

Volume 10, Issue 2 (Winter 2025)
Health in Emergencies and Disasters Quarterly 2025, 10(2): 115-122 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Atighechian G, Taghiyan Z, Nasr Isfahani M. Mortality of Road Traffic Injured Patients Admitted to a Hospital in Isfahan, Iran, Using the GAP Scoring System. Health in Emergencies and Disasters Quarterly 2025; 10 (2) :115-122
URL: http://hdq.uswr.ac.ir/article-1-491-en.html
URL: http://hdq.uswr.ac.ir/article-1-491-en.html



1- Department of Health in Disasters and Emergencies, Health Management and Economics Research Center, School of Management and Medical Information Sciences, Isfahan University of Medical Sciences, Isfahan, Iran.
2- Student Research Committee, Department of Health Services Management, School of Management and Medical Information Sciences, Isfahan University of Medical Sciences, Isfahan, Iran. ,ztaghiyan@yahoo.com
3- Department of Emergency Medicine, School of Medicine, Al-Zahra Hospital, Isfahan University of Medical Sciences, Isfahan, Iran.
2- Student Research Committee, Department of Health Services Management, School of Management and Medical Information Sciences, Isfahan University of Medical Sciences, Isfahan, Iran. ,
3- Department of Emergency Medicine, School of Medicine, Al-Zahra Hospital, Isfahan University of Medical Sciences, Isfahan, Iran.
Keywords: Road traffic accidents, GAP (Glasgow coma scale, age, systolic blood pressure) score, Mortality
Full-Text [PDF 584 kb]
(1160 Downloads)
| Abstract (HTML) (3479 Views)
Full-Text: (665 Views)
Introduction
Road traffic accidents are one of the most important causes of death in the whole world. According to the report of the World Health Organization (WHO) in 2018, there were 1.35 million deaths due to road traffic accidents, which means one person dies every 24 seconds on the roads [1, 2]. Low- and middle-income countries have the highest number of road traffic deaths compared to other countries in the world. Road traffic deaths in Iran are also increasing [3-5]. Road traffic deaths are those occur during a road traffic accident or within 30 days after the accident due to the severity of injury [6, 7].
Trauma is the most common cause of death and disability in people aged 1-44 and the third cause of death regardless of age. Also, it is the first cause of potential years of life lost [8, 9, 10]. The trauma caused by road traffic accidents, in addition to death and severe injuries, has many economic and social costs, such as the cost of treatment, the cost of loss of family income during hospitalization, and the cost and time spent on training a new profession for the injured who are unable to do their previous profession due to injury. Also, it reduces the productivity of the country and imposes the cessation of activities to the society [11, 12]. Trauma is a time-sensitive emergency. During the first hours after trauma, management, assessment, resuscitation and determination of care are very important. The definite effect of providing early care in trauma centers has been shown in reducing mortality. Early diagnosis of trauma can help shorten the time of emergency care and quickly transfer the patient to a medical center. The increase in health care costs and the difference in the quality of provided services among different trauma centers suggest the need to evaluate the performance of trauma care.
Mortality index is considered as the most accurate measurable outcome for trauma [13-16]. Different scales have been used in this field to determine the severity of trauma in the injured patient. These scales use anatomical, physiological or both criteria to determine the severity of trauma [10]. Trauma scoring systems make doctors and nurses aware of the injury to the patient and help them make decisions in the trauma process. Several scoring systems have been developed to make clinical decisions as quickly as possible for trauma patients. Recently, the modified Glasgow coma scale, age, and systolic blood pressure (GAP) scoring system has been developed to predict mortality in trauma patients. These systems are effective not only in the correct triage of patients, but also in predicting the severity of injury and mortality [17]. Easy scoring based on age, Glasgow coma scale (GCS), and systolic blood pressure (SBP), which are easily available at the beginning of the examination, are among the advantages of the GAP scoring system [18]. This system is superior to other scoring systems due to the need for fewer parameters, the ability to be implemented at the scene, and the high power of predicting mortality [9, 11].
So far, many studies have been conducted on road traffic accidents in Iran and the effective factors in reducing them [19, 20]. Considering the importance of preventing road traffic deaths, this study aims to predict the injury severity and death of road traffic accident victims in Isfahan, Iran using the GAP score.
Materials and Methods
This is a cross-sectional study using the existing data approved by the Ethics Committee of Isfahan University of Medical Sciences. The data of all those with road traffic injuries transferred to Ayatollah Kashani Hospital in Isfahan, Iran, by the emergency medical services (EMS) ambulances during a 3-month period (November and December, 2019 and January, 2020) were assessed. The criteria for selecting the samples were a road traffic accident injury, age 18-65 years, and transferred to the hospital by the EMS ambulances. The exclusion criteria were the absence of the electronic file of medical records or the incompleteness of medical records. To collect data, a checklist was designed based on literature review and consultation with emergency medicine specialists. This checklist surveys personal information, gender, GCS, SBP, and the mechanism of the accident. The variables related to the GPA scoring system were extracted from the patients’ electronic medical records in the specified time frame.
This study was done in 5 stages. In the first stage, demographic characteristics (age, gender), GCS, SBP, accident mechanism, heart rate, breathing rate and blood oxygen saturation level of the injured were obtained from the Statistics Unit of the hospital. In the second step, the extracted information was compared with the hospital information system data. In the third stage, the GAP scoring system was used to predict the mortality rate. In this scoring system, the patient receives a GCS score of 3-15. For age <60 years, the considered score is 3, and for age >60, the considered score is 0. Moreover, if SBP >120 mm Hg, the considered score is 6; for a SBP of 60–120 mm Hg, the considered score is 4; and for a SBP <60 mm Hg, the considered score is 0. Therefore, the GAP score was between 3 and 24. According to the GAP score, the injured people were classified into three high-risk (score 3-10), moderate-risk (score 11-18) and low-risk (score 19-24) groups. In the fourth stage, the health status of the injured people was examined 24 hours and 4 weeks after discharge from the hospital. In addition, the list of the deceased was received from the hospital and the process of death after discharge was followed up through a phone call by using the phone number in their file. Also, forensic statistics were used to compare with hospital mortality statistics and to identify deaths after discharge. In the final stage, using the GAP scoring system parameters, a system was proposed to predict the mortality of road traffic accident cases and help experts prioritize the patients.
Descriptive statistics (frequency, percentage, Mean±SD) were used to describe the data and the receiver operating characteristic (ROC) curve was used to evaluate the accuracy of the GAP scoring system in predicting the outcome of trauma patients. In this curve, sensitivity refers to the probability of a correct positive test result, and specificity refers to the probability of a negative test result. Also, the area under the curve (AUC) is a statistical indicator of the accuracy of measurement. SPSS software, version 26 was used for data analysis.
Results
During 2019-2020, the EMS department of Isfahan Province had carried out more than 46,000 missions and transport of traffic accident victims to various medical centers in the province. Table 1 shows the total number of road traffic injured patients admitted to Ayatollah Kashani Hospital and the road traffic death cases in different months.
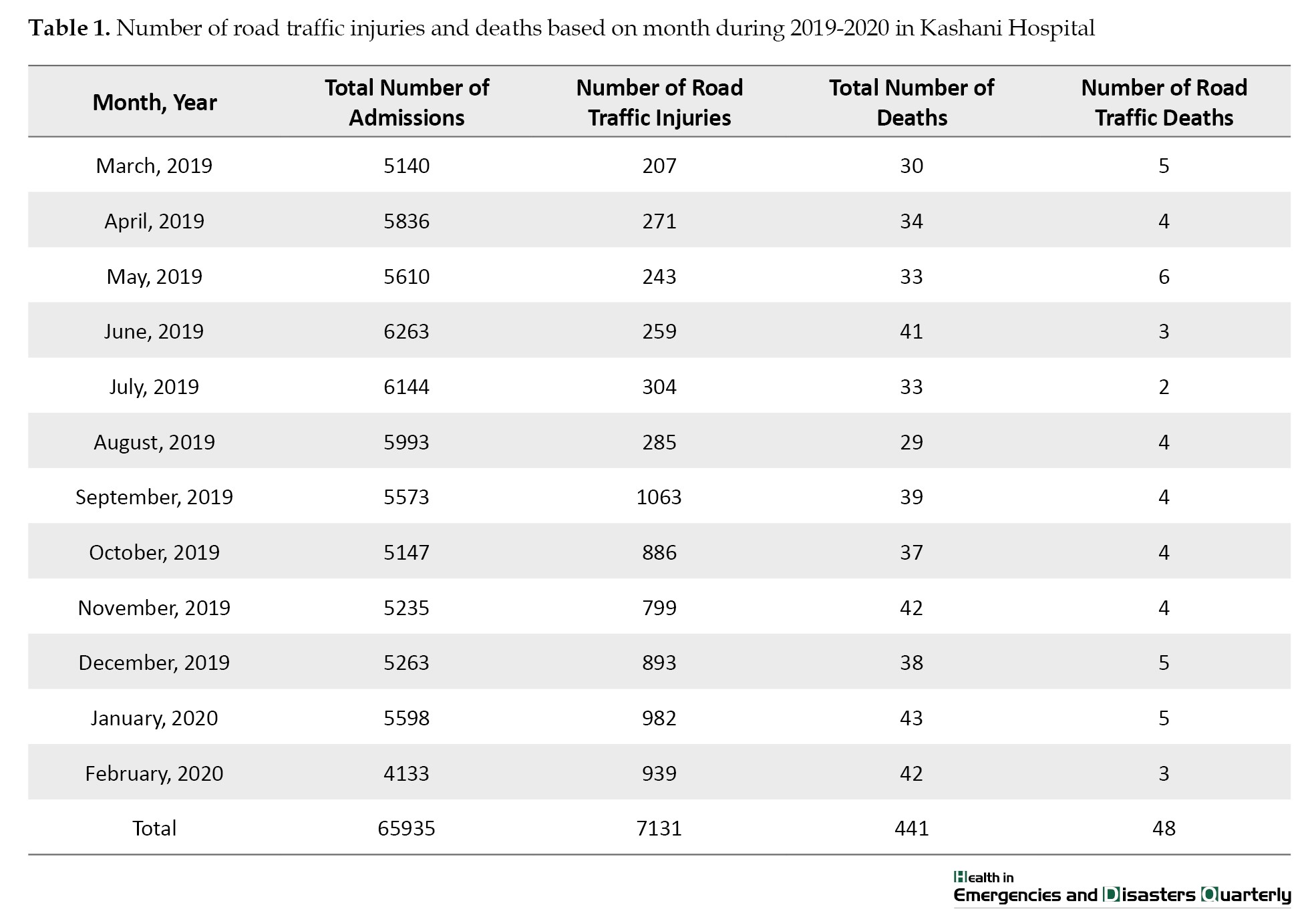
There were 7131 road traffic injured patients, which make up 15.3% of Isfahan Province population. The total number of patients admitted to Ayatollah Kashani Hospital in three months (November and December, 2019 and January, 2020) was 16096 people, of whom 123(4.6%) died. Also, the number of road traffic injured people transferred to the hospital by the EMS ambulances during these three months was 2674. Of these, the medical files of 1985 cases were complete. Of these, 1500(76%) were male and 485(24%) were female, and 14(2.5%) had died; most of them were motorcyclists and pedestrians. According to Figure 1, the most common vehicles involved in road traffic accidents were motorcycles, passenger cars and pickup trucks.
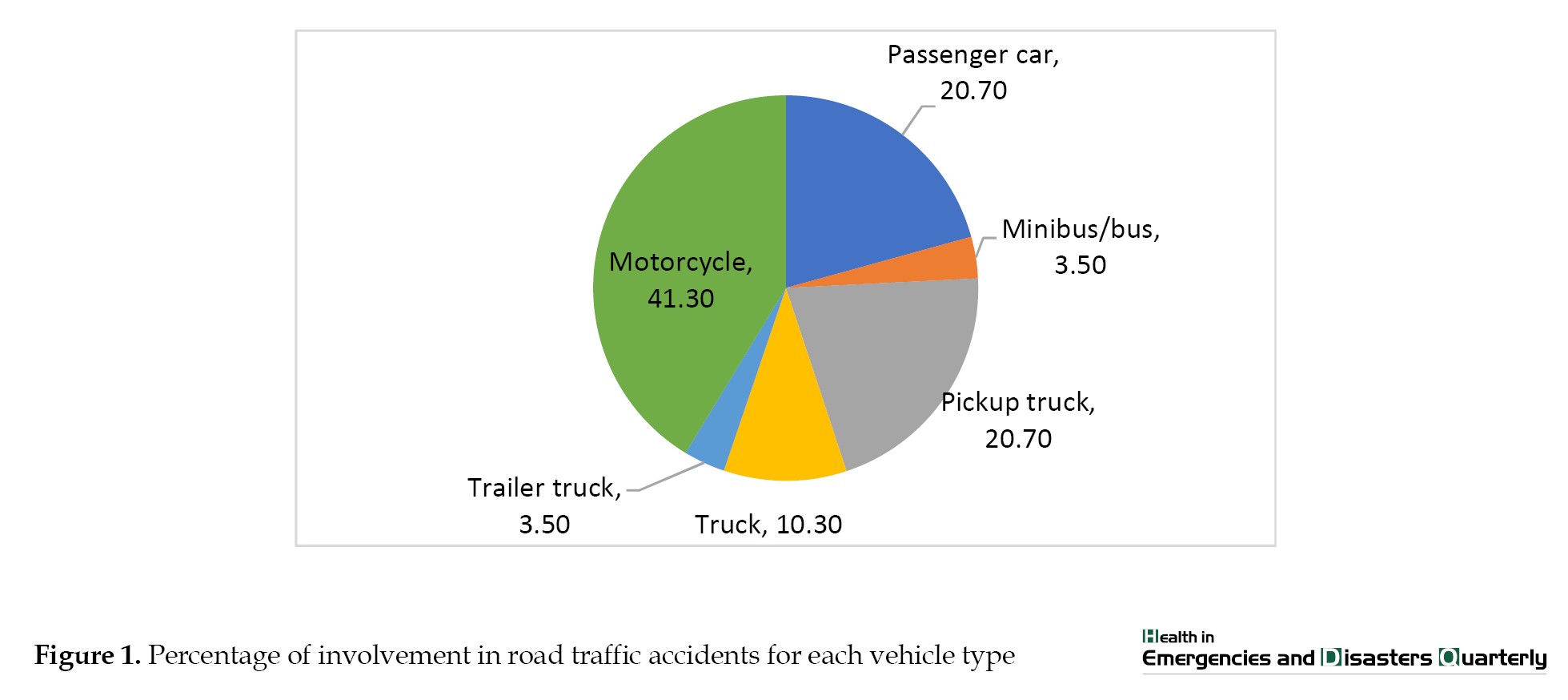 Table 2 shows the most common mechanism of accidents was vehicle collisions The most common mechanism of accidents was vehicle collisions.
Table 2 shows the most common mechanism of accidents was vehicle collisions The most common mechanism of accidents was vehicle collisions.
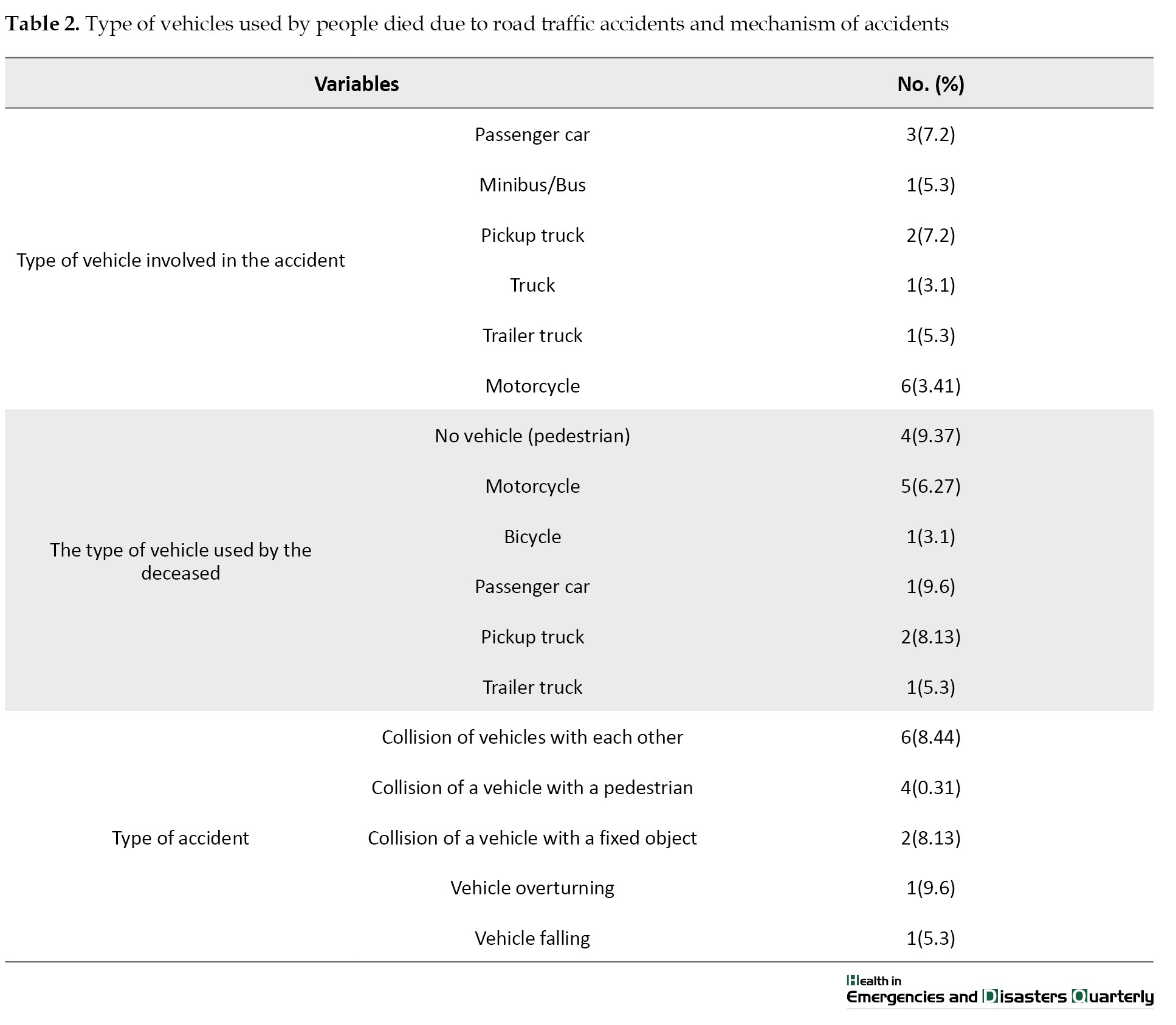
Of 14 deceased people, 2 were drivers, 9 were motorcyclists and pedestrians, and 3 were car/pillion passengers. The most common injured part of the body among deceased people was the face (62%) and the least common injured part was hands/arms (3.8%). The most common causes of death were head injury (59%) and multiple fractures (41%).
The classification of dead and injured people based on the GAP scoring system are shown in Table 3.
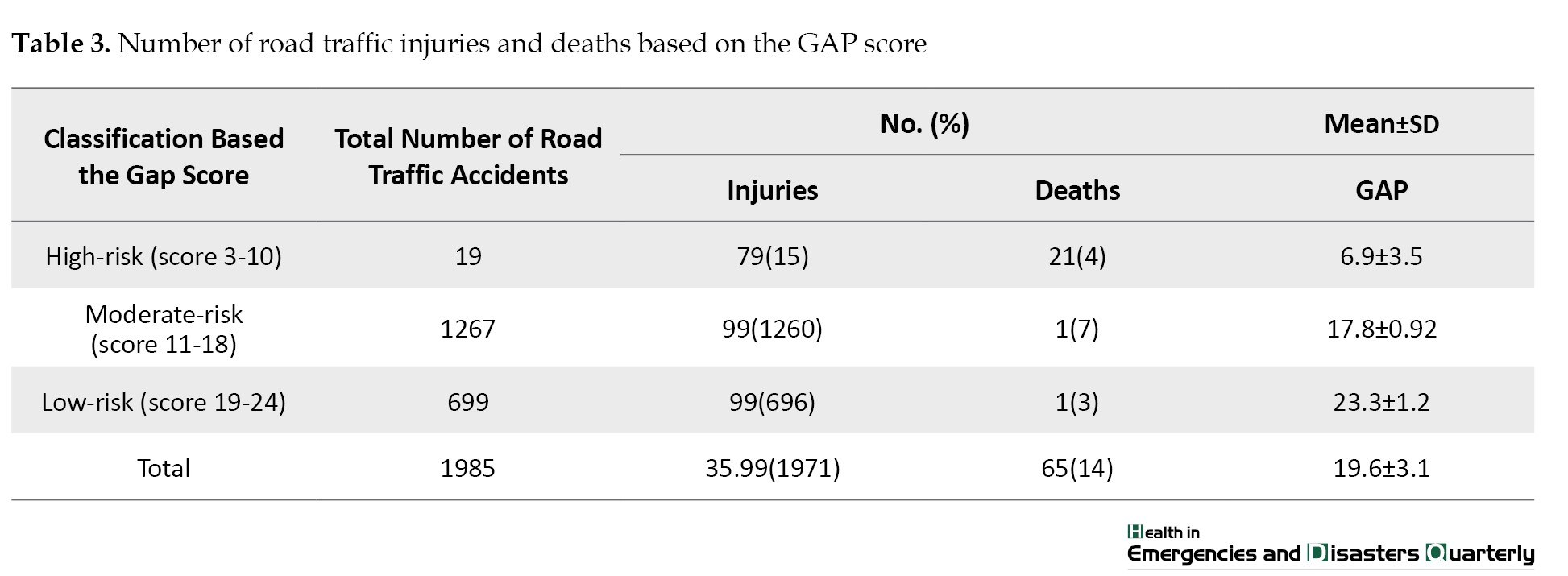
As can be seen, 19 people were in the high-risk group, 1267 were in the moderate-risk group and 699 were in the low-risk group. Among dead people, 4 were in the high-risk group (21%), 7 in the moderate-risk group (1%) and 3 in the low-risk group (1%). Table 4 shows the demographic characteristics of dead and injured people.
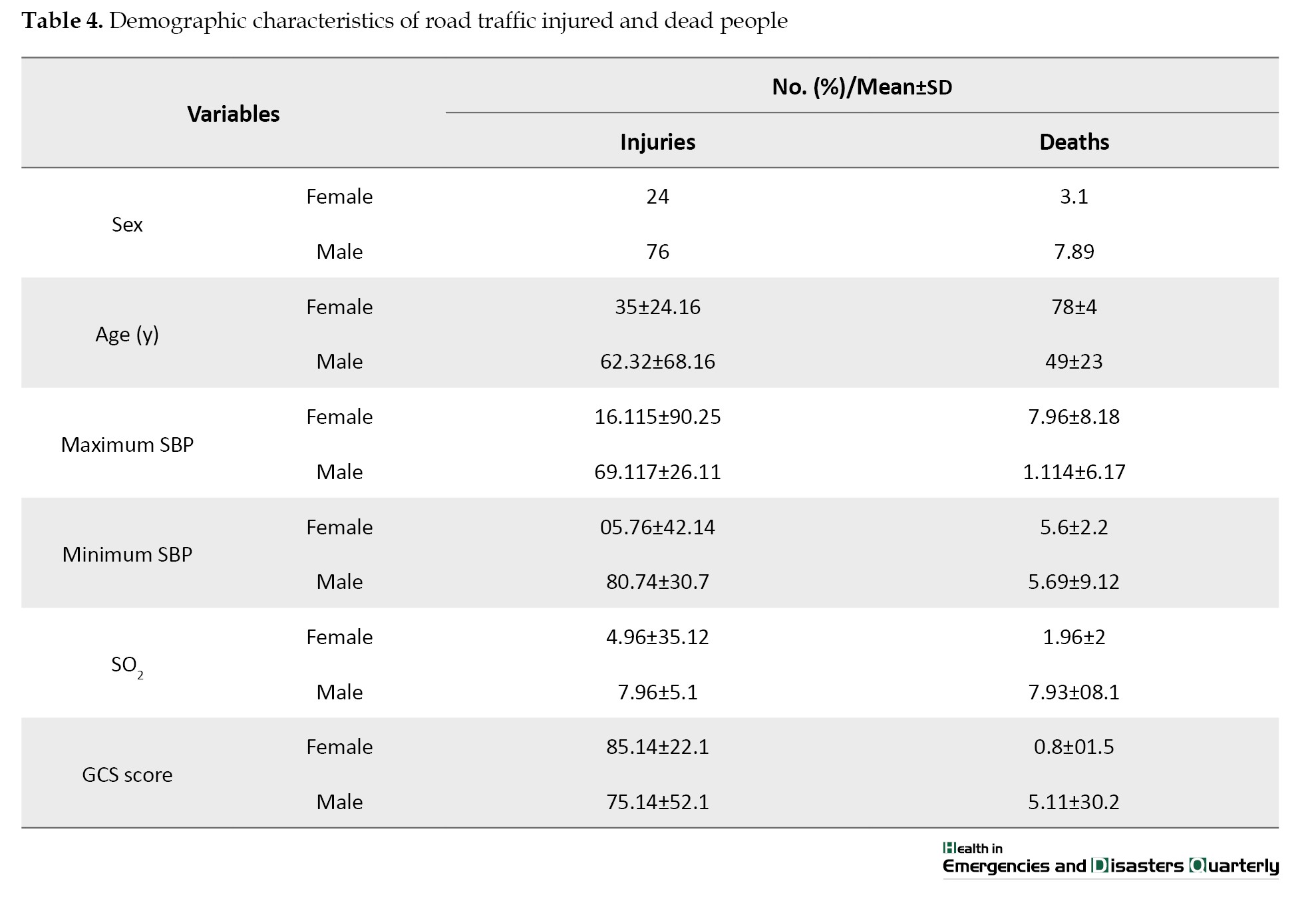
Overall, 76% were male (mean age=32 years) and 24% were female (mean age: 35 years). The male-to-female ratio of the death rates was 90:10. The mean age of deceased men and women was 49 and 78 years respectively. Moreover, the results showed that 1880 people had SBP of 60-120 mm Hg, of whom one person (0.05%) died; 60 had SBP >120, of whom 3(5%) died; and 45 had SBP<60, of whom 10(16.70%) died. The mean GCS score was 14.0±2.81 and the best cut-off point for GCS was 14; 73.1% of the injured people with a GCS score <14 had died. With the increase of age, the probability of death increased, and with the increase of SO2, the probability of death decreased.
According to Figure 2, the AUC was 0.96 for 24-hour mortality rate and 0.94 for 4-week mortality, indicating a good predictive power.
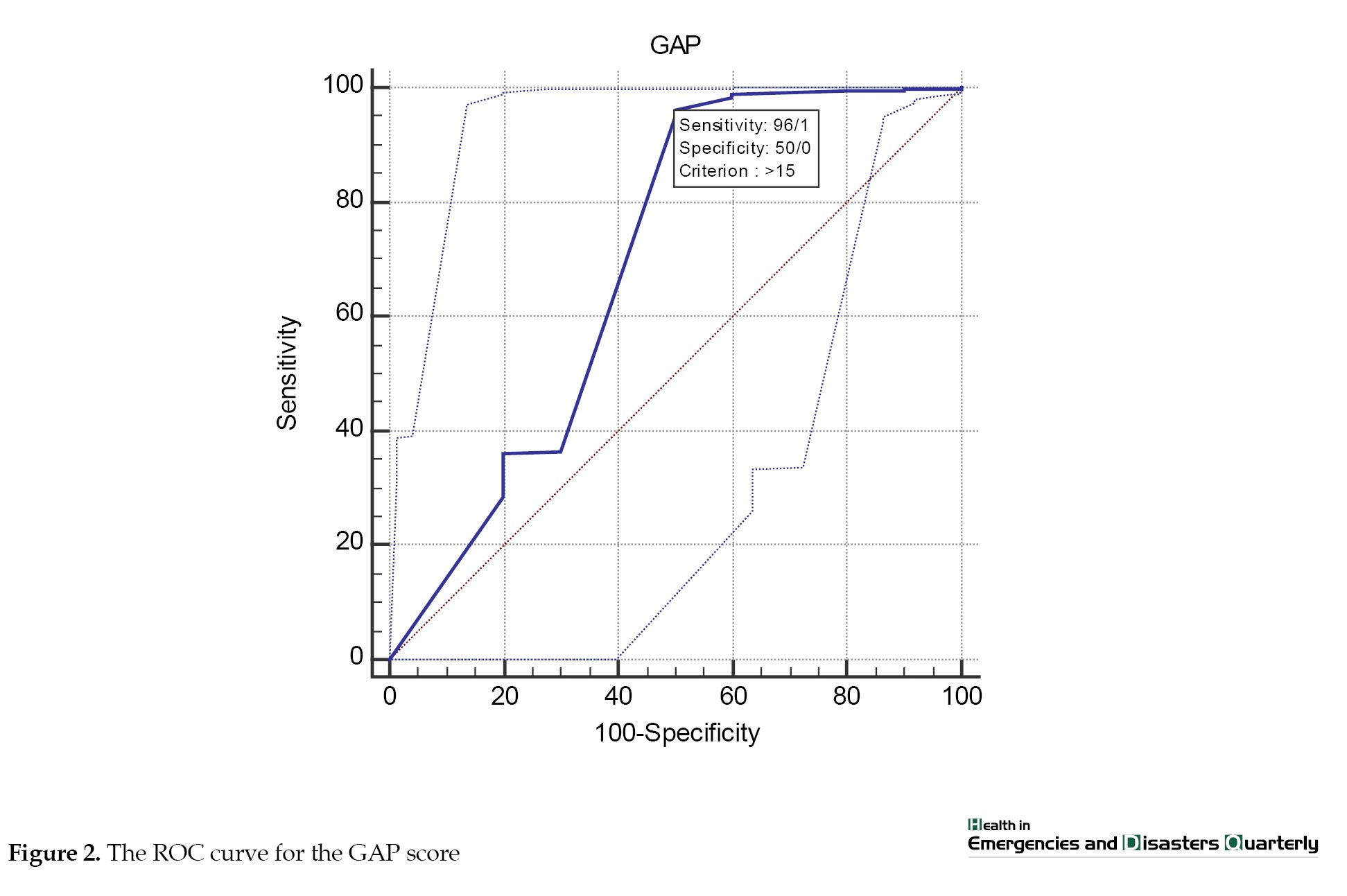 Also, the best cut-off point of the GAP scoring system in predicting 24-hour mortality was 15 and with a sensitivity of 96%.
Also, the best cut-off point of the GAP scoring system in predicting 24-hour mortality was 15 and with a sensitivity of 96%.
Discussion
It is important to deal with road traffic injuries in the shortest possible time, and the subsequent losses it causes to people. Consistent with other studies [18, 19, 21-23], the most road traffic deaths in Isfahan Province during three months (November and December, 2019 and January, 2020) were related to motorcycles (40%). Also, the most common mechanism of accidents was vehicle collisions. The most injured part of the body among the road traffic accident related death cases was the face (62%). Based on the GAP score, most of the road traffic death cases were in the high-risk group; the risk of death in the high-risk group was significantly higher than in the moderate- and low-risk groups, which is consistent with the results of other studies [10, 16, 24]. Also, the most of deceased people were under the age of 54(67.8%), which is consistent with the results of other studies [21-23]. This result indicates that age is one of the most important components in the GAP scoring system.
The GAP score is a better and more accurate predictor than other scoring systems due to the availability of required information and its use is more common and it predicts injury severity better than other systems [18, 20]. In the present study, the GAP system performed well in predicting the outcome of trauma patients, since the sensitivity, specificity, precision, positive and negative values, and the area under the ROC curve (AUC) were acceptable in this system. In Hasler et al.’s study, the AUC for the predictive power of the GAP score was 87.2% [17]. In other studies, a higher predictive power was reported for the GAP score. For example, in Ahun et al.’s study, the AUC was 0.904-0.910 [21]. In our study, the best cut-off point for the GAP scoring system in predicting short-term road traffic mortality was 15.8 with a sensitivity of 0.96. For long-term road traffic mortality, the best cut-off point was 18.22 with a sensitivity of 0.94. In the study by Baqi et al., the score of 22 was considered as the cut-off point for predicting hospital mortality [22], which is consistent with the reported cut-off point in predicting long-term (4-week) mortality in our study. In the study by Ahun et al., the best cut-off point for the GAP scoring system in predicting short-term mortality was 19, with a sensitivity of 83.33% [21].
One of the limitations of this study was the difficulty accessing to medical records and the lack of systematization and the absence of a codified data bank to separate different deaths, which caused a long time to review the files of each death. It is recommended that a registry system be established to record information and trace the road traffic injuries in Iran from the time of EMS arrival on scene to arriving at medical centers and the information about the discharge or death of the injured.
Conclusion
The GAP scoring system has a good power for predicting the mortality of road traffic accidents. Based on this system, Most of the deaths caused by road traffic accidents admitted to Ayatollah Kashani Hospital in Isfahan are related to the high-risk groups. It is recommended that all hospitals in Iran that accept road traffic injured people, use the GAP scoring system to evaluate the medical measures for these patients.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Isfahan University of Medical Sciences (Code: IR.MUI.RESEARCH.REC.1399.756)
Funding
This article was extracted from the master’s thesis of Zohreh Taghiyan, approved by the Department of Health Services Management, School of Management and Medical Information Sciences, Isfahan University of Medical Sciences, Isfahan, Iran. This study was funded by Isfahan University of Medical Sciences, Isfahan, Iran (Code: 399882).
Authors' contributions
Conceptualization and supervision: Golrokh Atighechian and Mohammed Nasr Isfahani; Methodology and data analysis: Golrokh Atighechian and Zohreh Taghiyan; Data collection: Zohreh Taghiyan and Mohammed Nasr Isfahani; Investigation and writing: All authors; Funding acquisition and recources: Golrokh Atighechian.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the Vice-Chancellor for Research of Isfahan University of Medical Sciences, the managers of Ayatollah Kashani Hospital in Isfahan, and the Emergency Medicine and Forensic Medicine organizations in Isfahan City for their support and cooperation in this study.
References
Road traffic accidents are one of the most important causes of death in the whole world. According to the report of the World Health Organization (WHO) in 2018, there were 1.35 million deaths due to road traffic accidents, which means one person dies every 24 seconds on the roads [1, 2]. Low- and middle-income countries have the highest number of road traffic deaths compared to other countries in the world. Road traffic deaths in Iran are also increasing [3-5]. Road traffic deaths are those occur during a road traffic accident or within 30 days after the accident due to the severity of injury [6, 7].
Trauma is the most common cause of death and disability in people aged 1-44 and the third cause of death regardless of age. Also, it is the first cause of potential years of life lost [8, 9, 10]. The trauma caused by road traffic accidents, in addition to death and severe injuries, has many economic and social costs, such as the cost of treatment, the cost of loss of family income during hospitalization, and the cost and time spent on training a new profession for the injured who are unable to do their previous profession due to injury. Also, it reduces the productivity of the country and imposes the cessation of activities to the society [11, 12]. Trauma is a time-sensitive emergency. During the first hours after trauma, management, assessment, resuscitation and determination of care are very important. The definite effect of providing early care in trauma centers has been shown in reducing mortality. Early diagnosis of trauma can help shorten the time of emergency care and quickly transfer the patient to a medical center. The increase in health care costs and the difference in the quality of provided services among different trauma centers suggest the need to evaluate the performance of trauma care.
Mortality index is considered as the most accurate measurable outcome for trauma [13-16]. Different scales have been used in this field to determine the severity of trauma in the injured patient. These scales use anatomical, physiological or both criteria to determine the severity of trauma [10]. Trauma scoring systems make doctors and nurses aware of the injury to the patient and help them make decisions in the trauma process. Several scoring systems have been developed to make clinical decisions as quickly as possible for trauma patients. Recently, the modified Glasgow coma scale, age, and systolic blood pressure (GAP) scoring system has been developed to predict mortality in trauma patients. These systems are effective not only in the correct triage of patients, but also in predicting the severity of injury and mortality [17]. Easy scoring based on age, Glasgow coma scale (GCS), and systolic blood pressure (SBP), which are easily available at the beginning of the examination, are among the advantages of the GAP scoring system [18]. This system is superior to other scoring systems due to the need for fewer parameters, the ability to be implemented at the scene, and the high power of predicting mortality [9, 11].
So far, many studies have been conducted on road traffic accidents in Iran and the effective factors in reducing them [19, 20]. Considering the importance of preventing road traffic deaths, this study aims to predict the injury severity and death of road traffic accident victims in Isfahan, Iran using the GAP score.
Materials and Methods
This is a cross-sectional study using the existing data approved by the Ethics Committee of Isfahan University of Medical Sciences. The data of all those with road traffic injuries transferred to Ayatollah Kashani Hospital in Isfahan, Iran, by the emergency medical services (EMS) ambulances during a 3-month period (November and December, 2019 and January, 2020) were assessed. The criteria for selecting the samples were a road traffic accident injury, age 18-65 years, and transferred to the hospital by the EMS ambulances. The exclusion criteria were the absence of the electronic file of medical records or the incompleteness of medical records. To collect data, a checklist was designed based on literature review and consultation with emergency medicine specialists. This checklist surveys personal information, gender, GCS, SBP, and the mechanism of the accident. The variables related to the GPA scoring system were extracted from the patients’ electronic medical records in the specified time frame.
This study was done in 5 stages. In the first stage, demographic characteristics (age, gender), GCS, SBP, accident mechanism, heart rate, breathing rate and blood oxygen saturation level of the injured were obtained from the Statistics Unit of the hospital. In the second step, the extracted information was compared with the hospital information system data. In the third stage, the GAP scoring system was used to predict the mortality rate. In this scoring system, the patient receives a GCS score of 3-15. For age <60 years, the considered score is 3, and for age >60, the considered score is 0. Moreover, if SBP >120 mm Hg, the considered score is 6; for a SBP of 60–120 mm Hg, the considered score is 4; and for a SBP <60 mm Hg, the considered score is 0. Therefore, the GAP score was between 3 and 24. According to the GAP score, the injured people were classified into three high-risk (score 3-10), moderate-risk (score 11-18) and low-risk (score 19-24) groups. In the fourth stage, the health status of the injured people was examined 24 hours and 4 weeks after discharge from the hospital. In addition, the list of the deceased was received from the hospital and the process of death after discharge was followed up through a phone call by using the phone number in their file. Also, forensic statistics were used to compare with hospital mortality statistics and to identify deaths after discharge. In the final stage, using the GAP scoring system parameters, a system was proposed to predict the mortality of road traffic accident cases and help experts prioritize the patients.
Descriptive statistics (frequency, percentage, Mean±SD) were used to describe the data and the receiver operating characteristic (ROC) curve was used to evaluate the accuracy of the GAP scoring system in predicting the outcome of trauma patients. In this curve, sensitivity refers to the probability of a correct positive test result, and specificity refers to the probability of a negative test result. Also, the area under the curve (AUC) is a statistical indicator of the accuracy of measurement. SPSS software, version 26 was used for data analysis.
Results
During 2019-2020, the EMS department of Isfahan Province had carried out more than 46,000 missions and transport of traffic accident victims to various medical centers in the province. Table 1 shows the total number of road traffic injured patients admitted to Ayatollah Kashani Hospital and the road traffic death cases in different months.
There were 7131 road traffic injured patients, which make up 15.3% of Isfahan Province population. The total number of patients admitted to Ayatollah Kashani Hospital in three months (November and December, 2019 and January, 2020) was 16096 people, of whom 123(4.6%) died. Also, the number of road traffic injured people transferred to the hospital by the EMS ambulances during these three months was 2674. Of these, the medical files of 1985 cases were complete. Of these, 1500(76%) were male and 485(24%) were female, and 14(2.5%) had died; most of them were motorcyclists and pedestrians. According to Figure 1, the most common vehicles involved in road traffic accidents were motorcycles, passenger cars and pickup trucks.
Of 14 deceased people, 2 were drivers, 9 were motorcyclists and pedestrians, and 3 were car/pillion passengers. The most common injured part of the body among deceased people was the face (62%) and the least common injured part was hands/arms (3.8%). The most common causes of death were head injury (59%) and multiple fractures (41%).
The classification of dead and injured people based on the GAP scoring system are shown in Table 3.
As can be seen, 19 people were in the high-risk group, 1267 were in the moderate-risk group and 699 were in the low-risk group. Among dead people, 4 were in the high-risk group (21%), 7 in the moderate-risk group (1%) and 3 in the low-risk group (1%). Table 4 shows the demographic characteristics of dead and injured people.
Overall, 76% were male (mean age=32 years) and 24% were female (mean age: 35 years). The male-to-female ratio of the death rates was 90:10. The mean age of deceased men and women was 49 and 78 years respectively. Moreover, the results showed that 1880 people had SBP of 60-120 mm Hg, of whom one person (0.05%) died; 60 had SBP >120, of whom 3(5%) died; and 45 had SBP<60, of whom 10(16.70%) died. The mean GCS score was 14.0±2.81 and the best cut-off point for GCS was 14; 73.1% of the injured people with a GCS score <14 had died. With the increase of age, the probability of death increased, and with the increase of SO2, the probability of death decreased.
According to Figure 2, the AUC was 0.96 for 24-hour mortality rate and 0.94 for 4-week mortality, indicating a good predictive power.
Discussion
It is important to deal with road traffic injuries in the shortest possible time, and the subsequent losses it causes to people. Consistent with other studies [18, 19, 21-23], the most road traffic deaths in Isfahan Province during three months (November and December, 2019 and January, 2020) were related to motorcycles (40%). Also, the most common mechanism of accidents was vehicle collisions. The most injured part of the body among the road traffic accident related death cases was the face (62%). Based on the GAP score, most of the road traffic death cases were in the high-risk group; the risk of death in the high-risk group was significantly higher than in the moderate- and low-risk groups, which is consistent with the results of other studies [10, 16, 24]. Also, the most of deceased people were under the age of 54(67.8%), which is consistent with the results of other studies [21-23]. This result indicates that age is one of the most important components in the GAP scoring system.
The GAP score is a better and more accurate predictor than other scoring systems due to the availability of required information and its use is more common and it predicts injury severity better than other systems [18, 20]. In the present study, the GAP system performed well in predicting the outcome of trauma patients, since the sensitivity, specificity, precision, positive and negative values, and the area under the ROC curve (AUC) were acceptable in this system. In Hasler et al.’s study, the AUC for the predictive power of the GAP score was 87.2% [17]. In other studies, a higher predictive power was reported for the GAP score. For example, in Ahun et al.’s study, the AUC was 0.904-0.910 [21]. In our study, the best cut-off point for the GAP scoring system in predicting short-term road traffic mortality was 15.8 with a sensitivity of 0.96. For long-term road traffic mortality, the best cut-off point was 18.22 with a sensitivity of 0.94. In the study by Baqi et al., the score of 22 was considered as the cut-off point for predicting hospital mortality [22], which is consistent with the reported cut-off point in predicting long-term (4-week) mortality in our study. In the study by Ahun et al., the best cut-off point for the GAP scoring system in predicting short-term mortality was 19, with a sensitivity of 83.33% [21].
One of the limitations of this study was the difficulty accessing to medical records and the lack of systematization and the absence of a codified data bank to separate different deaths, which caused a long time to review the files of each death. It is recommended that a registry system be established to record information and trace the road traffic injuries in Iran from the time of EMS arrival on scene to arriving at medical centers and the information about the discharge or death of the injured.
Conclusion
The GAP scoring system has a good power for predicting the mortality of road traffic accidents. Based on this system, Most of the deaths caused by road traffic accidents admitted to Ayatollah Kashani Hospital in Isfahan are related to the high-risk groups. It is recommended that all hospitals in Iran that accept road traffic injured people, use the GAP scoring system to evaluate the medical measures for these patients.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Isfahan University of Medical Sciences (Code: IR.MUI.RESEARCH.REC.1399.756)
Funding
This article was extracted from the master’s thesis of Zohreh Taghiyan, approved by the Department of Health Services Management, School of Management and Medical Information Sciences, Isfahan University of Medical Sciences, Isfahan, Iran. This study was funded by Isfahan University of Medical Sciences, Isfahan, Iran (Code: 399882).
Authors' contributions
Conceptualization and supervision: Golrokh Atighechian and Mohammed Nasr Isfahani; Methodology and data analysis: Golrokh Atighechian and Zohreh Taghiyan; Data collection: Zohreh Taghiyan and Mohammed Nasr Isfahani; Investigation and writing: All authors; Funding acquisition and recources: Golrokh Atighechian.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the Vice-Chancellor for Research of Isfahan University of Medical Sciences, the managers of Ayatollah Kashani Hospital in Isfahan, and the Emergency Medicine and Forensic Medicine organizations in Isfahan City for their support and cooperation in this study.
References
- Chang FR, Huang HL, Schwebel DC, Chan AHS, Hu GQ. Global road traffic injury statistics: Challenges, mechanisms and solutions. Chinese Journal of Traumatology. 2020; 23(4):216-8. [DOI:10.1016/j.cjtee.2020.06.001] [PMID]
- Moradi A, Rahmani K, Hoshmandi Shoja M, Rahimi Sepehr H, Khorshidi A. [An overview of the situation of traffic accidents in Iran in comparison with other countries (Persian)]. Iranian Journal of Forensic Medicine. 2016; 22(1):45-53. [Link]
- Legal Medicine Organization. [Statistics of the dead and injured in traffic accidents according to the Iranian Legal Medicine organization (Persian)]. Tehran: Legal Medicine organization; 2021.
- Rezazadeh Z, Askarishahi M, Vakili M. [Trend of fetal traffic injuries in Iran from 2009 to 2018 (Persian)]. Tolooebehdasht. 2021; 19(6):50-62. [DOI:10.18502/tbj.v19i6.5709]
- Sarvari MH, Jani MR, Mohalli F, Alinejadmoghaddam M. [Epidemiology of trauma related to traffic accident in injured people referred to Shohada Hospital in Ghaen (Pesian)]. Paramedical Sciences and Military Health. 2020; 14(4):10-7. [Link]
- Cassignol A, Markarian T, Cotte J, Marmin J, Nguyen C, Cardinale M, et al. Evaluation and comparison of different prehospital triage scores of trauma patients on in-hospital mortality. Prehospital Emergency Care. 2019; 23(4):543-50. [DOI:10.1080/10903127.2018.1549627] [PMID]
- Servasius Ratu B, Yuyun Y, Yulian Wiji U. Comparison of Trauma scoring ability to predict survival rate in countries with low to middle-income. International Journal of Science and Society. 2020; 2(4):194-206. [DOI:10.54783/ijsoc.v2i4.204]
- Amirtharaj AD, Lazarus ER, Alzaabi O. Assessing validity and reliability of glasgow coma scale and full outline of unresponsiveness score: A systematic review. International Journal of Health Sciences. 2022; 6(S2):12293-306. [DOI:10.53730/ijhs.v6nS2.8259]
- Farzan N, Foroghi Ghomi SY, Mohammadi AR. A retrospective study on evaluating GAP, MGAP, RTS and ISS trauma scoring system for the prediction of mortality among multiple trauma patients. Annals of Medicine and Surgery. 2022; 76:103536. [DOI:10.1016/j.amsu.2022.103536] [PMID]
- Ghadirzadeh MR, Shojaei A, Khademi A, Khodadoost M, Kandi M, Alaeddini F, et al. Status and trend of deaths due to traffic accidents from 2001 to 2010 in Iran. Iranian Journal of Epidemiology. 2015; 11(2):13-22. [Link]
- Basak D, Chatterjee S, Attergrim J, Sharma MR, Soni KD, Verma S, et al. Glasgow coma scale compared to other trauma scores in discriminating in-hospital mortality of traumatic brain injury patients admitted to urban Indian hospitals: A multicentre prospective cohort study. Injury. 2023; 54(1):93-9. [DOI:10.1016/j.injury.2022.09.035] [PMID]
- Mkubwa JJ, Bedada AG, Esterhuizen TM. Traumatic brain injury: Association between the Glasgow Coma Scale score and intensive care unit mortality. The Southern African Journal of Critical Care. 2022; 38(2):10.7196/SAJCC.2022.v38i2.525. [DOI:10.7196/SAJCC.2022.v38i2.525] [PMID]
- Amini K, Abolghasemi Fakhri S, Salehi H, Ebrahimi Bakhtavar H, Rahmani F. Mortality prediction in multiple trauma patients using GAP, RTS and NTS Models. Trauma Monthly. 2021; 26(5):252-7. [DOI:10.30491/tm.2021.262592.1212]
- Khajoei R, Abadi MZ, Dehesh T, Heydarpour N, Shokohian S, Rahmani F. Predictive value of the glasgow coma scale, age, and arterial blood pressure and the new trauma score indicators to determine the hospital mortality of multiple trauma patients. Archives of Trauma Research. 2021; 10(2):86-91. [DOI:10.4103/atr.atr_72_20]
- Yadollahi M, Ghaedsharaf Z, Jamali K, Niakan MH, Pazhuheian F, Karajizadeh M. The accuracy of GAP and MGAP scoring systems in predicting mortality in trauma; a diagnostic accuracy study. Frontiers in Emergency Medicine. 2019; 4(3):e73. [Link]
- Tengku Isni Yuli Lestari P, Ahsan, Dhelya W. Glasgow coma scale, age and systolic blood pressure (gap) as impairment predictor of head injury patients. The Malaysian Journal of Nursing (MJN). 2019; 11(1):57-62. [DOI:10.31674/mjn.2019.v11i01.008]
- Hasler RM, Mealing N, Rothen HU, Coslovsky M, Lecky F, Jüni P. Validation and reclassification of MGAP and GAP in hospital settings using data from the Trauma Audit and Research Network. The Journal of Trauma and Acute Care Surgery. 2014; 77(5):757-63. [DOI:10.1097/TA.0000000000000452] [PMID]
- Rahmani F, Bakhtavar HE, Vahdati SS, Hosseini M, Esfanjani RM. Evaluation of MGAP and GAP trauma scores to predict prognosis of multiple-trauma patients. Trauma Monthly. 2017; 22(3):e33249. [Link]
- Ghelichkhani P, Esmaeili M, Hosseini M, Seylani K. Glasgow Coma Scale and FOUR Score in predicting the mortality of trauma patients; a diagnostic accuracy study. Emergency. 2018; 6(1):e42. [PMID]
- Soltani Y, Khaleghdoost Mohamadi T, Adib M, Kazemnejad E, Aghaei I, Ghanbari A. [Comparing the predictive ability for mortality rates by GAP and MGAP scoring systems in multiple-trauma patients (Persian)]. Journal of Mazandaran University of Medical Sciences. 2018; 27(157):118-32. [Link]
- Ahun E, Köksal Ö, Sığırlı D, Torun G, Dönmez SS, Armağan E. Value of the Glasgow coma scale, age, and arterial blood pressure score for predicting the mortality of major trauma patients presenting to the emergency department. Turkish Journal of Trauma & Emergency Surgery. 2014; 20(4):241-7. [DOI:10.5505/tjtes.2014.76399] [PMID]
- Baghi I, Shokrgozar L, Herfatkar MR, Ehsan KN, Amiri ZM. Mechanism of injury, glasgow coma scale, age, and systolic blood pressure: A new trauma scoring system to predict mortality in trauma patients. Trauma Monthly. 2015; 20(3):e24473. [PMID]
- Astawa P, Aryana N. W, Pratama NA. Relationship between the injury severity score and GAP score with IL-6 cytokine in fracture patients with multiple trauma. International Journal of Research in Medical Sciences. 2016; 4(11):4999-5001. [DOI:10.18203/2320-6012.ijrms20163806]
- Kondo Y, Abe T, Kohshi K, Tokuda Y, Cook EF, Kukita I. Revised trauma scoring system to predict in-hospital mortality in the emergency department: Glasgow Coma Scale, Age, and Systolic Blood Pressure score. Critical Care. 2011; 15(4):R191. [DOI:10.1186/cc10348] [PMID]
Type of article: Research |
Subject:
traffic accidents
Received: 2023/02/5 | Accepted: 2024/01/18 | Published: 2025/01/1
Received: 2023/02/5 | Accepted: 2024/01/18 | Published: 2025/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
