

Volume 8, Issue 1 (Autumn 2022)
Health in Emergencies and Disasters Quarterly 2022, 8(1): 65-76 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mueller-Haugk S, Stueck M. Relationship of Anxiety Management Types and Health-related Variables of People During Lockdown in a German Sample. Health in Emergencies and Disasters Quarterly 2022; 8 (1) :65-76
URL: http://hdq.uswr.ac.ir/article-1-490-en.html
URL: http://hdq.uswr.ac.ir/article-1-490-en.html



1- International Biocentric Research Academy (IBRA), Leipzig, Germnany.
Keywords: Pandemic management theory, Health psychology, COVID-19 and psyche, Biocentric health theory, Anxiety, Stress and coping, Disaster management, Biocentric-approach
Full-Text [PDF 790 kb]
(305 Downloads)
| Abstract (HTML) (1109 Views)
Full-Text: (354 Views)
1. Introduction
Central to the present study is the examination of anxiety coping types according to the “repressor-sensitizer construct” [1, 2]. This construct examines two variables, trait anxiety and social desirability, which, when combined, yield four cognitive styles of anxiety coping traits (Table 1).
.jpg)
One measures a person’s anxiety as an enduring personality trait (trait anxiety), and the other measures one’s tendency to defensively avoid unpleasant emotions in terms of social desirability [3]. The latter is typically measured using a “social desirability” scale, as individuals who are strongly motivated to behave in socially desirable ways are thought to cognitively try to ward off their anxiety (defensive avoiders). That is, they describe less anxiety because anxiety tends to be something that is socially undesirable.
Anxiety coping types can be described as follows:
- Individuals with low trait anxiety and low scores in defensiveness are thereby referred to as non-defensive. It is characterized by their high tolerance of emotional arousal and feelings of uncertainty. Depending on the situation, they take a closer look at threatening information or ignore it. It is a flexible, situation-adaptive mode.
- Repressors show low anxiety (exhibit low anxiety scores) and high levels of fear denial (high social desirability scores). Repressors suffer from low tolerance to arousal and high tolerance to uncertainty. They are classified as low vigilant, meaning there is no absorption and processing of threatening information. It is cognitive avoidance (turning attention away from threatening information), i.e. through consistent stimulus avoidance, they escape emotionally arousing situations. This behavior can be classified as “consistent avoidance” [4]. The defender ‘sees’ less and ‘talks’ less about it. It is a rigidly avoidant mode of stimulus processing.
- Sensitizers show much anxiety (exhibit high anxiety scores) and only a low tendency to deny anxiety (low social desirability scores). This configuration of high anxiety and low defensiveness has psychological implications. Bounds on tolerance to uncertainty are low, whereas those to arousal are high. Their behavior can be described as highly consistently monitoring (vigilant). That is, sensitizers, to control their situation, form a kind of cognitive expectancy template to be prepared for all threats. They are armed against the accompanying emotional arousal, and permanent vigilance keeps their behavior stable. It is a strict monitoring mode.
- The fourth group, with high anxiety and high defensiveness scores, can be described as highly anxious individuals with a dysfunctional or inconsistent anxiety coping pattern. Their threshold and tolerance are markedly low with respect to both uncertainty and emotional arousal. Since at least one of the two ambivalent dimensions, or both, are high (arousal by confronting the stimulus and or uncertainty by not confronting it), the individuals are in a predicament. This condition results in unstable behavior. The counterpart to the highly anxious individuals in this construct is the non-defensive individuals.
The studies on the four types of anxiety management have a long and heterogenous tradition. It has been shown that the displacement perspective is successful in the short term, in contrast to the sensitization perspective [4].
These studies cannot be presented in more depth within the scope of this article due to lack of space. However, some studies are interesting with regard to our question concerning the relationship between age and psychological health variables in the context of the COVID-19 event.
In the study by Bidzan-Bluma et al. [5], it is shown that people aged 60 years and older have significantly less problematic anxiety coping styles in contrast to middle age and young age [5]. These results were confirmed by another sample from Portugal [6]. Sensitizers, repressors, and highly anxious can be grouped as problematic anxiety management styles, as proposed in Stueck’s pandemic management theory [7].
There is very little research on the relationship between anxiety management types and psychological health variables related to COVID-19 occurrence. Therefore, in addition to the anxiety coping types, different variables were investigated by “repressor-sensitizer” (R-S) construct analysis (Table 2).
.jpg)
In connection with the anxiety coping types, the coherence experience plays a significant role. Coherence can be defined as “a global orientation that expresses the extent to which one has a generalized, enduring, and dynamic sense of confidence that one’s internal and external environment is predictable and that there is a high probability that things will turn out as one might reasonably expect” [8]. The coherence model positively correlates to various health-related parameters, such as wellbeing and mental health. Likewise, there is a connection between the coherence experience and physiological health parameters here, however, not so clear and intensive. It is assumed that coherence indirectly mediates, and physical health is expressed through actual coping behavior in stressful situations [9].
A second variable related to the anxiety coping types is the threat perception of the subjects. It also plays an important role in evaluating the situation [7]. Threat perception is one of the central situation evaluation mechanisms which influence the further development of the situation to a positive or negative stress consequence. Thereby the threat perception is attributed to the consequence of stress, fear, and hypersensitivity [7].
The study investigated the following questions:
1. What is the frequency distribution of the anxiety management types in the entire sample?
2. Are there age-specific differences in the distribution of the anxiety management types?
3. Do the four different anxiety management types differ with regard to selected health-related variables?
2. Materials and Methods
The present study was methodologically implemented as follows.
Schedule
The study started 10 days after the corona-induced lockdown in Germany, i.e. March 27, 2020. The lockdown in Germany was decided on March 16, 2020, implemented on March 22, 2020, and lasted for 7 weeks. During this period of intensive restriction of public life, further process surveys were conducted but did not play a role in this article.
Sampling plan
The sample consisted of 325 subjects with an average age of 46 years (SD=12.5). Five age groups were considered.
Variable plan and methods of data collection for questions 1, 2, and 3
In the present study, the following health-related variables and anxiety coping types were collected using the measurement procedures presented below.
Methods of data analysis for questions 1 and 2
In this study, among other things, the anxiety coping types were analyzed according to Krohne’s multidimensional R-S construct [2]. The analysis of these anxiety coping types was conducted using the statistical processing of two standardized scales: the Anxiety Inventory (STAI) [12] and the Social Desirability questionnaire [13]. Then, the anxiety types were classified using t-value transformation and Z value analysis.
Results were presented as descriptive statistics (percentage frequency distributions.
Methods of data analysis for research question 3
The Kruskal-Wallis nonparametric test was used for the comparative analysis, and pairwise mean comparisons were made using the Dunn-Bonferroni post hoc test. The
effect size of the significances was calculated using Cohen’s r [14]. According to Cohen, the intervals for evaluating the effect strength are as follows: r=0.1 (low), r=0.3 (medium), and r=0.5 (strong).
3. Results
Results for question 1
Regarding the frequency distribution of anxiety coping types, the problematic anxiety coping types (sensitizer, repressive, and highly anxious) are represented by 54.2% occurrence. The flexible-adaptive type (non-Defensive), which has acceptable adaptability to the anxiety-provoking situation, is prominent with 45.8%. The individual expressions of the 4 anxiety management types are presented in Table 3.
.jpg)
Results for question 2
Concerning age specificity, the frequency distributions are as follows (Table 4).
.jpg)
Again, problematic anxiety coping types increase with age (Table 5 & Figure 1). This increase is shown to be significant in the test (P=0.001).
.jpg)
.jpg)
Results for question 3
The test of normal distribution revealed the presence of a non-normal distribution of samples with respect to the health variables. In this case, the analysis of the distributional differences between the anxiety management types and the selected health variables shows the following results (Table 6).
.jpg)
The effect size was calculated using Cohen’s r (cf. Cohen, 1992).
According to Cohen, the intervals for evaluating the effect strength are as follows: r=0.1 (low), r=0.3 (medium), and r=0.5 (high). However, the effect size describes the direction of the difference, not the intensity of the effect.
For better presentation, the distribution differences of the median per variable are shown in the boxplots below.
The correlation between increased anxiety (anxiety management type sensitizer and highly anxious) and the reduced ability to relax is recognizable. This relationship is evident in the significant differences between the non-problematic anxiety management type “non-defensive” and the problematic anxiety management types “sensitizer” and “highly anxious.” The anxiety coping type “repressor” moves on the non-problematic level, similar to the “non-defensive” type (Figure 2).
.jpg)
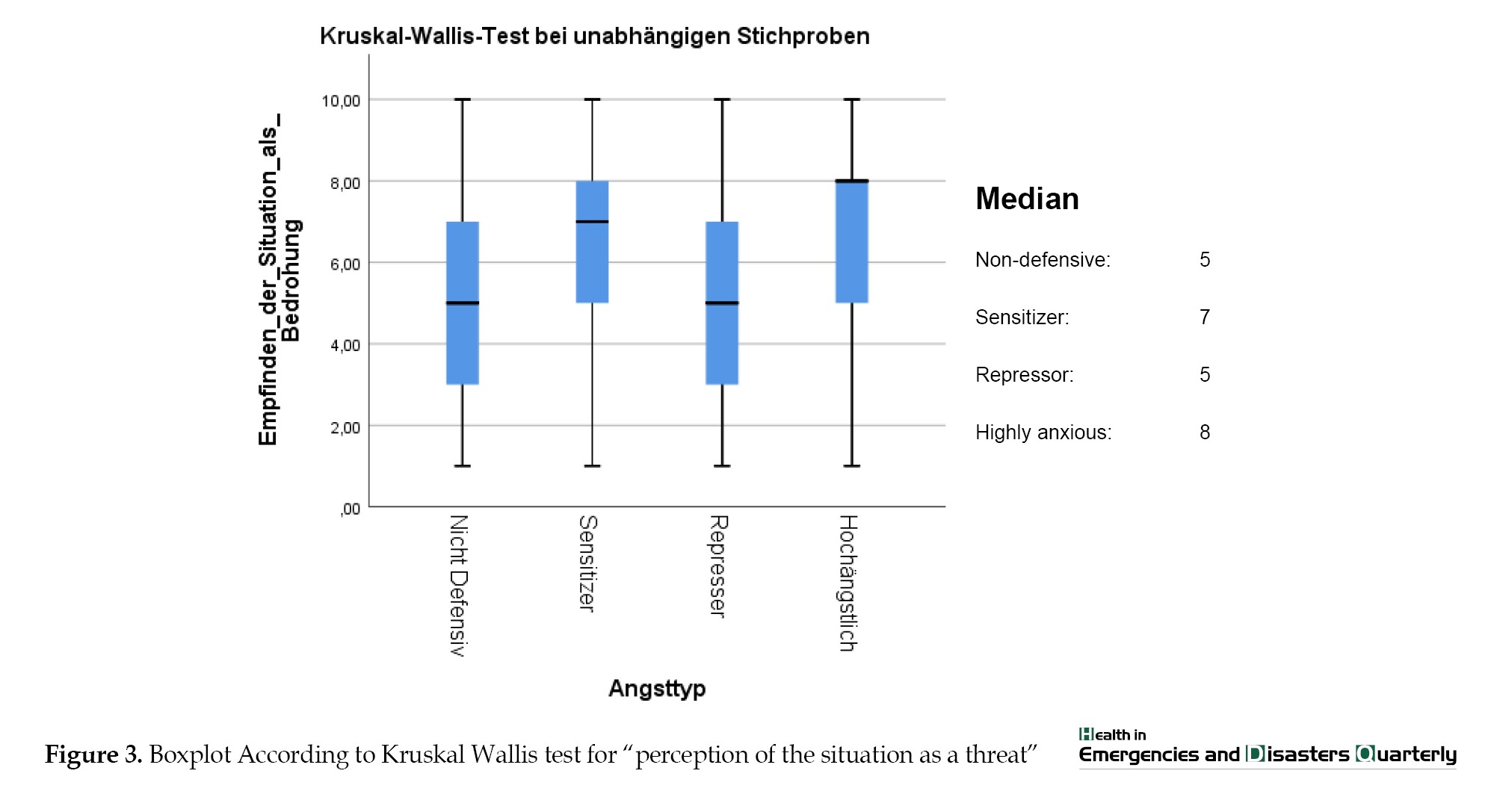
Regarding the threat perception variable, there is a significant difference between the fear coping type “non-defensive” and “sensitizer” and between the “repressor” and “sensitizer” (Figure 3).
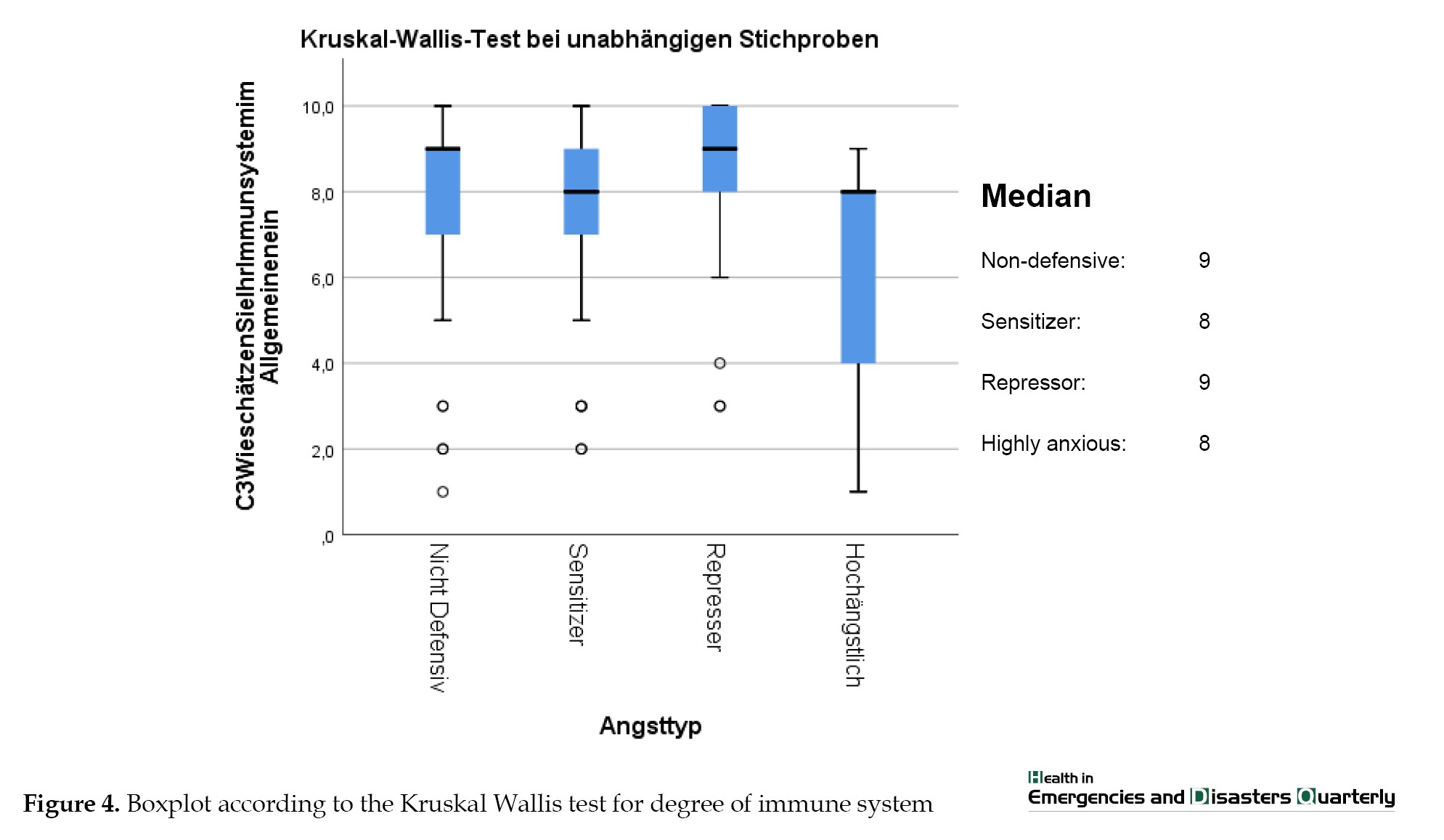
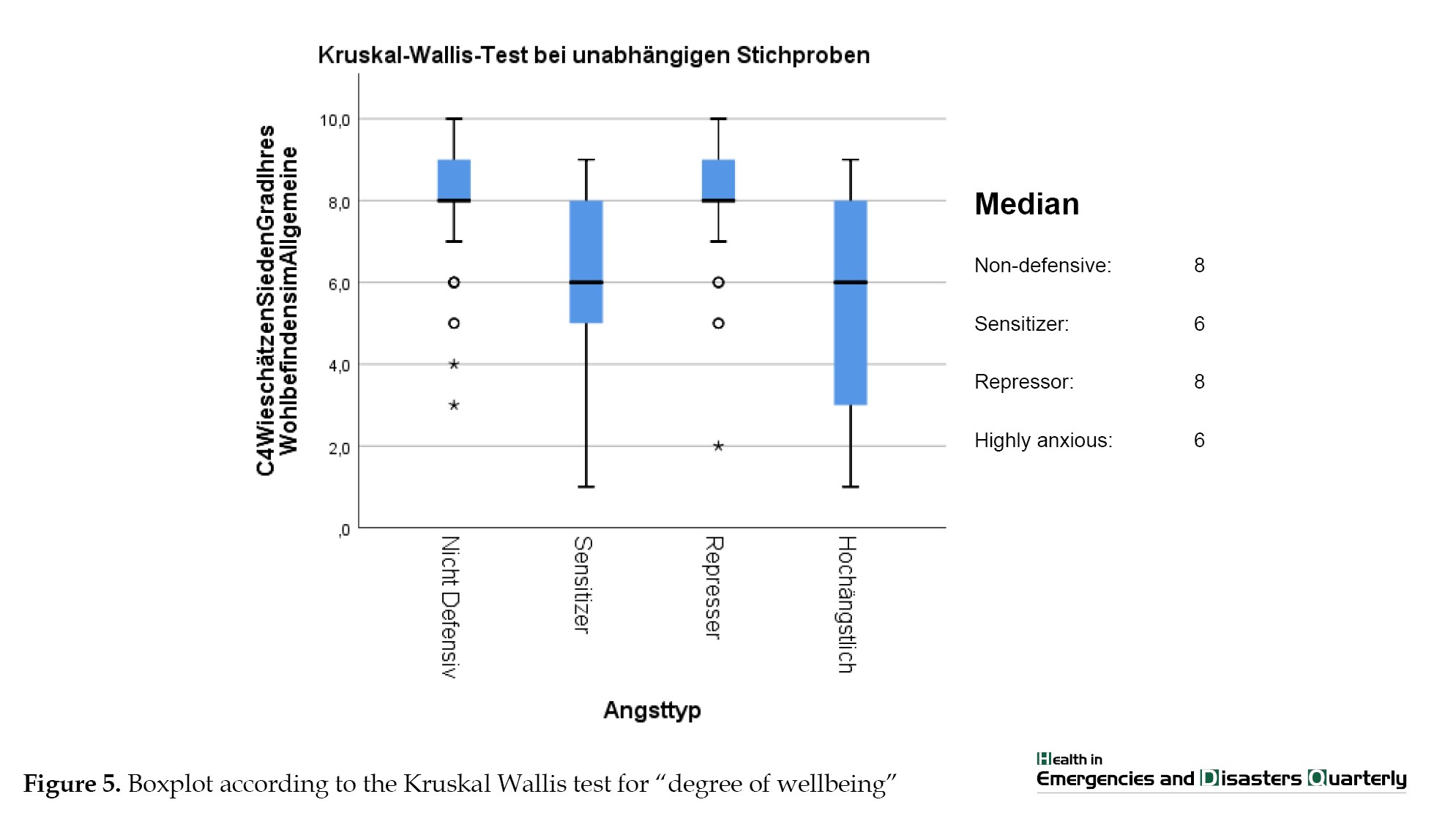
When assessing the functionality of one’s immune system, it becomes clear that the non-defensives and repressors show the same median (9) and report a very good function of their immune system. In comparison, the sensitizers and highly anxious show a lower median score (8). Significant differences were found between the repressor and sensitizers (P=0.000) and the repressor and highly anxious (P=0.001). In addition, significant differences were also found between the non-defensive and sensitizer (P=0.036) and between the non-defensive and highly anxious (P=0.023) (Figure 4, 5).
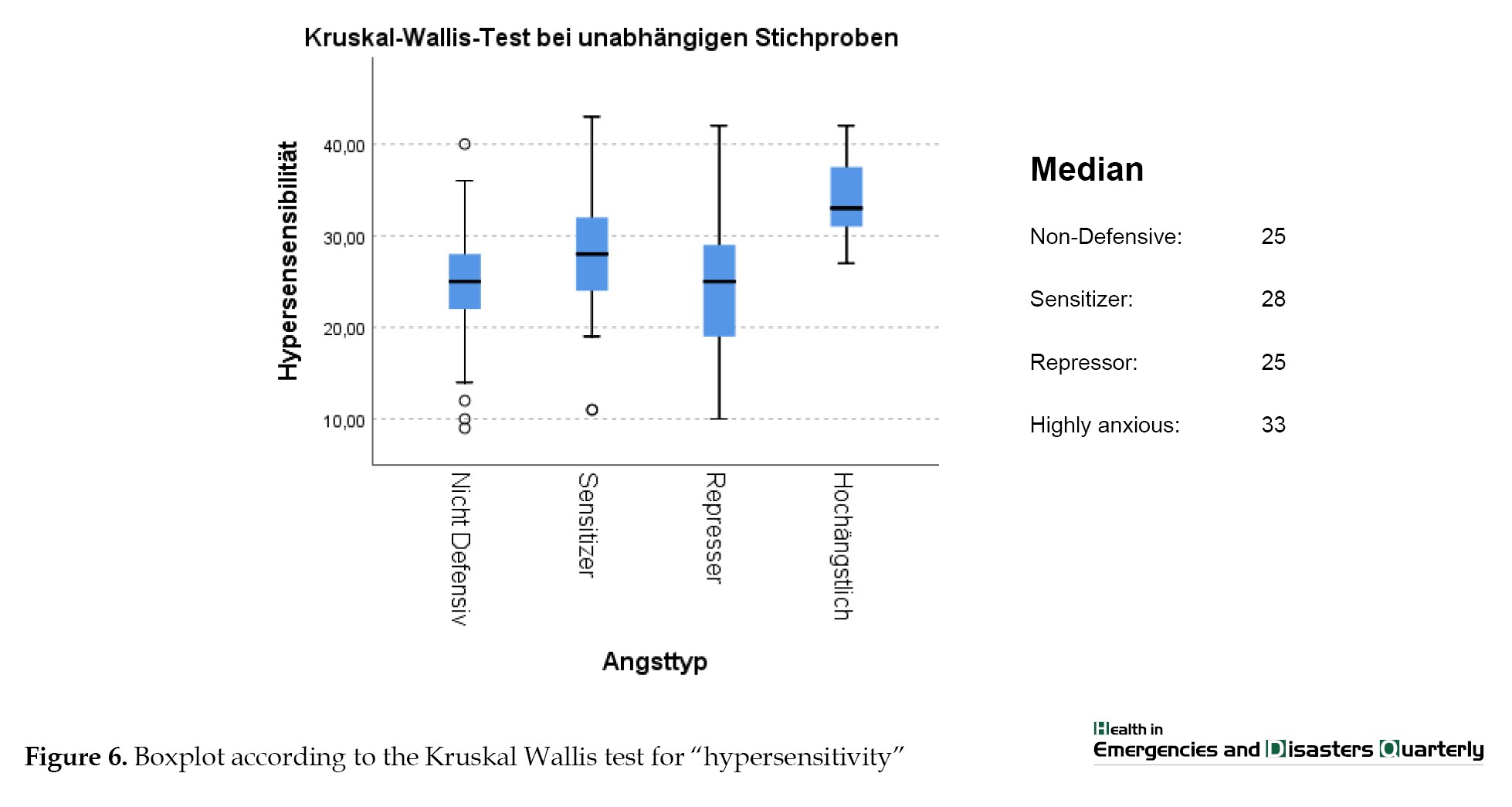
Regarding the hypersensitivity results, the highest effect is in the significant increase of hypersensitivity in the highly anxious compared to all other anxiety management types. The repressor shows the highest standard deviation, i.e. the values fluctuate most extremely around the median (Figure 6).
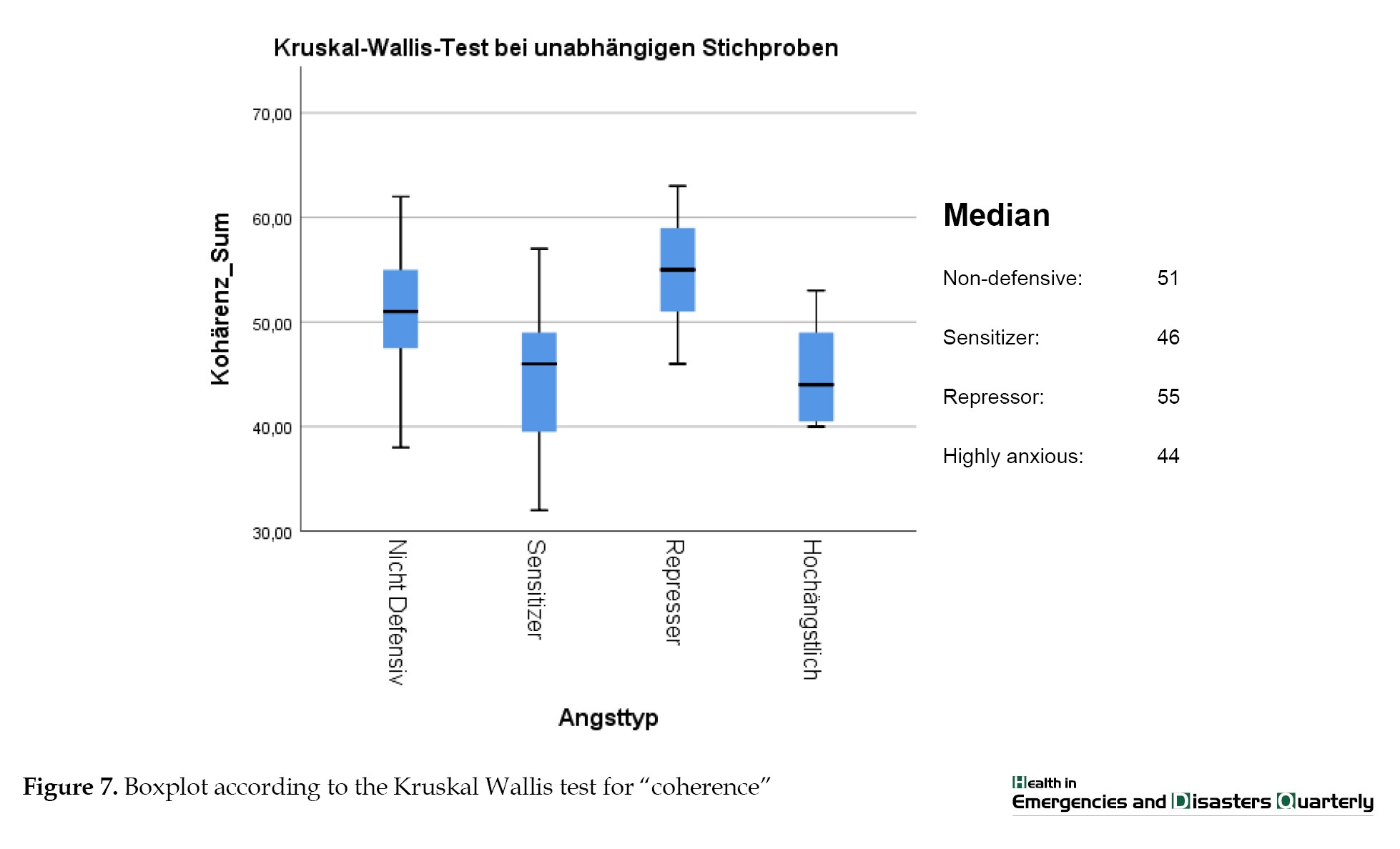
The highly anxious and the sensitizers show the lowest median values with regard to the coherence experience compared to the non-defensive and the repressor. It is interesting in this context that the repressor shows the highest median (55) followed by the non-defensive (51). Thus, the repressor stands out significantly from all other anxiety coping types (P≤0.005) (Figure 7).
4. Discussion
Discussion on question 1
Comparing the problematic to non-problematic anxiety coping styles (Table 1), the problematic ones (sensitizer, repressor, and highly anxious) are represented with 54.2% frequency of occurrence in contrast to 45.8% non-problematic anxiety coping types. When the individual types are compared, repressors have the highest frequency of occurrence, with 28.9%. According to Byrne and Krohne’s theory, this anxiety coping type is characterized by denying anxiety and thus exhibiting low anxiety. In the short term, this is an acceptable coping strategy, but in the longer term, it leads to psychological abnormalities [4]. In a recent study by Stueck 7], the repressors were those whose perceptions were significantly more externally oriented and who were more likely to exhibit externalized behavior in terms of behavior (e.g. participation in demonstrations). The second problematic anxiety coping strategy, sensitizers, ranked second in the present study’s ranking with 20.0%. This anxiety coping type is characterized by low social desirability and high anxiety. They feel high anxiety and cannot deny or cope with it. In the study by Stueck [7], there were correlations with more internalized behaviors (e.g. increased dreaming, depressive reactions, and psychosomatic reactions). The highly anxious anxiety coping types are a relatively insignificant subsample in the present study in terms of problematic coping styles, with a 5.3% frequency. The healthy anxiety coping style (non-defensive) ranks first in terms of individual types. This means that about 30% of the studied samples had low social desirability and also low anxiety at the time of measurement when the study took place (3 weeks after the lockdown). It would be interesting to investigate how this ranking of anxiety management types changes over the course of the Corona pandemic.
Discussion on question 2
Are there age-specific differences in the distribution of anxiety management types?
The indicated significant distribution difference with regard to the age-specific distribution differences of the anxiety coping types (the Chi-square test P=0.001) can be attributed, above all, to frequency differences in the older age groups. Here, the highest expression of problematic anxiety coping patterns is shown in the 50 to 59 age group. Those in the young age group (up to 29 years) and the middle age group (40-49 years) are in second place in the ranking. The present study found that people aged 60 years and older are less likely to show problematic anxiety coping styles. This finding is consistent with work on age-specific issues during a similar survey period as the present study [7]. In this study, it is found that the older population aged 60 years and above had significantly less TRAIT anxiety, as well as less difficulty relaxing, higher life satisfaction, and also increased well-being during the pandemic period, in contrast to the middle-aged and young. They also felt less threatened by the Corona virus (ibid). These findings were confirmed by a Portuguese sample. The reasons given for this were greater experience with unforeseen situations, less existential pressure on this age group and greater ability to cope with internal states of tension [6].
Discussion on question 3
Here it becomes apparent that the “repressor” represents a successful coping strategy in the short term. The low dispersion of the values for the “repressor” type is also striking, which indicates that the constellation between fear denial and fear perception describes the fear coping type well. However, the repressor shows fewer health complaints and has a low inward orientation and a tendency to cope with emotions through external activities. Repressors in this study were more likely to attend political demonstrations and express opinions [7]. How effective this coping strategy can be in the long term and if there are any other negative impacts on their health situation should be clarified with future studies by focusing on the biocentric theory and mechanisms [7].
Ethical Considerations
Compliance with ethical guidelines
This research has been conducted following ethical principles, including the Declaration of Helsinki and the additional requirements. The experiments were undertaken with the informed written consent of each subject and according to the principles mentioned above.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors
Authors' contributions
The both authors equally contributed to preparing this article.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgments
We thank our colleague Jessica Knietzsch for her preparational work in obtaining the health cube questionnaire. We thank also the research group of the project “COVID 19 & Biocentric Disaster Management”.
Central to the present study is the examination of anxiety coping types according to the “repressor-sensitizer construct” [1, 2]. This construct examines two variables, trait anxiety and social desirability, which, when combined, yield four cognitive styles of anxiety coping traits (Table 1).
One measures a person’s anxiety as an enduring personality trait (trait anxiety), and the other measures one’s tendency to defensively avoid unpleasant emotions in terms of social desirability [3]. The latter is typically measured using a “social desirability” scale, as individuals who are strongly motivated to behave in socially desirable ways are thought to cognitively try to ward off their anxiety (defensive avoiders). That is, they describe less anxiety because anxiety tends to be something that is socially undesirable.
Anxiety coping types can be described as follows:
- Individuals with low trait anxiety and low scores in defensiveness are thereby referred to as non-defensive. It is characterized by their high tolerance of emotional arousal and feelings of uncertainty. Depending on the situation, they take a closer look at threatening information or ignore it. It is a flexible, situation-adaptive mode.
- Repressors show low anxiety (exhibit low anxiety scores) and high levels of fear denial (high social desirability scores). Repressors suffer from low tolerance to arousal and high tolerance to uncertainty. They are classified as low vigilant, meaning there is no absorption and processing of threatening information. It is cognitive avoidance (turning attention away from threatening information), i.e. through consistent stimulus avoidance, they escape emotionally arousing situations. This behavior can be classified as “consistent avoidance” [4]. The defender ‘sees’ less and ‘talks’ less about it. It is a rigidly avoidant mode of stimulus processing.
- Sensitizers show much anxiety (exhibit high anxiety scores) and only a low tendency to deny anxiety (low social desirability scores). This configuration of high anxiety and low defensiveness has psychological implications. Bounds on tolerance to uncertainty are low, whereas those to arousal are high. Their behavior can be described as highly consistently monitoring (vigilant). That is, sensitizers, to control their situation, form a kind of cognitive expectancy template to be prepared for all threats. They are armed against the accompanying emotional arousal, and permanent vigilance keeps their behavior stable. It is a strict monitoring mode.
- The fourth group, with high anxiety and high defensiveness scores, can be described as highly anxious individuals with a dysfunctional or inconsistent anxiety coping pattern. Their threshold and tolerance are markedly low with respect to both uncertainty and emotional arousal. Since at least one of the two ambivalent dimensions, or both, are high (arousal by confronting the stimulus and or uncertainty by not confronting it), the individuals are in a predicament. This condition results in unstable behavior. The counterpart to the highly anxious individuals in this construct is the non-defensive individuals.
The studies on the four types of anxiety management have a long and heterogenous tradition. It has been shown that the displacement perspective is successful in the short term, in contrast to the sensitization perspective [4].
These studies cannot be presented in more depth within the scope of this article due to lack of space. However, some studies are interesting with regard to our question concerning the relationship between age and psychological health variables in the context of the COVID-19 event.
In the study by Bidzan-Bluma et al. [5], it is shown that people aged 60 years and older have significantly less problematic anxiety coping styles in contrast to middle age and young age [5]. These results were confirmed by another sample from Portugal [6]. Sensitizers, repressors, and highly anxious can be grouped as problematic anxiety management styles, as proposed in Stueck’s pandemic management theory [7].
There is very little research on the relationship between anxiety management types and psychological health variables related to COVID-19 occurrence. Therefore, in addition to the anxiety coping types, different variables were investigated by “repressor-sensitizer” (R-S) construct analysis (Table 2).
In connection with the anxiety coping types, the coherence experience plays a significant role. Coherence can be defined as “a global orientation that expresses the extent to which one has a generalized, enduring, and dynamic sense of confidence that one’s internal and external environment is predictable and that there is a high probability that things will turn out as one might reasonably expect” [8]. The coherence model positively correlates to various health-related parameters, such as wellbeing and mental health. Likewise, there is a connection between the coherence experience and physiological health parameters here, however, not so clear and intensive. It is assumed that coherence indirectly mediates, and physical health is expressed through actual coping behavior in stressful situations [9].
A second variable related to the anxiety coping types is the threat perception of the subjects. It also plays an important role in evaluating the situation [7]. Threat perception is one of the central situation evaluation mechanisms which influence the further development of the situation to a positive or negative stress consequence. Thereby the threat perception is attributed to the consequence of stress, fear, and hypersensitivity [7].
The study investigated the following questions:
1. What is the frequency distribution of the anxiety management types in the entire sample?
2. Are there age-specific differences in the distribution of the anxiety management types?
3. Do the four different anxiety management types differ with regard to selected health-related variables?
2. Materials and Methods
The present study was methodologically implemented as follows.
Schedule
The study started 10 days after the corona-induced lockdown in Germany, i.e. March 27, 2020. The lockdown in Germany was decided on March 16, 2020, implemented on March 22, 2020, and lasted for 7 weeks. During this period of intensive restriction of public life, further process surveys were conducted but did not play a role in this article.
Sampling plan
The sample consisted of 325 subjects with an average age of 46 years (SD=12.5). Five age groups were considered.
Variable plan and methods of data collection for questions 1, 2, and 3
In the present study, the following health-related variables and anxiety coping types were collected using the measurement procedures presented below.
Methods of data analysis for questions 1 and 2
In this study, among other things, the anxiety coping types were analyzed according to Krohne’s multidimensional R-S construct [2]. The analysis of these anxiety coping types was conducted using the statistical processing of two standardized scales: the Anxiety Inventory (STAI) [12] and the Social Desirability questionnaire [13]. Then, the anxiety types were classified using t-value transformation and Z value analysis.
Results were presented as descriptive statistics (percentage frequency distributions.
Methods of data analysis for research question 3
The Kruskal-Wallis nonparametric test was used for the comparative analysis, and pairwise mean comparisons were made using the Dunn-Bonferroni post hoc test. The
effect size of the significances was calculated using Cohen’s r [14]. According to Cohen, the intervals for evaluating the effect strength are as follows: r=0.1 (low), r=0.3 (medium), and r=0.5 (strong).
3. Results
Results for question 1
Regarding the frequency distribution of anxiety coping types, the problematic anxiety coping types (sensitizer, repressive, and highly anxious) are represented by 54.2% occurrence. The flexible-adaptive type (non-Defensive), which has acceptable adaptability to the anxiety-provoking situation, is prominent with 45.8%. The individual expressions of the 4 anxiety management types are presented in Table 3.
Results for question 2
Concerning age specificity, the frequency distributions are as follows (Table 4).
Again, problematic anxiety coping types increase with age (Table 5 & Figure 1). This increase is shown to be significant in the test (P=0.001).
Results for question 3
The test of normal distribution revealed the presence of a non-normal distribution of samples with respect to the health variables. In this case, the analysis of the distributional differences between the anxiety management types and the selected health variables shows the following results (Table 6).
The effect size was calculated using Cohen’s r (cf. Cohen, 1992).
According to Cohen, the intervals for evaluating the effect strength are as follows: r=0.1 (low), r=0.3 (medium), and r=0.5 (high). However, the effect size describes the direction of the difference, not the intensity of the effect.
For better presentation, the distribution differences of the median per variable are shown in the boxplots below.
The correlation between increased anxiety (anxiety management type sensitizer and highly anxious) and the reduced ability to relax is recognizable. This relationship is evident in the significant differences between the non-problematic anxiety management type “non-defensive” and the problematic anxiety management types “sensitizer” and “highly anxious.” The anxiety coping type “repressor” moves on the non-problematic level, similar to the “non-defensive” type (Figure 2).
Regarding the threat perception variable, there is a significant difference between the fear coping type “non-defensive” and “sensitizer” and between the “repressor” and “sensitizer” (Figure 3).
When assessing the functionality of one’s immune system, it becomes clear that the non-defensives and repressors show the same median (9) and report a very good function of their immune system. In comparison, the sensitizers and highly anxious show a lower median score (8). Significant differences were found between the repressor and sensitizers (P=0.000) and the repressor and highly anxious (P=0.001). In addition, significant differences were also found between the non-defensive and sensitizer (P=0.036) and between the non-defensive and highly anxious (P=0.023) (Figure 4, 5).
Regarding the hypersensitivity results, the highest effect is in the significant increase of hypersensitivity in the highly anxious compared to all other anxiety management types. The repressor shows the highest standard deviation, i.e. the values fluctuate most extremely around the median (Figure 6).
The highly anxious and the sensitizers show the lowest median values with regard to the coherence experience compared to the non-defensive and the repressor. It is interesting in this context that the repressor shows the highest median (55) followed by the non-defensive (51). Thus, the repressor stands out significantly from all other anxiety coping types (P≤0.005) (Figure 7).
4. Discussion
Discussion on question 1
Comparing the problematic to non-problematic anxiety coping styles (Table 1), the problematic ones (sensitizer, repressor, and highly anxious) are represented with 54.2% frequency of occurrence in contrast to 45.8% non-problematic anxiety coping types. When the individual types are compared, repressors have the highest frequency of occurrence, with 28.9%. According to Byrne and Krohne’s theory, this anxiety coping type is characterized by denying anxiety and thus exhibiting low anxiety. In the short term, this is an acceptable coping strategy, but in the longer term, it leads to psychological abnormalities [4]. In a recent study by Stueck 7], the repressors were those whose perceptions were significantly more externally oriented and who were more likely to exhibit externalized behavior in terms of behavior (e.g. participation in demonstrations). The second problematic anxiety coping strategy, sensitizers, ranked second in the present study’s ranking with 20.0%. This anxiety coping type is characterized by low social desirability and high anxiety. They feel high anxiety and cannot deny or cope with it. In the study by Stueck [7], there were correlations with more internalized behaviors (e.g. increased dreaming, depressive reactions, and psychosomatic reactions). The highly anxious anxiety coping types are a relatively insignificant subsample in the present study in terms of problematic coping styles, with a 5.3% frequency. The healthy anxiety coping style (non-defensive) ranks first in terms of individual types. This means that about 30% of the studied samples had low social desirability and also low anxiety at the time of measurement when the study took place (3 weeks after the lockdown). It would be interesting to investigate how this ranking of anxiety management types changes over the course of the Corona pandemic.
Discussion on question 2
Are there age-specific differences in the distribution of anxiety management types?
The indicated significant distribution difference with regard to the age-specific distribution differences of the anxiety coping types (the Chi-square test P=0.001) can be attributed, above all, to frequency differences in the older age groups. Here, the highest expression of problematic anxiety coping patterns is shown in the 50 to 59 age group. Those in the young age group (up to 29 years) and the middle age group (40-49 years) are in second place in the ranking. The present study found that people aged 60 years and older are less likely to show problematic anxiety coping styles. This finding is consistent with work on age-specific issues during a similar survey period as the present study [7]. In this study, it is found that the older population aged 60 years and above had significantly less TRAIT anxiety, as well as less difficulty relaxing, higher life satisfaction, and also increased well-being during the pandemic period, in contrast to the middle-aged and young. They also felt less threatened by the Corona virus (ibid). These findings were confirmed by a Portuguese sample. The reasons given for this were greater experience with unforeseen situations, less existential pressure on this age group and greater ability to cope with internal states of tension [6].
Discussion on question 3
Here it becomes apparent that the “repressor” represents a successful coping strategy in the short term. The low dispersion of the values for the “repressor” type is also striking, which indicates that the constellation between fear denial and fear perception describes the fear coping type well. However, the repressor shows fewer health complaints and has a low inward orientation and a tendency to cope with emotions through external activities. Repressors in this study were more likely to attend political demonstrations and express opinions [7]. How effective this coping strategy can be in the long term and if there are any other negative impacts on their health situation should be clarified with future studies by focusing on the biocentric theory and mechanisms [7].
Ethical Considerations
Compliance with ethical guidelines
This research has been conducted following ethical principles, including the Declaration of Helsinki and the additional requirements. The experiments were undertaken with the informed written consent of each subject and according to the principles mentioned above.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors
Authors' contributions
The both authors equally contributed to preparing this article.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgments
We thank our colleague Jessica Knietzsch for her preparational work in obtaining the health cube questionnaire. We thank also the research group of the project “COVID 19 & Biocentric Disaster Management”.
References
Type of Study: Research |
Subject:
Special
Received: 2023/02/5 | Accepted: 2023/01/1 | Published: 2023/01/1
Received: 2023/02/5 | Accepted: 2023/01/1 | Published: 2023/01/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Health in Emergencies and Disasters Quarterly
Health in Emergencies & Disasters Research Center, University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave, Tehran, Iran.
Journal Tel: +9821 71732816 (2816)
Publisher Tel: +9821 4535 5555 - 4535 5000
