

Volume 9, Issue 3 (Spring 2024)
Health in Emergencies and Disasters Quarterly 2024, 9(3): 239-246 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mohajervatan A, Ashabi M, Rezaei F. Investigating Emergency Medical System Challenges in Mass Casualty Incidents: A Case Report Study in Road Traffic Accidents in Northern Iran. Health in Emergencies and Disasters Quarterly 2024; 9 (3) :239-246
URL: http://hdq.uswr.ac.ir/article-1-468-en.html
URL: http://hdq.uswr.ac.ir/article-1-468-en.html



1- Department of Anesthesia and Pre-Hospital Emergency Care, School of Paramedical Sciences, Golestan University of Medical Sciences, Gorgan, Iran. , Mohajervatanali@yahoo.com
2- Golestan University of Medical Sciences, Gorgan, Iran.
3- Health Management and Economics Research Center, Faculty of Management and Medical Informatics, Isfahan University of Medical Science, Isfahan, Iran.
2- Golestan University of Medical Sciences, Gorgan, Iran.
3- Health Management and Economics Research Center, Faculty of Management and Medical Informatics, Isfahan University of Medical Science, Isfahan, Iran.
Full-Text [PDF 464 kb]
(43 Downloads)
| Abstract (HTML) (165 Views)
Full-Text: (24 Views)
Introduction
Mass casualty incidents (MCI) refer to situations where one or more health organizations need to work together for an effective and sustained response to a sudden event that causes a surge in the number of patients [1]. Most are marked by a relatively sudden and dramatic event that causes a surge in the number of patients. This is a significant healthcare issue, with road traffic accidents being a primary cause [2, 3]. Despite measures taken to ensure transportation safety, road accidents continue to result in numerous human injuries, deaths, and significant physical and environmental damage [4, 5]. By 2030, road traffic crashes are predicted to be a leading cause of death and disability worldwide, with developing countries bearing the brunt of these incidents [6, 7]. Currently, more than 90% of road traffic injuries occur in developing countries [8, 9]. Similarly, approximately 80% of deaths occur in the prehospital setting [10]. Emergency medical systems (EMS) play a critical role in reducing the disability and mortality resulting from road traffic accidents [11, 12]. Prehospital services in road traffic accidents are one of the essential aspects of health services. The goals of the prehospital services in traffic accidents are on-time interventions to emergency cases, prevention of disabilities, and rapid safe transportation by trained practitioners [13] Studies show that EMS teams face many challenges during mass casualty road traffic accidents [14]. MCIs often lead to resource shortages for emergency medical services, such as ambulances and emergency rooms. These resources must be managed effectively to save as many lives as possible [15]. Poor information management can lead to increased mortality in the pre-hospital period of an MCI, and there are also tactical challenges on the field in responding to MCIs [16]. According to Doohan’s research, there are also clear tactical challenges in the field of responding to MCIs in Sweden. The lack of networking and personal connections to the right people within the EMS was highlighted as a challenge [17]. This paper identifies and describes the common challenges for managing MCI situations using case reports from a practical perspective.
Materials and Methods
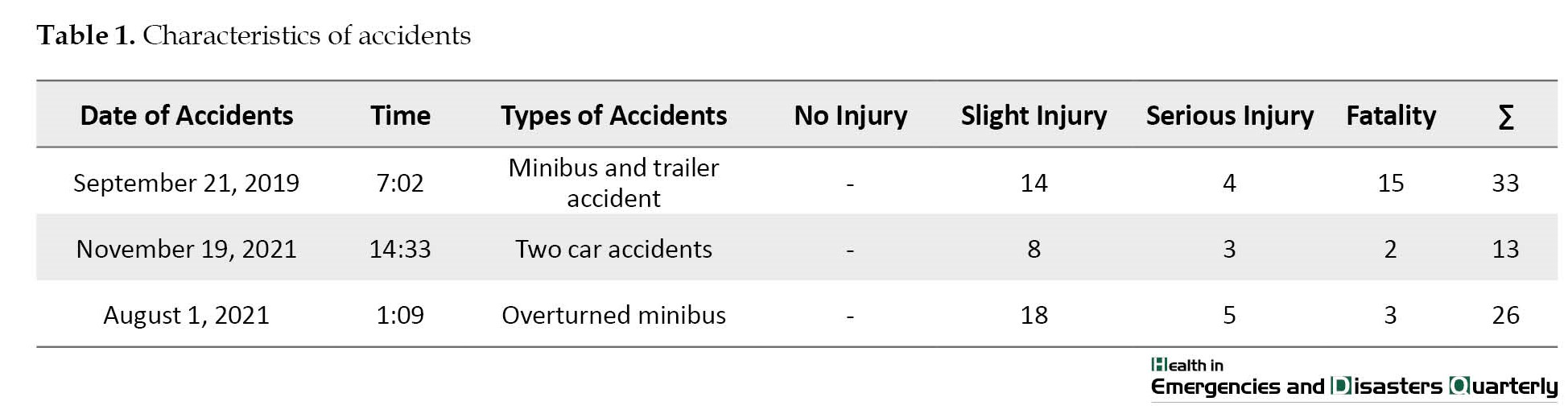
This is a case study focusing on three road accidents (Table 1) that injured more than 10 people in Golestan Province, Iran, from 2019 to 2021.
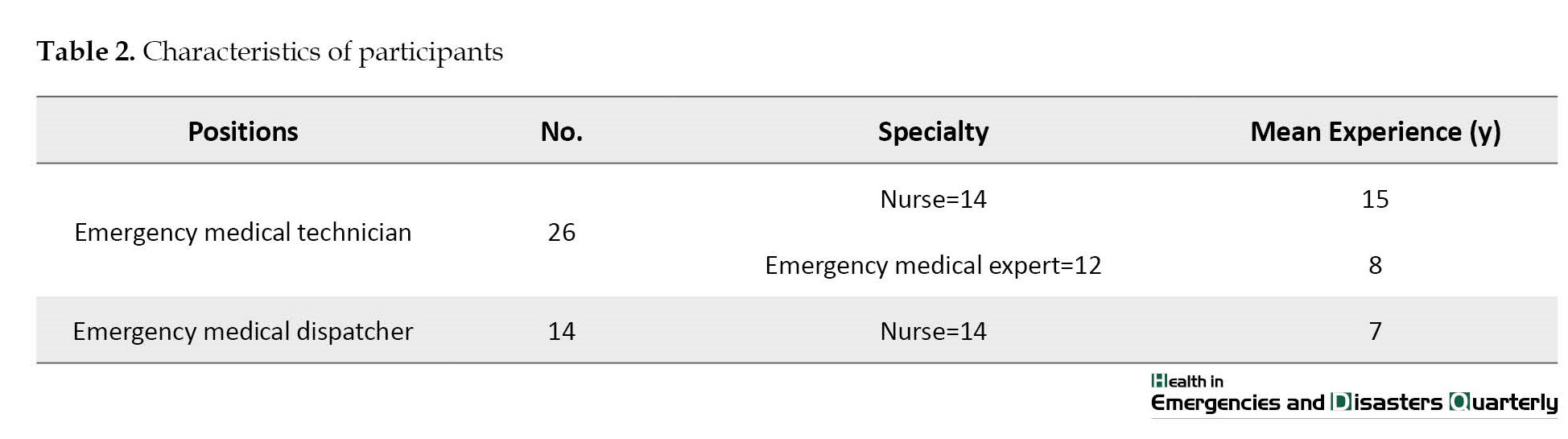
The data collection process involved recording pictures and videos from local people and aid organizations, analyzing hospital records, and reviewing pre-hospital care reports. Trained nurses extracted relevant information, such as the type and time of the accidents, the number of injured and dead, the time of calling the call center, the number of dispatched ambulances, and the EMS response time. Additionally, group meetings were held with emergency medical technicians and dispatchers who were present at the accident scenes (Table 2).
The observations and insights from these meetings were recorded, and content analysis was conducted to reach an agreement among the research team.
Cases Report
Case 1: Minibus and trailer accident
On September 21, 2019, at 7:02 AM, EMS dispatch received a call reporting an accident involving a minibus and trailer on the Gonbad-e Kavus – Incheh Borun roadway in Golestan Province, Iran. The nearest emergency station dispatched an on-call team to the scene, 22 km away. Emergency medical dispatchers initially reported a fire at the scene, and coordination was done to dispatch Red Crescent and firefighters at 7:04 AM; however, the fire department had already dispatched their teams based on calls received by their call center at 6:55 AM. The first responders were local people and road transport drivers who removed injured passengers from the minibus. Only the children could escape through the air conditioning windows when the fire spread. The Red Crescent, police, emergency organization, and the fire department were the first organizations to arrive at the scene. The first ambulance was responsible for triage and determining the collection zone, located at the nearest safe place to the accident and on the hospital side. A total of 8 ambulances arrived at the scene and transported the injured. The incident resulted in 15 deaths and 18 injuries, all caused by the fire. The response to the incident faced several challenges, including the following items: 1) Decentralization of emergency calls, leading to delays in the arrival of firefighters; 2) The first responders were not familiar with the fire extinguishing process, and despite having fire extinguishers in both vehicles, they were not used effectively, causing the fire to escalate; 3) Weaknesses in information management; 4) Concerns around the security and safety of the scene; 5) Lack of an incident commander to manage and coordinate the response efforts; and 6) Inadequate coordination between relief organizations, which further complicated the response to the incident.
Case 2: Car accident
On November 19, 2021, at 14:33, an accident involving two cars was reported to EMS dispatch on the Inche Barun-Aq Qala road. The first call reported 8 injured passengers, and the nearest ambulance was dispatched to the scene at 14:35, followed by Red Crescent rescue teams. The first ambulance arrived at the scene 7 min after the accident, but local people had already removed the injured passengers from the cars. A total of 4 ambulances were dispatched, and it took 1 h to transfer all the injured to the hospital. The accident site was crowded and the police had not yet arrived; meanwhile, the area was not properly isolated. Some local people were performing search and rescue operations, while others were bystanders. The first ambulance collected the injured passengers and triaged them, prioritizing them for specific and simultaneous dispatch to the nearest hospital. The nearest hospital was informed at the same time. When the second ambulance arrived, the first ambulance transported a patient with a lung injury that failed to recover. At that time, the second ambulance took cover at the scene; however, information was not properly shared, and a second injured passenger died due to severe internal bleeding and other injuries that were not treated in time. The incident resulted in two passengers being killed and 11 injured. The response to the incident was faced with several challenges, including the following items: 1) Issues related to information management; 2) Insufficient coordination between different organizations involved in the response efforts; 3) The challenge of establishing scene safety; and 4) Inadequate preparation of operational personnel for triage and re-triage.
Case 3: Overturned minibus
On August 1, 2021, at 1:09 AM, the EMS response center received a call reporting an overturned minibus on the Minudasht-Gonbad roadway. Emergency medical dispatchers immediately sent 10 ambulances to the accident scene. The first ambulance arrived at the scene at 1:19 AM, 9 min after the call was received; however, when the ambulance arrived, local people had already removed the injured from the vehicle. The first ambulance immediately began the process of collecting the injured in safe places and triaging them. The Red Crescent, police, and fire department arrived at the scene after the first ambulance. The incident resulted in 3 deaths and 23 injuries. The response to the incident faced several challenges including the following items: 1) The transfer of information from the incident field to decision centers; 2) Information sharing; 3) Cooperation of medical and security officers in scene management; 4) The continuation of providing pre-hospital care in other simultaneous emergency cases in other covered areas; 5) Compliance with legal and safety requirements; and 6) Management of dead bodies.
Discussion
The challenges that were found in this study are the inability to respond to road traffic accidents in three sections as follows: First responders, dispatch, and field functions. We will put forth these items into discussion in the following section:
First responder
The results of the conducted survey showed that local people and road users are usually the first responders to accidents; however, the study found that despite being the first to respond in all cases investigated, local communities were unable to play an effective role in reducing casualties due to their inability to provide rescue, firefighting, scene management, and coordination with relief teams. Other studies have also emphasized the potential of lay first responders (LFRs) as a cost-effective means of addressing road traffic injury (RTI) morbidity and mortality. Training LFRs can be an affordable first step toward formal EMS development [18]. However, cultural conditions, knowledge, relief organizations, and demographic factors can affect the interventions of ordinary people in the accident scene [19]. The results of Khankeh’s study showed that the public’s presence at the crash scene can lead to a crowded pile-up and poor communication due to personal curiosity, enthusiasm for humanistic help, excitement, and haste [13]. Other studies have emphasized that increasing the intervention of each type of trained first responder (bystander, laypeople, first responders, and LFRs) can have a significant impact on the reduction of complications caused by road traffic crashes [20]. According to the study by Eftekhari, poor management is one of the current challenges of RTIs in Iran, and passersby’s intervention at the crash scene can either facilitate or debilitate preventive care in RTIs [21].
Dispatch centers
Dispatch centers play a critical role in managing public calls during emergencies. In addition to sending ambulances, they are responsible for informing other relief organizations. Our study revealed that the main challenge faced by dispatch centers is the coordination and deployment of teams and the management of inter-organizational information. When a patient calls 115, the EMS team’s pathway to emergency care begins. Most EMS systems perform caller screening, triage, and paramedic deployment, followed by emergency response, on-scene assessment and care, and transfer to the emergency department [22]. Dispatch centers usually do their job correctly in screening calls and sending resources in needed cases; however, the challenge for dispatch centers is to continue providing services in the event of accidents without causing challenges in other areas. Sending ambulances without considering the potential request of EMS in other areas is one of the most significant challenges in responding to incidents under study. To address this issue, the management of such incidents should not cause challenges in other areas. The lack of resources in one area can be compensated by various methods, such as triage of the injured, prioritization and capacity-building programs, and the use of other local capacities. Special attention to the continuation of pre-hospital care in the event of high-risk accidents requires special attention, which can be a good context for future research. However, MCIs are unpredictable, uncertain, and dynamic, making it difficult to adequately prepare and respond to them. EMS and other resources are typically fully utilized for routine medical services, and dispatch personnel often cannot estimate or decide on the amounts and types of resources needed due to the unclear epidemiological characteristics of MCIs [23, 24]. According to our results, experienced personnel in dispatch centers are more capable of managing MCIs and dealing with uncertainty, and a lack of confirmed information, such as the number of injured people [25]. MCIs and most disasters, require incident commanders to use their intuitive sense or gut feeling, rather than exact information, to respond effectively [26, 27].
Field performance
One of the key findings of the study is that emergency responders arrived as quickly as possible at the scene in each case, which is crucial for stabilizing occupants with life-threatening injuries. Another study also found that early arrival of EMS teams at the scene, timely triage, and transfer to the hospital can stabilize patients with life-threatening injuries and reduce the risk of fatalities, which has a direct impact on the affected individuals’ standard of living [28, 29]. However, despite having quick access to the accident scene, some of the relief efforts lacked integrity, rendering them ineffective. Interventions involved locating the collection zone, triage area, and injured persons in the waiting area for loading, which are crucial tasks for the response teams according to other studies [30]. Triage is one of the most significant pre-hospital emergency challenges in accidents, where a lack of resources requires prioritization of patients. Although personnel could perform the initial triage, a lack of attention to re-triage has caused more injuries in some cases [31]. Triage occurs at various points and by various healthcare professionals for various reasons, including deciding whether a patient needs to be taken to a trauma center. The majority of emergency personnel make the same decisions every day, largely based on the same data that is used for triaging mass casualties. Tough decisions must be made more quickly in the case of mass casualty triage, leaving less time for providers to gather data. Additionally, in a mass casualty situation, the priority is to ensure the best outcome for the greatest number of patients rather than the best outcome for each patient [32]. However, sometimes triage mistakes lead to patients being categorized incorrectly, which ultimately results in the inappropriate use of resources, hindering the provision of efficient emergency care [33-35]. Under-triage happens when patients who need immediate care for life-threatening injuries are wrongly assigned to receive that care later, while over-triage happens when patients with non-critical injuries are labeled as urgent and need immediate care [36-38]. Failure to follow the triage algorithm is a significant factor in triage errors, which can occur up to 26% of the time [36, 39, 40]. Variations in triage performance were also found across different training levels of prehospital personnel, where the highest adherence rates occurred among the lowest-level trained personnel [39]. Selecting the most qualified responder to perform triage during a major incident may help minimize these errors [41]. Although triage is a crucial skill when dealing with MCIs, it is not always used in actual incidents, despite training. Disaster managers and EMS trainers should consider using MCI concepts in practical situations [31]. Apart from the lack of knowledge and protocol for performing triage, other factors, such as the lack of identification of the triage officer and the location of loading injured patients have also affected the quality of relief services. The review of reported cases showed that most organizations are confused at the beginning of the incident response due to limited reliable data on the number of casualties and lack of experience with similar incidents. This confusion has gradually decreased with the presence of relief teams. Dealing with uncertainty, unpredictability, and unexpected consequences was a significant challenge in many of the described events, with conflicting, unreliable, and a lack of information making decision-making more difficult than usual. The lack of a precise count of casualties caused frustration and made it difficult to decide whether the situation was a mass casualty or disaster [42]. When the first patients arrive in the emergency room, it takes some time before the emergency plan is put into action due to insufficient information [43]. Therefore, responsible organizations must be prepared and trained to respond to MCIs [44]. This study has potential limitations that may have influenced our results. The limitations include: 1) The lack of access to first responders to check the level of first aid training, causes and levels of intervention, 2) The lack of access to the database of relief organizations, and 3) Not using the opinions of other rescue teams present at the scene.
Conclusion
The challenges regarding mass casualty management are mainly concerned with the ability to manage the incident scene by the first responders and the call management and information exchange in message centers as well as field medical measures. In each of these cases, medical or non-medical factors and internal factors, such as experience and stress among staff influenced the medical management and decision-making process. In short, to respond in an effective, timely, and resilient way, all factors should be considered in both the planning and operation phases of MCI. The development of education, communication strategies, and standardized policies for EMS across all MCIs is essential to improve the EMS service in the future. Also, we believe that comparing different countries’ responses to MCI could be an important area of future research that helps improve planning.
Ethical Considerations
Compliance with ethical guidelines
The project has been executed in compliance with ethical principles and national regulations for conducting medical research in Iran and was approved by the Golestan University of Medical Sciences (Code: IR.GOUMS.REC.1400.283).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, data analysis and writing the original draft: Ali Mohajervatan; Review and editing: Mitra Ashabi and Fatemeh Rezaei; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all of the managers and staff from the emergency medical system who participated in the focus groups and shared their experiences with the study team.
References
Mass casualty incidents (MCI) refer to situations where one or more health organizations need to work together for an effective and sustained response to a sudden event that causes a surge in the number of patients [1]. Most are marked by a relatively sudden and dramatic event that causes a surge in the number of patients. This is a significant healthcare issue, with road traffic accidents being a primary cause [2, 3]. Despite measures taken to ensure transportation safety, road accidents continue to result in numerous human injuries, deaths, and significant physical and environmental damage [4, 5]. By 2030, road traffic crashes are predicted to be a leading cause of death and disability worldwide, with developing countries bearing the brunt of these incidents [6, 7]. Currently, more than 90% of road traffic injuries occur in developing countries [8, 9]. Similarly, approximately 80% of deaths occur in the prehospital setting [10]. Emergency medical systems (EMS) play a critical role in reducing the disability and mortality resulting from road traffic accidents [11, 12]. Prehospital services in road traffic accidents are one of the essential aspects of health services. The goals of the prehospital services in traffic accidents are on-time interventions to emergency cases, prevention of disabilities, and rapid safe transportation by trained practitioners [13] Studies show that EMS teams face many challenges during mass casualty road traffic accidents [14]. MCIs often lead to resource shortages for emergency medical services, such as ambulances and emergency rooms. These resources must be managed effectively to save as many lives as possible [15]. Poor information management can lead to increased mortality in the pre-hospital period of an MCI, and there are also tactical challenges on the field in responding to MCIs [16]. According to Doohan’s research, there are also clear tactical challenges in the field of responding to MCIs in Sweden. The lack of networking and personal connections to the right people within the EMS was highlighted as a challenge [17]. This paper identifies and describes the common challenges for managing MCI situations using case reports from a practical perspective.
Materials and Methods
This is a case study focusing on three road accidents (Table 1) that injured more than 10 people in Golestan Province, Iran, from 2019 to 2021.
The data collection process involved recording pictures and videos from local people and aid organizations, analyzing hospital records, and reviewing pre-hospital care reports. Trained nurses extracted relevant information, such as the type and time of the accidents, the number of injured and dead, the time of calling the call center, the number of dispatched ambulances, and the EMS response time. Additionally, group meetings were held with emergency medical technicians and dispatchers who were present at the accident scenes (Table 2).
The observations and insights from these meetings were recorded, and content analysis was conducted to reach an agreement among the research team.
Cases Report
Case 1: Minibus and trailer accident
On September 21, 2019, at 7:02 AM, EMS dispatch received a call reporting an accident involving a minibus and trailer on the Gonbad-e Kavus – Incheh Borun roadway in Golestan Province, Iran. The nearest emergency station dispatched an on-call team to the scene, 22 km away. Emergency medical dispatchers initially reported a fire at the scene, and coordination was done to dispatch Red Crescent and firefighters at 7:04 AM; however, the fire department had already dispatched their teams based on calls received by their call center at 6:55 AM. The first responders were local people and road transport drivers who removed injured passengers from the minibus. Only the children could escape through the air conditioning windows when the fire spread. The Red Crescent, police, emergency organization, and the fire department were the first organizations to arrive at the scene. The first ambulance was responsible for triage and determining the collection zone, located at the nearest safe place to the accident and on the hospital side. A total of 8 ambulances arrived at the scene and transported the injured. The incident resulted in 15 deaths and 18 injuries, all caused by the fire. The response to the incident faced several challenges, including the following items: 1) Decentralization of emergency calls, leading to delays in the arrival of firefighters; 2) The first responders were not familiar with the fire extinguishing process, and despite having fire extinguishers in both vehicles, they were not used effectively, causing the fire to escalate; 3) Weaknesses in information management; 4) Concerns around the security and safety of the scene; 5) Lack of an incident commander to manage and coordinate the response efforts; and 6) Inadequate coordination between relief organizations, which further complicated the response to the incident.
Case 2: Car accident
On November 19, 2021, at 14:33, an accident involving two cars was reported to EMS dispatch on the Inche Barun-Aq Qala road. The first call reported 8 injured passengers, and the nearest ambulance was dispatched to the scene at 14:35, followed by Red Crescent rescue teams. The first ambulance arrived at the scene 7 min after the accident, but local people had already removed the injured passengers from the cars. A total of 4 ambulances were dispatched, and it took 1 h to transfer all the injured to the hospital. The accident site was crowded and the police had not yet arrived; meanwhile, the area was not properly isolated. Some local people were performing search and rescue operations, while others were bystanders. The first ambulance collected the injured passengers and triaged them, prioritizing them for specific and simultaneous dispatch to the nearest hospital. The nearest hospital was informed at the same time. When the second ambulance arrived, the first ambulance transported a patient with a lung injury that failed to recover. At that time, the second ambulance took cover at the scene; however, information was not properly shared, and a second injured passenger died due to severe internal bleeding and other injuries that were not treated in time. The incident resulted in two passengers being killed and 11 injured. The response to the incident was faced with several challenges, including the following items: 1) Issues related to information management; 2) Insufficient coordination between different organizations involved in the response efforts; 3) The challenge of establishing scene safety; and 4) Inadequate preparation of operational personnel for triage and re-triage.
Case 3: Overturned minibus
On August 1, 2021, at 1:09 AM, the EMS response center received a call reporting an overturned minibus on the Minudasht-Gonbad roadway. Emergency medical dispatchers immediately sent 10 ambulances to the accident scene. The first ambulance arrived at the scene at 1:19 AM, 9 min after the call was received; however, when the ambulance arrived, local people had already removed the injured from the vehicle. The first ambulance immediately began the process of collecting the injured in safe places and triaging them. The Red Crescent, police, and fire department arrived at the scene after the first ambulance. The incident resulted in 3 deaths and 23 injuries. The response to the incident faced several challenges including the following items: 1) The transfer of information from the incident field to decision centers; 2) Information sharing; 3) Cooperation of medical and security officers in scene management; 4) The continuation of providing pre-hospital care in other simultaneous emergency cases in other covered areas; 5) Compliance with legal and safety requirements; and 6) Management of dead bodies.
Discussion
The challenges that were found in this study are the inability to respond to road traffic accidents in three sections as follows: First responders, dispatch, and field functions. We will put forth these items into discussion in the following section:
First responder
The results of the conducted survey showed that local people and road users are usually the first responders to accidents; however, the study found that despite being the first to respond in all cases investigated, local communities were unable to play an effective role in reducing casualties due to their inability to provide rescue, firefighting, scene management, and coordination with relief teams. Other studies have also emphasized the potential of lay first responders (LFRs) as a cost-effective means of addressing road traffic injury (RTI) morbidity and mortality. Training LFRs can be an affordable first step toward formal EMS development [18]. However, cultural conditions, knowledge, relief organizations, and demographic factors can affect the interventions of ordinary people in the accident scene [19]. The results of Khankeh’s study showed that the public’s presence at the crash scene can lead to a crowded pile-up and poor communication due to personal curiosity, enthusiasm for humanistic help, excitement, and haste [13]. Other studies have emphasized that increasing the intervention of each type of trained first responder (bystander, laypeople, first responders, and LFRs) can have a significant impact on the reduction of complications caused by road traffic crashes [20]. According to the study by Eftekhari, poor management is one of the current challenges of RTIs in Iran, and passersby’s intervention at the crash scene can either facilitate or debilitate preventive care in RTIs [21].
Dispatch centers
Dispatch centers play a critical role in managing public calls during emergencies. In addition to sending ambulances, they are responsible for informing other relief organizations. Our study revealed that the main challenge faced by dispatch centers is the coordination and deployment of teams and the management of inter-organizational information. When a patient calls 115, the EMS team’s pathway to emergency care begins. Most EMS systems perform caller screening, triage, and paramedic deployment, followed by emergency response, on-scene assessment and care, and transfer to the emergency department [22]. Dispatch centers usually do their job correctly in screening calls and sending resources in needed cases; however, the challenge for dispatch centers is to continue providing services in the event of accidents without causing challenges in other areas. Sending ambulances without considering the potential request of EMS in other areas is one of the most significant challenges in responding to incidents under study. To address this issue, the management of such incidents should not cause challenges in other areas. The lack of resources in one area can be compensated by various methods, such as triage of the injured, prioritization and capacity-building programs, and the use of other local capacities. Special attention to the continuation of pre-hospital care in the event of high-risk accidents requires special attention, which can be a good context for future research. However, MCIs are unpredictable, uncertain, and dynamic, making it difficult to adequately prepare and respond to them. EMS and other resources are typically fully utilized for routine medical services, and dispatch personnel often cannot estimate or decide on the amounts and types of resources needed due to the unclear epidemiological characteristics of MCIs [23, 24]. According to our results, experienced personnel in dispatch centers are more capable of managing MCIs and dealing with uncertainty, and a lack of confirmed information, such as the number of injured people [25]. MCIs and most disasters, require incident commanders to use their intuitive sense or gut feeling, rather than exact information, to respond effectively [26, 27].
Field performance
One of the key findings of the study is that emergency responders arrived as quickly as possible at the scene in each case, which is crucial for stabilizing occupants with life-threatening injuries. Another study also found that early arrival of EMS teams at the scene, timely triage, and transfer to the hospital can stabilize patients with life-threatening injuries and reduce the risk of fatalities, which has a direct impact on the affected individuals’ standard of living [28, 29]. However, despite having quick access to the accident scene, some of the relief efforts lacked integrity, rendering them ineffective. Interventions involved locating the collection zone, triage area, and injured persons in the waiting area for loading, which are crucial tasks for the response teams according to other studies [30]. Triage is one of the most significant pre-hospital emergency challenges in accidents, where a lack of resources requires prioritization of patients. Although personnel could perform the initial triage, a lack of attention to re-triage has caused more injuries in some cases [31]. Triage occurs at various points and by various healthcare professionals for various reasons, including deciding whether a patient needs to be taken to a trauma center. The majority of emergency personnel make the same decisions every day, largely based on the same data that is used for triaging mass casualties. Tough decisions must be made more quickly in the case of mass casualty triage, leaving less time for providers to gather data. Additionally, in a mass casualty situation, the priority is to ensure the best outcome for the greatest number of patients rather than the best outcome for each patient [32]. However, sometimes triage mistakes lead to patients being categorized incorrectly, which ultimately results in the inappropriate use of resources, hindering the provision of efficient emergency care [33-35]. Under-triage happens when patients who need immediate care for life-threatening injuries are wrongly assigned to receive that care later, while over-triage happens when patients with non-critical injuries are labeled as urgent and need immediate care [36-38]. Failure to follow the triage algorithm is a significant factor in triage errors, which can occur up to 26% of the time [36, 39, 40]. Variations in triage performance were also found across different training levels of prehospital personnel, where the highest adherence rates occurred among the lowest-level trained personnel [39]. Selecting the most qualified responder to perform triage during a major incident may help minimize these errors [41]. Although triage is a crucial skill when dealing with MCIs, it is not always used in actual incidents, despite training. Disaster managers and EMS trainers should consider using MCI concepts in practical situations [31]. Apart from the lack of knowledge and protocol for performing triage, other factors, such as the lack of identification of the triage officer and the location of loading injured patients have also affected the quality of relief services. The review of reported cases showed that most organizations are confused at the beginning of the incident response due to limited reliable data on the number of casualties and lack of experience with similar incidents. This confusion has gradually decreased with the presence of relief teams. Dealing with uncertainty, unpredictability, and unexpected consequences was a significant challenge in many of the described events, with conflicting, unreliable, and a lack of information making decision-making more difficult than usual. The lack of a precise count of casualties caused frustration and made it difficult to decide whether the situation was a mass casualty or disaster [42]. When the first patients arrive in the emergency room, it takes some time before the emergency plan is put into action due to insufficient information [43]. Therefore, responsible organizations must be prepared and trained to respond to MCIs [44]. This study has potential limitations that may have influenced our results. The limitations include: 1) The lack of access to first responders to check the level of first aid training, causes and levels of intervention, 2) The lack of access to the database of relief organizations, and 3) Not using the opinions of other rescue teams present at the scene.
Conclusion
The challenges regarding mass casualty management are mainly concerned with the ability to manage the incident scene by the first responders and the call management and information exchange in message centers as well as field medical measures. In each of these cases, medical or non-medical factors and internal factors, such as experience and stress among staff influenced the medical management and decision-making process. In short, to respond in an effective, timely, and resilient way, all factors should be considered in both the planning and operation phases of MCI. The development of education, communication strategies, and standardized policies for EMS across all MCIs is essential to improve the EMS service in the future. Also, we believe that comparing different countries’ responses to MCI could be an important area of future research that helps improve planning.
Ethical Considerations
Compliance with ethical guidelines
The project has been executed in compliance with ethical principles and national regulations for conducting medical research in Iran and was approved by the Golestan University of Medical Sciences (Code: IR.GOUMS.REC.1400.283).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, data analysis and writing the original draft: Ali Mohajervatan; Review and editing: Mitra Ashabi and Fatemeh Rezaei; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all of the managers and staff from the emergency medical system who participated in the focus groups and shared their experiences with the study team.
References
- Ryan JM, Doll D. Mass casualties and triage. In: Velmahos G, Degiannis E, Doll D, editors. Penetrating trauma. Berlin: Springer; 2012. [DOI:10.1007/978-3-642-20453-1_21]
- Doughty H, Glasgow S, Kristoffersen E. Mass casualty events: Blood transfusion emergency preparedness across the continuum of care. Transfusion. 2016; 56(S2):S208-16. [DOI:10.1111/trf.13488]
- McElroy JA, Steinberg S, Keller J, Falcone RE. Operation continued care: A large mass-casualty, full-scale exercise as a test of regional preparedness. Surgery. 2019; 166(4):587-92. [DOI:10.1016/j.surg.2019.05.045] [PMID]
- Fountas G, Sarwar MT, Anastasopoulos PC, Blatt A, Majka K. Analysis of stationary and dynamic factors affecting highway accident occurrence: A dynamic correlated grouped random parameters binary logit approach. Accident Analysis & Prevention. 2018; 113:330-40. [DOI:10.1016/j.aap.2017.05.018] [PMID]
- Najaf P, Isaai MT, Lavasani M, Thill JC. Evaluating traffic safety policies for developing countries based on equity considerations. Journal of Transportation Safety & Security. 2017; 9(sup1):178-203. [DOI:10.1080/19439962.2016.1230163]
- Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Medicine. 2006; 3(11):e442. [DOI:10.1371/journal.pmed.0030442] [PMID]
- WHO. The global burden of disease: 2004 update. Geneva: WHO; 2008. [Link]
- Hofman K, Primack A, Keusch G, Hrynkow S. Addressing the growing burden of trauma and injury in low- and middle-income countries. American Journal of Public Health. 2005; 95(1):13-7. [DOI:10.2105/AJPH.2004.039354] [PMID]
- Murray CJL, Lopez AD. Global health statistics: A compendium of incidence, prevalence and mortality estimates for over 200 conditions. Boston: Harvard University Press; 1996. [Link]
- Mock CN, Jurkovich GJ, nii-Amon-Kotei D, Arreola-Risa C, Maier RV. Trauma mortality patterns in three nations at different economic levels: Implications for global trauma system development. Journal of Trauma and Acute Care Surgery. 1998; 44(5):804-12. [DOI:10.1097/00005373-199805000-00011] [PMID]
- Candefjord S, Buendia R, Caragounis EC, Sjöqvist BA, Fagerlind H. Prehospital transportation decisions for patients sustaining major trauma in road traffic crashes in Sweden. Traffic Injury Prevention. 2016; 17 Suppl 1:16-20. [DOI:10.1080/15389588.2016.1198872] [PMID]
- Coats TJ, Davies G. Prehospital care for road traffic casualties. BMJ (Clinical Research ed.). 2002; 324(7346):1135-8. [DOI:10.1136/bmj.324.7346.1135] [PMID]
- Khankeh H, Alinia S, Masoumi G, Khorasani zavareh D, Ranjbar M, Daddoost L, et al. [Prehospital services by focus on road traffic accidents: Assessment developed and developing countries (Persian)]. Journal of Health Promotion Management. 2013; 2(2):71-9. [Link]
- Safi Keykaleh M, Sohrabizadeh S. The Emergency Medical System (EMS) response to Iraqi pilgrims' bus crash in Iran: A case report. BMC Emergency Medicine. 2019; 19(1):38. [DOI:10.1186/s12873-019-0253-2] [PMID]
- Shin K, Lee T. Emergency medical service resource allocation in a mass casualty incident by integrating patient prioritization and hospital selection problems. IISE Transactions. 2020; 52(10):1141-55. [DOI:10.1080/24725854.2020.1727069]
- Perry O, Jaffe E, Bitan Y. Dynamic communication quantification model for measuring information management during mass-casualty incident simulations. Human Factors. 2022; 64(1):228-49. [DOI:10.1177/00187208211018880] [PMID]
- Doohan IS, Saveman B-I, Gyllencreutz L. Limited medical perspective at a strategic level in relation to mass casualty incidents in Swedish tunnels. International Journal of Emergency Management. 2019; 15(4):360-74. [DOI:10.1504/IJEM.2019.104205]
- Delaney PG, Eisner ZJ, Bustos A, Hancock CJ, Thullah AH, Jayaraman S, et al. Cost-effectiveness of lay first responders addressing road traffic injury in Sub-Saharan Africa. The Journal of Surgical Research. 2022; 270:104-12. [DOI:10.1016/j.jss.2021.08.032] [PMID]
- Heidari M, Aryankhesal A, Khorasani-Zavareh D. Laypeople roles at road traffic crash scenes: A systematic review. International Journal of Injury Control and Safety Promotion. 2019; 26(1):82-91. [DOI:10.1080/17457300.2018.148186] [PMID]
- Aryankhesal A, Khorasani-Zavareh D, Heidari M. People present at road traffic crash scene: Challenges in defining and categorising. Journal of Clinical and Diagnostic Research. 2018; 12(1):LL01-2. [DOI:10.7860/JCDR/2018/32172.11132]
- Haghani F, Sadeghi N. [Training In pre-hospital emergency: Needs and truths (Persian)]. Iranian Journal of Medical Education. 2011; 10(5):1273-80. [Link]
- Jensen JL, Travers AH, Carter AJE. Care begins when 9-1-1 is called: The evolving role of paramedic specialists in EMS Medical Communications Centres. CJEM. 2022; 24(2):115-16. [DOI:10.1007/s43678-022-00284-2] [PMID]
- Kuisma M, Hiltunen T, Määttä T, Puolakka J, Boyd J, Nousila-Wiik M, et al. Analysis of multiple casualty incidents - A prospective cohort study. Acta Anaesthesiologica Scandinavica. 2005; 49(10):1527-33. [DOI:10.1111/j.1399-6576.2005.00761.x] [PMID]
- Park JO, Shin SD, Song KJ, Hong KJ, Kim J. Epidemiology of emergency medical services-Assessed mass casualty incidents according to causes. Journal of Korean Medical Science. 2016; 31(3):449-56. [DOI:10.3904/kjm.2016.90.5.449] [PMID]
- Glick JA, Barbara JA. Moving from situational awareness to decisions during disaster response: Transition to decision making. Journal of emergency management (Weston, Mass.). 2013; 11(6):423-32. [DOI:10.5055/jem.2013.0155] [PMID]
- Rimstad R, Braut GS. Literature review on medical incident command. Prehospital and Disaster Medicine. 2015; 30(2):205-15. [DOI:10.1017/S1049023X15000035] [PMID]
- Wong EG, Trelles M, Dominguez L, Gupta S, Burnham G, Kushner AL. Surgical skills needed for humanitarian missions in resource-limited settings: Common operative procedures performed at Médecins Sans Frontières facilities. Surgery. 2014; 156(3):642-9. [DOI:10.1016/j.surg.2014.02.002] [PMID]
- Brown J, Sajankila N, Claridge JA. Prehospital Assessment of Trauma. The Surgical Clinics of North America. 2017; 97(5):961-83. [DOI:10.1016/j.suc.2017.06.007] [PMID]
- Byrne JP, Mann NC, Dai M, Mason SA, Karanicolas P, Rizoli S, et al. Association between emergency medical service response time and motor vehicle crash mortality in the United States. JAMA Surgery. 2019; 154(4):286-93. [DOI:10.1001/jamasurg.2018.5097] [PMID]
- Raeisi A R, Mohajervatan A, Mehraein Nazdik Z. Mass casualty response to mine explosion: A case report in Iran. Health in Emergencies and Disasters Quarterly. 2019; 4(3):173-8. [DOI:10.32598/hdq.4.3.173]
- Ryan K, George D, Liu J, Mitchell P, Nelson K, Kue R. The use of field triage in disaster and mass casualty incidents: A survey of current practices by EMS personnel. Prehospital Emergency Care. 2018; 22(4):520-6. [DOI:10.1080/10903127.2017.1419323] [PMID]
- Lerner EB, Schwartz RB, Coule PL, Weinstein ES, Cone DC, Hunt RC, et al. Mass casualty triage: An evaluation of the data and development of a proposed national guideline. Disaster Medicine and Public Health Preparedness. 2008; 2(Suppl 1):S25-34. [DOI:10.1097/DMP.0b013e318182194e] [PMID]
- Ngabirano AA. A comparison between differently skilled pre-hospital emergency care providers in major incident triage in South Africa [MSc thesis]. Stellenbosch: Stellenbosch University; 2018. [Link]
- Frykberg ER. Triage: Principles and practice. Scandinavian Journal of Surgery. 2005; 94(4):272-8. [DOI:10.1177/145749690509400405] [PMID]
- Frykberg ER. Medical management of disasters and mass casualties from terrorist bombings: How can we cope? The Journal of Trauma. 2002; 53(2):201-12. [DOI:10.1097/00005373-200208000-00001] [PMID]
- van Laarhoven JJ, Lansink KW, van Heijl M, Lichtveld RA, Leenen LP. Accuracy of the field triage protocol in selecting severely injured patients after high energy trauma. Injury. 2014; 45(5):869-73. [DOI:10.1016/j.injury.2013.12.010] [PMID]
- Postma IL, Weel H, Heetveld MJ, van der Zande I, Bijlsma TS, Bloemers FW, et al. Patient distribution in a mass casualty event of an airplane crash. Injury. 2013; 44(11):1574-8. [DOI:10.1016/j.injury.2013.04.027] [PMID]
- Postma IL, Weel H, Heetveld MJ, van der Zande I, Bijlsma TS, Bloemers FW, et al. Mass casualty triage after an airplane crash near Amsterdam. Injury. 2013; 44(8):1061-7. [DOI:10.1016/j.injury.2013.03.038] [PMID]
- Fitzharris M, Stevenson M, Middleton P, Sinclair G. Adherence with the pre-hospital triage protocol in the transport of injured patients in an urban setting. Injury. 2012; 43(9):1368-76. [DOI:10.1016/j.injury.2011.10.019] [PMID]
- Wong C, Lui C, So F, Tsui K, Tang S. Prevalence and predictors of under-diversion in the Primary Trauma Diversion System in Hong Kong. Hong Kong Journal of Emergency Medicine. 2013; 20(5):276-86. [DOI:10.1177/102490791302000503]
- Robertson-Steel I. Evolution of triage systems. Emergency Medicine Journal: EMJ. 2006; 23(2):154-5. [DOI:10.1136/emj.2005.030270] [PMID]
- Carli P, Telion C. Paris City disaster: Response to the recent terror attacks and lessons learned. Current Trauma Reports. 2018; 4(2):96-102. [DOI:10.1007/s40719-018-0119-1]
- El Sayed M, Chami AF, Hitti E. Developing a hospital disaster preparedness plan for mass casualty incidents: Lessons learned from the downtown beirut bombing. Disaster Medicine and Public Health Preparedness. 2018; 12(3):379-85. [DOI:10.1017/dmp.2017.83] [PMID]
- Hugelius K, Becker J, Adolfsson A. Five challenges when managing mass casualty or disaster situations: A review study. International Journal of Environmental Research and Public Health. 2020; 17(9):3068. [DOI:10.3390/ijerph17093068] [PMID]
Type of Study: Case Report |
Subject:
Special
Received: 2022/11/2 | Accepted: 2024/01/18 | Published: 2024/04/1
Received: 2022/11/2 | Accepted: 2024/01/18 | Published: 2024/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Health in Emergencies and Disasters Quarterly
Health in Emergencies & Disasters Research Center, University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave, Tehran, Iran.
Journal Tel: +9821 71732816 (2816)
Publisher Tel: +9821 4535 5555 - 4535 5000
