

Volume 8, Issue 1 (Autumn 2022)
Health in Emergencies and Disasters Quarterly 2022, 8(1): 55-64 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Soltanzadeh A, Mahdinia M, Mohammadfam I. Fuzzy Logic-based Risk Analysis of COVID-19 Infection: A Case Study in Healthcare Facilities. Health in Emergencies and Disasters Quarterly 2022; 8 (1) :55-64
URL: http://hdq.uswr.ac.ir/article-1-433-en.html
URL: http://hdq.uswr.ac.ir/article-1-433-en.html



1- Department of Occupational Health and Safety Engineering, Environmental Pollutants Research Center, School of Health, Qom University of Medical Sciences, Qom, Iran.
2- Department of Ergonomics, Health Research Center in Accidents and Disasters, University of Rehabilitation Sciences and Social Health, Tehran, Iran. ,ir.mohammadfam@uswr.ac.ir
2- Department of Ergonomics, Health Research Center in Accidents and Disasters, University of Rehabilitation Sciences and Social Health, Tehran, Iran. ,
Full-Text [PDF 627 kb]
(1678 Downloads)
| Abstract (HTML) (4128 Views)
Full-Text: (950 Views)
1. Introduction
With the official announcement of the COVID-19 pandemic by the World Health Organization (WHO) on March 11, 2020, many efforts and studies have been made to identify the origin of this viral disease, the ways of infections, and the methods to prevent it, the treatment mechanisms, as well as the development of a vaccine for the virus and it is still under research. The main volume of all kinds of studies in the world due to COVID-19 is known as the largest challenge of the century for public health, international economy, and national and even the international policies in most fields [1-3].
Today, modern global standards and management systems establishing and implementing these standards show that identifying potentially harmful risks and sources, along with the risk assessment of the occurrence of an event or disturbance caused by the actualization of these risks, is one of the crucial steps in the implementation and optimal establishment of management systems based on novel worldwide standards and perhaps the vital goal of establishing these systems is for of the sustainable development and continuous improvement. The results of the establishment of new structures governing the management of systems, including production and service organizations, show that the main consequence of identifying and assessing the risk of dangers that threaten the health and safety of human resources as the main base of a system will cause the success of that organization and leads to its continuous productivity. Therefore, according to the main consequence of the COVID-19 pandemic, which affects people’s health, safety, and life, taking any action to reduce the risk of COVID-19 can improve the efficiency and effectiveness of a working system and can return organizational productivity to the initial conditions before the outbreak of pandemic [4-7].
COVID-19 threatens the health of human resources as the critical pillar of job societies. It has a high viral speed; therefore according to global statistics until January 2, 2021, it has infected 84 480 308 people and has caused the death of 1 837 569 people in the world in less than a year. Therefore, based on these terrible statistics, one should try to reduce the risk of viral infection by using different methods [8, 9].
Although in various working places, different methods have been developed to analyze the risks threatening the health and safety of people and assets in the working regions, most of these methods and techniques are based on dangers and harmful physical, chemical, and ergonomic factors in the working area which is known as the most common sources of high risk in the work environments to date. The risk analysis of biological hazard sources, such as the causative agent of COVID-19 is very different from the risk analysis of ergonomic, chemical, and physical dangers that have been used in manufacturing and service industries and organizations to date. Due to the existence of standard values for exposure to most risks (ergonomic, chemical and physical), one of the most common methods of risk analysis of these hazards includes measuring the level of exposure to ergonomic, chemical and physical risks by quantifying them and determining the amount of individual environmental exposure, and comparing the measured values with the standard and permissible limits of exposure to these risks [10, 11]. If the risk assessment and analysis of exposure to different types of biological risk sources are based on factors, such as the hazard potential of the biological agent, the sensitivity of the exposed person or persons, the ability to cause disease and damage by the biological agent, the stability of the biological agent in the exposure environment, the access status to primary preventive and therapeutic care, as well as the level of preparedness of the advanced medical system of that society about the source of biological risk and other factors [12], in addition, the risk of contracting diseases related to harmful biological factors using a qualitative or semi-quantitative method can often be estimated and analyzed.
According to the previously mentioned cases, the spread of COVID-19 to the working area based on different studies and reports in which the various effects of the COVID-19 on the health of workers have been pointed out [12-15], Mohammadfam and Mirzaei Aliabadi (2020) presented a technique to assess the risk of exposure of workers to this disease called, rapid COVID-19 hazard analysis (RCHA) [16]. The technique developed in this study included the analysis of COVID-19 risk based on three parameters, including the severity of the outcome, the level of the person’s health attitude, and the probability of infection. In this technique, qualitative and semi-quantitative risk assessment methods have been used to estimate COVID-19 risk [17]. Therefore, to quantify COVID-19 risk and reduce or eliminate the errors caused by using people’s opinions, this study was designed and conducted to analyzing COVID-19 risk based on fuzzy logic.
2. Materials and Methods
Participants
This study was a cross-sectional and descriptive-analytical survey that was conducted in the health and treatment sector as the crucial occupational environment facing the risk of COVID-19 (2019). This study is based on the quick risk analysis technique of COVID-19 designed by Mohammadfam and Mirzaei Aliabadi (RCHA) [16] and using fuzzy logic.
Population
The people evaluated in this study were selected from the employees working in 5 hospitals and treatment centers as the crucial occupational environment with the risk of COVID-19. The sample size was calculated for this study based on the results achieved by Mohammadfam et al. (2020) [17], considering the unlimited population and the error level of 0.04, including 228 people. According to the selection of samples from 5 hospitals and medical centers, proportional distribution sampling or classification sampling was used to select the number of samples. The factors influenced the study included at least one year of work experience and exposure to patients and companions of patients with or suspected of having COVID-19. The exclusion criteria for this study included insufficient satisfaction to participate in the study. To increase the power of the study and also to predict the withdrawal of some samples from the study, the number of samples that entered the study was 10% more than the calculated sample and included 251 people.
Fuzzification of rapid COVID-19 hazard analysis (RCHA)
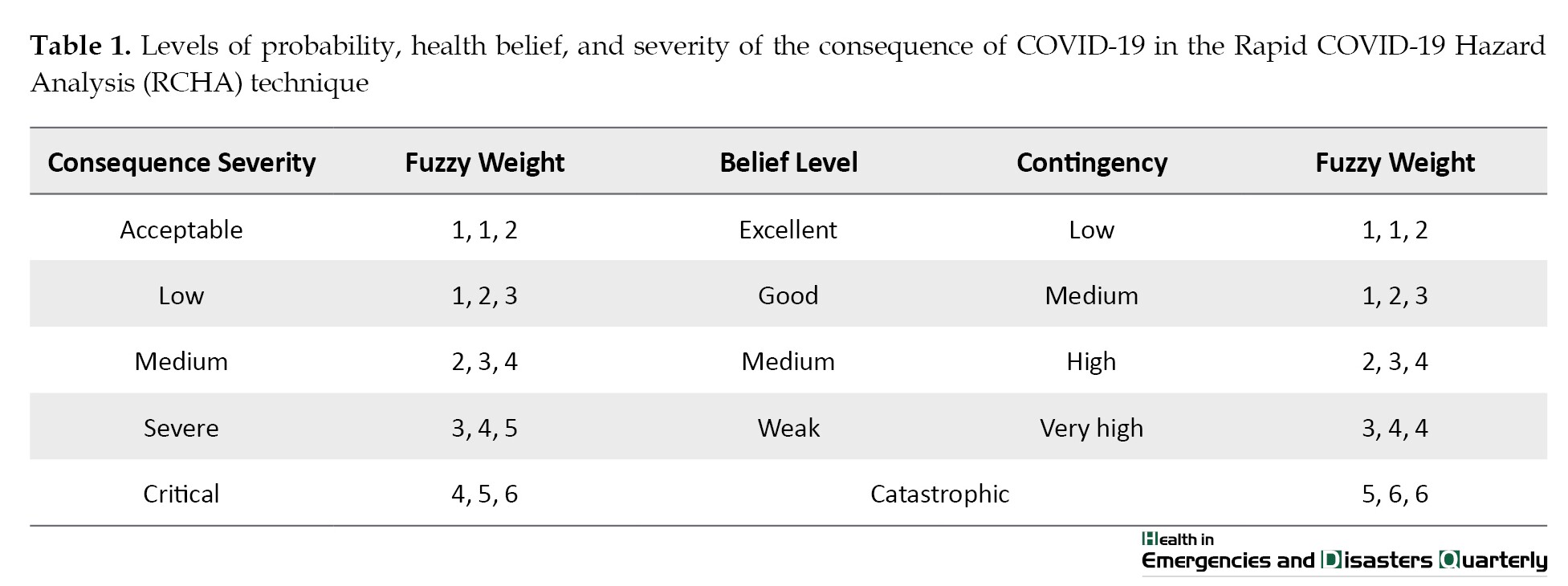
The rapid analysis technique of COVID-19 risk has estimated the risk level based on three components, such as the probability of the disease, the level of the individual’s health belief, and the severity of the consequences. The probability of disease component is divided into four levels from low to very high, the health belief level component is divided into four levels from weak to excellent, and the consequence severity component is divided into six acceptable to catastrophic levels (Table 1) [16].
As is common in many risk assessment methods, including the method used in this study, the opinion of the assessors about the levels of the main components of the risk level is usually expressed in the form imprecise, inconclusive, and ambiguous linguistic expressions, and this makes it difficult to analyze and summarize the results [18]. In these cases, quantifying the results with the definite scoring methods is faced with ambiguity caused by the judgment of people, and on the other hand, the changes in the value of linguistic expressions are ignored by converting them into numbers, and as a result, the subjective judgment of people and the choice of priorities have a great impact on the results [19]. Since fuzzy logic is a very useful tool to measure ambiguous concepts related to people’s mental judgments [18], as a result, it is a powerful tool suitable to overcome the mentioned problems and makes it possible to obtain more accurate information in the form of verbal expressions [20, 21]. Therefore, based on the objectives of this study, to weight and quantify the mentioned levels for the three main components of the risk level, instead of using definite numbers used in the study by Mohammadfam and Mirzaei Aliabadi [16], triangular fuzzy numbers were used.
Fuzzy logic is a form of multi-valued logic that is used to apply the concept of partial correctness so that the values are between completely true and completely false. This theory is a strong tool to deal with the ambiguity and uncertainty of human judgment and evaluation in decision-making. According to fuzzy logic, fuzzy logic and fuzzy numbers are used instead of Aristotelian logic and classical numbers to value a phenomenon [22]. Therefore, in the present study, triangular fuzzy numbers were used instead of definite numbers to score different levels of the three components of the risk level. Fuzzy numbers have different types, the most useful of which are triangular fuzzy numbers. A triangular fuzzy number is represented as A= (l, m, u) where l, m, and u are defining a fuzzy set. The upper bound, denoted by u, is the maximum value that the fuzzy number A can take. The lower limit indicated by l is the minimum value that the fuzzy number A can take. The value of m is the most probable value of a fuzzy number.
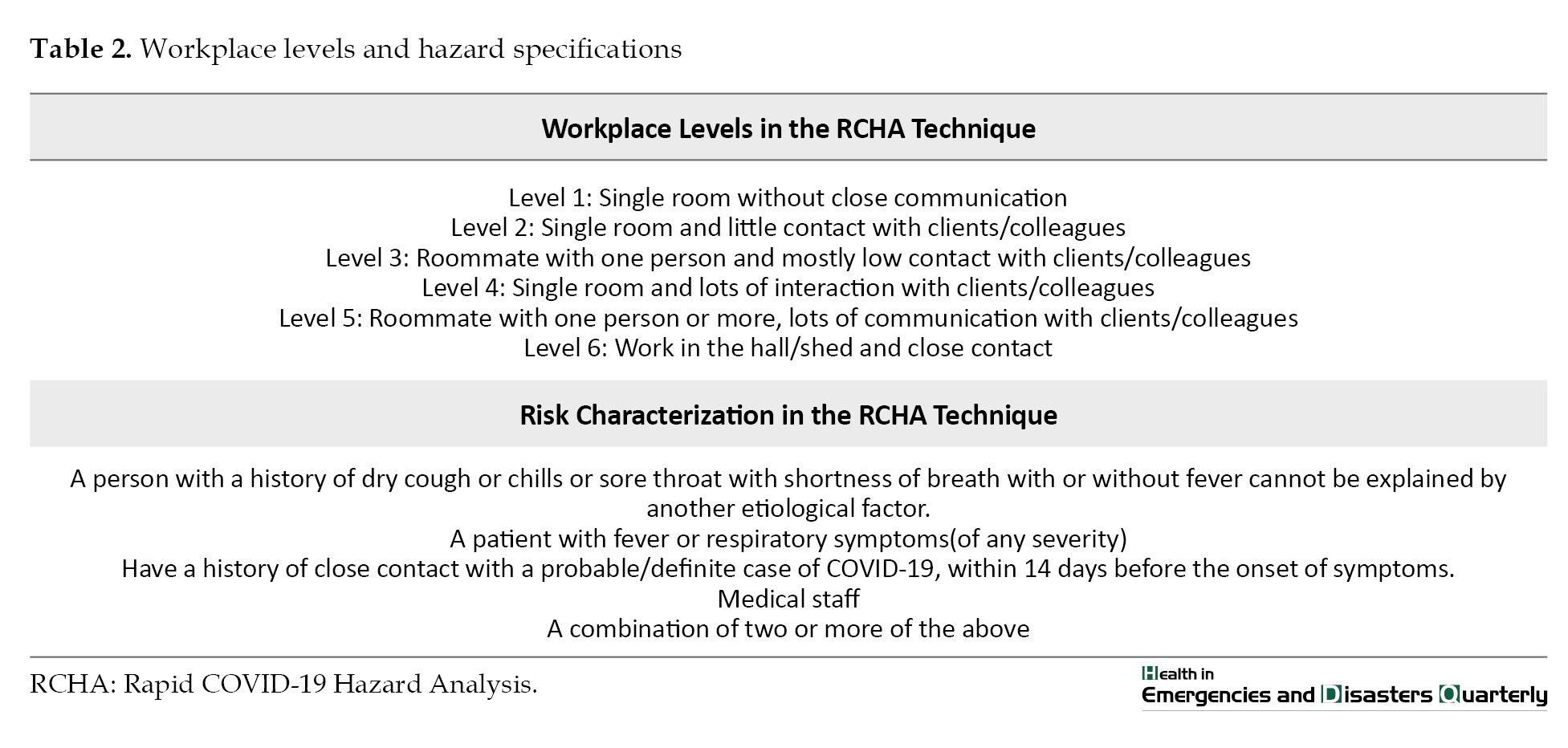
By definition of risk, the characteristics of the type of job, workplace, and risk specification are used for the proper estimation and interpretation of the evaluators of probability, consequence, and intensity components. People’s workplaces were in six levels one to six and the risk characteristics according to the risk definition included 5 characteristics A, B, C, D, and E (Table 2) [16, 17]. Relying on the fuzzy analysis of COVID-19 risk, the final number or index is obtained from the product of these three components of probability, consequence, and intensity and has a range between 1.25 and 73.5. According to this, the absolute COVID-19 risk is based on three levels of risk, including level 1 or acceptable (1.25-1.5), level 2 or tolerable, but the need to take corrective actions and solutions (12.25-5.0) and level 3 or unacceptable (25.73-0.5) was divided.
3. Results
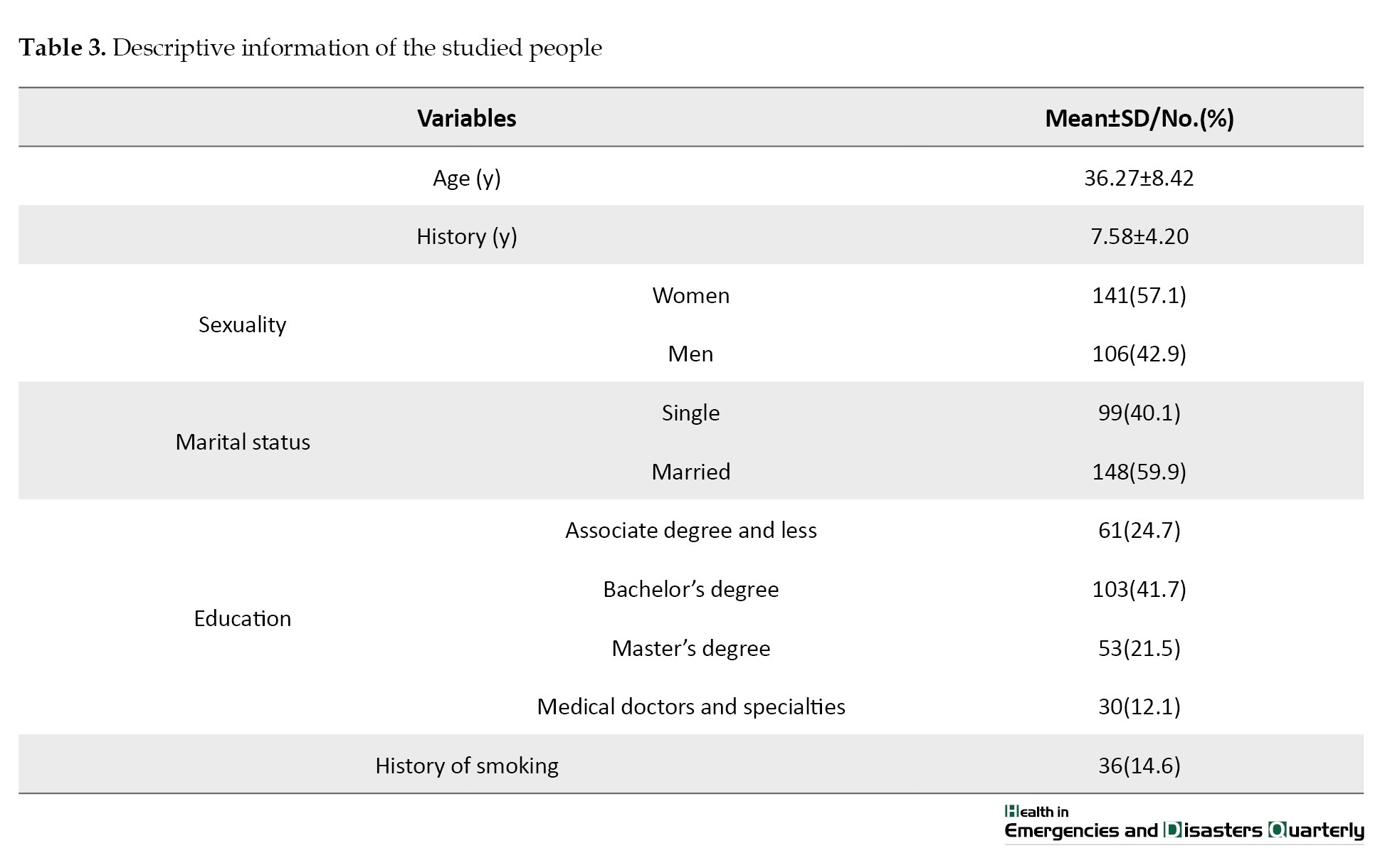
A total of 247 employees from five hospitals and medical centers participated in this study. The studied people include eight groups of doctors and specialists (21 people), superintendent (16 people), ward services (21 people), receptionist and secretary (19 people), nurses (115 people), porters (25 people), and laboratory experts (23 people) and Computerized Tomography (CT) scan expert (7 people). The Mean±SD age and work experience of these people were 36.27±8.42 and 7.58±4.20 years, respectively. The evaluated people included 57.1% women and 42.9% men; 40.1% of the studied people were single and 59.9% were married. The results of the survey on the level of education of the people studied in these health and treatment centers showed that almost one-fifth of the people studied had a post-secondary education or less (24.7%), 41.7% had a bachelor’s degree, and more than 20% had a master’s degree (21.5%) and more than 10% had a doctorate and specialty education (12.1%). Also, 14.6% of the studied subjects had a history of smoking (Table 3).
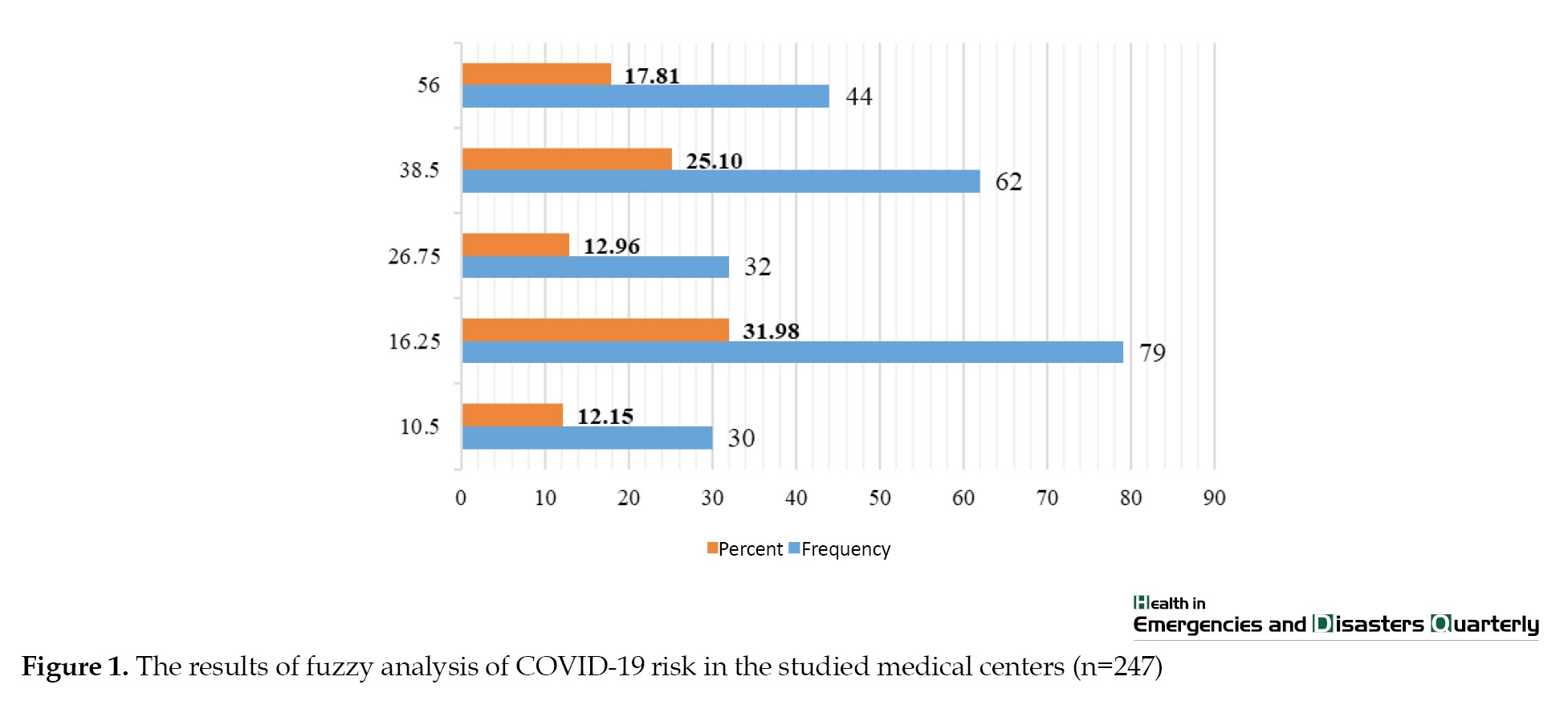
The findings of the analysis of COVID-19 risk based on fuzzy logic in the studied medical centers showed that the studied people were placed in five risk levels, including 10.5, 16.25, 26.75, 38.5 and 56. The highest and lowest frequency of COVID-19 risk was related to the risk levels of 16.25 and 10.5 with 31.98% and 12.15%, respectively (Figure 1).
Level of definite COVID-19 risk vs percent (red) and frequency (blue)
The evaluation of the results obtained from the calculation and analysis of COVID-19 risk based on fuzzy logic showed that of the 247 people studied, 12.15% were at an acceptable risk level, about one-third (31.98%) of the people in tolerable risk level and more than half of them (55.87%) are in unacceptable risk level. These results showed that the highest level of COVID-19 risk belongs to the group of nurses with a definite risk level of 56.0. The lowest level of COVID-19 risk was related to six groups of medical doctors and specialists, supervisors, receptionists and ward secretaries, laboratory experts and CT scan experts with a definite risk level equal to 5.10.
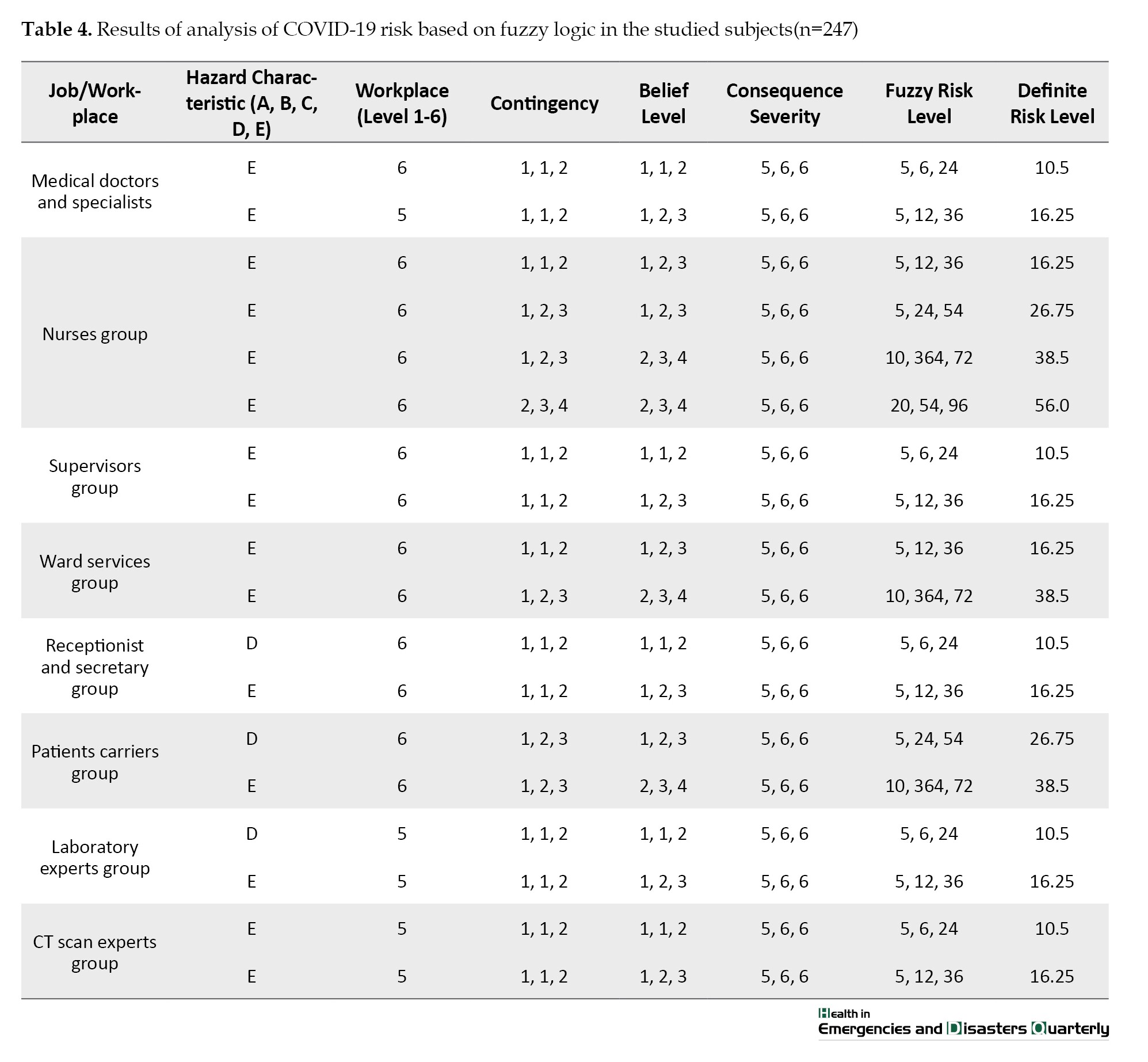
The results of fuzzy analysis of COVID-19 risk revealed that the group of nurses is in four risk levels and seven other groups, including groups of doctors and specialists, supervisors, ward services, receptionists and secretaries, patients’ carriers, laboratory experts and CT scan experts, each of them is in two risk levels. In the group of medical doctors and specialists, 8 people faced a risk level of 10.5 and 13 people faced a risk level of 16.25. The level of COVID-19 risk was estimated 10.5 for 7 people from the group of supervisors and 16.25 for 9 people. In the service group, 6 people faced a risk level of 16.25 and 15 people faced a risk level of 38.5. The level of COVID-19 risk in 8 and 11 people in the receptionist group was calculated 10.5 and 16.25, respectively. In the patients’ porters group, 11 people faced a risk level of 26.75 and 14 people faced a risk level of 38.5. Five laboratory experts and 2 CT scan department experts have a definite COVID-19 risk equal to 10.5. In addition, the level of COVID-19 risk was estimated 16.25 for 18 laboratory experts and 5 CT scan department experts. Calculating the COVID-19 risk based on fuzzy logic in the group of nurses with four different risk levels showed that 17 people face a risk level of 16.25 and 21 people face a risk level of 26.75. This analysis showed that the definite risk level of COVID-19 was calculated as 38.5 for 33 people and 56.0 for 44 people (Table 4).
4. Discussion
The results of various studies have shown that the spread of the COVID-19 has caused countless challenges in the human, economic, social, and even political fields. Its prevalence reduced the level and rate of organizational productivity, including the effectiveness of providing products and services, and directly and indirectly caused all kinds of damage to the human resources of organizations [14, 23]. Due to its high contagiousness and the need to provide various types of medical services in treatment centers and hospitals, one of the crucial centers of COVID-19 risk includes these centers [24, 25]. Previous findings have shown that the epidemic of viral diseases, in addition to infecting workers, can also affect the job performance of people in the workplace and cause them unable to perform their job duties. Also, the physical and mental effects of these diseases can have a lasting impact on people’s general health and lead to the accidents and injuries in the workplace. Therefore, protecting the physical and mental health of employees is essential to control this pandemic and reduce the risk of contracting it [26, 27]. The results of Mohammadfam et al.’s study in three occupational environments, including bank, postal and medical center employees, showed that the level of COVID-19 risk is high for all the people studied [17].
Although Mohammadfam and Mirzaei Aliabadi in their studies have designed, presented, and implemented RCHA to screen people suspected of COVID-19 disease in work environments [16, 17], the review of these studies and attention to the types of the consequences and direct and collateral damage caused by COVID-19 show that the error of diagnosis and human estimation can exist in this risk assessment, despite the qualitative assessment and semi-quantitative estimation of COVID-19 risk based on this method can lead to a good estimate of COVID-19 risk. Therefore, this study was designed and implemented with the approach of applying fuzzy logic and based on RCHA in medical environments.
The results of this study indicated that more than half of the people studied are at high risk of COVID-19. Findings stated that the combination of fuzzy logic and RCHA can help or lead to a more accurate estimate of exposure to COVID-19 risk. The results of the fuzzy analysis of COVID-19 risk showed that the lowest and highest definite risk estimates were equal to 10.5 and 56.0. These results revealed that the group of nurses has the highest risk of COVID-19 compared to the other seven groups working in the studied medical centers, including the group of doctors and specialists, supervisors, ward services, receptionists and secretaries, patients’ carriers, laboratory experts, and CT scan experts. These results showed that the definite COVID-19 risk in nurses is 16.25, 26.75, 38.5, and 56.0 in four levels. In addition, they indicated that after group of nurses, group of patient carriers with a definite risk level of 26.75 and 38.5 as well as the group of ward services with a definite risk level of 16.25 and 38.5 respectively, have the highest COVID-19 risk. Therefore, it shows that the risk of COVID-19 in these three occupational groups in medical centers is very high, and due to the high prevalence of it, protective and health measures should be taken according to the risk level for these three groups. In addition, these three groups should be prioritized in the design and implementation of various strategies to reduce COVID-19 risk. In addition, the results of Schröder’s study (2020) show that despite the low lethality of the COVID-19 compared to other viral and infectious diseases, such as Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS), the risk of this disease is high due to its high contagion power in environments with high communication possibilities. Therefore, implementing a risk assessment program in which parameters, such as time of exposure to the source (for example, infected people), and distance to the source can lead to measures that causes a reduction in the incidence of this disease [28]. Also, the results of Chatterjee’s study (2020) show that the development of a risk assessment tool is very useful for creating awareness and decision-making, and the results of this assessment can be very effective for the response and the management of COVID-19 [29].
Based on the findings as well as the purpose of designing and implementing in this study, which included the analysis of COVID-19 risk based on fuzzy logic, the use of fuzzy logic according to the instructions provided can act as a suitable complement to the technique of quick analysis of the risk of COVID-19, therefore this approach can be used as a simple, fast, low-cost and high-accuracy method to assess COVID-19 risk for various purposes, including the screening of workplaces for COVID-19 to determine priorities to design and implement corrective measures as well as a criterion for macro-management decisions.
5. Conclusion
The results of the study indicated that the use of fuzzy logic to assess the COVID-19 risk based on the developed method (RCHA) can lead to an acceptable and appropriate estimate of it, especially in high-risk jobs, such as working in medical centers. Also, the results of the fuzzy analysis of COVID-19 risk demonstrated that it was higher for the three groups of nurses, patient carriers, and ward services. Therefore, in designing and implementing the necessary strategies to reduce COVID-19 risk, these groups should be prioritized for the COVID-19.
Ethical Considerations
Compliance with ethical guidelines
The present study was registered as a research project in the Ethics Committee of Qom University of Medical Sciences (Code: IR.MUQ.REC.1399.228).
Funding
This article is a part of research project (No.: 1564) approved by the Vice-chancellor for Research and Technology of Qom University of Medical Sciences.
Authors' contributions
Study concept and design: Iraj Mohammadfam and Ahmad Soltanzadeh; Data analysis and interpretation of data: Mohsen Mahdinia; Writing--original draft: Ahmad Soltanzadeh and Mohsen Mahdinia; Review of the article and final approval: Iraj Mohammadfam; Data collection, reading, and approval of the final manuscript: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
With the official announcement of the COVID-19 pandemic by the World Health Organization (WHO) on March 11, 2020, many efforts and studies have been made to identify the origin of this viral disease, the ways of infections, and the methods to prevent it, the treatment mechanisms, as well as the development of a vaccine for the virus and it is still under research. The main volume of all kinds of studies in the world due to COVID-19 is known as the largest challenge of the century for public health, international economy, and national and even the international policies in most fields [1-3].
Today, modern global standards and management systems establishing and implementing these standards show that identifying potentially harmful risks and sources, along with the risk assessment of the occurrence of an event or disturbance caused by the actualization of these risks, is one of the crucial steps in the implementation and optimal establishment of management systems based on novel worldwide standards and perhaps the vital goal of establishing these systems is for of the sustainable development and continuous improvement. The results of the establishment of new structures governing the management of systems, including production and service organizations, show that the main consequence of identifying and assessing the risk of dangers that threaten the health and safety of human resources as the main base of a system will cause the success of that organization and leads to its continuous productivity. Therefore, according to the main consequence of the COVID-19 pandemic, which affects people’s health, safety, and life, taking any action to reduce the risk of COVID-19 can improve the efficiency and effectiveness of a working system and can return organizational productivity to the initial conditions before the outbreak of pandemic [4-7].
COVID-19 threatens the health of human resources as the critical pillar of job societies. It has a high viral speed; therefore according to global statistics until January 2, 2021, it has infected 84 480 308 people and has caused the death of 1 837 569 people in the world in less than a year. Therefore, based on these terrible statistics, one should try to reduce the risk of viral infection by using different methods [8, 9].
Although in various working places, different methods have been developed to analyze the risks threatening the health and safety of people and assets in the working regions, most of these methods and techniques are based on dangers and harmful physical, chemical, and ergonomic factors in the working area which is known as the most common sources of high risk in the work environments to date. The risk analysis of biological hazard sources, such as the causative agent of COVID-19 is very different from the risk analysis of ergonomic, chemical, and physical dangers that have been used in manufacturing and service industries and organizations to date. Due to the existence of standard values for exposure to most risks (ergonomic, chemical and physical), one of the most common methods of risk analysis of these hazards includes measuring the level of exposure to ergonomic, chemical and physical risks by quantifying them and determining the amount of individual environmental exposure, and comparing the measured values with the standard and permissible limits of exposure to these risks [10, 11]. If the risk assessment and analysis of exposure to different types of biological risk sources are based on factors, such as the hazard potential of the biological agent, the sensitivity of the exposed person or persons, the ability to cause disease and damage by the biological agent, the stability of the biological agent in the exposure environment, the access status to primary preventive and therapeutic care, as well as the level of preparedness of the advanced medical system of that society about the source of biological risk and other factors [12], in addition, the risk of contracting diseases related to harmful biological factors using a qualitative or semi-quantitative method can often be estimated and analyzed.
According to the previously mentioned cases, the spread of COVID-19 to the working area based on different studies and reports in which the various effects of the COVID-19 on the health of workers have been pointed out [12-15], Mohammadfam and Mirzaei Aliabadi (2020) presented a technique to assess the risk of exposure of workers to this disease called, rapid COVID-19 hazard analysis (RCHA) [16]. The technique developed in this study included the analysis of COVID-19 risk based on three parameters, including the severity of the outcome, the level of the person’s health attitude, and the probability of infection. In this technique, qualitative and semi-quantitative risk assessment methods have been used to estimate COVID-19 risk [17]. Therefore, to quantify COVID-19 risk and reduce or eliminate the errors caused by using people’s opinions, this study was designed and conducted to analyzing COVID-19 risk based on fuzzy logic.
2. Materials and Methods
Participants
This study was a cross-sectional and descriptive-analytical survey that was conducted in the health and treatment sector as the crucial occupational environment facing the risk of COVID-19 (2019). This study is based on the quick risk analysis technique of COVID-19 designed by Mohammadfam and Mirzaei Aliabadi (RCHA) [16] and using fuzzy logic.
Population
The people evaluated in this study were selected from the employees working in 5 hospitals and treatment centers as the crucial occupational environment with the risk of COVID-19. The sample size was calculated for this study based on the results achieved by Mohammadfam et al. (2020) [17], considering the unlimited population and the error level of 0.04, including 228 people. According to the selection of samples from 5 hospitals and medical centers, proportional distribution sampling or classification sampling was used to select the number of samples. The factors influenced the study included at least one year of work experience and exposure to patients and companions of patients with or suspected of having COVID-19. The exclusion criteria for this study included insufficient satisfaction to participate in the study. To increase the power of the study and also to predict the withdrawal of some samples from the study, the number of samples that entered the study was 10% more than the calculated sample and included 251 people.
Fuzzification of rapid COVID-19 hazard analysis (RCHA)
The rapid analysis technique of COVID-19 risk has estimated the risk level based on three components, such as the probability of the disease, the level of the individual’s health belief, and the severity of the consequences. The probability of disease component is divided into four levels from low to very high, the health belief level component is divided into four levels from weak to excellent, and the consequence severity component is divided into six acceptable to catastrophic levels (Table 1) [16].
As is common in many risk assessment methods, including the method used in this study, the opinion of the assessors about the levels of the main components of the risk level is usually expressed in the form imprecise, inconclusive, and ambiguous linguistic expressions, and this makes it difficult to analyze and summarize the results [18]. In these cases, quantifying the results with the definite scoring methods is faced with ambiguity caused by the judgment of people, and on the other hand, the changes in the value of linguistic expressions are ignored by converting them into numbers, and as a result, the subjective judgment of people and the choice of priorities have a great impact on the results [19]. Since fuzzy logic is a very useful tool to measure ambiguous concepts related to people’s mental judgments [18], as a result, it is a powerful tool suitable to overcome the mentioned problems and makes it possible to obtain more accurate information in the form of verbal expressions [20, 21]. Therefore, based on the objectives of this study, to weight and quantify the mentioned levels for the three main components of the risk level, instead of using definite numbers used in the study by Mohammadfam and Mirzaei Aliabadi [16], triangular fuzzy numbers were used.
Fuzzy logic is a form of multi-valued logic that is used to apply the concept of partial correctness so that the values are between completely true and completely false. This theory is a strong tool to deal with the ambiguity and uncertainty of human judgment and evaluation in decision-making. According to fuzzy logic, fuzzy logic and fuzzy numbers are used instead of Aristotelian logic and classical numbers to value a phenomenon [22]. Therefore, in the present study, triangular fuzzy numbers were used instead of definite numbers to score different levels of the three components of the risk level. Fuzzy numbers have different types, the most useful of which are triangular fuzzy numbers. A triangular fuzzy number is represented as A= (l, m, u) where l, m, and u are defining a fuzzy set. The upper bound, denoted by u, is the maximum value that the fuzzy number A can take. The lower limit indicated by l is the minimum value that the fuzzy number A can take. The value of m is the most probable value of a fuzzy number.
By definition of risk, the characteristics of the type of job, workplace, and risk specification are used for the proper estimation and interpretation of the evaluators of probability, consequence, and intensity components. People’s workplaces were in six levels one to six and the risk characteristics according to the risk definition included 5 characteristics A, B, C, D, and E (Table 2) [16, 17]. Relying on the fuzzy analysis of COVID-19 risk, the final number or index is obtained from the product of these three components of probability, consequence, and intensity and has a range between 1.25 and 73.5. According to this, the absolute COVID-19 risk is based on three levels of risk, including level 1 or acceptable (1.25-1.5), level 2 or tolerable, but the need to take corrective actions and solutions (12.25-5.0) and level 3 or unacceptable (25.73-0.5) was divided.
3. Results
A total of 247 employees from five hospitals and medical centers participated in this study. The studied people include eight groups of doctors and specialists (21 people), superintendent (16 people), ward services (21 people), receptionist and secretary (19 people), nurses (115 people), porters (25 people), and laboratory experts (23 people) and Computerized Tomography (CT) scan expert (7 people). The Mean±SD age and work experience of these people were 36.27±8.42 and 7.58±4.20 years, respectively. The evaluated people included 57.1% women and 42.9% men; 40.1% of the studied people were single and 59.9% were married. The results of the survey on the level of education of the people studied in these health and treatment centers showed that almost one-fifth of the people studied had a post-secondary education or less (24.7%), 41.7% had a bachelor’s degree, and more than 20% had a master’s degree (21.5%) and more than 10% had a doctorate and specialty education (12.1%). Also, 14.6% of the studied subjects had a history of smoking (Table 3).
The findings of the analysis of COVID-19 risk based on fuzzy logic in the studied medical centers showed that the studied people were placed in five risk levels, including 10.5, 16.25, 26.75, 38.5 and 56. The highest and lowest frequency of COVID-19 risk was related to the risk levels of 16.25 and 10.5 with 31.98% and 12.15%, respectively (Figure 1).
Level of definite COVID-19 risk vs percent (red) and frequency (blue)
The evaluation of the results obtained from the calculation and analysis of COVID-19 risk based on fuzzy logic showed that of the 247 people studied, 12.15% were at an acceptable risk level, about one-third (31.98%) of the people in tolerable risk level and more than half of them (55.87%) are in unacceptable risk level. These results showed that the highest level of COVID-19 risk belongs to the group of nurses with a definite risk level of 56.0. The lowest level of COVID-19 risk was related to six groups of medical doctors and specialists, supervisors, receptionists and ward secretaries, laboratory experts and CT scan experts with a definite risk level equal to 5.10.
The results of fuzzy analysis of COVID-19 risk revealed that the group of nurses is in four risk levels and seven other groups, including groups of doctors and specialists, supervisors, ward services, receptionists and secretaries, patients’ carriers, laboratory experts and CT scan experts, each of them is in two risk levels. In the group of medical doctors and specialists, 8 people faced a risk level of 10.5 and 13 people faced a risk level of 16.25. The level of COVID-19 risk was estimated 10.5 for 7 people from the group of supervisors and 16.25 for 9 people. In the service group, 6 people faced a risk level of 16.25 and 15 people faced a risk level of 38.5. The level of COVID-19 risk in 8 and 11 people in the receptionist group was calculated 10.5 and 16.25, respectively. In the patients’ porters group, 11 people faced a risk level of 26.75 and 14 people faced a risk level of 38.5. Five laboratory experts and 2 CT scan department experts have a definite COVID-19 risk equal to 10.5. In addition, the level of COVID-19 risk was estimated 16.25 for 18 laboratory experts and 5 CT scan department experts. Calculating the COVID-19 risk based on fuzzy logic in the group of nurses with four different risk levels showed that 17 people face a risk level of 16.25 and 21 people face a risk level of 26.75. This analysis showed that the definite risk level of COVID-19 was calculated as 38.5 for 33 people and 56.0 for 44 people (Table 4).
4. Discussion
The results of various studies have shown that the spread of the COVID-19 has caused countless challenges in the human, economic, social, and even political fields. Its prevalence reduced the level and rate of organizational productivity, including the effectiveness of providing products and services, and directly and indirectly caused all kinds of damage to the human resources of organizations [14, 23]. Due to its high contagiousness and the need to provide various types of medical services in treatment centers and hospitals, one of the crucial centers of COVID-19 risk includes these centers [24, 25]. Previous findings have shown that the epidemic of viral diseases, in addition to infecting workers, can also affect the job performance of people in the workplace and cause them unable to perform their job duties. Also, the physical and mental effects of these diseases can have a lasting impact on people’s general health and lead to the accidents and injuries in the workplace. Therefore, protecting the physical and mental health of employees is essential to control this pandemic and reduce the risk of contracting it [26, 27]. The results of Mohammadfam et al.’s study in three occupational environments, including bank, postal and medical center employees, showed that the level of COVID-19 risk is high for all the people studied [17].
Although Mohammadfam and Mirzaei Aliabadi in their studies have designed, presented, and implemented RCHA to screen people suspected of COVID-19 disease in work environments [16, 17], the review of these studies and attention to the types of the consequences and direct and collateral damage caused by COVID-19 show that the error of diagnosis and human estimation can exist in this risk assessment, despite the qualitative assessment and semi-quantitative estimation of COVID-19 risk based on this method can lead to a good estimate of COVID-19 risk. Therefore, this study was designed and implemented with the approach of applying fuzzy logic and based on RCHA in medical environments.
The results of this study indicated that more than half of the people studied are at high risk of COVID-19. Findings stated that the combination of fuzzy logic and RCHA can help or lead to a more accurate estimate of exposure to COVID-19 risk. The results of the fuzzy analysis of COVID-19 risk showed that the lowest and highest definite risk estimates were equal to 10.5 and 56.0. These results revealed that the group of nurses has the highest risk of COVID-19 compared to the other seven groups working in the studied medical centers, including the group of doctors and specialists, supervisors, ward services, receptionists and secretaries, patients’ carriers, laboratory experts, and CT scan experts. These results showed that the definite COVID-19 risk in nurses is 16.25, 26.75, 38.5, and 56.0 in four levels. In addition, they indicated that after group of nurses, group of patient carriers with a definite risk level of 26.75 and 38.5 as well as the group of ward services with a definite risk level of 16.25 and 38.5 respectively, have the highest COVID-19 risk. Therefore, it shows that the risk of COVID-19 in these three occupational groups in medical centers is very high, and due to the high prevalence of it, protective and health measures should be taken according to the risk level for these three groups. In addition, these three groups should be prioritized in the design and implementation of various strategies to reduce COVID-19 risk. In addition, the results of Schröder’s study (2020) show that despite the low lethality of the COVID-19 compared to other viral and infectious diseases, such as Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS), the risk of this disease is high due to its high contagion power in environments with high communication possibilities. Therefore, implementing a risk assessment program in which parameters, such as time of exposure to the source (for example, infected people), and distance to the source can lead to measures that causes a reduction in the incidence of this disease [28]. Also, the results of Chatterjee’s study (2020) show that the development of a risk assessment tool is very useful for creating awareness and decision-making, and the results of this assessment can be very effective for the response and the management of COVID-19 [29].
Based on the findings as well as the purpose of designing and implementing in this study, which included the analysis of COVID-19 risk based on fuzzy logic, the use of fuzzy logic according to the instructions provided can act as a suitable complement to the technique of quick analysis of the risk of COVID-19, therefore this approach can be used as a simple, fast, low-cost and high-accuracy method to assess COVID-19 risk for various purposes, including the screening of workplaces for COVID-19 to determine priorities to design and implement corrective measures as well as a criterion for macro-management decisions.
5. Conclusion
The results of the study indicated that the use of fuzzy logic to assess the COVID-19 risk based on the developed method (RCHA) can lead to an acceptable and appropriate estimate of it, especially in high-risk jobs, such as working in medical centers. Also, the results of the fuzzy analysis of COVID-19 risk demonstrated that it was higher for the three groups of nurses, patient carriers, and ward services. Therefore, in designing and implementing the necessary strategies to reduce COVID-19 risk, these groups should be prioritized for the COVID-19.
Ethical Considerations
Compliance with ethical guidelines
The present study was registered as a research project in the Ethics Committee of Qom University of Medical Sciences (Code: IR.MUQ.REC.1399.228).
Funding
This article is a part of research project (No.: 1564) approved by the Vice-chancellor for Research and Technology of Qom University of Medical Sciences.
Authors' contributions
Study concept and design: Iraj Mohammadfam and Ahmad Soltanzadeh; Data analysis and interpretation of data: Mohsen Mahdinia; Writing--original draft: Ahmad Soltanzadeh and Mohsen Mahdinia; Review of the article and final approval: Iraj Mohammadfam; Data collection, reading, and approval of the final manuscript: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
- Anderson M, Mckee M, Mossialos E. Developing a sustainable exit strategy for covid-19: Health, economic and public policy implications. Journal of the Royal Society of Medicine. 2020; 113(5):176-8. [DOI:10.1177/0141076820925229] [PMID]
- McKibbin W, Fernando R. The economic impact of covid-19. In: Baldwin R, Weder di Mauro B, editors. Economics in the time of covid-19. Washington: CEPR Press; 2020. [Link]
- Kalantary S, Khadem M. Occupation groups and covid-19. Journal of Health and Safety at Work. 2020; 10(2):1-3. [Link]
- Pak A, Adegboye OA, Adekunle AI, Rahman KM, McBryde ES, Eisen DP. Economic consequences of the covid-19 outbreak: The need for epidemic preparedness. Frontiers in Public Health. 2020; 8:241. [DOI:10.3389/fpubh.2020.00241] [PMID] [PMCID]
- Obrenovic B, Du J, Godinic D, Tsoy D, Khan MAS, Jakhongirov I. Sustaining enterprise operations and productivity during the covid-19 pandemic: Enterprise effectiveness and sustainability model. Sustainability. 2020; 12(15):5981. [DOI:10.3390/su12155981]
- Fana M, Pérez ST, Fernández-Macías E. Employment impact of covid-19 crisis: From short term effects to long terms prospects. Journal of Industrial and Business Economics. 2020; 47(3):391-410. [DOI:10.1007/s40812-020-00168-5] [PMCID]
- Zaroushani V. [Occupational safety and health and response to covid-19 using the fourth industrial revolution technologies (Persian)]. Journal of Health and Safety at Work. 2020; 10(4):329-48. [Link]
- Boldog P, Tekeli T, Vizi Z, Dénes A, Bartha FA, Röst G. Risk assessment of novel coronavirus covid-19 outbreaks outside China. Journal of Clinical Medicine. 2020; 9(2):571. [DOI:10.3390/jcm9020571] [PMID] [PMCID]
- Kim I, Lee J, Lee J, Shin E, Chu C, Lee SK. KCDC risk assessments on the initial phase of the covid-19 outbreak in Korea. Osong Public Health and Research Perspectives. 2020; 11(2):67. [DOI:10.24171/j.phrp.2020.11.2.02] [PMID] [PMCID]
- Ozdemir Y, Gul M, Celik E. Assessment of occupational hazards and associated risks in fuzzy environment: A case study of a university chemical laboratory. Human and Ecological Risk Assessment. 2017; 23(4):895-924. [DOI:10.1080/10807039.2017.1292844]
- Eisler R. Handbook of chemical risk assessment: Health hazards to humans, plants, and animals. Washington: CRC Press; 2000. [DOI:10.1201/9781420032741]
- Burdorf A, Porru F, Rugulies R. The covid-19 (coronavirus) pandemic: Consequences for occupational health. Scandinavian Journal of Work, Environment & Health. 2020; 46(3):229-30. [DOI:10.5271/sjweh.3893] [PMID]
- Sadeghi Yarandi M, Gholami A, Ghasemi M, Sadeghi Yarandi M, Ghasemi Koozekonan A, Soltanzadeh A. [Investigating the psychological consequences of the covid-19 outbreak in the occupational society (Persian)]. Journal of Military Medicine. 2020; 22(6):562-9. [DOI:10.30491/JMM.22.6.562]
- Koh D. Occupational risks for covid-19 infection. Occupational Medicine. 2020; 70(1):3-5. [DOI:10.1093/occmed/kqaa036] [PMID] [PMCID]
- Gholami A, Sadeghi Yarandi M, Ghasemi M, Sadeghi Yarandi M, Ghasemi Koozekonan A, Soltanzadeh A. [Effect of coronavirus epidemic on job stress and mental workload: A longitudinal study in a chemical industry (Persian)]. Iran Occupational Health. 2020; 17(S1):81-9. [Link]
- Mohammadfam I, Mirzaei Aliabadi M. [Developing a method for assessing and managing the risk of covid-19; Rapid covid-19 hazard analysis (Persian)]. Iran Occupational Health. 2020; 17(1):1-12. [Link]
- Mohammadfam I, Mahdinia M, Salimi V, Koupal R, Soltanzadeh A. [Assessing the risk of covid-19 in workplace environments using rapid risk analysis (Persian)]. Journal of Military Medicine. 2020; 22(6):607-15. [DOI:10.30491/JMM.22.6.607]
- Zhou Q, Huang W, Zhang Y. Identifying critical success factors in emergency management using a fuzzy DEMATEL method. Safety Science. 2011; 49(2):243-52. [DOI:10.1016/j.ssci.2010.08.005]
- Esfahani AN, Sarand VF, Arian A. Explain the impact of organizational factors affecting food safety performance using fuzzy DEMATEL. International Journal of Management Sciences. 2015; 5(7):531-43. [Link]
- Kabak Ö, Ülengin F, Çekyay B, Önsel Ş, Özaydın Ö. Critical success factors for the iron and steel industry in Turkey: A fuzzy DEMATEL approach. International Journal of Fuzzy Systems. 2016; 18(3):523-36. [DOI:10.1007/s40815-015-0067-7]
- Ahmadi M, Zakerian SA, Salmanzadeh H, Mortezapour A. Identification of the ergonomic interventions goals from the viewpoint of ergonomics experts of Iran using fuzzy Delphi method. International Journal of Occupational Hygiene. 2016; 8(3):151-7. [Link]
- Novák V, Perfilieva I, Mockor J. Mathematical principles of fuzzy logic. New York: Springer. 1999. [DOI:10.1007/978-1-4615-5217-8]
- Semple S, Cherrie JW. Covid-19: Protecting worker health. Annals of Work Exposures and Health. 2020; 64(5):461-4. [DOI:10.1093/annweh/wxaa033] [PMID] [PMCID]
- Saban O, Levy J, Chowers I. Risk of SARS-CoV-2 transmission to medical staff and patients from an exposure to a covid-19-positive ophthalmologist. Graefe’s Archive for Clinical and Experimental Ophthalmology. 2020; 258(10):2271-4. [DOI:10.1007/s00417-020-04790-w] [PMID] [PMCID]
- The Lancet. Covid-19: Protecting health-care workers. The Lancet. 2020; 395(10228):922. [DOI:10.1016/S0140-6736(20)30644-9] [PMID] [PMCID]
- Kang L, Li Y, Hu S, Chen M, Yang C, Yang BX, et al. The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavirus. The Lancet Psychiatry. 2020; 7(3):e14. [DOI:10.1016/S2215-0366(20)30047-X] [PMID] [PMCID]
- Kim KW, Park SJ, Lim HS, Cho HH. Safety climate and occupational stress according to occupational accidents experience and employment type in shipbuilding industry of Korea. Safety and Health at Work. 2017; 8(3):290-5. [DOI:10.1016/j.shaw.2017.08.002]
- Schröder I. Covid-19: A risk assessment perspective. Journal of Chemical Health and Safety. 2020; 11:acs.chas.0c00035. [DOI:10.1021/acs.chas.0c00035] [PMCID]
- Chatterjee R, Bajwa S, Dwivedi D, Kanji R, Ahammed M, Shaw R. Covid-19 risk assessment tool: Dual application of risk communication and risk governance. Progress in Disaster Science. 2020; 7:100109. [DOI:10.1016/j.pdisas.2020.100109] [PMID] [PMCID]
Type of article: Research |
Subject:
Special
Received: 2022/05/2 | Accepted: 2022/06/12 | Published: 2022/10/1
Received: 2022/05/2 | Accepted: 2022/06/12 | Published: 2022/10/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
