

Volume 8, Issue 4 (Summer 2023)
Health in Emergencies and Disasters Quarterly 2023, 8(4): 313-322 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Abbasabadi-Arab M, Miadfar J, Yousefian S, Mobini A, Mehran Amin S. Assessing Hospital Safety Index in the Iranian Hospitals. Health in Emergencies and Disasters Quarterly 2023; 8 (4) :313-322
URL: http://hdq.uswr.ac.ir/article-1-457-en.html
URL: http://hdq.uswr.ac.ir/article-1-457-en.html



1- National Medical Emergency Organization, Ministry of Health & Medical Education, Tehran, Iran.
2- National Medical Emergency Organization, Ministry of Health & Medical Education, Tehran, Iran. ,shivayousefian2003@yahoo.com
2- National Medical Emergency Organization, Ministry of Health & Medical Education, Tehran, Iran. ,
Full-Text [PDF 881 kb]
(2219 Downloads)
| Abstract (HTML) (4073 Views)
Full-Text: (1543 Views)
1. Introduction
Hospitals are an integral part of the health system and a symbol of the social progress of a society. During disasters, the resilience of hospitals and continuing to provide medical services to the injured causes security in society [1]. With increasing the incidence of accidents and disasters, the health system in different countries is facing many challenges to respond to these incidents. The Centre for Research on the Epidemiology of Disasters (CRED) has reported about 347 cases of natural disasters that occurred in the world, including earthquakes, volcanoes, floods, landslides, droughts, fires, etc. between 2001 and 2020. While in 2021, about 432 cases of natural disasters have been reported, affecting about 101.8 million people with economic damage of 252 billion dollars [2]. In most natural disasters, hospitals are directly affected by the accident and are damaged in terms of building, equipment, staff, and management system, and they will not be able to provide services for the injuries caused by accidents and disasters. In 2003, an earthquake with a magnitude of 6.6 occurred in Bam City, Iran. Hospitals in the region could not provide services due to structural and non-structural damage and lost their performance [3]. In 2009, the flood in Jeddah, Saudi Arabia, put the region’s hospitals in a critical situation, and computer and software systems failed. Due to flooding, the equipment in the basement of the hospitals failed and many hospital services were disrupted [4]. A 7.6 magnitude earthquake in Pakistan in 2005 led to the destruction and inactivation of 68% of healthcare centers [5]. In the Sichuan earthquake of China in 2008, 67.5% of the buildings of health care centers in the earthquake area were destructed [6].
The World Health Organization (WHO) has always requested that governments should seriously intervene to improve the level of preparedness of hospitals and health-treatment centers. Following the global campaign of the United Nations titled making hospitals safe against disasters in 2008 and 2009, the hospital safety index (HSI) tool was developed by the Pan American Health Organization (PAHO) and the Disaster Mitigation Advisory Group (DiMAG) [7]. This tool was designed to help hospitals to assess safety, prioritize planning, and prevent hospital damage due to accidents and disasters, and, the HSI represents the possibility that the hospital can be active and perform its duties in the event of disasters. This is a set of tools that includes hospital areas, including structural, non-structural, and operational elements of the hospital, and finally determines the HSI [8]. The Ministry of Health and Medical Education translated and localized this tool, and in 2012, the safety status of 224 hospitals was evaluated using this tool, and the report was published. In 2014, 421 hospitals participated. Among these, 82 hospitals (19.4%) have low safety levels and 339 hospitals (80.6%) have mean safety levels in accidents. None of the evaluated hospitals have high safety [9]. The results of investigating HSI in Shush City, Khuzestan Province, Iran in 2015 showed that the HSI was 56.73 [10]. A study conducted in Shiraz hospitals determined the HSI at 6 out of 10 [11]. The results of the evaluation of hospital safety based on HSI in Indonesia also showed that the safety of hospitals is at an mean level [12].
Many changes have been made in recent years, including the health transformation plan, upgrading hospital hoteling, and developing accreditation standards for risk management of accidents and disasters, developing and communicating risk management programs, which have increased the level of preparedness of hospitals. This study was conducted to investigate the status of the HSI in Iranian hospitals in 2020 and to provide solutions for its improvement.
2. Materials and Methods
A cross-sectional descriptive study was conducted for all Iranian hospitals in 2020. The tool under study was the Farsi version hospital safety index (FHSI) checklist, which includes 151 options and evaluates hospital safety in three areas of structural, non-structural, and functional safety. The field of functional safety by the book of hospital safety evaluation includes the creation of a structure and plan for dealing with accidents and emergencies, which includes the formation of a committee, preparation of a plan, and operational guidelines for preparation, response, and rehabilitation. The field of structural safety includes components that bear the weight of the building, such as columns, beams, concrete slabs, and roofs. The non-structural safety area includes components of the building that do not play a role in bearing the weight of the building, such as vital systems (electricity, communication, water reserves, fuel, medical gases), heating, cooling, and air conditioning, office equipment, medical and laboratory equipment, and architectural components. After the scores of different areas of the hospital are determined and recorded by the specialists of each area, the score of the HSI and leveling are obtained. In the first level (A), the hospital can protect the lives of the people inside it and can continue its operation in the conditions of accidents and disasters. In the second level (B), the hospital can withstand accidents and disasters, but the equipment and its vital services are at risk, and the third level (C) at the time of the accident, the hospital and all the people in it are at risk [8].
Using this checklist, hospital teams performed a self-assessment of hospital safety and recorded it in FHSI the system of the Ministry of Health and Medical Education. The assessment was carried out by a multidisciplinary team of Ayaz Hospital, including structural engineers and trained architects, experts in the hospital’s critical systems, medical and facilities engineers, mechanical and electrical systems engineers, health and hygiene experts, including doctors, nurses, and disaster and emergency management experts. Table 1 presents the axes related to the evaluation of each area.
.JPG)
The scores for each option are recorded as zero (low safety), one (medium safety), and two (high safety) according to the checklist guide, and the sum of the scores determines the level of safety in each area. The registered results were collected from the system based on hospitals and universities of medical sciences in the country. Descriptive statistics (Mean±SD, and percentage) were used to analyze data.
3. Results
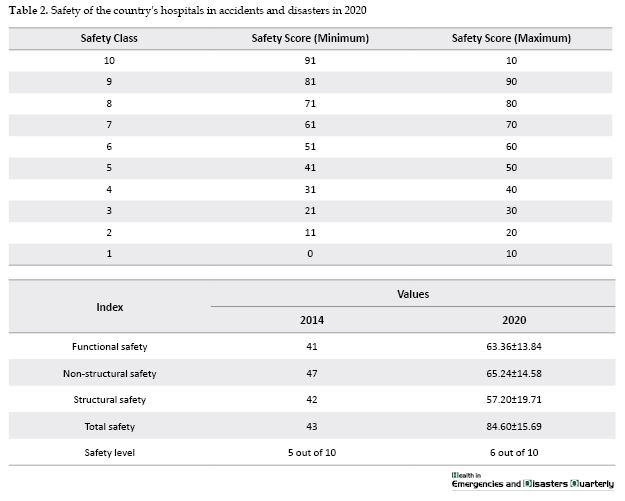
In 2020, 1026 hospitals existed in the country [13], of which the safety evaluation information of 604 hospitals from 52 universities of medical sciences in the country was registered in the FHSI system. The participation rate of hospitals in completing the FHSI system was 58.9% and the participation rate of universities was 77%. The evaluation results showed that the mean safety score of the country’s hospitals in 2020 was 60.84. The mean of structural, non-structural, and management safety in the country’s hospitals is 57.20, 65.24, and 63.36, respectively, and is at an mean level. Table 1 presents the results of evaluating hospital safety by the safety axis and its components. A total of 130 hospitals (21.5%) had a low safety level, 418 hospitals (69%) had a medium safety level, and 56 hospitals (9.2%) had a high safety level against accidents and disasters. Table 2 compares the safety level of hospitals in 2014 and 2020. The results show that the safety level of hospitals has reached the level of 6 out of 10 with a step up compared to 2014.
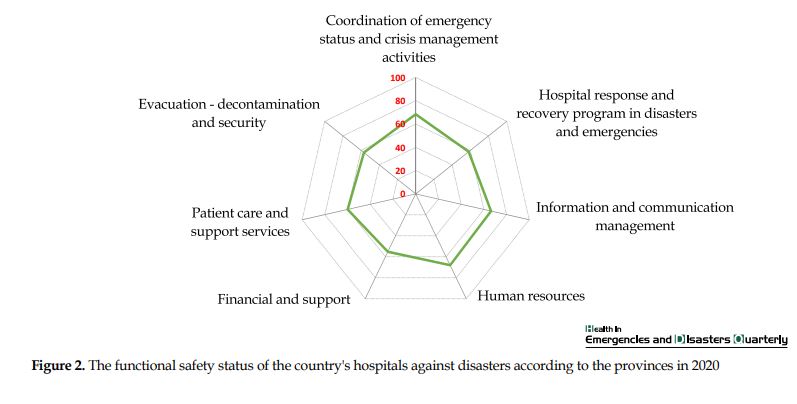
Figures 1 and 2 show the state of non-structural and functional safety in the country’s hospitals. The lowest score in non-structural safety was related to the axis of office supplies and warehouses (14.55) and the lowest score in functional safety was related to the support and financial axis (14.55).
Figure 3 shows the mean scores obtained according to the provinces of the country. Hamedan (76.81) and Kerman (75.61) Provinces in Iran, gained the highest score, and Yazd (53.74) and Lorestan (57.31) Provinces in Iran, gained the lowest score in the country.
.JPG)
.JPG)
4. Discussion
This research was conducted to investigate the Iranian hospital’s safety against accidents and disasters. The mean safety score of the country’s hospitals was 60.84% at the mean level (B), which is consistent with the results of this research [14]. The level of hospital safety was determined at level 6 out of 10, which is consistent with the study conducted in Shiraz hospitals [11]. The results of the hospital safety evaluation based on HSI in Indonesia also showed that the safety of hospitals is at B level [12]. In a study, the level of preparedness of Yemeni hospitals against accidents and disasters was 46.6% [15] and in another study, the level of preparedness of Jordanian hospitals was also weak [16]. In Saudi Arabia, despite the development of hospital standards, the level of preparedness of hospitals has not been reported as favorable [4]. The study of the preparedness level of Swedish and Iranian hospitals showed that Swedish hospitals were more prepared [4].
The results of these studies show that the HSI in developing hospitals is not optimal. While more than 40% of the world’s accidents happen in the Asian continent [2], serious damage to the infrastructure and the spending of the country’s income to compensate for these damages lead to further lagging behind sustainable development.
The results of this evaluation compared to 2014 showed an improvement in the hospital safety status covered by the country’s universities of medical sciences from a safety score of 43 to about 61(41.5%). This improvement is due to the development of accident and disaster risk management standards in the hospital accreditation program [17, 18, 19] and the annual evaluation of hospitals, increasing the awareness level of hospital employees through training courses and exercises, as well as the development of programs, including health transformation plan and the instructions of the Ministry of Health and Medical Education that occurred during this period. Based on the results of the evaluation and the visits, the status of the hospitals has a higher level of safety in Hamedan, Kerman, Qazvin, Fars, and Zanjan Provinces in Iran. In Yazd, Lorestan, Mazandaran, Ardabil, and North Khorasan Provinces in Iran, the topics related to improving the safety level of medical centers should be a higher priority.
Evaluation of structural safety
Structural safety gained the lowest score (20.57) among the safety axes. A systematic review study has also shown that hospitals are at a weak level in structural safety (49%) and an mean level in non-structural safety (57%) [14]. In a review study in China, the crucial challenge in the preparation of hospitals is infrastructure safety [20]. About half of the country’s hospitals (55%) are more than 20 years old, and about 15% of hospitals are more than 50 years old. The old age of hospitals leads to increased costs, reduced efficiency, and increased dissatisfaction among employees and patients [21]. Despite the upward trend of the structural safety status of hospitals (increasing the safety score from 42 in 2014 to 20.57 in 2020), there is still a long way to achieve the desired status and it requires more investment than other safety components.
Although in 2016, following the reforms in the safety evaluation tool, changes were made in some questions and assessment criteria, the structural safety status has been on the rise in recent years. Considering the importance of improving the safety of medical centers, this issue is raised in paragraph (c) of article [14] of the country’s crisis management law (Resolution No. 44473/90 dated 2019 of the Islamic Council) and as one of the tasks of the Ministry of Health and Medical Education, are monitored [22]. Therefore, planning to improve the safety status of medical centers should be considered as one of the priority programs at the national level as well as in universities of medical sciences and hospitals for policy-makers, managers, and decision-makers in the health field.
Evaluation of non-structural safety
Non-structural safety gained the highest score (24.65) among the safety axes. Despite the upward trend of the non-structural safety status of hospitals (increasing the safety score from 47 in 2014 to 24.65 in 2020), there is still a long way to achieve the desired status. The axis of office supplies, storage (50.73), fire protection (50.91), and long-distance communication facilities (51.33) gained the lowest score on this axis. In a study in 2019, the status of Bushehr hospitals was matched with the international standards of NFPA101, the status of the hospitals was at an mean level, and defects, such as the lack of a smoke control system, the absence of automatic geysers in the buildings, and the inappropriate type of fire detectors in the kitchen existed [23]. In the study of Shiraz hospitals, moderate fire safety was also reported [24], which is consistent with the results of this study. In a study conducted in 2020, the status of passive defense in food and drug warehouses of hospitals was evaluated in two universities of medical sciences, which showed that the general status of compliance with the principles of passive defense in warehouses is mean, but in terms of the security status of the internal area and outside, the principle of camouflage and dispersion due to the lack of initial construction of the structure for the warehouse is weak, and improving the safety of warehouses is a priority in the planning of hospitals [25]. Long-distance facilities and communication equipment are other weak points of hospitals. Defects in the communication system caused by the crisis, lack of facilities concerning communication equipment and technologies, and insufficient storage of communication systems, which causes inconsistency of performance between organs, increase the complications and effects caused by the crisis [26].
The safety of electrical systems showed a score of 62.60 on this axis. A study was conducted to evaluate the electrical and diesel generator safety status in Tabriz hospitals. The designed checklists had the minimum standards in this field and the scores were 61.4% and 52.8%, indicating the low level of safety and maintenance for the emergency power system for hospitals, and in case of accidents and disasters, hospitals will face many problems. [27]. The safety of the electrical systems of the hospital and the continuity of the supply of electrical energy is vital to the safety of patients and require the serious attention of managers and officials of hospitals and the Ministry of Health and Medical Education.
Evaluation of functional safety
Functional safety also scored (63.36) and has improved compared to the functional safety score of hospitals in 2014 (41). This section examines the level of preparedness of the hospital and its staff and the necessity of the hospital’s performance to provide services to patients when responding to accidents and disasters. Coordination, hospital response, and recovery plan, communication and information management, human resources, financial resources and support, care and support services, evacuation, decontamination, and security are among the key and specialized measures of functional safety.
The activity of the hospitals’ crisis committee, holding workshops and specialized training in the field of disaster risk management, and requiring hospitals to comply with disaster risk management accreditation standards in the form of an annual accreditation program led to reforms and changes in this area, such as other components of hospital safety assessment. About 16% of hospitals are at the low level, about 78% at the medium level, and 5.5% at the high level in terms of management measures, which suggests the need to develop a crisis management operational plan based on priority risks and risk assessment. Disaster preparedness and response planning is a scientific process and requires the training and empowerment of managers and employees. Planning in accidents and disasters starts with risk assessment and continues throughout the cycle of accidents and disasters [28].
Managers and employees of hospitals should receive the necessary training in the field of providing services in emergencies to a large number of injured, triaging, and how manage the injured. Doing exercises is used to measure the level of preparation, coordination, and repetition of what has been learned to acquire skills and examine the correctness of policies and plans for the risk management of accidents and disasters. Planning, holding effective training courses and simulated exercises for managers and employees are vital in increasing the preparedness level and proper response of hospitals in accidents and disasters. Simulated exercises are more effective to strengthen and improve the preparedness of the organization and employees in response to accidents and disasters because they put the person in a similar situation [29]. Evacuation, decontamination, and security also gained a low score, the study conducted by Beyramijam et al. showed that hospitals had a low score in terms of safety and security (53.91) [30]. Although the timely, effective, and safe evacuation of patients with a critical status during disasters is crucial, many service providers have received little or no training on evacuation preparedness and implementation [31]. Developing national guidelines and training them for employees is mandatory in this field. Financial support gained the lowest score on this axis, which is consistent with the results of other domestic and foreign studies [20, 32]. Therefore, policy-makers and senior managers of the health system, through the crisis management organization law, seriously follow up the provision of financial resources to develop infrastructure, equipment, resources, and security of hospitals.
5. Conclusion
This study shows the results of the HSI of the whole country in the issue of risk management of accidents and disasters. The results of this study showed that despite the increase of 41.5% in safety compared to 2014, the safety status of hospitals is still mean and they are not properly prepared to deal with accidents and disasters. Considering that hospitals are located in a complex political, economic, social, and environmental system, they are influenced by many factors. A hospital prepared against accidents and disasters requires the support of upstream laws and policies, provision of funds for hospital security, detailed planning and provision of resources and facilities, training and training, sufficient financial resources, and a strong management and leadership system to provide high-quality and equitable services during accidents and disasters. Therefore, improving the safety level of hospitals requires changes and reforms at different levels. Planning and paying attention to the safety and retrofitting of hospitals, improving the safety of medical equipment, improving the knowledge and skills of managers in the scientific development of preparedness, response, and recovery programs, providing financial resources and supporting crisis programs, paying attention to security programs, decontamination, and evacuation is one of the ways to improve hospital preparedness.
Research limitations
This research was conducted based on the information sent from the accident and emergency management centers of the universities of medical sciences in the country, and due to the confidentiality of the information, the names and specifications of the hospitals were not included in the submitted list, and only the scores obtained in the axes of hospital safety by the universities of medical sciences were included. Therefore, it was impossible to relate the number of scores with the characteristics of the hospitals and a more detailed analysis.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Jafar Miadfar; Methodology: Shiva Yousefian; Investigation, writing–original draft, review and editing: Masoumeh Abbasabadi-Arab; Data analysis: Sara Mehran Amin and Atieh Mobini.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We hereby thank the colleagues of medical emergency and accident management centers, managers, and employees of the country’s hospitals who cooperated in collecting information. Also, the authors thank the respected referees who helped to improve the quality of this article with their constructive criticism and expert opinions.
References
Hospitals are an integral part of the health system and a symbol of the social progress of a society. During disasters, the resilience of hospitals and continuing to provide medical services to the injured causes security in society [1]. With increasing the incidence of accidents and disasters, the health system in different countries is facing many challenges to respond to these incidents. The Centre for Research on the Epidemiology of Disasters (CRED) has reported about 347 cases of natural disasters that occurred in the world, including earthquakes, volcanoes, floods, landslides, droughts, fires, etc. between 2001 and 2020. While in 2021, about 432 cases of natural disasters have been reported, affecting about 101.8 million people with economic damage of 252 billion dollars [2]. In most natural disasters, hospitals are directly affected by the accident and are damaged in terms of building, equipment, staff, and management system, and they will not be able to provide services for the injuries caused by accidents and disasters. In 2003, an earthquake with a magnitude of 6.6 occurred in Bam City, Iran. Hospitals in the region could not provide services due to structural and non-structural damage and lost their performance [3]. In 2009, the flood in Jeddah, Saudi Arabia, put the region’s hospitals in a critical situation, and computer and software systems failed. Due to flooding, the equipment in the basement of the hospitals failed and many hospital services were disrupted [4]. A 7.6 magnitude earthquake in Pakistan in 2005 led to the destruction and inactivation of 68% of healthcare centers [5]. In the Sichuan earthquake of China in 2008, 67.5% of the buildings of health care centers in the earthquake area were destructed [6].
The World Health Organization (WHO) has always requested that governments should seriously intervene to improve the level of preparedness of hospitals and health-treatment centers. Following the global campaign of the United Nations titled making hospitals safe against disasters in 2008 and 2009, the hospital safety index (HSI) tool was developed by the Pan American Health Organization (PAHO) and the Disaster Mitigation Advisory Group (DiMAG) [7]. This tool was designed to help hospitals to assess safety, prioritize planning, and prevent hospital damage due to accidents and disasters, and, the HSI represents the possibility that the hospital can be active and perform its duties in the event of disasters. This is a set of tools that includes hospital areas, including structural, non-structural, and operational elements of the hospital, and finally determines the HSI [8]. The Ministry of Health and Medical Education translated and localized this tool, and in 2012, the safety status of 224 hospitals was evaluated using this tool, and the report was published. In 2014, 421 hospitals participated. Among these, 82 hospitals (19.4%) have low safety levels and 339 hospitals (80.6%) have mean safety levels in accidents. None of the evaluated hospitals have high safety [9]. The results of investigating HSI in Shush City, Khuzestan Province, Iran in 2015 showed that the HSI was 56.73 [10]. A study conducted in Shiraz hospitals determined the HSI at 6 out of 10 [11]. The results of the evaluation of hospital safety based on HSI in Indonesia also showed that the safety of hospitals is at an mean level [12].
Many changes have been made in recent years, including the health transformation plan, upgrading hospital hoteling, and developing accreditation standards for risk management of accidents and disasters, developing and communicating risk management programs, which have increased the level of preparedness of hospitals. This study was conducted to investigate the status of the HSI in Iranian hospitals in 2020 and to provide solutions for its improvement.
2. Materials and Methods
A cross-sectional descriptive study was conducted for all Iranian hospitals in 2020. The tool under study was the Farsi version hospital safety index (FHSI) checklist, which includes 151 options and evaluates hospital safety in three areas of structural, non-structural, and functional safety. The field of functional safety by the book of hospital safety evaluation includes the creation of a structure and plan for dealing with accidents and emergencies, which includes the formation of a committee, preparation of a plan, and operational guidelines for preparation, response, and rehabilitation. The field of structural safety includes components that bear the weight of the building, such as columns, beams, concrete slabs, and roofs. The non-structural safety area includes components of the building that do not play a role in bearing the weight of the building, such as vital systems (electricity, communication, water reserves, fuel, medical gases), heating, cooling, and air conditioning, office equipment, medical and laboratory equipment, and architectural components. After the scores of different areas of the hospital are determined and recorded by the specialists of each area, the score of the HSI and leveling are obtained. In the first level (A), the hospital can protect the lives of the people inside it and can continue its operation in the conditions of accidents and disasters. In the second level (B), the hospital can withstand accidents and disasters, but the equipment and its vital services are at risk, and the third level (C) at the time of the accident, the hospital and all the people in it are at risk [8].
Using this checklist, hospital teams performed a self-assessment of hospital safety and recorded it in FHSI the system of the Ministry of Health and Medical Education. The assessment was carried out by a multidisciplinary team of Ayaz Hospital, including structural engineers and trained architects, experts in the hospital’s critical systems, medical and facilities engineers, mechanical and electrical systems engineers, health and hygiene experts, including doctors, nurses, and disaster and emergency management experts. Table 1 presents the axes related to the evaluation of each area.
The scores for each option are recorded as zero (low safety), one (medium safety), and two (high safety) according to the checklist guide, and the sum of the scores determines the level of safety in each area. The registered results were collected from the system based on hospitals and universities of medical sciences in the country. Descriptive statistics (Mean±SD, and percentage) were used to analyze data.
3. Results
In 2020, 1026 hospitals existed in the country [13], of which the safety evaluation information of 604 hospitals from 52 universities of medical sciences in the country was registered in the FHSI system. The participation rate of hospitals in completing the FHSI system was 58.9% and the participation rate of universities was 77%. The evaluation results showed that the mean safety score of the country’s hospitals in 2020 was 60.84. The mean of structural, non-structural, and management safety in the country’s hospitals is 57.20, 65.24, and 63.36, respectively, and is at an mean level. Table 1 presents the results of evaluating hospital safety by the safety axis and its components. A total of 130 hospitals (21.5%) had a low safety level, 418 hospitals (69%) had a medium safety level, and 56 hospitals (9.2%) had a high safety level against accidents and disasters. Table 2 compares the safety level of hospitals in 2014 and 2020. The results show that the safety level of hospitals has reached the level of 6 out of 10 with a step up compared to 2014.
Figures 1 and 2 show the state of non-structural and functional safety in the country’s hospitals. The lowest score in non-structural safety was related to the axis of office supplies and warehouses (14.55) and the lowest score in functional safety was related to the support and financial axis (14.55).
Figure 3 shows the mean scores obtained according to the provinces of the country. Hamedan (76.81) and Kerman (75.61) Provinces in Iran, gained the highest score, and Yazd (53.74) and Lorestan (57.31) Provinces in Iran, gained the lowest score in the country.
4. Discussion
This research was conducted to investigate the Iranian hospital’s safety against accidents and disasters. The mean safety score of the country’s hospitals was 60.84% at the mean level (B), which is consistent with the results of this research [14]. The level of hospital safety was determined at level 6 out of 10, which is consistent with the study conducted in Shiraz hospitals [11]. The results of the hospital safety evaluation based on HSI in Indonesia also showed that the safety of hospitals is at B level [12]. In a study, the level of preparedness of Yemeni hospitals against accidents and disasters was 46.6% [15] and in another study, the level of preparedness of Jordanian hospitals was also weak [16]. In Saudi Arabia, despite the development of hospital standards, the level of preparedness of hospitals has not been reported as favorable [4]. The study of the preparedness level of Swedish and Iranian hospitals showed that Swedish hospitals were more prepared [4].
The results of these studies show that the HSI in developing hospitals is not optimal. While more than 40% of the world’s accidents happen in the Asian continent [2], serious damage to the infrastructure and the spending of the country’s income to compensate for these damages lead to further lagging behind sustainable development.
The results of this evaluation compared to 2014 showed an improvement in the hospital safety status covered by the country’s universities of medical sciences from a safety score of 43 to about 61(41.5%). This improvement is due to the development of accident and disaster risk management standards in the hospital accreditation program [17, 18, 19] and the annual evaluation of hospitals, increasing the awareness level of hospital employees through training courses and exercises, as well as the development of programs, including health transformation plan and the instructions of the Ministry of Health and Medical Education that occurred during this period. Based on the results of the evaluation and the visits, the status of the hospitals has a higher level of safety in Hamedan, Kerman, Qazvin, Fars, and Zanjan Provinces in Iran. In Yazd, Lorestan, Mazandaran, Ardabil, and North Khorasan Provinces in Iran, the topics related to improving the safety level of medical centers should be a higher priority.
Evaluation of structural safety
Structural safety gained the lowest score (20.57) among the safety axes. A systematic review study has also shown that hospitals are at a weak level in structural safety (49%) and an mean level in non-structural safety (57%) [14]. In a review study in China, the crucial challenge in the preparation of hospitals is infrastructure safety [20]. About half of the country’s hospitals (55%) are more than 20 years old, and about 15% of hospitals are more than 50 years old. The old age of hospitals leads to increased costs, reduced efficiency, and increased dissatisfaction among employees and patients [21]. Despite the upward trend of the structural safety status of hospitals (increasing the safety score from 42 in 2014 to 20.57 in 2020), there is still a long way to achieve the desired status and it requires more investment than other safety components.
Although in 2016, following the reforms in the safety evaluation tool, changes were made in some questions and assessment criteria, the structural safety status has been on the rise in recent years. Considering the importance of improving the safety of medical centers, this issue is raised in paragraph (c) of article [14] of the country’s crisis management law (Resolution No. 44473/90 dated 2019 of the Islamic Council) and as one of the tasks of the Ministry of Health and Medical Education, are monitored [22]. Therefore, planning to improve the safety status of medical centers should be considered as one of the priority programs at the national level as well as in universities of medical sciences and hospitals for policy-makers, managers, and decision-makers in the health field.
Evaluation of non-structural safety
Non-structural safety gained the highest score (24.65) among the safety axes. Despite the upward trend of the non-structural safety status of hospitals (increasing the safety score from 47 in 2014 to 24.65 in 2020), there is still a long way to achieve the desired status. The axis of office supplies, storage (50.73), fire protection (50.91), and long-distance communication facilities (51.33) gained the lowest score on this axis. In a study in 2019, the status of Bushehr hospitals was matched with the international standards of NFPA101, the status of the hospitals was at an mean level, and defects, such as the lack of a smoke control system, the absence of automatic geysers in the buildings, and the inappropriate type of fire detectors in the kitchen existed [23]. In the study of Shiraz hospitals, moderate fire safety was also reported [24], which is consistent with the results of this study. In a study conducted in 2020, the status of passive defense in food and drug warehouses of hospitals was evaluated in two universities of medical sciences, which showed that the general status of compliance with the principles of passive defense in warehouses is mean, but in terms of the security status of the internal area and outside, the principle of camouflage and dispersion due to the lack of initial construction of the structure for the warehouse is weak, and improving the safety of warehouses is a priority in the planning of hospitals [25]. Long-distance facilities and communication equipment are other weak points of hospitals. Defects in the communication system caused by the crisis, lack of facilities concerning communication equipment and technologies, and insufficient storage of communication systems, which causes inconsistency of performance between organs, increase the complications and effects caused by the crisis [26].
The safety of electrical systems showed a score of 62.60 on this axis. A study was conducted to evaluate the electrical and diesel generator safety status in Tabriz hospitals. The designed checklists had the minimum standards in this field and the scores were 61.4% and 52.8%, indicating the low level of safety and maintenance for the emergency power system for hospitals, and in case of accidents and disasters, hospitals will face many problems. [27]. The safety of the electrical systems of the hospital and the continuity of the supply of electrical energy is vital to the safety of patients and require the serious attention of managers and officials of hospitals and the Ministry of Health and Medical Education.
Evaluation of functional safety
Functional safety also scored (63.36) and has improved compared to the functional safety score of hospitals in 2014 (41). This section examines the level of preparedness of the hospital and its staff and the necessity of the hospital’s performance to provide services to patients when responding to accidents and disasters. Coordination, hospital response, and recovery plan, communication and information management, human resources, financial resources and support, care and support services, evacuation, decontamination, and security are among the key and specialized measures of functional safety.
The activity of the hospitals’ crisis committee, holding workshops and specialized training in the field of disaster risk management, and requiring hospitals to comply with disaster risk management accreditation standards in the form of an annual accreditation program led to reforms and changes in this area, such as other components of hospital safety assessment. About 16% of hospitals are at the low level, about 78% at the medium level, and 5.5% at the high level in terms of management measures, which suggests the need to develop a crisis management operational plan based on priority risks and risk assessment. Disaster preparedness and response planning is a scientific process and requires the training and empowerment of managers and employees. Planning in accidents and disasters starts with risk assessment and continues throughout the cycle of accidents and disasters [28].
Managers and employees of hospitals should receive the necessary training in the field of providing services in emergencies to a large number of injured, triaging, and how manage the injured. Doing exercises is used to measure the level of preparation, coordination, and repetition of what has been learned to acquire skills and examine the correctness of policies and plans for the risk management of accidents and disasters. Planning, holding effective training courses and simulated exercises for managers and employees are vital in increasing the preparedness level and proper response of hospitals in accidents and disasters. Simulated exercises are more effective to strengthen and improve the preparedness of the organization and employees in response to accidents and disasters because they put the person in a similar situation [29]. Evacuation, decontamination, and security also gained a low score, the study conducted by Beyramijam et al. showed that hospitals had a low score in terms of safety and security (53.91) [30]. Although the timely, effective, and safe evacuation of patients with a critical status during disasters is crucial, many service providers have received little or no training on evacuation preparedness and implementation [31]. Developing national guidelines and training them for employees is mandatory in this field. Financial support gained the lowest score on this axis, which is consistent with the results of other domestic and foreign studies [20, 32]. Therefore, policy-makers and senior managers of the health system, through the crisis management organization law, seriously follow up the provision of financial resources to develop infrastructure, equipment, resources, and security of hospitals.
5. Conclusion
This study shows the results of the HSI of the whole country in the issue of risk management of accidents and disasters. The results of this study showed that despite the increase of 41.5% in safety compared to 2014, the safety status of hospitals is still mean and they are not properly prepared to deal with accidents and disasters. Considering that hospitals are located in a complex political, economic, social, and environmental system, they are influenced by many factors. A hospital prepared against accidents and disasters requires the support of upstream laws and policies, provision of funds for hospital security, detailed planning and provision of resources and facilities, training and training, sufficient financial resources, and a strong management and leadership system to provide high-quality and equitable services during accidents and disasters. Therefore, improving the safety level of hospitals requires changes and reforms at different levels. Planning and paying attention to the safety and retrofitting of hospitals, improving the safety of medical equipment, improving the knowledge and skills of managers in the scientific development of preparedness, response, and recovery programs, providing financial resources and supporting crisis programs, paying attention to security programs, decontamination, and evacuation is one of the ways to improve hospital preparedness.
Research limitations
This research was conducted based on the information sent from the accident and emergency management centers of the universities of medical sciences in the country, and due to the confidentiality of the information, the names and specifications of the hospitals were not included in the submitted list, and only the scores obtained in the axes of hospital safety by the universities of medical sciences were included. Therefore, it was impossible to relate the number of scores with the characteristics of the hospitals and a more detailed analysis.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Jafar Miadfar; Methodology: Shiva Yousefian; Investigation, writing–original draft, review and editing: Masoumeh Abbasabadi-Arab; Data analysis: Sara Mehran Amin and Atieh Mobini.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We hereby thank the colleagues of medical emergency and accident management centers, managers, and employees of the country’s hospitals who cooperated in collecting information. Also, the authors thank the respected referees who helped to improve the quality of this article with their constructive criticism and expert opinions.
References
- Ciottone GR, Keim ME , Molloy MS, Biddinger PD, Darling RG, Fares S, et al. Ciottone’s disaster medicine. Amsterdam: Elsevier; 2015. [Link]
- Centre for Research on the Epidemiology of Disasters. The EM-DAT higher resolution disaster data. Brussels: Centre for Research on the Epidemiology of Disasters; 2021. [Link]
- Khankeh H, Masoumi G. [National hospital disaster risk management program based on accreditation indicators (Persion)]. Tehran: University of Social Welfare and Rehabilitation Sciences; 2018. [Link]
- Bajow N, Alkhalil S. Evaluation and analysis of hospital disaster preparedness in Jeddah. Health. 2014; 6(19):2668-87.[DOI:10.4236/health.2014.619306]
- Emergency Nutrition Network. Real-time evaluation of Pakistan flood response. Kidlington: Emergency Nutrition Network; 2008. [Link]
- Chan EY. The untold stories of the Sichuan earthquake. Lancet. 2008; 372(9636):359-62. [DOI:10.1016/S0140-6736(08)61141-1] [PMID]
- World Health Organization, Pan American Health Organization. Hospital safety index: Guide for evaluators. Geneva: World Health Organization; 2015. [Link]
- Ardalan A, Najafi A, Sabzghabaie A, Zonoobi V, Ardalan S, Khankeh H, et al. [A pilot study: Development of a local model to hospital disaster risk assessment (Persion)]. Journal of Hospital. 2011; 9(3 and 4):7-14. [Link]
- Ardalan A, Kandi Keleh M, Saberinia A, Khorasani-Zavareh D, Khankeh H, Miadfar J, et al. 2015 estimation of hospitals safety from disasters in Iran: The results from the assessment of 421 hospitals. PloS One. 2016; 11(9):e0161542. [DOI:10.1371/journal.pone.0161542] [PMID] [PMCID]
- Raeisi AR, Torabipour A, Karimi L. Evaluating hospital safety index in Susa Public Hospital: An action research study. Bali Medical Journal. 2018; 7(2):457-61. [DOI:10.15562/bmj.v7i2.845] [Link]
- Peyravi M, Marzaleh MA, Gandomkar F, Zamani AA, Khorram-Manesh A. Hospital safety index analysis in Fars province hospitals, Iran, 2015-2016. American Journal of Disaster Medicine. 2019; 14(1):25-32. [DOI:10.5055/ajdm.2019.0313] [PMID]
- Sunindijo RY, Lestari F, Wijaya O. Hospital safety index: Assessing the readiness and resiliency of hospitals in Indonesia. Facilities. 2020; 38(1/2):39-51. [DOI:10.1108/F-12-2018-0149]
- Ministry of Health and Medical Education. [Yearbook of statistics and hospital information in 2020 (Persian)]. Tehran: Ministry of Health and Medical Education; 2020. [Link]
- Abbasabadi-Arab M. [Disaster base hospitals: A model for the military hospitals (Persian)]. Journal of Marine Medicine. 2023; 5(2):66-7. [Link]
- Naser WN, Ingrassia PL, Aladhrae S, Abdulraheem WA. A study of hospital disaster preparedness in South Yemen. Prehospital and Disaster Medicine. 2018; 33(2):133-8. [DOI:10.1017/S1049023X18000158] [PMID]
- Al Khalaileh MA, Bond E, Alasad JA. Jordanian nurses' perceptions of their preparedness for disaster management. International Emergency Nursing. 2012; 20(1):14-23. [DOI:10.1016/j.ienj.2011.01.001] [PMID]
- Djalali A, Castren M, Khankeh H, Gryth D, Radestad M, Ohlen G, et al. Hospital disaster preparedness as measured by functional capacity: A comparison between Iran and Sweden. Prehospital and Disaster Medicine. 2013; 28(5):454-61. [DOI:10.1017/S1049023X13008807] [PMID]
- Khankeh H, Abbasabadi Arab M. Developing accreditation standards for disaster risk management: An approach for hospital preparedness improvementâ-editorial (Persion)]. Journal of Military Medicine. 2022; 20(6):574-6. [Link]
- Abbasabadi M, Khankeh H, Mosadegh Rad AM. Designing of disaster risk management accreditation standards in Iranians Hospitals. International Journal for Quality in Health Care. 2018; 30(suppl 2):45-6. [DOI:10.1093/intqhc/mzy167.67]
- Zhong S, Clark M, Hou XY, Zang Y, FitzGerald G. Progress and challenges of disaster health management in China: A scoping review. Global Health Action. 2014; 7:24986. [DOI:10.3402/gha.v7.24986] [PMID] [PMCID]
- Mosadeghrad AM, Janbabaei G, Kalantari B, Darrudi A, Dehnavi H. [Equity in distribution of hospital beds in Iran (Persian)]. Scientific Journal of Kurdistan University of Medical Sciences. 2020; 24(6):12-36. [DOI:10.29252/sjku.24.6.12]
- Presidential Legal Assistant. Iran Disaster management laws. Tehran: Deputy for Compiling, Revising and Publishing Laws and Regulations; 2019. [Link]
- Madadzadeh M. Fire risk management using Fire Risk Assessment System (CFSES) software and developing a response plan in emergency situations: A case study in a hospital in Bushehr city in 2020 (Persian)] [PhD dissertation]. Kerman: Kerman University of Medical Sciences; 2020.
- Jahangiri M, Rajabi F, Darooghe F. Fire risk assessment in the selected Hospitals of Shiraz University of Medical Sciences in accordance with NFPA101. Iran Occupational Health. 2016; 13(1):99-106. [Link]
- Masoumbeigi H, Ghanizadeh G, Mirshafiee A, Raei M, Roshan Cheraghi B. [Assessment of passive defense status in Hospitalsâ food material and pharmaceutical warehouses (Persian)]. Journal of Militery Medicine. 2021; 23(6):541-51. [DOI:10.30491/JMM.23.6.541]
- Abbasabad Arab M, Navahi M, Momeni M. [Communication and information in unexpected disasters (Persian)]. Paper presented at: 2nd international Congress of Health, Care and Disaster Management. 2004; Tehran, Iran.
- Ghoddoosi-Nejad J, Daemi A, Janati A, Yaghoubi R. Investigating of safety standards and performance of emergency power diesel generators in hospitals of Tabriz, Iran. Health Technology Assessment in Action. 2021; 4(4):1-5. [DOI:10.18502/htaa.v4i4.6863]
- Abbasabadi Arab M, Khankeh HR, Mosadeghrad AM, Farrokhi M. Developing a hospital disaster risk management evaluation model. Risk Management and Healthcare Policy. 2019; 12:287-96. [DOI:10.2147/RMHP.S215444] [PMID] [PMCID]
- Jung Y. Virtual reality simulation for disaster preparedness training in hospitals: Integrated review. Journal of Medical Internet Research. 2022; 24(1):e30600. [DOI:10.2196/30600] [PMID] [PMCID]
- Beyramijam M, Khankeh H, Shahabi-Rabori MA, Aminizadeh M, Sheikhbardsiri H. Hospital disaster preparedness in Iranian province: A cross-sectional study using a standard tool. American Journal of Disaster Medicine. 2021; 16(3):233-9. [DOI:10.5055/ajdm.2021.0406] [PMID]
- Hazrati E, Mosaed R, Hamidi Farehani R, Rajabi J, Akhavan Rezayat A. Review of the Protocol for evacuation and transfer of patients in the intensive care unit in disasters. Military Caring Sciences Journal. 2020; 7(3):277-88. [DOI:10.29252/mcs.7.3.277]
- Kolivand P, Motlagh ME, Ashrafian Amiri H, Jalali SF, Yousefi Khoshsabegheh H, Nasrollahpour Shirvani SD, et al. [Strengths, weaknesses, opportunities, and threats of crisis and disaster management in Iranian public hospitals (Persian)]. Hakim Health System Research Journal. 2020; 23(3):270-81. [Link]
Type of article: Research |
Subject:
General
Received: 2022/08/16 | Accepted: 2022/10/29 | Published: 2023/07/24
Received: 2022/08/16 | Accepted: 2022/10/29 | Published: 2023/07/24
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
