plans and approaches and are very different from those of adults [14, 15]. Nevertheless, the children’s needs and special conditions are usually ignored; for example, early discharge during disasters is frequently occurred in this age group [16]. Despite the significance of this issue, few studies have been conducted on identifying children appropriate for early discharge during disasters. Therefore, no tools or models to identify such children were found.
Kelen et al. offered a 5-level classification for the risk level of health-threatening events caused by early discharge of a pediatric patient [17]. However, they did not present any criterion, indicator or variable to consider a child in any class. In fact, this study only calculated and classified the acceptable risk level of the early discharge of pediatric patients, approved by a group of pediatricians.
In normal conditions, the attending physician is best person to decide about the discharge of a patient. He/she can make the best decision about the early discharge of their patients based on a range of clinical and non-clinical variables during disasters [18]. In other words, consulting the attending physician is one of the ways to recognize patients appropriate for early discharge. However, finding an attending physician could be restricted in disasters.
Therefore, regarding the knowledge gap in this area, and also the significance of early discharge as an effective strategy to increase hospital capacity, the current study aimed at estimating a model for predicting pediatric patients appropriate for early discharge, based on the attending physician’s opinion. This model not only assist the hospital clinical staff to discharge patients during disasters in the absence of the attending physician but also can be used as a tool to assess the capability of an early discharge during normal conditions to plan for the hospital surge capacity and improve hospital disaster preparedness.
2. Materials and Methods
This cross-sectional study was conducted on 210 pediatric patients (younger than 14 years) hospitalized in the emergency and pediatrics wards of Imam Reza, Ghaem, Shahid Hasheminejad, and Doctor Sheikh hospitals covered by Mashhad University of Medical Sciences (MUMS). Sampling was conducted through census method because the sampling could not be achieved in the studied hospitals in one day. It was started at the time of data collection until the required subjects were achieved (three days of three weeks). The exclusion criterion was the due date of discharge at data collection day.
A trained clinician visited the hospitals and asked the patient’s attending physician to fill the first part of the questionnaire. Subsequently, he filled the second part of the questionnaire after obtaining consent from the patient’s parents.
Data collection was done through a researcher-made questionnaire. After conducting an extensive literature review, the research team developed the initial questionnaire, which consisted of 29 questions in two parts. Content Validity Ratio (CVR) was used to assess the validity of the initial questionnaire. Accordingly, a group of experts including 20 pediatricians was asked for their opinion about 29 questions. The calculated CVRs are presented in Table 1. The validity of 10 out of the 28 questions of the second part, and the only question of the first part were approved (Table 1). As the patient’s conditions and consequently, the physician’s opinion could change at any moment, the reliability was not considered.
Therefore, the final questionnaire consisted of two parts. The second part consisted of 10 questions (to measure the independent variables), whereas the first part included one question to assess the dependent variable. In this stage, the first early discharge during disasters was defined briefly, and then the patient’s attending physician was provided with a short scenario about a disaster taking place near the studied hospital along with some assumptions. Based on the presented scenario and assumptions, the patient’s attending physician was asked to give his opinion on the early discharge or not for his/her patient in the form of a yes/no question.
Data analysis was done by STATA v14.1. To investigate the relationship between each independent variable and the dependent variable, the Chi-squared test was used for qualitative independent variables and the T-test was employed for quantitative independent variables. Subsequently, variables with a P-value of less than or equal to 0.2 (P≤0.2) entered the final logistic regression model.
3. Results
The results of validity of the initial questionnaire (the calculated CVRs) are presented in Table 1. As shown in Table 1, 11 questions (38%) of the initial questionnaire were approved by the experts. Regarding gender, 107 cases (51.7%)were male and 100 cases (48.3%) were female with an average age of 4.42±3.77 years. According to the attending physicians’ opinions, 56.5% (n=117) of the patients were appropriate for an early discharge.
Table 2 indicates the results of the Pearson chi-squared test and t-test conducted to assess the relationship between each independent variables and the dependent variable of the study (early discharge). Table 2 indicates that there was a significant relationship between the five independent variables, such as consciousness level, dehydration status, ability to take milk/swallow, blood oxygen saturation level, and body temperature and the dependent variable (P≤0.05). The effect of these variables and also the pulse rate were calculated simultaneously using the logistic regression method. The estimated model and its coefficients are represented in Table 3.
As shown in Table 3, all variables with a significant relationship with early discharge. Only pulse rate showed no significant effect on the dependent variable in this regression model. Based on the Table 3, for each unit increase in the oxygen saturation level, the chance of early discharge of the pediatric patient by the attending physician increased by 1.186%, whereas it decreased by .530% with each unit increase in the body temperature. The Table 3 indicates that the chance of early discharge was 4.677 times higher in conscious patients compared with the other patients and 2.596 higher in patients with no dehydration than those with certain degrees of dehydration. The chance of early discharge in children who had the ability to take milk/swallow was almost twice as much as those with inability to take milk/swallow (1.930 times higher).
Diagram 1 represents the ROC curve to predict the estimated regression model. Diagram 1 indicates the area under the curve of .846 with a standard error of .028, which was significant (P-value ≤.05). The area under the curve was within the 95% confidence interval of between 0.791 and 0.901. Due to the area under the curve of between 0.8 and 0.9, this model had a good curve fit.
4. Discussion
Five variables of oxygen saturation, body temperature, consciousness level, dehydration status, and ability to take milk/swallow were entered the estimated model and determined as the predictors for pediatric patients appropriate for early discharge. No relevant study has been conducted to provide a model to predict which pediatric patients can be considered for early discharge during disasters. However, the findings of this study can be compared with “triage” and “reverse triage” models or models evaluating the patients’ conditions, specifically pediatric patients.
Early discharge during disasters is also called reverse triage. Although in the early discharge, patients at good conditions are selected, in triage, those at bad health conditions are considered; it can be said that both types have almost similar factors that are related to the general conditions of the patients.
It can be concluded that the consciousness level, as the most important predictor in the current study (OR=4.67), was also the major variable and the common component in almost all of the triage and assuagement models and tools. These models can be used for evaluating pediatric patients, such as “Pediatric South African Triage Score Chart”, “Jump START Pediatric Mass Casualty Incidents Triage” and “Pediatric Triage Tape” or assessing adults, such as “Glasgow Coma Scale”, “The Acute Physiology and Chronic Health Evaluation” and “Care Flight Triage” [19-24]. Nevertheless, the method to evaluate the consciousness level or the scoring system is varied in each model. Severe life-threatening dangers caused by disorders in the central nervous system could justify the significance and presence of consciousness level in all the available models.
Although two other predictors of dehydration status and ability to take milk/swallow are less common in triage models and algorithms and also models for evaluating pediatric patients, this inconsistency could be caused by the difference in their context. Most of these models and studies have been conducted in developed countries, whereas the current study was conducted in a developing country, where some parts of total disease burden and mortality rate in children’ are attributed to dehydration (caused by gastrointestinal infections) and malnutrition. This challenge has been noted in the Guidelines of Integrated Healthcare for children’s Illnesses, which is considered as the national clinical guidelines for the management of ill children. Assessing the pediatric patient’s dehydration and nutrition status, such as their ability to take milk/swallow, is a part of the emergent signs’ evaluation in the mentioned guidelines [25].
Based on the findings of this research, blood oxygen saturation level is another predictor for selecting pediatric patients appropriate for early discharge during disasters, which is consistent with the “Save a Child and Pediatric Assessment Triangle” guidelines [26, 27]. In this guideline, the ventilation status is somehow an indicator of the blood oxygen saturation level. The significance of sufficient oxygen supply for the brain and also the risk of reduced brain oxygen could explain the presence of blood oxygen saturation in the current model.
Body temperature is an indicator evaluated in most methods and algorithms evaluating children’s emergencies, namely the “Revised Pediatric Emergency Assessment Tool”, “WHO’s Pediatric Emergency Triage”, and “Assessment and Treatment Guideline”. Severe complications caused by high fevers and high body temperatures, such as convulsion can justify the presence of this variable in this model and the other models, as well [28-30].
The limitation of the current study was the used method for evaluating early discharge: ‘Appropriate for early discharge’ or ‘inappropriate for early discharge’, based on the attending physician’s opinion. Theoretically, the best and most accurate method for evaluating this factor could have been discharging all pediatric patients for 72 h and checking their probable complications and severe life-threatening health consequences; however, this strategy is not applicable practically and ethically. Therefore, as mentioned in the introduction, the best alternative was using the attending physician’s opinion on the early discharge by a hypothetical scenario. However, another alternative could be using real data during disasters. It is suggested to evaluate the sensitivity of this model in future studies using real data obtained from children discharged early from hospitals during a real disaster.
5. Conclusion
Finally, given the area under the curve of .84, the model was found at a good level and acceptable for practice to correctly identify hospitalized children for early discharge during disasters [31]. In general, the model presented in the current study can be used as a framework for developing a tool in order to recognize hospitalized children appropriate for early discharge during disasters, and consequently can increase hospital capacity during disasters.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Research Ethics Committee of Mashhad University of Medical Sciences (Code: IR.MUMS.REC.1395.430).
Funding
This study was supported by the Mashhad University of Medical Sciences.
Authors' contributions
All authors contributed to prepare this research.
Conflict of interest
All authors contributed in designing, running, and writing all parts of the research.
References
Bonnett CJ, Peery BN, Cantrill SV, Haukoos JS, McVaney KE, Colwell CB, et al., Surge capacity: A proposed conceptual framework. The American Journal of Emergency Medicine. 2007; 25(3):297-306. [DOI:10.1016/j.ajem.2006.08.011] [PMID]
Faghisolouk F, Khani Jazani R, Sohrabizadeh S. Hospital disaster risk management: The case of Urmia hospitals. Asian Journal of Pharmaceutical and Clinical Research. 2018; 11(3):447-50. [DOI:10.22159/ajpcr.2018.v11i3.23625]
Barbisch D, Haik J, Tessone A, Hanfling D. Surge capacity. In: Koenig KL, Schultz CH, editors. Koenig and Schultz’s disaster medicine: Comprehensive principles and practices. Cambridge: Cambridge University Press; 2011. [DOI:10.1017/CBO9780511902482.005]
Abolghasem Gorgi H, Jafari M, Shabanikia HR, Seyedin H, Rahimi A, Vafaee-Najar A. Hospital surge capacity in disasters in a developing country: Challenges and strategies. Trauma Monthly. 2017; 22(5):e59238. [DOI:10.5812/TRAUMAMON.59238]
Shabanikiya HR, Jafari M, Abolghasem Gorgi H, Seyedin H, Rahimi A. Developing a practical toolkit for evaluating hospital preparedness for surge capacity in disasters. International Journal of Disaster Risk Reduction. 2019; 34:423-8. [DOI:10.1016/j.ijdrr.2018.12.011]
Zhou JC, Pan KH, Huang X, Yu WQ, Zhao HC. Delayed admission to ICU does not increase the mortality of patients post neurosurgery. International Journal of Neuroscience. 2015; 125(6):420-8. [DOI:10.3109/00207454.2014.943370] [PMID]
Barbisch DF, Koenig KL. Understanding surge capacity: Essential elements. Academic Emergency Medicine. 2006; 13(11):1098-102. [DOI:10.1197/j.aem.2006.06.041] [PMID]
Hick JL, Barbera JA, Kelen GD. Refining surge capacity: Conventional, contingency, and crisis capacity. Disaster Medicine and Public Health Preparedness. 2009; 3(S1):S59-S67. [DOI:10.1097/DMP.0b013e31819f1ae2] [PMID]
Kelen GD, McCarthy ML, Kraus CK, Ding R, Hsu EB, Li G, et al. Creation of surge capacity by early discharge of hospitalized patients at low risk for untoward events. Disaster Medicine and Public Health Preparedness. 2009; 3(S1):S10-S6. [DOI:10.1097/DMP.0b013e3181a5e7cd] [PMID]
Satterthwaite PS, Atkinson CJ. Using ‘reverse triage’ to create hospital surge capacity: Royal Darwin Hospital’s response to the Ashmore Reef disaster. Emergency Medicine Journal. 2012; 29(2):160-2. [DOI:10.1136/emj.2010.098087] [PMID]
Kelen GD, Kraus CK, McCarthy ML, Bass E, Hsu EB, Li G, et al. Inpatient disposition classification for the creation of hospital surge capacity: A multiphase study. The Lancet. 2006; 368(9551):1984-90. [DOI:10.1016/S0140-6736(06)69808-5]
Pollaris G, Sabbe M. Reverse triage: More than just another method. European Journal of Emergency Medicine. 2016; 23(4):240-7. [DOI:10.1097/MEJ.0000000000000339] [PMID]
Dyb G, Jensen TK, Nygaard E, Ekeberg Ø, Diseths TH, Wentzel-Larsen T, et al. Post-traumatic stress reactions in survivors of the 2011 massacre on Utøya Island, Norway. The British Journal of Psychiatry. 2014; 204(5):361-7. [DOI:10.1192/bjp.bp.113.133157] [PMID]
Allen GM, Parrillo SJ, Will J, Mohr JA. Principles of disaster planning for the pediatric population. Prehospital and Disaster Medicine. 2007; 22(6):537-40. [DOI:10.1017/S1049023X00005392] [PMID]
Matheny Antommaria A, Powell T, Miller JE, Christian MD, Adirim T, Anderson M, et al. Ethical issues in pediatric emergency mass critical care. Pediatric Critical Care Medicine. 2011; 12(6):S163-8. [DOI:10.1097/PCC.0b013e318234a88b] [PMID]
Kanter RK. Strategies to improve pediatric disaster surge response: Potential mortality reduction and tradeoffs. Critical Care Medicine. 2007; 35(12):2837-42. [DOI:10.1097/01.CCM.0000287579.10746.43] [PMID]
Kelen GD, Sauer L, Clattenburg E, Lewis-Newby M, Fackler J. Pediatric disposition classification (Reverse Triage) system to create surge capacity. Disaster Medicine and Public Health Preparedness. 2015; 9(3):283-90. [DOI:10.1017/dmp.2015.27] [PMID]
Schull MJ, Stukel TA, Vermeulen MJ, Guttmann A, Zwarenstein M. Surge capacity associated with restrictions on nonurgent hospital utilization and expected admissions during an influenza pandemic: Lessons from the Toronto severe acute respiratory syndrome outbreak. Academic Emergency Medicine. 2006; 13(11):1228-31. [DOI:10.1197/j.aem.2006.04.011] [PMID]
Illinois Department of Public Health. Pediatric disaster triage training scenarios: Utilizing the JumpSTART Method. Illinois: Emergency Medical Services for Children; 2016. Available from: http://www.jumpstarttriage.com/uploads/Simplified_Algorithm_3.pdf
Centers for Disease Control and Prevention. Glasgow Coma Scale [Internet]. 2017 [Updated 2017 October 17]. Available from: https://www.cdc.gov/masstrauma/resources/gcs.pdf
Western Cape Government. The South African Triage Scale (SATS): Training manual. Cape Town: Western Cape Government; 2012. Available from: https://emssa.org.za/wp-content/uploads/2011/04/SATS-Manual-A5-LR-spreads.pdf
Culley JM, Svendsen E. A review of the literature on the validity of mass casualty triage systems with a focus on chemical exposures. American Journal of Disaster Medicine. 2014; 9(2):137-50. [DOI:10.5055/ajdm.2014.0150] [PMID] [PMCID]
Garner A, Lee A, Harrison K, Schultz CH. Comparative analysis of multiple-casualty incident triage algorithms. Annals of Emergency Medicine. 2001; 38(5):541-8. [DOI:10.1067/mem.2001.119053] [PMID]
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: A severity of disease classification system. Critical Care Medicine. 1985; 13(10):818-29. [DOI:10.1097/00003246-198510000-00009] [PMID]
Ministry of Health and Medical Education. [Integrated management of child illnesses (Persian)]. Tehran: Ministry of Health and Medical Education; 2016.
Baren JM. Pediatric emergency medicine. Philadelphia, PA: Saunders/Elsevier; 2008.
Horeczko T, Enriquez B, McGrath NE, Gausche-Hill M, Lewis RJ. The pediatric assessment triangle: Accuracy of its application by nurses in the triage of children. Journal of Emergency Nursing. 2013; 39(2):182-9. [DOI:10.1016/j.jen.2011.12.020] [PMID] [PMCID]
World Health Organization (WHO). Updated guideline: Paediatric emergency triage, assessment and treatment: Care of critically-ill children. Geneva: World Health Organization; 2016.
Ebrahimian AA, Shabanikiya HR, Khalesi N. The role of physiological scores for decision making in internal pre-hospital emergency situations. Journal of Society for Development in New Net Environment in B&H. 2012; 6(11):3612-5.
Gorelick MH, Alessandrini EA, Cronan K, Shults J. Revised Pediatric Emergency Assessment Tool (RePEAT): A severity index for pediatric emergency care. Academic Emergency Medicine. 2007; 14(4):316-23. [DOI:10.1197/j.aem.2006.11.015] [PMID]
Hajian-Tilaki K. Receiver Operating Characteristic (ROC) curve analysis for medical diagnostic test evaluation. Caspian Journal of Internal Medicine. 2013; 4(2):627-35. [PMID] [PMCID]
Based on the findings of this research, blood oxygen saturation level is another predictor for selecting pediatric patients appropriate for early discharge during disasters, which is consistent with the “Save a Child and Pediatric Assessment Triangle” guidelines [26, 27]. In this guideline, the ventilation status is somehow an indicator of the blood oxygen saturation level. The significance of sufficient oxygen supply for the brain and also the risk of reduced brain oxygen could explain the presence of blood oxygen saturation in the current model.
Body temperature is an indicator evaluated in most methods and algorithms evaluating children’s emergencies, namely the “Revised Pediatric Emergency Assessment Tool”, “WHO’s Pediatric Emergency Triage”, and “Assessment and Treatment Guideline”. Severe complications caused by high fevers and high body temperatures, such as convulsion can justify the presence of this variable in this model and the other models, as well [28-30].
The limitation of the current study was the used method for evaluating early discharge: ‘Appropriate for early discharge’ or ‘inappropriate for early discharge’, based on the attending physician’s opinion. Theoretically, the best and most accurate method for evaluating this factor could have been discharging all pediatric patients for 72 h and checking their probable complications and severe life-threatening health consequences; however, this strategy is not applicable practically and ethically. Therefore, as mentioned in the introduction, the best alternative was using the attending physician’s opinion on the early discharge by a hypothetical scenario. However, another alternative could be using real data during disasters. It is suggested to evaluate the sensitivity of this model in future studies using real data obtained from children discharged early from hospitals during a real disaster.
5. Conclusion
Finally, given the area under the curve of .84, the model was found at a good level and acceptable for practice to correctly identify hospitalized children for early discharge during disasters [31]. In general, the model presented in the current study can be used as a framework for developing a tool in order to recognize hospitalized children appropriate for early discharge during disasters, and consequently can increase hospital capacity during disasters.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Research Ethics Committee of Mashhad University of Medical Sciences (Code: IR.MUMS.REC.1395.430).
Funding
This study was supported by the Mashhad University of Medical Sciences.
Authors' contributions
All authors contributed to prepare this research.
Conflict of interest
All authors contributed in designing, running, and writing all parts of the research.
References
Bonnett CJ, Peery BN, Cantrill SV, Haukoos JS, McVaney KE, Colwell CB, et al., Surge capacity: A proposed conceptual framework. The American Journal of Emergency Medicine. 2007; 25(3):297-306. [DOI:10.1016/j.ajem.2006.08.011] [PMID]
Faghisolouk F, Khani Jazani R, Sohrabizadeh S. Hospital disaster risk management: The case of Urmia hospitals. Asian Journal of Pharmaceutical and Clinical Research. 2018; 11(3):447-50. [DOI:10.22159/ajpcr.2018.v11i3.23625]
Barbisch D, Haik J, Tessone A, Hanfling D. Surge capacity. In: Koenig KL, Schultz CH, editors. Koenig and Schultz’s disaster medicine: Comprehensive principles and practices. Cambridge: Cambridge University Press; 2011. [DOI:10.1017/CBO9780511902482.005]
Abolghasem Gorgi H, Jafari M, Shabanikia HR, Seyedin H, Rahimi A, Vafaee-Najar A. Hospital surge capacity in disasters in a developing country: Challenges and strategies. Trauma Monthly. 2017; 22(5):e59238. [DOI:10.5812/TRAUMAMON.59238]
Shabanikiya HR, Jafari M, Abolghasem Gorgi H, Seyedin H, Rahimi A. Developing a practical toolkit for evaluating hospital preparedness for surge capacity in disasters. International Journal of Disaster Risk Reduction. 2019; 34:423-8. [DOI:10.1016/j.ijdrr.2018.12.011]
Zhou JC, Pan KH, Huang X, Yu WQ, Zhao HC. Delayed admission to ICU does not increase the mortality of patients post neurosurgery. International Journal of Neuroscience. 2015; 125(6):420-8. [DOI:10.3109/00207454.2014.943370] [PMID]
Barbisch DF, Koenig KL. Understanding surge capacity: Essential elements. Academic Emergency Medicine. 2006; 13(11):1098-102. [DOI:10.1197/j.aem.2006.06.041] [PMID]
Hick JL, Barbera JA, Kelen GD. Refining surge capacity: Conventional, contingency, and crisis capacity. Disaster Medicine and Public Health Preparedness. 2009; 3(S1):S59-S67. [DOI:10.1097/DMP.0b013e31819f1ae2] [PMID]
Kelen GD, McCarthy ML, Kraus CK, Ding R, Hsu EB, Li G, et al. Creation of surge capacity by early discharge of hospitalized patients at low risk for untoward events. Disaster Medicine and Public Health Preparedness. 2009; 3(S1):S10-S6. [DOI:10.1097/DMP.0b013e3181a5e7cd] [PMID]
Satterthwaite PS, Atkinson CJ. Using ‘reverse triage’ to create hospital surge capacity: Royal Darwin Hospital’s response to the Ashmore Reef disaster. Emergency Medicine Journal. 2012; 29(2):160-2. [DOI:10.1136/emj.2010.098087] [PMID]
Kelen GD, Kraus CK, McCarthy ML, Bass E, Hsu EB, Li G, et al. Inpatient disposition classification for the creation of hospital surge capacity: A multiphase study. The Lancet. 2006; 368(9551):1984-90. [DOI:10.1016/S0140-6736(06)69808-5]
Pollaris G, Sabbe M. Reverse triage: More than just another method. European Journal of Emergency Medicine. 2016; 23(4):240-7. [DOI:10.1097/MEJ.0000000000000339] [PMID]
Dyb G, Jensen TK, Nygaard E, Ekeberg Ø, Diseths TH, Wentzel-Larsen T, et al. Post-traumatic stress reactions in survivors of the 2011 massacre on Utøya Island, Norway. The British Journal of Psychiatry. 2014; 204(5):361-7. [DOI:10.1192/bjp.bp.113.133157] [PMID]
Allen GM, Parrillo SJ, Will J, Mohr JA. Principles of disaster planning for the pediatric population. Prehospital and Disaster Medicine. 2007; 22(6):537-40. [DOI:10.1017/S1049023X00005392] [PMID]
Matheny Antommaria A, Powell T, Miller JE, Christian MD, Adirim T, Anderson M, et al. Ethical issues in pediatric emergency mass critical care. Pediatric Critical Care Medicine. 2011; 12(6):S163-8. [DOI:10.1097/PCC.0b013e318234a88b] [PMID]
Kanter RK. Strategies to improve pediatric disaster surge response: Potential mortality reduction and tradeoffs. Critical Care Medicine. 2007; 35(12):2837-42. [DOI:10.1097/01.CCM.0000287579.10746.43] [PMID]
Kelen GD, Sauer L, Clattenburg E, Lewis-Newby M, Fackler J. Pediatric disposition classification (Reverse Triage) system to create surge capacity. Disaster Medicine and Public Health Preparedness. 2015; 9(3):283-90. [DOI:10.1017/dmp.2015.27] [PMID]
Schull MJ, Stukel TA, Vermeulen MJ, Guttmann A, Zwarenstein M. Surge capacity associated with restrictions on nonurgent hospital utilization and expected admissions during an influenza pandemic: Lessons from the Toronto severe acute respiratory syndrome outbreak. Academic Emergency Medicine. 2006; 13(11):1228-31. [DOI:10.1197/j.aem.2006.04.011] [PMID]
Illinois Department of Public Health. Pediatric disaster triage training scenarios: Utilizing the JumpSTART Method. Illinois: Emergency Medical Services for Children; 2016. Available from: http://www.jumpstarttriage.com/uploads/Simplified_Algorithm_3.pdf
Centers for Disease Control and Prevention. Glasgow Coma Scale [Internet]. 2017 [Updated 2017 October 17]. Available from: https://www.cdc.gov/masstrauma/resources/gcs.pdf
Western Cape Government. The South African Triage Scale (SATS): Training manual. Cape Town: Western Cape Government; 2012. Available from: https://emssa.org.za/wp-content/uploads/2011/04/SATS-Manual-A5-LR-spreads.pdf
Culley JM, Svendsen E. A review of the literature on the validity of mass casualty triage systems with a focus on chemical exposures. American Journal of Disaster Medicine. 2014; 9(2):137-50. [DOI:10.5055/ajdm.2014.0150] [PMID] [PMCID]
Garner A, Lee A, Harrison K, Schultz CH. Comparative analysis of multiple-casualty incident triage algorithms. Annals of Emergency Medicine. 2001; 38(5):541-8. [DOI:10.1067/mem.2001.119053] [PMID]
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: A severity of disease classification system. Critical Care Medicine. 1985; 13(10):818-29. [DOI:10.1097/00003246-198510000-00009] [PMID]
Ministry of Health and Medical Education. [Integrated management of child illnesses (Persian)]. Tehran: Ministry of Health and Medical Education; 2016.
Baren JM. Pediatric emergency medicine. Philadelphia, PA: Saunders/Elsevier; 2008.
Horeczko T, Enriquez B, McGrath NE, Gausche-Hill M, Lewis RJ. The pediatric assessment triangle: Accuracy of its application by nurses in the triage of children. Journal of Emergency Nursing. 2013; 39(2):182-9. [DOI:10.1016/j.jen.2011.12.020] [PMID] [PMCID]
World Health Organization (WHO). Updated guideline: Paediatric emergency triage, assessment and treatment: Care of critically-ill children. Geneva: World Health Organization; 2016.
Ebrahimian AA, Shabanikiya HR, Khalesi N. The role of physiological scores for decision making in internal pre-hospital emergency situations. Journal of Society for Development in New Net Environment in B&H. 2012; 6(11):3612-5.
Gorelick MH, Alessandrini EA, Cronan K, Shults J. Revised Pediatric Emergency Assessment Tool (RePEAT): A severity index for pediatric emergency care. Academic Emergency Medicine. 2007; 14(4):316-23. [DOI:10.1197/j.aem.2006.11.015] [PMID]
Hajian-Tilaki K. Receiver Operating Characteristic (ROC) curve analysis for medical diagnostic test evaluation. Caspian Journal of Internal Medicine. 2013; 4(2):627-35. [PMID] [PMCID]
Type of article: Research |
Subject:
Special
Received: 2019/07/19 | Accepted: 2019/10/28 | Published: 2020/04/8
Received: 2019/07/19 | Accepted: 2019/10/28 | Published: 2020/04/8
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
