

Volume 9, Issue 2 (Winter 2024)
Health in Emergencies and Disasters Quarterly 2024, 9(2): 107-114 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Eskandari Z, Dehghani A, Farzaneh H, Masoumi G. Development of a National Guide for Designing the Structure of Makeshift Hospital: With Focus on Pandemics. Health in Emergencies and Disasters Quarterly 2024; 9 (2) :107-114
URL: http://hdq.uswr.ac.ir/article-1-477-en.html
URL: http://hdq.uswr.ac.ir/article-1-477-en.html



1- Department of Medical Emergencies, School of Nursing, Alborz University of Medical Sciences, Alborz, Iran.
2- Safety Promotion and Injury Prevention Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
3- Department of Health in Emergencies and Disasters, Emergency Management Research Center, School of Health Management and Information Services, Iran University of Medical Sciences, Tehran, Iran.
4- Department of Health in Emergencies and Disasters, Emergency Management Research Center, School of Health Management and Information Services, Iran University of Medical Sciences, Tehran, Iran. , greza.masoumi@gmail.com
2- Safety Promotion and Injury Prevention Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
3- Department of Health in Emergencies and Disasters, Emergency Management Research Center, School of Health Management and Information Services, Iran University of Medical Sciences, Tehran, Iran.
4- Department of Health in Emergencies and Disasters, Emergency Management Research Center, School of Health Management and Information Services, Iran University of Medical Sciences, Tehran, Iran. , greza.masoumi@gmail.com
Full-Text [PDF 549 kb]
(98 Downloads)
| Abstract (HTML) (778 Views)
Full-Text: (44 Views)
Introduction
Epidemics are threats to communities and their health. Epidemics have deeply affected societies throughout history and drastically changed the economic, political, and social aspects of human civilization. Epidemics and outbreaks, such as COVID-19, irreparably impact psychological, social, and economic aspects and change the health service delivery system. Since epidemics are considered a threat to humans, their management is critical [1].
The COVID-19 infection was detected in December 2019 in Wuhan, China, with a high capacity to spread from one person to another quickly. It immediately spread worldwide [2] and was pronounced a critical public health concern by the World Health Organization (WHO) [3]. Iran is experiencing the widespread ongoing transmission of COVID-19 and is one of the level III warning countries with a total of 7 562 610 COVID-19 cases and 144 727 deaths (January 15, 2023, 17:49 GMT) [4].
After detecting COVID-19 and the first case on February 29, 2019, countries faced a short-term increase in inpatients. As one of the challenges for the healthcare system, health authorities were forced to plan and set up temporary hospital hotspots to provide care to patients and healthcare services. A total of 27 000 beds with suitable logistics and treatment systems were available in 300 areas [5]. The preparedness of makeshift hospitals for management, planning, execution, construction incidents, disasters, and epidemics is fundamental to providing appropriate and timely health services [6].
These centers can accept people who were not hospitalized; however, they need to be isolated and under care, and this possibility is unavailable to them at home [7]. Various services, such as medical, pharmaceuticals, nutrition, personal hygiene, education, health promotion services, mental health, and spiritual counseling, were offered to all patients in makeshift hospitals [8].
One of the practical components of managing medical centers in incidents and disasters is the presence of standard operating procedures and incident command systems [9].
Using globally recognized strategies to manage the hospital emergency management system can help improve the quality of healthcare services [10]. In makeshift hospitals, there is a need to plan an incident command system and describe the organizational obligations to respond appropriately and timely [11]. These documents are not specific regarding the features and type of services in makeshift hospitals. Considering that all countries in incidents, disasters, and epidemics require the establishment of makeshift hospitals, this study plans for an eligible and appropriate organizational construction to provide services an executive and operational plan to manage makeshift hospitals in epidemics, disasters, and incidents.
Materials and Methods
Study design
This was a cross-sectional descriptive-analytical study in two phases of review and Delphi studies to develop a public fact sheet guide and the construction of the makeshift hospitals.
In the first phase of the research, the required data was extracted by exploring the sources and texts of various documents regarding the makeshift hospital and the management of the diseases of the COVID-19 epidemic. The final records were analyzed.
In the second phase, the expert panel method was used to design the construction of the makeshift hospital.
Study participants
The participants consisted of professionals, policymakers, senior and middle managers, and experts in the health sector, such as the Ministry of Health and Medical Education, universities of medical sciences, health services, and the health network, and people with practical experience in setting up temporary hospitals. The participants were selected through the purposive sampling and then included in the study.
Data collection
In phase 1, all published documents regarding makeshift hospitals and disaster management were extracted without any time limitation. To design the search strategy, the “AND/OR” operators were used (Table 1).

Official documents of leading organizations intervening in disaster management or makeshift hospital establishments were also searched and analyzed. All records were collected and analyzed in 2022.
In the second stage, the fact sheet and management structure of the makeshift hospital are designed for validation, which is the result of the findings of the first stage of the research, and to reach the final model, the expert meeting method will be used with a qualitative approach. In this phase, the final structure is presented according to the opinions of the experts and experts involved. At the beginning of the meeting, explanations of the study objectives were given, after which the participants were asked to express their opinions on the factors extracted from the study’s first phase.
Data analysis
In this study, two researchers analyzed all documents and articles. Related components and ideas were extracted. In the second phase, the research team recorded and listened to the participants’ opinions several times. Necessary corrections were made to the factors. Based on the summary, some factors were removed, and others were added. In the second meeting of the expert panel, the revised draft design was presented and approved by the participants.
Results
Literature review
Based on the analysis of the available articles and documents, 18 articles were included in the study, the majority (85%) of which were published from 2015 to 2020. Most of the articles (43%) were done by content analysis method 40% of the documents were upstream documents, and the rest were articles. Most of these articles described the hospital’s incident command system and the staff and roles involved in its management. These articles mentioned the presence of the director, safety consultant, public relations consultant, operation, planning, and support unit. Table 2 describes the findings of this step.

Expert panel
Based on the findings of the first stage, a general diagram of the chain of command of the makeshift hospital was designed. In the panel of experts, which was formed with experts in the hospital and disaster management (the demographic information of the participants is shown in Table 3), the management framework of the makeshift hospital and the description of the duties of different units were finalized.

Considering the limited resources in developing countries and the importance of managing resources (financial, human, equipment) and improving the quality of health services, developing an administration construction, implementing operations, and operational fact sheets will be helpful. The makeshift health system hospital can be operated in the shortest possible time. This study explained the operational construction of a makeshift hospital as follows. The construction intended for makeshift hospital is displayed in Figure 1.
 The administrative and operational construction of the makeshift hospital is taken from the hospital incident command system. Utilizing the hospital incident command system can create preparedness in the face of disasters, constructive management in disasters, and disaster management strategies. The preparation of the makeshift hospital in pre-crisis conditions will be increased based on various components, such as command, communication, security, safety, planning, and operations. Depending on the type of services and the activation time of the makeshift hospital, the presence of the head of the makeshift center and a management group consisting of a liaison officer, a security officer, a coordination officer, a security officer, and a specialist doctor is essential. This is similar to a hospital’s operations control system.
The administrative and operational construction of the makeshift hospital is taken from the hospital incident command system. Utilizing the hospital incident command system can create preparedness in the face of disasters, constructive management in disasters, and disaster management strategies. The preparation of the makeshift hospital in pre-crisis conditions will be increased based on various components, such as command, communication, security, safety, planning, and operations. Depending on the type of services and the activation time of the makeshift hospital, the presence of the head of the makeshift center and a management group consisting of a liaison officer, a security officer, a coordination officer, a security officer, and a specialist doctor is essential. This is similar to a hospital’s operations control system.
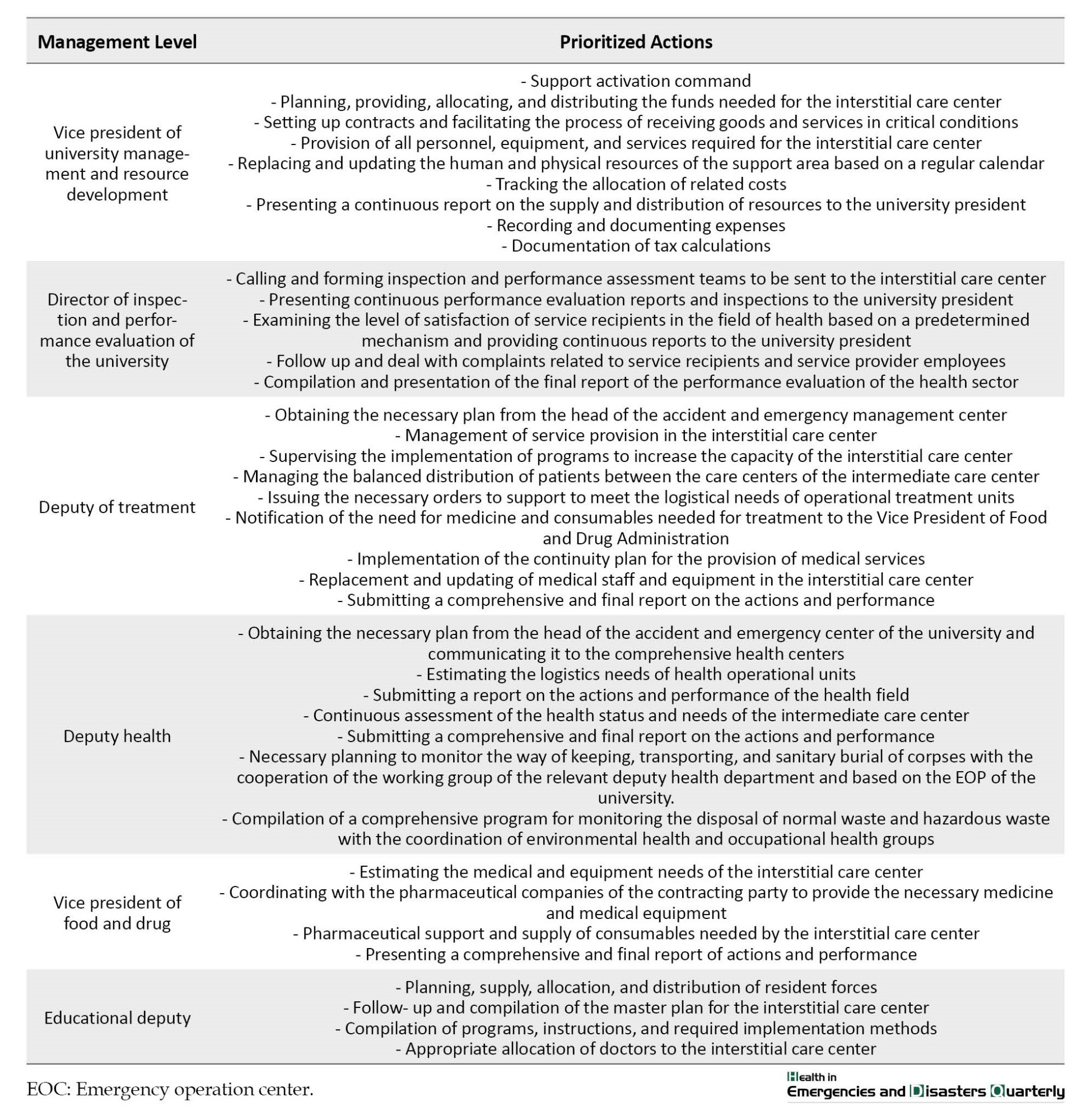
In addition to the general structure, for each position, the description of duties, hierarchy of responsibility, qualification conditions, training, operational history, preparation, and physical health have been explained, which can be seen in Table 4.

Discussion
Considering the limited resources in developing countries and the importance of managing resources (financial, human, equipment) and improving the quality of health services, it will be helpful to formulate a management structure and implement operational worksheets in the least possible time. This study extracted two executive documents named the fact sheet and operational structure of makeshift hospitals.
All the staff of the makeshift hospital should be familiar with their duties; therefore, changing the attitude of staff through training and effective operational exercises, creating required drills, and the time interval between the occurrence of incidents and disasters and epidemics and the establishment of the makeshift hospital will be minimized [12].
The hospital incident command system is a flexible and applicable model in all hospitals [13]. This principle also applies to the construction of temporary hospitals. It is the only active operational unit among the four executive units in the hospital’s operational control system, and the support and financial management units have also been combined. As indicated by a similar guideline, the operational unit of the makeshift hospital construction includes sub-branches of nursing services, such as nurses who provide services, infection control, paramedics, education and health promotion [14], and medical services (emergency medicine and infectious/internal medicine specialist) and mental health. The specialist doctor will change based on the incident’s type, severity, and extent and patients’ need for health services.
The support/administrative-financial unit also includes the manager’s sub-branches of employees’ attendance and absence, admission, discharge and archiving, medical equipment expert, cost and resources manager, services, environmental health expert, and nutritional health expert. All of these units will be removed or activated according to the mission and activity level of the makeshift hospital and at the manager’s discretion.
As mentioned in the study by Dehghani et al., safety and infection control lead to the safety of makeshift hospitals [15]. In this study, the presence of the safety officer and the infection control nurse are among the main elements of the makeshift hospital management structure.
In addition to the general construction, the description of assignments, hierarchy of responsibility, qualification conditions, educational history, operational history, preparation, and physical health have been explained for each position. The clarity of these indicators will reduce the parallel work and chaos in providing services and lead to integrated management [16]. This construction is planned at the management level of the intermediate health center. However, this center operates under the supervision of the University of Medical Sciences and Health Services. Furthermore, these centers are similarly associated with other hospitals and medical centers [17]. This administrative construction can be used to manage emergency military expedients for optimal use of resources and infrastructure.
Conclusion
The preparedness of a temporary hospital acts as a mediator, communicator, and exchange of resources between organizations and healthcare facilities. The existence of a command and administrative structure with a description of specific tasks and an explanation of how to communicate and coordinate between the management and other departments of health centers. By interacting with other collaborating and supporting organizations, the quality of services is improved, and the mortality rate of patients is reduced. The use of command and management construction improves decision-making in critical situations, which increases the need for quarantine, the need to care for large numbers of injured, the speed of decision-making, and the adoption of critical decisions in golden times during epidemics.
Study limitations
Since most of the incident command system was designed and implemented for hospitals, the structure and information sheet for health centers in this study were designed through qualitative studies and document review.
Ethical Considerations
Compliance with ethical guidelines
The present research is a part of choosing the best place to set up a makeshift hospital using a genetic algorithm in Tehran, Iran, emphasizing disaster management and epidemics, which the Ethics Committee of Iran University of Medical Sciences approved (Code: IR.IUMS.REC.1401.807).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, data collection, study design, analysis and interpretation of results: Zahra Eskandari and Arezoo Dehghani; Draft manuscript preparation: Zahra Eskandari; Review and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank all authors whose articles were used in this study and the experts who participated in this research.
References
Epidemics are threats to communities and their health. Epidemics have deeply affected societies throughout history and drastically changed the economic, political, and social aspects of human civilization. Epidemics and outbreaks, such as COVID-19, irreparably impact psychological, social, and economic aspects and change the health service delivery system. Since epidemics are considered a threat to humans, their management is critical [1].
The COVID-19 infection was detected in December 2019 in Wuhan, China, with a high capacity to spread from one person to another quickly. It immediately spread worldwide [2] and was pronounced a critical public health concern by the World Health Organization (WHO) [3]. Iran is experiencing the widespread ongoing transmission of COVID-19 and is one of the level III warning countries with a total of 7 562 610 COVID-19 cases and 144 727 deaths (January 15, 2023, 17:49 GMT) [4].
After detecting COVID-19 and the first case on February 29, 2019, countries faced a short-term increase in inpatients. As one of the challenges for the healthcare system, health authorities were forced to plan and set up temporary hospital hotspots to provide care to patients and healthcare services. A total of 27 000 beds with suitable logistics and treatment systems were available in 300 areas [5]. The preparedness of makeshift hospitals for management, planning, execution, construction incidents, disasters, and epidemics is fundamental to providing appropriate and timely health services [6].
These centers can accept people who were not hospitalized; however, they need to be isolated and under care, and this possibility is unavailable to them at home [7]. Various services, such as medical, pharmaceuticals, nutrition, personal hygiene, education, health promotion services, mental health, and spiritual counseling, were offered to all patients in makeshift hospitals [8].
One of the practical components of managing medical centers in incidents and disasters is the presence of standard operating procedures and incident command systems [9].
Using globally recognized strategies to manage the hospital emergency management system can help improve the quality of healthcare services [10]. In makeshift hospitals, there is a need to plan an incident command system and describe the organizational obligations to respond appropriately and timely [11]. These documents are not specific regarding the features and type of services in makeshift hospitals. Considering that all countries in incidents, disasters, and epidemics require the establishment of makeshift hospitals, this study plans for an eligible and appropriate organizational construction to provide services an executive and operational plan to manage makeshift hospitals in epidemics, disasters, and incidents.
Materials and Methods
Study design
This was a cross-sectional descriptive-analytical study in two phases of review and Delphi studies to develop a public fact sheet guide and the construction of the makeshift hospitals.
In the first phase of the research, the required data was extracted by exploring the sources and texts of various documents regarding the makeshift hospital and the management of the diseases of the COVID-19 epidemic. The final records were analyzed.
In the second phase, the expert panel method was used to design the construction of the makeshift hospital.
Study participants
The participants consisted of professionals, policymakers, senior and middle managers, and experts in the health sector, such as the Ministry of Health and Medical Education, universities of medical sciences, health services, and the health network, and people with practical experience in setting up temporary hospitals. The participants were selected through the purposive sampling and then included in the study.
Data collection
In phase 1, all published documents regarding makeshift hospitals and disaster management were extracted without any time limitation. To design the search strategy, the “AND/OR” operators were used (Table 1).
Official documents of leading organizations intervening in disaster management or makeshift hospital establishments were also searched and analyzed. All records were collected and analyzed in 2022.
In the second stage, the fact sheet and management structure of the makeshift hospital are designed for validation, which is the result of the findings of the first stage of the research, and to reach the final model, the expert meeting method will be used with a qualitative approach. In this phase, the final structure is presented according to the opinions of the experts and experts involved. At the beginning of the meeting, explanations of the study objectives were given, after which the participants were asked to express their opinions on the factors extracted from the study’s first phase.
Data analysis
In this study, two researchers analyzed all documents and articles. Related components and ideas were extracted. In the second phase, the research team recorded and listened to the participants’ opinions several times. Necessary corrections were made to the factors. Based on the summary, some factors were removed, and others were added. In the second meeting of the expert panel, the revised draft design was presented and approved by the participants.
Results
Literature review
Based on the analysis of the available articles and documents, 18 articles were included in the study, the majority (85%) of which were published from 2015 to 2020. Most of the articles (43%) were done by content analysis method 40% of the documents were upstream documents, and the rest were articles. Most of these articles described the hospital’s incident command system and the staff and roles involved in its management. These articles mentioned the presence of the director, safety consultant, public relations consultant, operation, planning, and support unit. Table 2 describes the findings of this step.
Expert panel
Based on the findings of the first stage, a general diagram of the chain of command of the makeshift hospital was designed. In the panel of experts, which was formed with experts in the hospital and disaster management (the demographic information of the participants is shown in Table 3), the management framework of the makeshift hospital and the description of the duties of different units were finalized.
Considering the limited resources in developing countries and the importance of managing resources (financial, human, equipment) and improving the quality of health services, developing an administration construction, implementing operations, and operational fact sheets will be helpful. The makeshift health system hospital can be operated in the shortest possible time. This study explained the operational construction of a makeshift hospital as follows. The construction intended for makeshift hospital is displayed in Figure 1.
In addition to the general structure, for each position, the description of duties, hierarchy of responsibility, qualification conditions, training, operational history, preparation, and physical health have been explained, which can be seen in Table 4.
Discussion
Considering the limited resources in developing countries and the importance of managing resources (financial, human, equipment) and improving the quality of health services, it will be helpful to formulate a management structure and implement operational worksheets in the least possible time. This study extracted two executive documents named the fact sheet and operational structure of makeshift hospitals.
All the staff of the makeshift hospital should be familiar with their duties; therefore, changing the attitude of staff through training and effective operational exercises, creating required drills, and the time interval between the occurrence of incidents and disasters and epidemics and the establishment of the makeshift hospital will be minimized [12].
The hospital incident command system is a flexible and applicable model in all hospitals [13]. This principle also applies to the construction of temporary hospitals. It is the only active operational unit among the four executive units in the hospital’s operational control system, and the support and financial management units have also been combined. As indicated by a similar guideline, the operational unit of the makeshift hospital construction includes sub-branches of nursing services, such as nurses who provide services, infection control, paramedics, education and health promotion [14], and medical services (emergency medicine and infectious/internal medicine specialist) and mental health. The specialist doctor will change based on the incident’s type, severity, and extent and patients’ need for health services.
The support/administrative-financial unit also includes the manager’s sub-branches of employees’ attendance and absence, admission, discharge and archiving, medical equipment expert, cost and resources manager, services, environmental health expert, and nutritional health expert. All of these units will be removed or activated according to the mission and activity level of the makeshift hospital and at the manager’s discretion.
As mentioned in the study by Dehghani et al., safety and infection control lead to the safety of makeshift hospitals [15]. In this study, the presence of the safety officer and the infection control nurse are among the main elements of the makeshift hospital management structure.
In addition to the general construction, the description of assignments, hierarchy of responsibility, qualification conditions, educational history, operational history, preparation, and physical health have been explained for each position. The clarity of these indicators will reduce the parallel work and chaos in providing services and lead to integrated management [16]. This construction is planned at the management level of the intermediate health center. However, this center operates under the supervision of the University of Medical Sciences and Health Services. Furthermore, these centers are similarly associated with other hospitals and medical centers [17]. This administrative construction can be used to manage emergency military expedients for optimal use of resources and infrastructure.
Conclusion
The preparedness of a temporary hospital acts as a mediator, communicator, and exchange of resources between organizations and healthcare facilities. The existence of a command and administrative structure with a description of specific tasks and an explanation of how to communicate and coordinate between the management and other departments of health centers. By interacting with other collaborating and supporting organizations, the quality of services is improved, and the mortality rate of patients is reduced. The use of command and management construction improves decision-making in critical situations, which increases the need for quarantine, the need to care for large numbers of injured, the speed of decision-making, and the adoption of critical decisions in golden times during epidemics.
Study limitations
Since most of the incident command system was designed and implemented for hospitals, the structure and information sheet for health centers in this study were designed through qualitative studies and document review.
Ethical Considerations
Compliance with ethical guidelines
The present research is a part of choosing the best place to set up a makeshift hospital using a genetic algorithm in Tehran, Iran, emphasizing disaster management and epidemics, which the Ethics Committee of Iran University of Medical Sciences approved (Code: IR.IUMS.REC.1401.807).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, data collection, study design, analysis and interpretation of results: Zahra Eskandari and Arezoo Dehghani; Draft manuscript preparation: Zahra Eskandari; Review and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank all authors whose articles were used in this study and the experts who participated in this research.
References
- Huremović D. Brief history of pandemics (pandemics throughout history). In: Huremović D, editor. Psychiatry of pandemics. Cham: Springer; 2019. [DOI:10.1007/978-3-030-15346-5_2]
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020; 323(13):1239-42. [DOI:10.1001/jama.2020.2648] [PMID]
- Peeri NC, Shrestha N, Rahman MS, Zaki R, Tan Z, Bibi S, et al. The SARS, MERS and novel Coronavirus (COVID-19) epidemics, the newest and biggest global health threats: What lessons have we learned? International Journal of Epidemiology. 2020; 49(3):717-26. [DOI:10.1093/ije/dyaa033] [PMID]
- Anbari E, Yarmohammadian MH, Isfahani MN. From investigation of hospital protocols and guidelines to designing a generic protocol for responding to chemical, biological, radiological, and nuclear incidents. International Journal of Health System and Disaster Management. 2015; 3(4):195-9. [DOI:10.4103/2347-9019.162553]
- IRIB News Agency. Patients with COVID-19 are quarantined in Fangcang Hospital [internet]. 2020. [Link]
- Bazyar J, Pourvakhshoori N, Safarpour H, Farrokhi M, Khankeh HR, Daliri S, et al. Hospital disaster preparedness in Iran: A systematic review and meta-analysis. Iranian Journal of Public Health. 2020; 49(5):837-50. [DOI:10.18502/ijph.v49i5.3201] [PMID]
- Dehghani A, Ghomian Z. Safety assessment of the largest Fangcang Hospital for COVID-19 management in Iran. Trauma Monthly. 2022; 27(Especial Issue (COVID-19 and Emergency Medicine)):18-25. [DOI:10.30491/tm.2021.282998.1282]
- Kassaeian S, Gohari A, Masoumi G, Ghomian Z, Dehghani A. Post-hospital discharge strategy for COVID-19 treatment and control: Focus on Fangcang hospitals. Disaster Medicine and Public Health Preparedness. 2022; 16(5):1795-7. [Link]
- Borhannejad Z, Sadat Madah SB, Khankeh HR, Falahi Khoshknab M, Rezasoltani P, Ahmadi S. Effect of hospital incident command system establishment on the preparedness level of Disaster Committee and nursing staff of Imam Ali Hospital, Zarand, Iran, 2010. Health in Emergencies and Disasters. 2019; 4(2):101-8. [DOI:10.32598/hdq.4.2.101]
- Abbasi S, Shooshtari S, Tofighi S. Developing a conceptual model of the Hospital Incident Command System (HICS) via quality improvement models in Iran. Journal of Research in Medical and Dental Science. 2018; 6(2):257-68. [DOI:10.5455/jrmds.20186240]
- Dehghani A, Ghomian Z, Eskandari Z. Design and psychometrics of risk assessment tool for makeshift hospitals: Focusing on pandemics. Heliyon. 2023; 9(4):e14973. [DOI:10.1016/j.heliyon.2023.e14973] [PMID]
- Shooshtari S, Tofighi S, Abbasi S. Benefits, barriers, and limitations on the use of hospital incident command system. Journal of Research in Medical Sciences: The Official Journal of Isfahan University of Medical Sciences. 2017; 22:36. [DOI:10.4103/1735-1995.202146] [PMID]
- Rafieepour A, Masoumi G, Dehghani A. Health responses during the COVID-19 pandemic: An international strategy and experience analysis. Health in Emergencies and Disasters Quarterly. 2021; 6(3):147-60. [DOI:10.32598/hdq.6.3.310.1]
- Hashempour R, Hosseinpour Ghahremanlou H, Etemadi S, Poursadeghiyan M. The relationship between quality of work life and organizational commitment of Iranian emergency nurses. Health in Emergencies and Disasters Quarterly. 2018; 4(1):49-54. [DOI:10.32598/hdq.4.1.49]
- Dehghani A, Ghomian Z, Eskandari Z. Design and psychometrics of risk assessment tool for makeshift hospitals: Focusing on pandemics. Heliyon. 2023; 9(4):e14973. [DOI:10.1016/j.heliyon.2023.e14973] [PMID]
- Fletcher B, Knight A, Pockrus B, Wain MJ, Lehman-Huskamp K. Hospital incident command: First responders or receiving centers? American Journal of Disaster Medicine. 2016; 11(2):125-30. [DOI:10.5055/ajdm.2016.0231] [PMID]
- Persoff J, Patel H, Singh S, Ehrenfeucht C, Kutner J, Little C, et al. Expanding the hospital incident command system with a physician-centric role during a pandemic: The role of the physician clinical support supervisor. Journal of Hospital Administration. 2020; 9(3):7-10. [DOI:10.5430/jha.v9n3p7]
Type of Study: Research |
Subject:
General
Received: 2023/01/16 | Accepted: 2023/10/8 | Published: 2024/01/1
Received: 2023/01/16 | Accepted: 2023/10/8 | Published: 2024/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Health in Emergencies and Disasters Quarterly
Health in Emergencies & Disasters Research Center, University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave, Tehran, Iran.
Journal Tel: +9821 71732816 (2816)
Publisher Tel: +9821 4535 5555 - 4535 5000
