

Volume 9, Issue 1 (Autumn 2023)
Health in Emergencies and Disasters Quarterly 2023, 9(1): 33-42 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rezaee Ghalee M, Mohammadi Zeidi I, Akbari Shahrestanaki Y, Maleki A, Kalhor R. Effects of a Theory-based Educational Intervention on Skills of Emergency Medical Service Personnel for Scene Management in Chemical Accidents. Health in Emergencies and Disasters Quarterly 2023; 9 (1) :33-42
URL: http://hdq.uswr.ac.ir/article-1-513-en.html
URL: http://hdq.uswr.ac.ir/article-1-513-en.html
Mohammadreza Rezaee Ghalee1 

 , Isa Mohammadi Zeidi2 , Yousof Akbari Shahrestanaki3 , Aisa Maleki1 , Rohollah Kalhor * 4
, Isa Mohammadi Zeidi2 , Yousof Akbari Shahrestanaki3 , Aisa Maleki1 , Rohollah Kalhor * 4
, Isa Mohammadi Zeidi2 , Yousof Akbari Shahrestanaki3 , Aisa Maleki1 , Rohollah Kalhor * 4
1- Student Research Committee, Faculty of Health, Qazvin University of Medical Sciences, Qazvin, Iran.
2- Social Determinants of Health Research Center, Research Institute for Prevention of Non-communicable Diseases, Qazvin University of Medical Sciences, Qazvin, Iran.
3- Department of Prehospital Medical Emergencies, School of Paramedicine, Qazvin University of Medical Sciences, Qazvin, Iran.
4- Social Determinants of Health Research Center, Research Institute for Prevention of Non-communicable Diseases, Qazvin University of Medical Sciences, Qazvin, Iran. , r.kalhor@qums.ac.ir
2- Social Determinants of Health Research Center, Research Institute for Prevention of Non-communicable Diseases, Qazvin University of Medical Sciences, Qazvin, Iran.
3- Department of Prehospital Medical Emergencies, School of Paramedicine, Qazvin University of Medical Sciences, Qazvin, Iran.
4- Social Determinants of Health Research Center, Research Institute for Prevention of Non-communicable Diseases, Qazvin University of Medical Sciences, Qazvin, Iran. , r.kalhor@qums.ac.ir
Full-Text [PDF 541 kb]
(171 Downloads)
| Abstract (HTML) (772 Views)
Full-Text: (107 Views)
Introduction
Chemical compounds play significant roles in the development of human society [1]. In recent decades, their production and use have significantly increased. As a result, the accidental release of chemicals into the environment might have grown due to industrial incidents, natural disasters, or deliberate terrorist attacks. The explosion of the ammonium nitrate depot in Beirut is an example of such a catastrophe [2].
Despite the magnitude of chemical accidents, there are no centralized and classified general statistics of these accidents worldwide. According to the US Occupational Safety and Health Administration (OSHA), 742000 people die every year due to cancers after exposure to chemical compounds [3]. Iran lacks accurate reports on chemical accidents and their classifications [4]. According to statistics, Iran has been listed among the 5 countries with the highest death toll from accidents in 2017 [5]. Chemical accidents are more critical due to their wide and high diffusion rate [6]. These accidents have multiple domino effects, with widespread casualties, financial loss, and environmental pollution [7]. These accidents, with their high casualties, create an unexpected and sudden demand for medical care, exceeding the normal capacity of service providers and imposing a heavy burden on healthcare systems [8]. In Iran, health and safety inspections in the public sector have been carried out as a control measure for the last 30 years [6].
Studies in the United States indicate that unpreparedness for accidents causes $280 million of damage to its healthcare system every year [9]. Survival rates in chemical accidents are markedly associated with readiness levels, specialized expertise, and coping and control skills of hospital services and prehospital emergency service providers [10].
The Iranian emergency system encompasses two main parts: Prehospital emergency and hospital emergency. Each provides specific time and performance indicators. The prehospital emergency department duty starts by contacting the emergency center and transferring the injured to the hospital emergency department. The care process continues until the stabilization of the injured condition. In each stage, scene management is of great importance. In major chemical accidents, scene management is subject to the proper performance, namely the triage of patients, prompt medical care, and transfer of casualties that, in turn, require the technicians’ functional role to manage the scene [11]. Therefore, active, up-to-date, standard education and health care services are the key to coping with the crisis [12].
Occupational health behavior effectively prevents unsafe performance and manages the incident scene. This concept means providing and maintaining the highest level of mental, physical, and social well-being through risk control, employee-to-job adaptation, and health maintenance [13]. In addition, the staff’s professional and teamwork skills are also determining factors [14].
Technicians show different behaviors in the workplace despite having sufficient awareness. This diversity in actions indicates that other factors besides awareness contribute to technicians’ reporting behavior. Safety climate, risk understanding, and belief increase the probability of success in health promotion interventions in the workplace [15].
According to studies, the most effective training programs are based on theoretical approaches rooted in behavioral change patterns. Using patterns and behavior change theories increases the impact of health training programs and helps identify the effective individual and environmental characteristics [16].
The theory of planned behavior (TPB) is one of the most comprehensive and suitable theories for investigating behavior. The theory was developed by Ajzen and Fishbein in 1980 to predict and explain individual behavior. The theory assumes an individual is a rational performer, so the person processes information before performing a behavior. Individuals’ fundamental beliefs and, consequently, their behavior may change. According to the theory, the main cause of behavior is the intention to do that behavior. Intention is the main index by which individuals can understand how much they want to do something and try to plan a certain behavior. Results of interventional research in Iran using different models and behavior change theories indicated a significant improvement in safe behaviors in workers and other safety groups [17-19].
Apart from a few studies in the field of accident management in Iran, many suffer from various limitations. For instance, a lot of studies have relied on traditional education and overlooked behavior change patterns. Furthermore, they were designed without considering the study’s main purpose and using appropriate models and theories. The other limitations of previous studies were their short follow-up periods, the lack of a control group, and the loss of control over the confounders.
Given the frequency of chemical accidents and their serious consequences, the present study aimed to determine the effect of theoretical-based educational intervention on emergency medical personnel’s skills to manage scenes in chemical accidents.
Materials and Methods
The present research was a quasi-experimental randomized controlled study conducted in Qazvin Province, Iran, from the beginning of February 2018 to the end of August 2019. The statistical population consisted of all emergency medical personnel of Qazvin Province. Among the emergency medical personnel, 70 were selected to participate in the study based on the inclusion and exclusion criteria using the available sampling method. In doing so, a list of all emergency medical personnel working in each emergency medical center was prepared. The centers were then assigned to experimental and control groups. The individuals were selected to participate in the study using a table of random numbers while observing the issue of possible overlap and the likelihood of exposure to control and experimental group personnel. The sample size was equal to 35 for each experimental and control group using G*Power software. We assumed a 95% confidence level, an 80% test power, a 50% impact factor, and a 10% drop estimate. The entry and exit of all technicians to study were voluntary. The control group received no training or intervention until the end of the second phase follow-up.
The inclusion criteria were as follows: At least 22 years of age; operational personnel with a medical degree such as nursing, medical emergency, anesthesia, or operating room; at least 2 years of experience in a prehospital emergency and operation unit; and working in one of urban, rural and air centers of Qazvin Province. The exclusion criteria were as follows: Retirement of medical emergency personnel during the study, non-participation of personnel in training classes, working in emergency centers of other provinces, and not providing the consent form.
After initial coordination with the Qazvin University of Medical Sciences and obtaining a research permit and submitting it to Qazvin Medical Emergency Center, technicians of the experimental and control groups were invited to complete the study questionnaires and participate in training classes with prior notice from the training unit. The study data were collected using self-report questionnaires in experimental and control groups before and two months after the theory-based intervention. Data collection tools were as follows.
We used a demographic questionnaire that collected information regarding age, marital status, education level, field of study, job, work experience, and history of exposure to chemical accidents.
A scale assessed the theory of planned behavior (TPB). First, while reviewing previous studies, a quasi-in-depth interview was conducted with 10 medical emergency technicians using 5 open-ended questions to discover their opinions on design scales relating to the TBP model. By categorizing the technicians’ answers into 3 general concepts, namely behavioral, normative, and control beliefs, the most profuse ideas about each belief were used to design the questions. Then, the initial format of the questionnaire was given to the panel of experts in occupational health, nursing, occupational medicine, ergonomics, health psychology, and health education. So, the ability to understand and the formal validity of questions were first examined by investigating the physical characteristics of questions such as clarity, length of items, meaning of words and sentences, use of specialized vocabulary, etc. In the second step, the content validity indicator (CVI) and content validity ratio (CVR) were calculated by assessing the questions’ necessity, importance, simplicity, and clarity. After determining the indicators, the questionnaire was completed by a sample of 10 technicians twice in 15 days, and the correlation of their answers was used as a test re-test to evaluate the reliability of questions. All personnel participating in the pilot study were banned from attending the final study.
Finally, the theory-related scales included the following cases:
The attitude scale consisted of 18 items. The personnel were asked to express their opinions about each item using a 5-point Likert scale from “1=completely disagree” to “5=completely agree”.
The scale of subjective norms consisted of 7 items in which the personnel were asked to express their opinion about the sentences based on a 5-point Likert scale from “1=not true at all” to “5=absolutely correct”.
The perceived behavioral control scale consisted of 8 items in which the personnel were asked to express their opinion about the sentences based on a 5-point Likert scale from “1=I am not sure at all” to “5=I am completely sure”.
The behavioral intention scale consisted of 3 items in which the personnel were asked to express their opinion about the sentences based on a 5-point Likert scale from “1=completely disagree” to “5=completely agree”.
The self-reporting behavior scale consisted of two items in which personnel were asked to express their opinion about the sentences based on the 5-point Likert scale from “1=never” to “5=always”. The internal consistency of all items was measured using the Cronbach α coefficient, and the reliability of questions was measured by the test re-test coefficient.
Answering the questions took about 30 minutes, and the technicians responded to the questionnaires in the presence of a research team member to ensure an accurate response to questions. Before the study, the research purpose was clearly explained to technicians while coordinating with the medical emergency manager. The technicians were ensured that their answers remained confidential by the research team. All questionnaires were anonymous and without any identification number. The results were generally presented to officials, and the technicians’ responses did not affect their occupational evaluation. All participants in the research signed the written consent forms. After the final phase of the research, the control group was provided with a 1-hour training with purposive training files and pamphlets on introducing chemicals and scene management in accidents.
After evaluating and analyzing the questionnaire results, interviews, and past studies, the training program was provided. It was developed after approval by the panel of experts regarding the importance and relevance of content, amount and complexity of content, order, and relevance of content and goals with the TPB in 4 group training sessions for 60 to 90 minutes. The program was implemented for the experimental group through focus group discussion (8-12 persons per group). Therefore, more focus was provided on attitude change, strengthening positive beliefs, improving self-efficacy, identifying and eliminating barriers, verbal feedback, and individual counseling in designing the educational content and determining the educational strategies. Finally, the educational intervention (Table 1) was implemented for technicians of the experimental group in the Qazvin Medical Emergency Service Center training class.

After face-to-face sessions, a virtual group was established to remind and retrain the classroom content and show educational videos and photos for managing chemical accidents. The mentioned items were continuously and daily reminded through several slides, photos, and short videos. The educational sessions started with a trained occupational health expert lecture about confronting chemical incidents. Then, the issues and problems relating to chemical incidents and scene management were discussed with emergency medical technicians using group discussion, questions and answers, and brainstorming. Finally, the acquired data were inserted into the SPSS software, version 23. The descriptive statistics such as Mean±SD, percentage and frequency along with a paired t-test, chi-square test, and analysis of covariance were analyzed after ensuring the normal distribution of data using the Kolmogorov-Smirnov test.
3. Results
The participants’ Mean±SD age was 35.03±5.57 years, with an age range of 25 and 53 years. In terms of marital status, 82.6% were married. Regarding education, 50.7% had associate degrees, 34.8% were employed in urban centers, and 36.2% in road centers. In terms of field of study, 59.4% were medical emergency graduates. Table 2 presents the characteristics of the samples.

No significant difference was noted between the experimental and control groups regarding their demographic characteristics.
The findings of Table 3 pertain to the psychometric properties of TBP constructs in the present research.
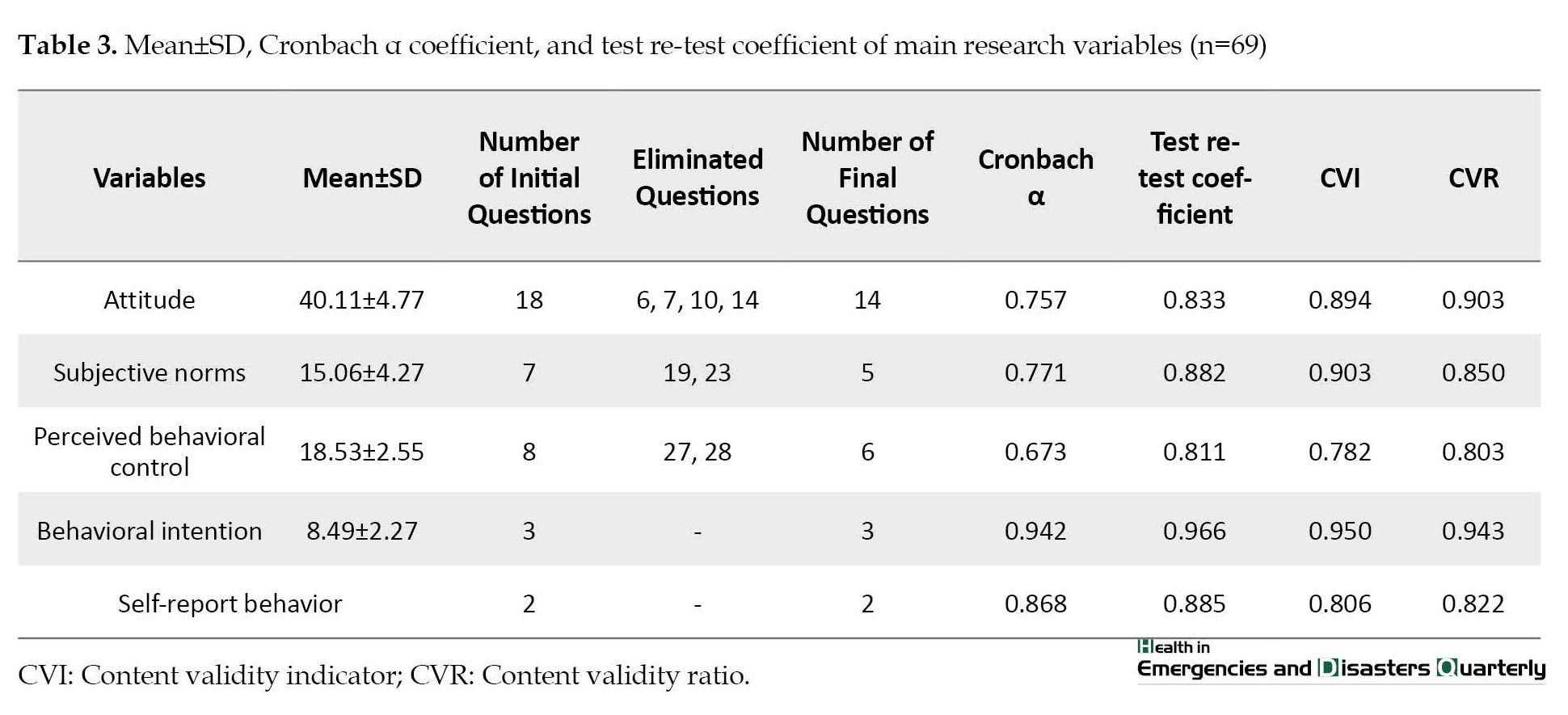
According to the results, all constructs have proper internal consistency and acceptable reliability. The content validity of constructs was also approved using CVR and CVI.
Table 4 presents the Mean±SD of the variables.

According to this table, all variables increased after the intervention in the experiment group. Also, the findings of Table 5 indicate that the difference between the pre-test and post-test scores of the two groups was significant regarding the scores of attitude, subjective norms, and perceived behavioral control (P<0.001).
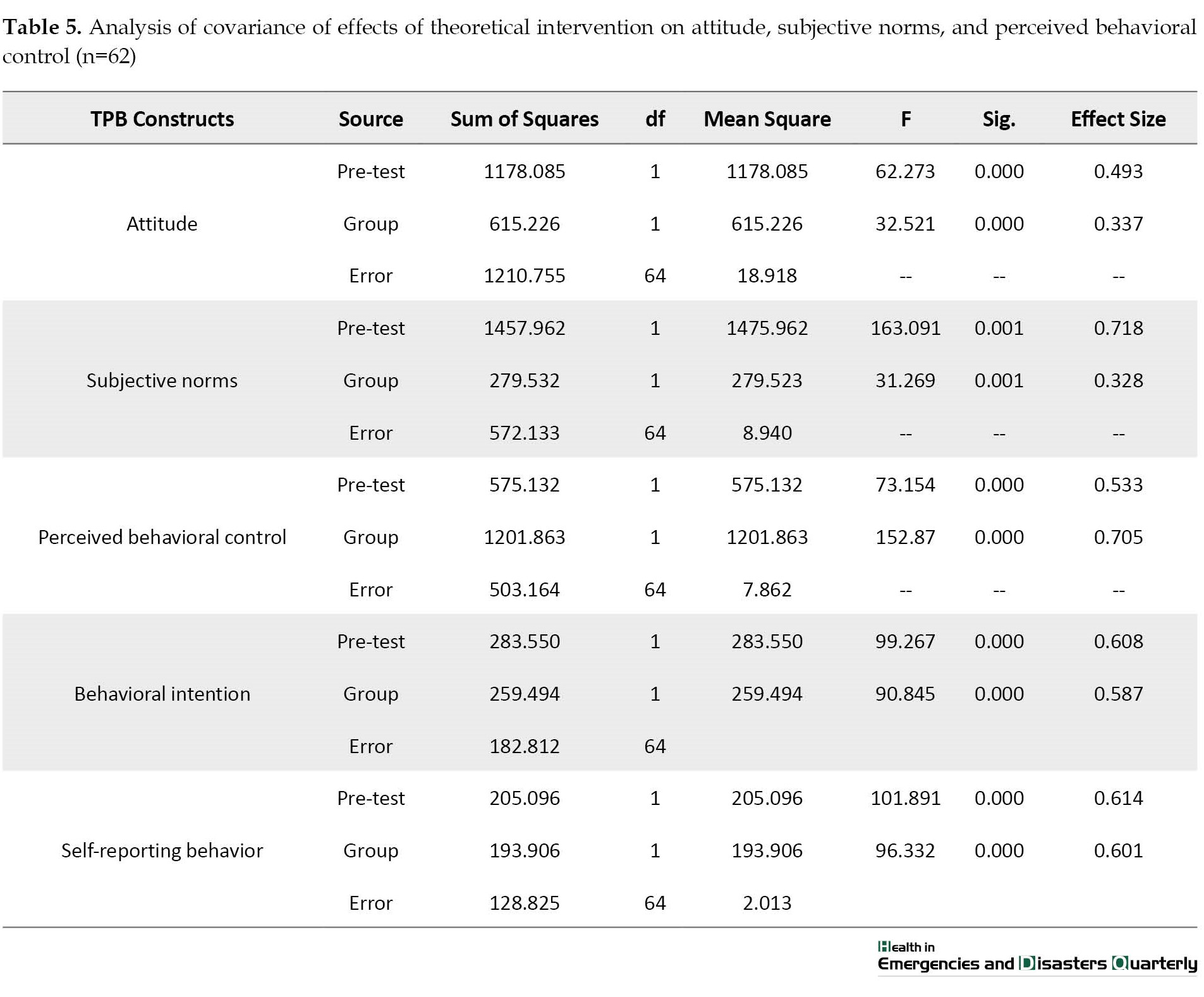
Also, the scores of the experimental group in the dependent variables were significantly higher than the control group (P<0.001). According to Eta squared, theoretical training explained 33.7% of the variance of mean attitude, 32.8% of the variance of mean subjective norms, and 70.5% of the variance of mean perceived behavioral control by emergency personnel to comply with the protocol for dealing with chemical accidents.
Table 5 indicates that the difference between the pre-test and post-test scores of the two groups was significant for the mean behavioral intention and self-report behavior of study participants (P<0.001). The mean score of the experimental group in the dependent variable was also significantly higher than the control group (P<0.001). According to the Eta squared, the theory-based training explained 58.7% of the variance of mean behavioral intention and 60.1% of the mean self-reporting behavior of emergency personnel in compliance with the protocol for dealing with chemical accidents.
Discussion
There was a significant difference between the mean attitude scores before and 2 months after training in the experimental group (P<0.001). However, the mean score of the construct in the control group did not show any significant difference in the two measurements. Studies on predictors of using personal protective equipment indicated that attitude and awareness played decisive roles in the constant use of the equipment. In a Atti et al. study, EMS personnel reported improved performance after receiving chemical incident safety training [20]. In a study by Morrowati et al. on the constructs of protection motivation theory, the “perceived severity” and the “fear” constructs had the maximum and minimum effects on protective behavior, respectively [18].
The finding showed a significant increase in the mean score of subjective norms in the experimental group after the educational intervention in medical emergency service technicians (P<0.001). The change indicates the increased rate of perceived support in medical emergency service technicians in their workplace and life, representing personal protection equipment and doing safety missions in chemical accidents. The findings of Gerard et al.’s study indicate that attitude management directly affects the workers’ attitudes, group norms, and workload. The fact is that workers see managers as controlling individuals. The quality of their work through workplace managers depends on issues like quality versus production and safe operation. In short, the theory of planned behavior is useful in this regard [21]. Therefore, using a participatory ergonomic approach to share knowledge between technicians and management improves problem-solving skills, reduces resistance to change, increases workplace communication, and enhances work motivation. It can strengthen educational interventions and improve the safe performance of medical emergency technicians.
Perceived behavioral control is another component of the TBP. The findings indicated that the mean score of the perceived behavioral control construct increased in the experimental group after the intervention (P<0.001). Since the factors influencing the pre-test behavior were similar in the experimental and control groups, training led to the higher perceived behavioral control in the experimental group by changing the attitudes of technicians and strengthening individual beliefs and values, as well as improving the perception of group and social support by other technicians and officials. Mohammadi et al. indicated that the results of educational intervention based on constructs of TPB could change the knowledge, attitudes, subjective norms, and perceived behavioral control in workers about unsafe behavior and improve their safety performance [22].
Barkhordari et al. calculated the highest rate of unsafe behavior, equal to 43.8%, and the lowest 27.2%. In 9 fields of safety climate, the eighth field (personnel perception of risk), with a score of 4.07, had the lowest score; the fourth field (safety rules and regulations), with a score of 8.05, had the highest score. The research results indicated that the approach to using active (prospective) performance indices could be effective as a suitable tool in evaluating the safety performance of organizations [23].
Hazavehei et al. found that mean scores of workers’ awareness, perceived benefits, and perceived barriers were moderate before the intervention. The performance score was lower than the average. Still, after the educational intervention, the results indicated that the mean scores of awareness, sensitivity, perceived severity, perceived benefits and barriers, and workers’ performance in the case group were significantly greater than in the control group [24]. Pedro et al. found that behavior change was useful for understanding, explaining, and predicting, and they considered a set of relevant structures practical [25]. Ebrahimipour et al. indicated the effectiveness of the theory of planned behavior in predicting the adoption of oral health care in pregnant women [26].
Finally, our findings indicated a significant increase in medical emergency service personnel skills for scene management in chemical accidents after the educational intervention. Results of the above studies suggested that the theory of planned behavior could change employees’ awareness, attitudes, subjective norms, and perceived behavioral control about unsafe behaviors and improve their safety performance, whether the insecure behavior was in the workplace or individual high-risk behaviors. The lack of a significant correlation between subjective norms and behavior may give rise to the mentality that the TPB is not a reasonable model to explain this behavior. However, this theory never indicates that all elements contribute significantly to predicting behavior [27]. The present study revealed that training based on the theory of planned behavior positively affected all theory constructs and changed safe behavior among medical emergency technicians if the theory-based training continued. Recent studies have indicated that training based on the theory of planned behavior helps change the safe behavior in staff because a change in attitude would change the safe behavior.
Conclusion
Results of the present study indicated that an educational intervention based on the theory of planned behavior could change the awareness, attitudes, subjective norms, and perceived behavioral control about skills of medical emergency personnel to manage scenes in chemical accidents and enhance safety in doing their missions. Therefore, we suggested using this behavioral change model in other workplaces and for other occupational behaviors and health risks.
The strengths of the study compared to previous studies were the use of a control group in the research and the use of a detailed educational protocol based on the purpose of the study.
The study’s limitations were the long distance of most emergency medical centers from the training place. To solve this problem, informing and setting the training time in advance and necessary coordination with the officials of the bases was done. Then, there was a possibility of non-participation of the personnel in the training sessions due to the difficulty of the work and fatigue. To solve this problem, a 10% drop was considered in calculating the sample volume.
Ethical Considerations
Compliance with ethical guidelines
The research was approved by the Ethics Committee of Qazvin University of Medical Sciences (Code: IR.QUMS.REC.1397.313).
Funding
The paper was extracted from the Master' s thesis of Mohammadreza Rezaee Ghalee, approved by Department of Health Services Management, Faculty of Health, Qazvin University of Medical Sciences.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
References
Chemical compounds play significant roles in the development of human society [1]. In recent decades, their production and use have significantly increased. As a result, the accidental release of chemicals into the environment might have grown due to industrial incidents, natural disasters, or deliberate terrorist attacks. The explosion of the ammonium nitrate depot in Beirut is an example of such a catastrophe [2].
Despite the magnitude of chemical accidents, there are no centralized and classified general statistics of these accidents worldwide. According to the US Occupational Safety and Health Administration (OSHA), 742000 people die every year due to cancers after exposure to chemical compounds [3]. Iran lacks accurate reports on chemical accidents and their classifications [4]. According to statistics, Iran has been listed among the 5 countries with the highest death toll from accidents in 2017 [5]. Chemical accidents are more critical due to their wide and high diffusion rate [6]. These accidents have multiple domino effects, with widespread casualties, financial loss, and environmental pollution [7]. These accidents, with their high casualties, create an unexpected and sudden demand for medical care, exceeding the normal capacity of service providers and imposing a heavy burden on healthcare systems [8]. In Iran, health and safety inspections in the public sector have been carried out as a control measure for the last 30 years [6].
Studies in the United States indicate that unpreparedness for accidents causes $280 million of damage to its healthcare system every year [9]. Survival rates in chemical accidents are markedly associated with readiness levels, specialized expertise, and coping and control skills of hospital services and prehospital emergency service providers [10].
The Iranian emergency system encompasses two main parts: Prehospital emergency and hospital emergency. Each provides specific time and performance indicators. The prehospital emergency department duty starts by contacting the emergency center and transferring the injured to the hospital emergency department. The care process continues until the stabilization of the injured condition. In each stage, scene management is of great importance. In major chemical accidents, scene management is subject to the proper performance, namely the triage of patients, prompt medical care, and transfer of casualties that, in turn, require the technicians’ functional role to manage the scene [11]. Therefore, active, up-to-date, standard education and health care services are the key to coping with the crisis [12].
Occupational health behavior effectively prevents unsafe performance and manages the incident scene. This concept means providing and maintaining the highest level of mental, physical, and social well-being through risk control, employee-to-job adaptation, and health maintenance [13]. In addition, the staff’s professional and teamwork skills are also determining factors [14].
Technicians show different behaviors in the workplace despite having sufficient awareness. This diversity in actions indicates that other factors besides awareness contribute to technicians’ reporting behavior. Safety climate, risk understanding, and belief increase the probability of success in health promotion interventions in the workplace [15].
According to studies, the most effective training programs are based on theoretical approaches rooted in behavioral change patterns. Using patterns and behavior change theories increases the impact of health training programs and helps identify the effective individual and environmental characteristics [16].
The theory of planned behavior (TPB) is one of the most comprehensive and suitable theories for investigating behavior. The theory was developed by Ajzen and Fishbein in 1980 to predict and explain individual behavior. The theory assumes an individual is a rational performer, so the person processes information before performing a behavior. Individuals’ fundamental beliefs and, consequently, their behavior may change. According to the theory, the main cause of behavior is the intention to do that behavior. Intention is the main index by which individuals can understand how much they want to do something and try to plan a certain behavior. Results of interventional research in Iran using different models and behavior change theories indicated a significant improvement in safe behaviors in workers and other safety groups [17-19].
Apart from a few studies in the field of accident management in Iran, many suffer from various limitations. For instance, a lot of studies have relied on traditional education and overlooked behavior change patterns. Furthermore, they were designed without considering the study’s main purpose and using appropriate models and theories. The other limitations of previous studies were their short follow-up periods, the lack of a control group, and the loss of control over the confounders.
Given the frequency of chemical accidents and their serious consequences, the present study aimed to determine the effect of theoretical-based educational intervention on emergency medical personnel’s skills to manage scenes in chemical accidents.
Materials and Methods
The present research was a quasi-experimental randomized controlled study conducted in Qazvin Province, Iran, from the beginning of February 2018 to the end of August 2019. The statistical population consisted of all emergency medical personnel of Qazvin Province. Among the emergency medical personnel, 70 were selected to participate in the study based on the inclusion and exclusion criteria using the available sampling method. In doing so, a list of all emergency medical personnel working in each emergency medical center was prepared. The centers were then assigned to experimental and control groups. The individuals were selected to participate in the study using a table of random numbers while observing the issue of possible overlap and the likelihood of exposure to control and experimental group personnel. The sample size was equal to 35 for each experimental and control group using G*Power software. We assumed a 95% confidence level, an 80% test power, a 50% impact factor, and a 10% drop estimate. The entry and exit of all technicians to study were voluntary. The control group received no training or intervention until the end of the second phase follow-up.
The inclusion criteria were as follows: At least 22 years of age; operational personnel with a medical degree such as nursing, medical emergency, anesthesia, or operating room; at least 2 years of experience in a prehospital emergency and operation unit; and working in one of urban, rural and air centers of Qazvin Province. The exclusion criteria were as follows: Retirement of medical emergency personnel during the study, non-participation of personnel in training classes, working in emergency centers of other provinces, and not providing the consent form.
After initial coordination with the Qazvin University of Medical Sciences and obtaining a research permit and submitting it to Qazvin Medical Emergency Center, technicians of the experimental and control groups were invited to complete the study questionnaires and participate in training classes with prior notice from the training unit. The study data were collected using self-report questionnaires in experimental and control groups before and two months after the theory-based intervention. Data collection tools were as follows.
We used a demographic questionnaire that collected information regarding age, marital status, education level, field of study, job, work experience, and history of exposure to chemical accidents.
A scale assessed the theory of planned behavior (TPB). First, while reviewing previous studies, a quasi-in-depth interview was conducted with 10 medical emergency technicians using 5 open-ended questions to discover their opinions on design scales relating to the TBP model. By categorizing the technicians’ answers into 3 general concepts, namely behavioral, normative, and control beliefs, the most profuse ideas about each belief were used to design the questions. Then, the initial format of the questionnaire was given to the panel of experts in occupational health, nursing, occupational medicine, ergonomics, health psychology, and health education. So, the ability to understand and the formal validity of questions were first examined by investigating the physical characteristics of questions such as clarity, length of items, meaning of words and sentences, use of specialized vocabulary, etc. In the second step, the content validity indicator (CVI) and content validity ratio (CVR) were calculated by assessing the questions’ necessity, importance, simplicity, and clarity. After determining the indicators, the questionnaire was completed by a sample of 10 technicians twice in 15 days, and the correlation of their answers was used as a test re-test to evaluate the reliability of questions. All personnel participating in the pilot study were banned from attending the final study.
Finally, the theory-related scales included the following cases:
The attitude scale consisted of 18 items. The personnel were asked to express their opinions about each item using a 5-point Likert scale from “1=completely disagree” to “5=completely agree”.
The scale of subjective norms consisted of 7 items in which the personnel were asked to express their opinion about the sentences based on a 5-point Likert scale from “1=not true at all” to “5=absolutely correct”.
The perceived behavioral control scale consisted of 8 items in which the personnel were asked to express their opinion about the sentences based on a 5-point Likert scale from “1=I am not sure at all” to “5=I am completely sure”.
The behavioral intention scale consisted of 3 items in which the personnel were asked to express their opinion about the sentences based on a 5-point Likert scale from “1=completely disagree” to “5=completely agree”.
The self-reporting behavior scale consisted of two items in which personnel were asked to express their opinion about the sentences based on the 5-point Likert scale from “1=never” to “5=always”. The internal consistency of all items was measured using the Cronbach α coefficient, and the reliability of questions was measured by the test re-test coefficient.
Answering the questions took about 30 minutes, and the technicians responded to the questionnaires in the presence of a research team member to ensure an accurate response to questions. Before the study, the research purpose was clearly explained to technicians while coordinating with the medical emergency manager. The technicians were ensured that their answers remained confidential by the research team. All questionnaires were anonymous and without any identification number. The results were generally presented to officials, and the technicians’ responses did not affect their occupational evaluation. All participants in the research signed the written consent forms. After the final phase of the research, the control group was provided with a 1-hour training with purposive training files and pamphlets on introducing chemicals and scene management in accidents.
After evaluating and analyzing the questionnaire results, interviews, and past studies, the training program was provided. It was developed after approval by the panel of experts regarding the importance and relevance of content, amount and complexity of content, order, and relevance of content and goals with the TPB in 4 group training sessions for 60 to 90 minutes. The program was implemented for the experimental group through focus group discussion (8-12 persons per group). Therefore, more focus was provided on attitude change, strengthening positive beliefs, improving self-efficacy, identifying and eliminating barriers, verbal feedback, and individual counseling in designing the educational content and determining the educational strategies. Finally, the educational intervention (Table 1) was implemented for technicians of the experimental group in the Qazvin Medical Emergency Service Center training class.
After face-to-face sessions, a virtual group was established to remind and retrain the classroom content and show educational videos and photos for managing chemical accidents. The mentioned items were continuously and daily reminded through several slides, photos, and short videos. The educational sessions started with a trained occupational health expert lecture about confronting chemical incidents. Then, the issues and problems relating to chemical incidents and scene management were discussed with emergency medical technicians using group discussion, questions and answers, and brainstorming. Finally, the acquired data were inserted into the SPSS software, version 23. The descriptive statistics such as Mean±SD, percentage and frequency along with a paired t-test, chi-square test, and analysis of covariance were analyzed after ensuring the normal distribution of data using the Kolmogorov-Smirnov test.
3. Results
The participants’ Mean±SD age was 35.03±5.57 years, with an age range of 25 and 53 years. In terms of marital status, 82.6% were married. Regarding education, 50.7% had associate degrees, 34.8% were employed in urban centers, and 36.2% in road centers. In terms of field of study, 59.4% were medical emergency graduates. Table 2 presents the characteristics of the samples.
No significant difference was noted between the experimental and control groups regarding their demographic characteristics.
The findings of Table 3 pertain to the psychometric properties of TBP constructs in the present research.
According to the results, all constructs have proper internal consistency and acceptable reliability. The content validity of constructs was also approved using CVR and CVI.
Table 4 presents the Mean±SD of the variables.
According to this table, all variables increased after the intervention in the experiment group. Also, the findings of Table 5 indicate that the difference between the pre-test and post-test scores of the two groups was significant regarding the scores of attitude, subjective norms, and perceived behavioral control (P<0.001).
Also, the scores of the experimental group in the dependent variables were significantly higher than the control group (P<0.001). According to Eta squared, theoretical training explained 33.7% of the variance of mean attitude, 32.8% of the variance of mean subjective norms, and 70.5% of the variance of mean perceived behavioral control by emergency personnel to comply with the protocol for dealing with chemical accidents.
Table 5 indicates that the difference between the pre-test and post-test scores of the two groups was significant for the mean behavioral intention and self-report behavior of study participants (P<0.001). The mean score of the experimental group in the dependent variable was also significantly higher than the control group (P<0.001). According to the Eta squared, the theory-based training explained 58.7% of the variance of mean behavioral intention and 60.1% of the mean self-reporting behavior of emergency personnel in compliance with the protocol for dealing with chemical accidents.
Discussion
There was a significant difference between the mean attitude scores before and 2 months after training in the experimental group (P<0.001). However, the mean score of the construct in the control group did not show any significant difference in the two measurements. Studies on predictors of using personal protective equipment indicated that attitude and awareness played decisive roles in the constant use of the equipment. In a Atti et al. study, EMS personnel reported improved performance after receiving chemical incident safety training [20]. In a study by Morrowati et al. on the constructs of protection motivation theory, the “perceived severity” and the “fear” constructs had the maximum and minimum effects on protective behavior, respectively [18].
The finding showed a significant increase in the mean score of subjective norms in the experimental group after the educational intervention in medical emergency service technicians (P<0.001). The change indicates the increased rate of perceived support in medical emergency service technicians in their workplace and life, representing personal protection equipment and doing safety missions in chemical accidents. The findings of Gerard et al.’s study indicate that attitude management directly affects the workers’ attitudes, group norms, and workload. The fact is that workers see managers as controlling individuals. The quality of their work through workplace managers depends on issues like quality versus production and safe operation. In short, the theory of planned behavior is useful in this regard [21]. Therefore, using a participatory ergonomic approach to share knowledge between technicians and management improves problem-solving skills, reduces resistance to change, increases workplace communication, and enhances work motivation. It can strengthen educational interventions and improve the safe performance of medical emergency technicians.
Perceived behavioral control is another component of the TBP. The findings indicated that the mean score of the perceived behavioral control construct increased in the experimental group after the intervention (P<0.001). Since the factors influencing the pre-test behavior were similar in the experimental and control groups, training led to the higher perceived behavioral control in the experimental group by changing the attitudes of technicians and strengthening individual beliefs and values, as well as improving the perception of group and social support by other technicians and officials. Mohammadi et al. indicated that the results of educational intervention based on constructs of TPB could change the knowledge, attitudes, subjective norms, and perceived behavioral control in workers about unsafe behavior and improve their safety performance [22].
Barkhordari et al. calculated the highest rate of unsafe behavior, equal to 43.8%, and the lowest 27.2%. In 9 fields of safety climate, the eighth field (personnel perception of risk), with a score of 4.07, had the lowest score; the fourth field (safety rules and regulations), with a score of 8.05, had the highest score. The research results indicated that the approach to using active (prospective) performance indices could be effective as a suitable tool in evaluating the safety performance of organizations [23].
Hazavehei et al. found that mean scores of workers’ awareness, perceived benefits, and perceived barriers were moderate before the intervention. The performance score was lower than the average. Still, after the educational intervention, the results indicated that the mean scores of awareness, sensitivity, perceived severity, perceived benefits and barriers, and workers’ performance in the case group were significantly greater than in the control group [24]. Pedro et al. found that behavior change was useful for understanding, explaining, and predicting, and they considered a set of relevant structures practical [25]. Ebrahimipour et al. indicated the effectiveness of the theory of planned behavior in predicting the adoption of oral health care in pregnant women [26].
Finally, our findings indicated a significant increase in medical emergency service personnel skills for scene management in chemical accidents after the educational intervention. Results of the above studies suggested that the theory of planned behavior could change employees’ awareness, attitudes, subjective norms, and perceived behavioral control about unsafe behaviors and improve their safety performance, whether the insecure behavior was in the workplace or individual high-risk behaviors. The lack of a significant correlation between subjective norms and behavior may give rise to the mentality that the TPB is not a reasonable model to explain this behavior. However, this theory never indicates that all elements contribute significantly to predicting behavior [27]. The present study revealed that training based on the theory of planned behavior positively affected all theory constructs and changed safe behavior among medical emergency technicians if the theory-based training continued. Recent studies have indicated that training based on the theory of planned behavior helps change the safe behavior in staff because a change in attitude would change the safe behavior.
Conclusion
Results of the present study indicated that an educational intervention based on the theory of planned behavior could change the awareness, attitudes, subjective norms, and perceived behavioral control about skills of medical emergency personnel to manage scenes in chemical accidents and enhance safety in doing their missions. Therefore, we suggested using this behavioral change model in other workplaces and for other occupational behaviors and health risks.
The strengths of the study compared to previous studies were the use of a control group in the research and the use of a detailed educational protocol based on the purpose of the study.
The study’s limitations were the long distance of most emergency medical centers from the training place. To solve this problem, informing and setting the training time in advance and necessary coordination with the officials of the bases was done. Then, there was a possibility of non-participation of the personnel in the training sessions due to the difficulty of the work and fatigue. To solve this problem, a 10% drop was considered in calculating the sample volume.
Ethical Considerations
Compliance with ethical guidelines
The research was approved by the Ethics Committee of Qazvin University of Medical Sciences (Code: IR.QUMS.REC.1397.313).
Funding
The paper was extracted from the Master' s thesis of Mohammadreza Rezaee Ghalee, approved by Department of Health Services Management, Faculty of Health, Qazvin University of Medical Sciences.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
References
- Peña Fernández A. [Presencia y distribución medioambiental de metales pesados y metaloides en Alcalá de Henares, Madrid. Evaluación del riesgo para la población y biomonitorización de la población escolar (Spanish)] [PhD dissertation]. Spain: Universidad de Alcalá; 2011. [Link]
- Pasman HJ, Fouchier C, Park S, Quddus N, Laboureur D. Beirut ammonium nitrate explosion: Are not we really learning anything? Process Safety Progress. 2020; 39(4):e12203. [DOI:10.1002/prs.12203]
- Kalatpour O. Industrial chemical incident management. Tehran: Torfeh International Group, Hak Publications; 2016. [Link]
- Kako M, Hammad K, Mitani S, Arbon P. Existing approaches to Chemical, Biological, Radiological, And Nuclear (CBRN) education and training for health professionals: Findings from an integrative literature review. Prehospital and Disaster Medicine. 2018; 33(2):182-90. [DOI:10.1017/S1049023X18000043] [PMID]
- Nakhaei M, Tabiee S, Saadatjou S A, SabzehKar F. [The effect of educational intervention on nurses' preparedness in emergencies and disasters (Persian)]. Journal of Birjand University of Medical Sciences. 2019; 26(3):237-48. [DOI:10.32592/JBirjandUnivMedSci.2019.26.3.105]
- Abbasi H, Dehghani A, Mohammadi AA, Ghadimi T, Keshavarzi A. The epidemiology of chemical burns among the patients referred to burn centers in Shiraz, Southern Iran, 2008–2018. Bulletin of Emergency & Trauma. 2021; 9(4):195-200. [DOI:10.30476/beat.2021.90754.1261] [PMID] [PMCID]
- Wang J, Fu G, Yan M. Investigation and analysis of a hazardous chemical accident in the process industry: Triggers, roots, and lessons learned. Processes. 2020; 8(4):477. [DOI:10.3390/pr8040477]
- Ben-Ishay O, Mitaritonno M, Catena F, Sartelli M, Ansaloni L, Kluger Y. Mass casualty incidents - time to engage. World Journal of Emergency Surgery. 2016; 11(1):8. [DOI:10.1186/s13017-016-0064-7] [PMID] [PMCID]
- Martin AJ, Lohse CM, Sztajnkrycer MD. A Descriptive analysis of prehospital response to hazardous materials events. Prehospital and Disaster Medicine. 2015; 30(5):466-71. [DOI:10.1017/S1049023X1500504X] [PMID]
- van der Woude I, de Cock JS, Bierens JJ, Christiaanse JC. TAP CBRN preparedness: Knowledge, training and networks. Prehospital and Disaster Medicine. 2008; 23(4):s65-9. [DOI:10.1017/S1049023X00021270] [PMID]
- Khoury A, Halberthal M, Hymes G, Utitz L, Reisner SM, Mosheiff R, Liebergal M. Civilian hospital role in Mass Casualty Event (MCE). In: Wolfson N, Lerner A, Roshal L, editors. Orthopedics in Disasters. Berlin: Springer; 2016. [DOI:10.1007/978-3-662-48950-5_7]
- Parga CJ. Very high temperature measurements: Applications to nuclear reactor safety tests; mesures des tres hautes temperatures: Applications a des essais de surete des reacteurs nucleaires [PhD dissertation]. Idaho: University of Idaho; 2013. [Link]
- Moradhaseli S, Ataei P, Van den Broucke S, Karimi H. The process of farmers' occupational health behavior by health belief model: Evidence from Iran. Journal of Agromedicine. 2021; 26(2):231-44. [DOI:10.1080/1059924X.2020.1837316] [PMID]
- Latif M, Abbasi M, Momenian S. The effect of educating confronting accidents and disasters on the improvement of nurses’ professional competence in response to the crisis. Health in Emergencies and Disasters Quarterly. 2019; 4(3):147-56. [DOI:10.32598/hdq.4.3.147]
- Fakhri A, Morshedi H, Zeidi IM. Effect of an educational intervention based on the theory of planned behavior on the use of hearing protection devices (Persian)]. Scientific Journal of Kurdistan University of Medical Sciences. 2017; 22(2):80-95. [DOI:10.22102/22.2.80]
- Tehrani H, Majlessi F, Shojaeizadeh D, Sadeghi R, Hasani Kabootarkhani M. Applying socioecological model to improve women's physical activity: A randomized control trial. Iranian Red Crescent Medical Journal. 2016; 18(3):e21072. [DOI:10.5812/ircmj.21072] [PMID] [PMCID]
- Loukzadeh Z, Mehrparvar A, Shojaaddini Ardekani A, Nabi Meybodi R. [Evaluation of effective factors of hearing protection use in tile workers (Persian)]. Tibbi-i-kar. 2011; 3(1):8-13. [Link]
- Morowatisharifabad M, Hadi varnamkhavasti L, Zare M, Fallahzadeh H, Karimiankakolaki Z. [Study of determinants of lung cancer protective behaviors in Esfahan Steel Company workers based on protection motivation theory (Persian)]. Jurnal of Toloo-e-behdasht. 2017; 16(3):67-80. [Link]
- Cook S, McSween TE. The role of supervisors in behavioral safety observations. Professional Safety. 2000; 45(10):33-6. [Link]
- Atti SK, Miles W, Moran T, Kazzi Z. Emergency medical services: An Under-Utilized Group for improved chemical security surveillance? Journal of Chemical Education. 2020; 97(7):1764-68. [DOI:10.1021/acs.jchemed.9b00971]
- Fogarty GJ, Shaw A. Safety climate and the theory of planned behavior: Towards the prediction of unsafe behavior. Accident Analysis & Prevention. 2010; 42(5):1455-9. [DOI:10.1016/j.aap.2009.08.008] [PMID]
- Zeidi IM, Hajiaghaye AP, Zeidi BM. [Investigating the effect of education based on the theory of planned behavior on employee safety behaviors (Persian)]. Knowledge and Health in Basic Medical Sciences. 2013; 8(3):105-11. [DOI:10.22100/jkh.v8i3.24]
- Barkhordari A, Dehghani A, Kianfar A, Mahmoudi S, Aminifard F. [Safety performance evaluation using proactive indicators in a selected industry (Persian)]. Journal of Occupational Hygiene Engineering. 2015; 1(4):49-59. [Link]
- Hazavehei S, Shadzi S, Asgari T, Pourabdian S, Hasanzadeh A. [The effect of safety education based on Health Belief Model (HBM) on the workers practice of Borujen Industrial Town in using the personal protection respiratory equipments (Persian)]. Iran Occupational Health. 2008; 5(1 and 2):21-30. [Link]
- Teixeira PJ, Marques MM. Health behavior change for obesity management. Obesity Facts. 2017; 10(6):666-73. [DOI:10.1159/000484933] [PMID] [PMCID]
- Ebrahimipour H, Mohamadzadeh M, Niknami S, Ismaili H, Vafaii Najjar A. [Predictors of oral health care in pregnant women based on theory of planned behavior (Persian)]. Journal of Health System Research. 2015; 11(3):496-504. [Link]
- Mohahammadi-Zeidi I, Khalaj M, Mohahammadi-Zeidi B. [Assessing the readiness of assembly line workers to adopt the upright posture (Persian)]. Journal of Inflammatory Diseases. 2012; 15(4):77-85. [Link]
Type of Study: Research |
Subject:
Emergency
Received: 2023/04/3 | Accepted: 2023/06/27 | Published: 2023/09/11
Received: 2023/04/3 | Accepted: 2023/06/27 | Published: 2023/09/11
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Health in Emergencies and Disasters Quarterly
Health in Emergencies & Disasters Research Center, University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave, Tehran, Iran.
Journal Tel: +9821 71732816 (2816)
Publisher Tel: +9821 4535 5555 - 4535 5000
