

Volume 9, Issue 2 (Winter 2024)
Health in Emergencies and Disasters Quarterly 2024, 9(2): 99-106 |
Back to browse issues page


Ethics code: IR.NUMS.REC.1400.030
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Raiati R, Khorashadizadeh F, Hosseini S S, Malekan F, Samghani A, Ghodsi H. Identifying the Barriers to Performing Dispatcher-assisted Bystander Cardiopulmonary Resuscitation in Out-of-hospital Cardiac Arrest. Health in Emergencies and Disasters Quarterly 2024; 9 (2) :99-106
URL: http://hdq.uswr.ac.ir/article-1-543-en.html
URL: http://hdq.uswr.ac.ir/article-1-543-en.html
Roohollah Raiati1 

 , Fatemeh Khorashadizadeh2 , Somayeh Sadat Hosseini3 , Fatemeh Malekan3 , Ameneh Samghani3 , Hasan Ghodsi * 4
, Fatemeh Khorashadizadeh2 , Somayeh Sadat Hosseini3 , Fatemeh Malekan3 , Ameneh Samghani3 , Hasan Ghodsi * 4
, Fatemeh Khorashadizadeh2 , Somayeh Sadat Hosseini3 , Fatemeh Malekan3 , Ameneh Samghani3 , Hasan Ghodsi * 4
1- Pre-Hospital Emergency Medical Services and Disaster Management Center, Neyshabur University of Medical Sciences, Neyshabur, Iran.
2- Department of Biostatistics, Faculty of Health, Neyshabur University of Medical Sciences, Neyshabur, Iran.
3- Department of Medical Emergencies, School of Nursing and Midwifery, Neyshabur University of Medical Sciences, Neyshabur, Iran.
4- Department of Medical Emergencies, School of Nursing and Midwifery, Neyshabur University of Medical Sciences, Neyshabur, Iran. , ghodsih1@nums.ac.ir
2- Department of Biostatistics, Faculty of Health, Neyshabur University of Medical Sciences, Neyshabur, Iran.
3- Department of Medical Emergencies, School of Nursing and Midwifery, Neyshabur University of Medical Sciences, Neyshabur, Iran.
4- Department of Medical Emergencies, School of Nursing and Midwifery, Neyshabur University of Medical Sciences, Neyshabur, Iran. , ghodsih1@nums.ac.ir
Keywords: Out-of-hospital cardiac arrest, Cardiopulmonary resuscitation, Dispatcher-assisted cardiopulmonary resuscitation
Full-Text [PDF 580 kb]
(125 Downloads)
| Abstract (HTML) (865 Views)
Full-Text: (43 Views)
Introduction
Cardiopulmonary resuscitation (CPR) is a process performed to restore the activity of the heart, brain, and lungs in order to prevent sudden death and save people in cardiopulmonary arrest [1, 2]. In general, the survival rate in cases of in-hospital cardiac arrest (IHCA) in Western countries is less than 20%, and this rate is reported to be 17%-31% in the US. However, this rate is reported to be about 10% in cases of out-of-hospital cardiac arrest (OHCA) [2-4].
The first line of CPR and response to cardiac arrest is basic life support (BLS), which is the key part of saving lives, resulting in reducing the mortality rate and increasing the hospital discharge rate following cardiac arrest [3]. Without a qualified BLS, advanced cardiac life support (ALS) interventions will be ineffective. The main factors of BLS include recognizing cardiopulmonary arrest, activating the emergency system, initiating effective and quality CPR as soon as possible, and safely using an automated external defibrillator (AED) [3, 5].
Although the golden time to survive a person after cardiac arrest is 4 to 6 minutes, and the best outcome in patients with cardiopulmonary arrest is when basic resuscitation measures are started in the first 4 minutes [6], in most cases, the arrival of emergency medical technicians (EMTs) at the patient’s bedside takes more than this time. Therefore, a solution must be provided to initiate initial resuscitation interventions before emergency medical services (EMSs) arrive. One of these solutions is training the public in basic resuscitation interventions, which organizations such as the Red Crescent carry out. Another solution is training emergency callers in basic resuscitation interventions by the dispatcher of the Emergency Communications Center (ECC). This measure, named dispatcher-assisted bystander CPR (DA-BCPR), has explicitly been emphasized by the 2015 guideline of the American Heart Association (AHA) and the European Resuscitation Council [7, 8, 9, 10].
Pre-arrival instructions have been used for the first time in US EMS. Based on this protocol, the dispatcher asks the caller critical questions about the patient’s condition and, if necessary, offers advice and guidance until the ambulance arrives [11].
Some studies have also evaluated the association between DA-BCPR and ambulance response time. It has been found that DA-BCPR improves the survival of patients with OHCA despite delays in ambulance response time, emphasizing the importance of DA-BCPR in improving the survival of victims while waiting for an ambulance [12-14]. Several observational studies have also reported that DA-BCPR is associated with favorable neurological outcomes in patients with OHCA [15-17].
However, some studies have shown a low rate of performing CPR by bystanders [10, 18]. For example, a low rate of DA-BCPR has been reported in Iran [19]. Some barriers to performing BCPR include fear of infections, fear of harming the patient, legal concerns, and lack of previous CPR training [19-22].
Investigating the barriers to performing BLS procedures in OHCA patients can provide valuable information to strengthen the chain of survival and improve patient prognosis. This study aimed to identify barriers to performing DA-BCPR in OHCA patients.
Materials and Methods
Study setting
EMS in Iran was established in 1974 and managed by the Ministry of Health and Medical Education. Access to EMSs anywhere in the country is possible through calling 115, which provides free services to people since the government finances it. All 115 call-receiving employees are nurses or emergency medical technicians, the medical telephone consultants are physicians, and the dispatch operators are intermediate emergency medicine technicians or nurses. All ambulances are equipped with defibrillators to provide BLS. In 2018, a DA-BCPR program was initiated in Iran. The dispatcher asks two key questions to detect OHCA (following the 2010 AHA guidelines): Altered mental status and abnormal breathing. If the caller answers “yes” to both questions, the dispatcher will recommend standard CPR instruction to the caller. At the same time, the dispatcher sends information to the nearest ambulance station using the ASAYAR application. Until the ambulance arrives at the address, the dispatcher or physician supports bystanders by talking on the phone.
Study design and data collection
This cross-sectional study was conducted in two phases. In the first phase, the researcher reviewed dispatch audio recordings at the Neyshabur EMS Dispatch Center, Neyshabur City, Iran, from June 2022 to June 2023 and selected all records related to OHCA. The reviews of these records were targeted at DA-BCPR. Cases due to trauma and those without receiving dispatch assistance for CPR were excluded. Then, data related to each DA-BCPR were collected from retrospective medical records in EMSs and hospitals. Trained medical record reviewers extracted these records. In the second phase, the researchers contacted bystanders in each OHCA who called EMS and received additional data. For data gathering, we used a researcher-made questionnaire consisting of demographic data (age and gender of patients and their bystanders, education, and relation of bystanders with the patients, and the place of CPR) and specific questions (the bystander CPR experience, reasons for refusal to perform CPR, and the actions performed by a bystander). The instrument’s validity was confirmed by 7 university faculty members and 4 emergency medicine specialists (content validity ratio [CVR]=0.78 and content validity index [CVI]=0.84). Also, its reliability was confirmed by the test re-test method with a coefficient of 90% and considering a sample size of 15 people.
In addition, the chi-square and Fisher exact tests were used to determine the relationship between study variables. All statistical analyses were performed using R software, version 4.0.1 at P≤0.05.
Results
Among 391 EMS-assessed OHCA cases, we excluded patients with traumatic OHCA (n=31, 7.92%) and those who were not recommended for CPR by a dispatcher because the diagnosis of OHCA was not confirmed by a qualified person or medical staff (n=209, 58.05%). A total of 151 OHCA cases were included in this final analysis (Figure 1).
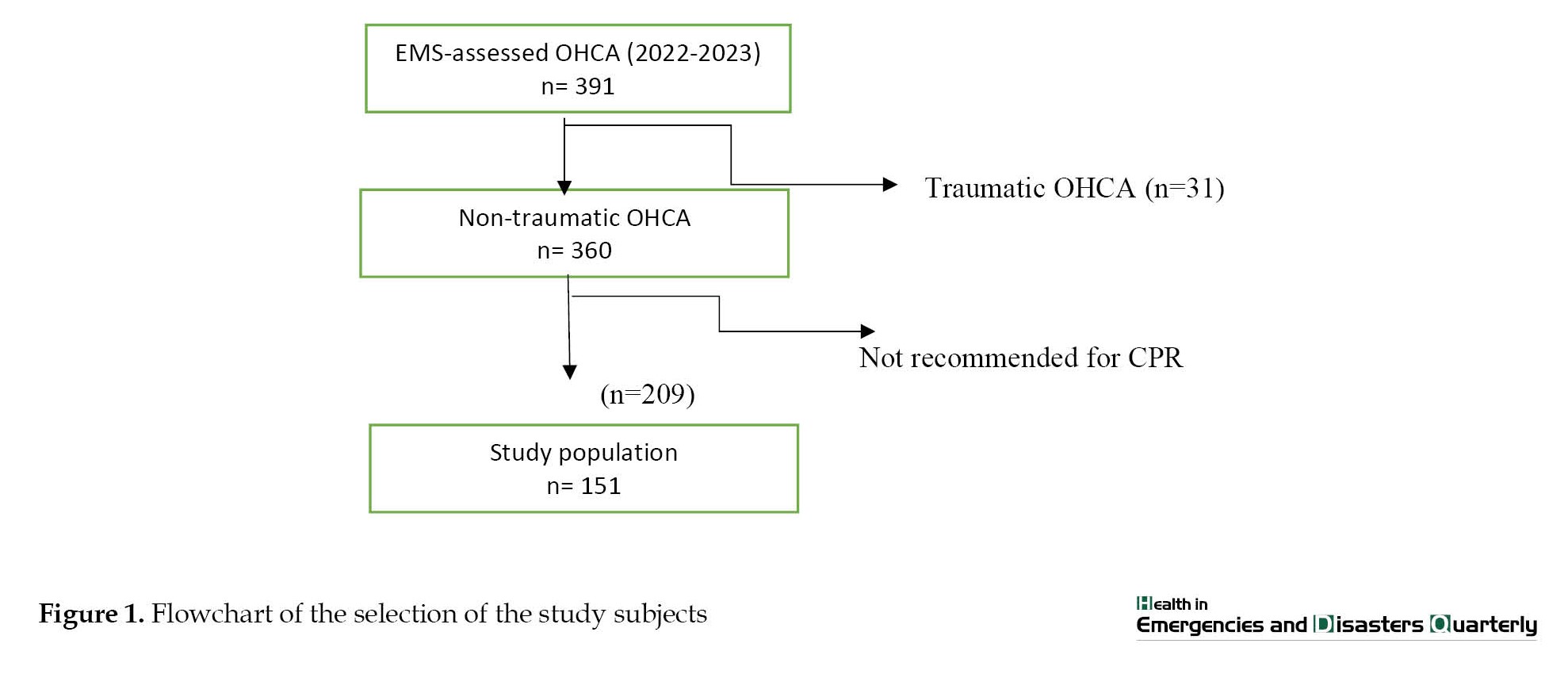 Of 151 eligible patients, DA-BCPR was provided to 125(84.46%).
Of 151 eligible patients, DA-BCPR was provided to 125(84.46%).
Patients’ and bystanders’ characteristics
Of 151 OHCA patients included in this study, most were males (70.27%), aged 50 years and older (81.08%), with a median age of 70 years (interquartile range=55-80 y). Most collapsed out of their homes (80.45%) and received OHCA in urban areas (70.20%).
The Mean±SD age of bystanders was 39.47±10.33 years; 51 bystanders (38.35%) had received CPR training, and only 10.53% of them experienced presumed cardiac arrest. The review of the audio records showed that of the bystanders, 86 cases (68.80%) performed CPR with only one request from the dispatcher; however, they rarely recognized pulselessness. Most patients (89.39%) did not receive mouth-to-mouth breathing.
The median response time interval was 9.21 min (±4.58). In 104 OHCA cases (68.9%), the arrival time was less than 6 minutes. In 31(20.5%), it was 6-10 minutes; in 16(10.6%), it was more than 10 minutes.
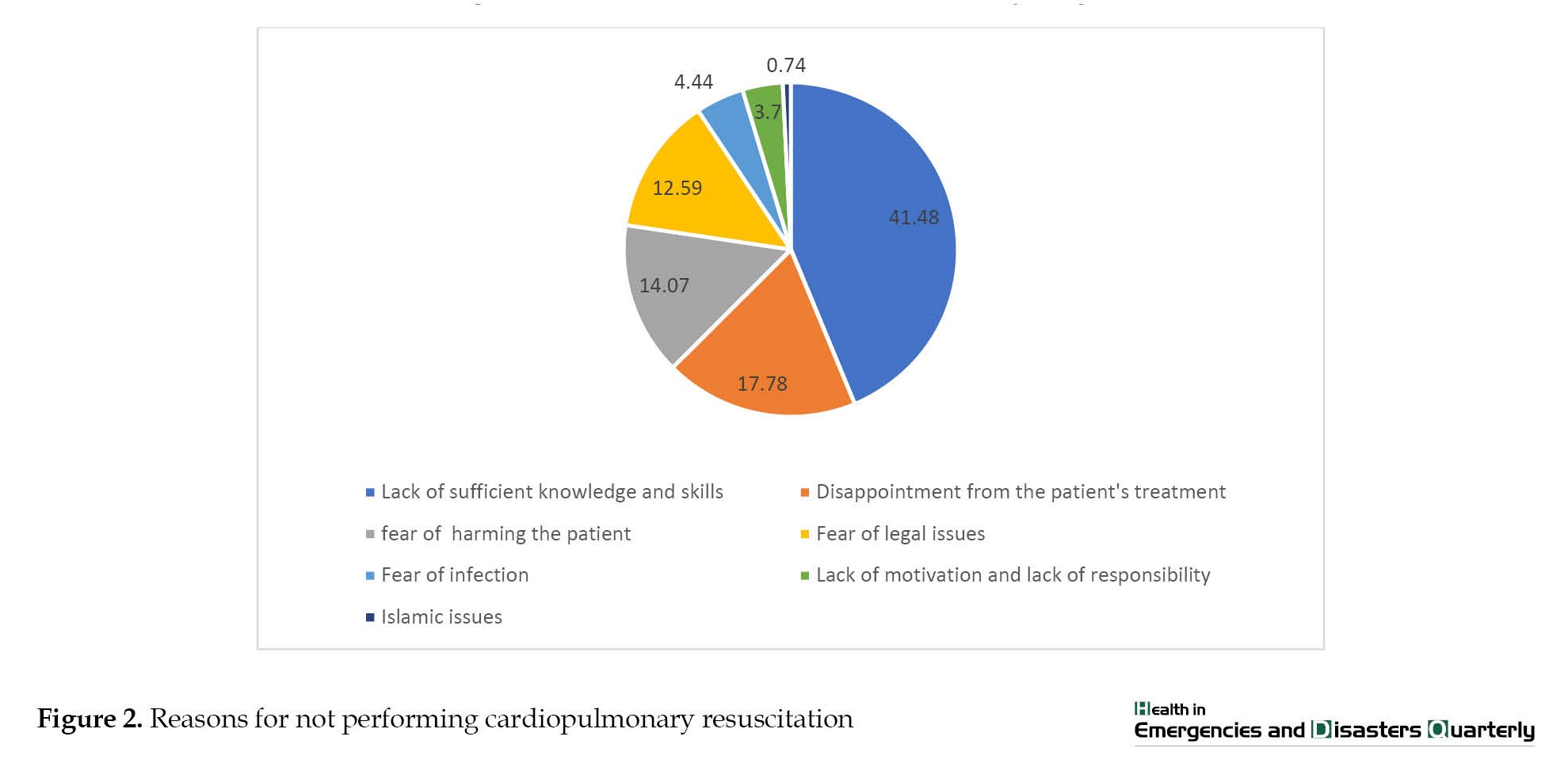
Of the bystanders who did not provide CPR, most (41.48%) indicated their “insufficient knowledge and skills” followed by “disappointment from the patient’s treatment” (17.78%) as the main barriers to performing CPR (Figure 2).
 The Fisher exact test showed a statistically significant relationship between the callers’ familiarity with CPR and performing CPR (Table 1).
The Fisher exact test showed a statistically significant relationship between the callers’ familiarity with CPR and performing CPR (Table 1).
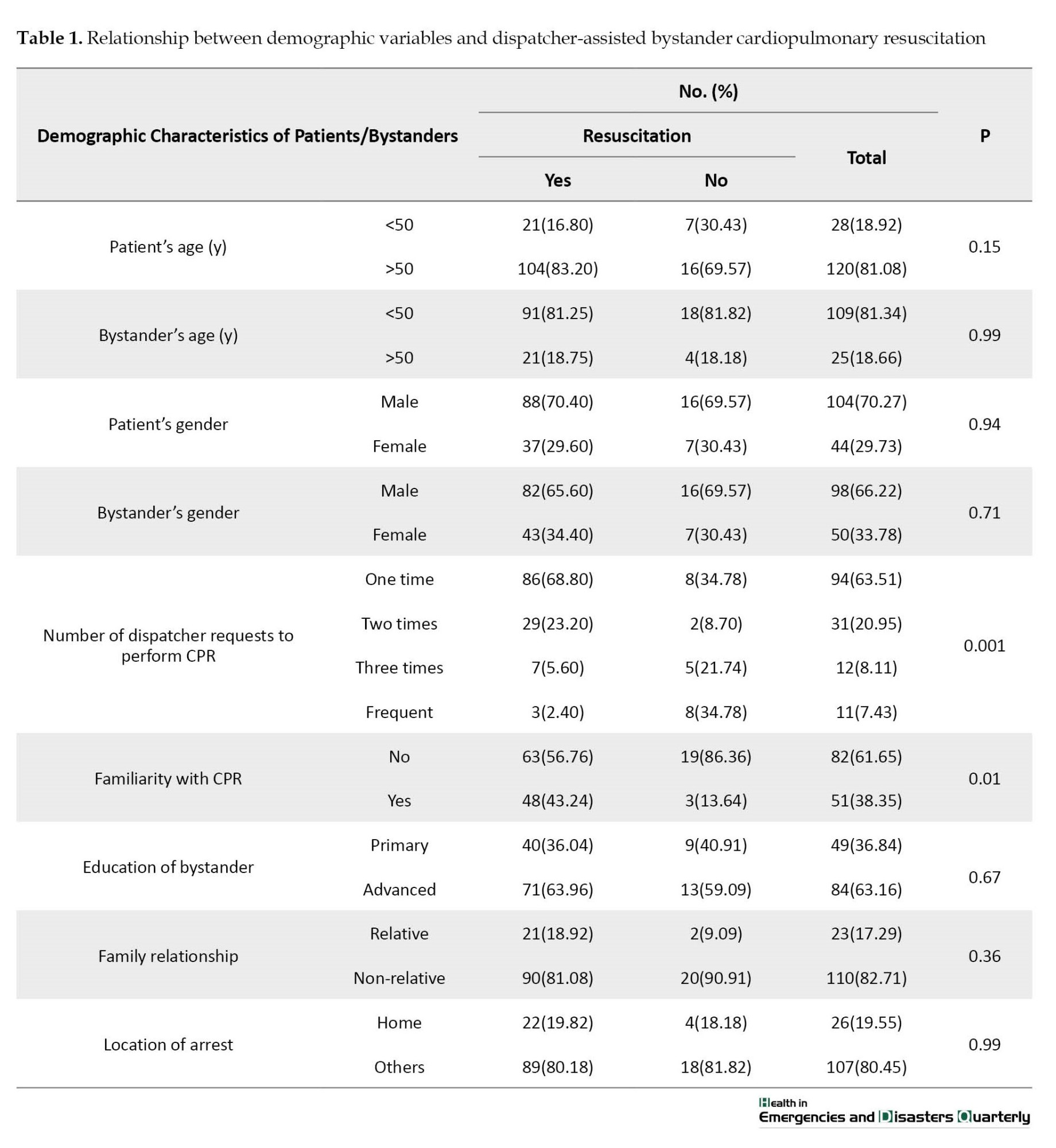
In other words, bystanders who had previously received CPR training had a greater chance of performing DA-BCPR. Other factors, such as the age and gender of patients; age, gender, and education of bystanders; and the number of dispatcher requests to perform CPR, were influential in performing CPR.
Of 151 OHCA patients, 139(92.05%) died on the scene or before arrival at the hospital, and only 12(7.95%) returned to spontaneous circulation before hospital arrival. Of 151 bystanders, only 51(38.35%) had previous CPR training.
Discussion
This study showed two main factors for not performing DA-BCPR in OHCA: Not recognizing cardiac arrest and the lack of knowledge on performing CPR. This finding indicates the importance of training non-specialists and dispatchers in identifying cardiac arrest.
Since the diagnosis of cardiac arrest is difficult for non-specialists, in the new training program, it should be emphasized that CPR should be started when noticing agonal gasping or unusual breathing. Additionally, dispatcher training for DA-BCPR should be prioritized. Dispatchers should identify cardiac arrest based on information from callers and provide appropriate instructions for chest compression over the call.
The rate of DA-BCPR in this study was higher than in other studies [16, 19, 23, 24]. Still, the rates of the return to spontaneous circulation before hospital arrival and survival at discharge after two weeks were lower than in similar studies [7, 16]. Our findings showed a low survival effect of DA-BCPR, while other studies have reported increased survival and hospital discharge [12, 13]. In previous studies, the quality of CPR and the long interval from arrest to CPR have been suggested as possible reasons for the limited effectiveness of DA-BCPR [12-14]. In addition, other factors, such as poor prognosis of patients, delay in arrest recognition and starting CPR, the unstable emotional status of bystanders, low quality of interventions, delay in using AED, and dispatcher’s inadequate instruction, can decrease the quality of DA-BCPR. Our findings do not necessarily negate the importance of dispatcher assistance to bystanders, as DA-BCPR helps a trained bystander recall the CPR procedure and helps him or her initiate CPR according to instructions [14, 16].
In this study, the median EMS response time interval was 7.9 minutes in urban and 12.3 minutes in rural areas. Chang showed that EMS response time interval faster than 4-5 minutes was associated with a higher hospital discharge rate and good neurological recovery [25]. Timely use of AED in shockable rhythms can increase survival at discharge and neurological outcomes [7, 26, 27]. Thus, in this study, delay in using AED may be a reason for the limited effectiveness of DA-BCPR. Although the use of AED, in general, brings challenges, along with the implementation of DA-BCPR instruction, it should be used so the chance of survival of OHCA patients can be increased with the timely use of AED.
Our study showed a statistically significant relationship between the familiarity of bystanders with CPR and its implementing with an assistance dispatcher (P=0.01), which is consistent with other studies [1, 3, 5, 7, 14, 28]. This finding indicates the importance of training non-specialists regarding identifying cardiac arrest and other aspects of CPR. Since identifying cardiac arrest is difficult for non-specialists, they should be trained to perform CPR. Furthermore, dispatcher training about DA-BCPR instruction should be emphasized because dispatchers should identify cardiac arrest based on information from bystanders and provide appropriate instructions for chest compression over the call. Teaching non-specialists first aid can increase the number of community members with the skills and ability to provide CPR in case of OHCA.
Lack of sufficient knowledge and skills to recognize cardiac arrest and start CPR and fear of harm to patients were the most common reasons for not performing CPR. These findings are consistent with the results of Dianati et al. [19] and Vu et al. [29]. In some studies, the fear of fighting or transmitting infection is mentioned as the most important barrier [20, 22, 30]. Training CPR for non-specialists has many positive results. In Iran, there is no formal community-based CPR training program; however, there are some educational efforts by EMS and the Red Crescent. In other countries, CPR training in the community has been practiced in many forms. For example, CPR education in high school is mandatory in the USA [31], and CPR training became compulsory in middle school in Denmark [32]. CPR training for non-specialists can effectively increase the number of people with basic skills who want to help others in hard times, such as OHCA patients. Such positive results were observed in the Vietnam and Thailand [33, 34].
Conclusion
This study showed that the most important barrier to not performing CPR in OHCA despite recommendations of dispatch (based on DA-BCPR instruction) was insufficient knowledge and skills to recognize and perform CPR by bystanders. These issues should be addressed through CPR training for the public, improving dispatch skills, and raising awareness about cardiac arrest in the community. CPR training courses in the communities should be mandatory for some groups, such as high school students, police officers, and school teachers. In addition, promoting more CPR training for non-specialists by developing and adapting protocols and devices for DA-BCPR could improve clinical outcomes. Also, it is essential to provide training and education programs for dispatchers through protocols and simulation training focusing on communication challenges.
Study limitations
This study had several limitations. First, it had inherent problems with data collection. Because this study was based on secondary data analysis, there may be cases with missing information in some of the evaluated variables. Second, we gathered some data through interviews with bystanders; thus, we did not assess the quality of CPR, such as depth and rate of chest compression and rescue ventilation, which would influence the survival outcomes. Third, the small sample size in this study was another limitation.
Ethical Considerations
Compliance with ethical guidelines
The study protocol was approved by the Research and Ethics Committee of the Neyshabur University of Medical Sciences (Code: IR.NUMS.REC.1400.030). All participants provided their consent before taking part in the study. Participation was completely voluntary, and participants could withdraw from the study at any time without any consequence.
Funding
This study was supported by a research grant (Grant No.: 1400-01-259) from the Research Chancellor of Neyshabur University of Medical Sciences. The funding source had no role in the study design, data collection, data analysis, data interpretation, or preparation of the
manuscript.
Authors' contributions
Conceptualization, study design and writing: Hasan Ghodsi and Roohollah Raiyati; Methodology and data analysis: Fatemeh Khorashadizadeh; Data gathering, drafting the manuscript and critically revising it for important intellectual content: Ameneh Samghani, Fatemeh Malekan and Seyedeh Somayeh Hoseini.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank Neyshabur University of Medical Sciences for the financial support.
References
Cardiopulmonary resuscitation (CPR) is a process performed to restore the activity of the heart, brain, and lungs in order to prevent sudden death and save people in cardiopulmonary arrest [1, 2]. In general, the survival rate in cases of in-hospital cardiac arrest (IHCA) in Western countries is less than 20%, and this rate is reported to be 17%-31% in the US. However, this rate is reported to be about 10% in cases of out-of-hospital cardiac arrest (OHCA) [2-4].
The first line of CPR and response to cardiac arrest is basic life support (BLS), which is the key part of saving lives, resulting in reducing the mortality rate and increasing the hospital discharge rate following cardiac arrest [3]. Without a qualified BLS, advanced cardiac life support (ALS) interventions will be ineffective. The main factors of BLS include recognizing cardiopulmonary arrest, activating the emergency system, initiating effective and quality CPR as soon as possible, and safely using an automated external defibrillator (AED) [3, 5].
Although the golden time to survive a person after cardiac arrest is 4 to 6 minutes, and the best outcome in patients with cardiopulmonary arrest is when basic resuscitation measures are started in the first 4 minutes [6], in most cases, the arrival of emergency medical technicians (EMTs) at the patient’s bedside takes more than this time. Therefore, a solution must be provided to initiate initial resuscitation interventions before emergency medical services (EMSs) arrive. One of these solutions is training the public in basic resuscitation interventions, which organizations such as the Red Crescent carry out. Another solution is training emergency callers in basic resuscitation interventions by the dispatcher of the Emergency Communications Center (ECC). This measure, named dispatcher-assisted bystander CPR (DA-BCPR), has explicitly been emphasized by the 2015 guideline of the American Heart Association (AHA) and the European Resuscitation Council [7, 8, 9, 10].
Pre-arrival instructions have been used for the first time in US EMS. Based on this protocol, the dispatcher asks the caller critical questions about the patient’s condition and, if necessary, offers advice and guidance until the ambulance arrives [11].
Some studies have also evaluated the association between DA-BCPR and ambulance response time. It has been found that DA-BCPR improves the survival of patients with OHCA despite delays in ambulance response time, emphasizing the importance of DA-BCPR in improving the survival of victims while waiting for an ambulance [12-14]. Several observational studies have also reported that DA-BCPR is associated with favorable neurological outcomes in patients with OHCA [15-17].
However, some studies have shown a low rate of performing CPR by bystanders [10, 18]. For example, a low rate of DA-BCPR has been reported in Iran [19]. Some barriers to performing BCPR include fear of infections, fear of harming the patient, legal concerns, and lack of previous CPR training [19-22].
Investigating the barriers to performing BLS procedures in OHCA patients can provide valuable information to strengthen the chain of survival and improve patient prognosis. This study aimed to identify barriers to performing DA-BCPR in OHCA patients.
Materials and Methods
Study setting
EMS in Iran was established in 1974 and managed by the Ministry of Health and Medical Education. Access to EMSs anywhere in the country is possible through calling 115, which provides free services to people since the government finances it. All 115 call-receiving employees are nurses or emergency medical technicians, the medical telephone consultants are physicians, and the dispatch operators are intermediate emergency medicine technicians or nurses. All ambulances are equipped with defibrillators to provide BLS. In 2018, a DA-BCPR program was initiated in Iran. The dispatcher asks two key questions to detect OHCA (following the 2010 AHA guidelines): Altered mental status and abnormal breathing. If the caller answers “yes” to both questions, the dispatcher will recommend standard CPR instruction to the caller. At the same time, the dispatcher sends information to the nearest ambulance station using the ASAYAR application. Until the ambulance arrives at the address, the dispatcher or physician supports bystanders by talking on the phone.
Study design and data collection
This cross-sectional study was conducted in two phases. In the first phase, the researcher reviewed dispatch audio recordings at the Neyshabur EMS Dispatch Center, Neyshabur City, Iran, from June 2022 to June 2023 and selected all records related to OHCA. The reviews of these records were targeted at DA-BCPR. Cases due to trauma and those without receiving dispatch assistance for CPR were excluded. Then, data related to each DA-BCPR were collected from retrospective medical records in EMSs and hospitals. Trained medical record reviewers extracted these records. In the second phase, the researchers contacted bystanders in each OHCA who called EMS and received additional data. For data gathering, we used a researcher-made questionnaire consisting of demographic data (age and gender of patients and their bystanders, education, and relation of bystanders with the patients, and the place of CPR) and specific questions (the bystander CPR experience, reasons for refusal to perform CPR, and the actions performed by a bystander). The instrument’s validity was confirmed by 7 university faculty members and 4 emergency medicine specialists (content validity ratio [CVR]=0.78 and content validity index [CVI]=0.84). Also, its reliability was confirmed by the test re-test method with a coefficient of 90% and considering a sample size of 15 people.
In addition, the chi-square and Fisher exact tests were used to determine the relationship between study variables. All statistical analyses were performed using R software, version 4.0.1 at P≤0.05.
Results
Among 391 EMS-assessed OHCA cases, we excluded patients with traumatic OHCA (n=31, 7.92%) and those who were not recommended for CPR by a dispatcher because the diagnosis of OHCA was not confirmed by a qualified person or medical staff (n=209, 58.05%). A total of 151 OHCA cases were included in this final analysis (Figure 1).
Patients’ and bystanders’ characteristics
Of 151 OHCA patients included in this study, most were males (70.27%), aged 50 years and older (81.08%), with a median age of 70 years (interquartile range=55-80 y). Most collapsed out of their homes (80.45%) and received OHCA in urban areas (70.20%).
The Mean±SD age of bystanders was 39.47±10.33 years; 51 bystanders (38.35%) had received CPR training, and only 10.53% of them experienced presumed cardiac arrest. The review of the audio records showed that of the bystanders, 86 cases (68.80%) performed CPR with only one request from the dispatcher; however, they rarely recognized pulselessness. Most patients (89.39%) did not receive mouth-to-mouth breathing.
The median response time interval was 9.21 min (±4.58). In 104 OHCA cases (68.9%), the arrival time was less than 6 minutes. In 31(20.5%), it was 6-10 minutes; in 16(10.6%), it was more than 10 minutes.
Of the bystanders who did not provide CPR, most (41.48%) indicated their “insufficient knowledge and skills” followed by “disappointment from the patient’s treatment” (17.78%) as the main barriers to performing CPR (Figure 2).
In other words, bystanders who had previously received CPR training had a greater chance of performing DA-BCPR. Other factors, such as the age and gender of patients; age, gender, and education of bystanders; and the number of dispatcher requests to perform CPR, were influential in performing CPR.
Of 151 OHCA patients, 139(92.05%) died on the scene or before arrival at the hospital, and only 12(7.95%) returned to spontaneous circulation before hospital arrival. Of 151 bystanders, only 51(38.35%) had previous CPR training.
Discussion
This study showed two main factors for not performing DA-BCPR in OHCA: Not recognizing cardiac arrest and the lack of knowledge on performing CPR. This finding indicates the importance of training non-specialists and dispatchers in identifying cardiac arrest.
Since the diagnosis of cardiac arrest is difficult for non-specialists, in the new training program, it should be emphasized that CPR should be started when noticing agonal gasping or unusual breathing. Additionally, dispatcher training for DA-BCPR should be prioritized. Dispatchers should identify cardiac arrest based on information from callers and provide appropriate instructions for chest compression over the call.
The rate of DA-BCPR in this study was higher than in other studies [16, 19, 23, 24]. Still, the rates of the return to spontaneous circulation before hospital arrival and survival at discharge after two weeks were lower than in similar studies [7, 16]. Our findings showed a low survival effect of DA-BCPR, while other studies have reported increased survival and hospital discharge [12, 13]. In previous studies, the quality of CPR and the long interval from arrest to CPR have been suggested as possible reasons for the limited effectiveness of DA-BCPR [12-14]. In addition, other factors, such as poor prognosis of patients, delay in arrest recognition and starting CPR, the unstable emotional status of bystanders, low quality of interventions, delay in using AED, and dispatcher’s inadequate instruction, can decrease the quality of DA-BCPR. Our findings do not necessarily negate the importance of dispatcher assistance to bystanders, as DA-BCPR helps a trained bystander recall the CPR procedure and helps him or her initiate CPR according to instructions [14, 16].
In this study, the median EMS response time interval was 7.9 minutes in urban and 12.3 minutes in rural areas. Chang showed that EMS response time interval faster than 4-5 minutes was associated with a higher hospital discharge rate and good neurological recovery [25]. Timely use of AED in shockable rhythms can increase survival at discharge and neurological outcomes [7, 26, 27]. Thus, in this study, delay in using AED may be a reason for the limited effectiveness of DA-BCPR. Although the use of AED, in general, brings challenges, along with the implementation of DA-BCPR instruction, it should be used so the chance of survival of OHCA patients can be increased with the timely use of AED.
Our study showed a statistically significant relationship between the familiarity of bystanders with CPR and its implementing with an assistance dispatcher (P=0.01), which is consistent with other studies [1, 3, 5, 7, 14, 28]. This finding indicates the importance of training non-specialists regarding identifying cardiac arrest and other aspects of CPR. Since identifying cardiac arrest is difficult for non-specialists, they should be trained to perform CPR. Furthermore, dispatcher training about DA-BCPR instruction should be emphasized because dispatchers should identify cardiac arrest based on information from bystanders and provide appropriate instructions for chest compression over the call. Teaching non-specialists first aid can increase the number of community members with the skills and ability to provide CPR in case of OHCA.
Lack of sufficient knowledge and skills to recognize cardiac arrest and start CPR and fear of harm to patients were the most common reasons for not performing CPR. These findings are consistent with the results of Dianati et al. [19] and Vu et al. [29]. In some studies, the fear of fighting or transmitting infection is mentioned as the most important barrier [20, 22, 30]. Training CPR for non-specialists has many positive results. In Iran, there is no formal community-based CPR training program; however, there are some educational efforts by EMS and the Red Crescent. In other countries, CPR training in the community has been practiced in many forms. For example, CPR education in high school is mandatory in the USA [31], and CPR training became compulsory in middle school in Denmark [32]. CPR training for non-specialists can effectively increase the number of people with basic skills who want to help others in hard times, such as OHCA patients. Such positive results were observed in the Vietnam and Thailand [33, 34].
Conclusion
This study showed that the most important barrier to not performing CPR in OHCA despite recommendations of dispatch (based on DA-BCPR instruction) was insufficient knowledge and skills to recognize and perform CPR by bystanders. These issues should be addressed through CPR training for the public, improving dispatch skills, and raising awareness about cardiac arrest in the community. CPR training courses in the communities should be mandatory for some groups, such as high school students, police officers, and school teachers. In addition, promoting more CPR training for non-specialists by developing and adapting protocols and devices for DA-BCPR could improve clinical outcomes. Also, it is essential to provide training and education programs for dispatchers through protocols and simulation training focusing on communication challenges.
Study limitations
This study had several limitations. First, it had inherent problems with data collection. Because this study was based on secondary data analysis, there may be cases with missing information in some of the evaluated variables. Second, we gathered some data through interviews with bystanders; thus, we did not assess the quality of CPR, such as depth and rate of chest compression and rescue ventilation, which would influence the survival outcomes. Third, the small sample size in this study was another limitation.
Ethical Considerations
Compliance with ethical guidelines
The study protocol was approved by the Research and Ethics Committee of the Neyshabur University of Medical Sciences (Code: IR.NUMS.REC.1400.030). All participants provided their consent before taking part in the study. Participation was completely voluntary, and participants could withdraw from the study at any time without any consequence.
Funding
This study was supported by a research grant (Grant No.: 1400-01-259) from the Research Chancellor of Neyshabur University of Medical Sciences. The funding source had no role in the study design, data collection, data analysis, data interpretation, or preparation of the
manuscript.
Authors' contributions
Conceptualization, study design and writing: Hasan Ghodsi and Roohollah Raiyati; Methodology and data analysis: Fatemeh Khorashadizadeh; Data gathering, drafting the manuscript and critically revising it for important intellectual content: Ameneh Samghani, Fatemeh Malekan and Seyedeh Somayeh Hoseini.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank Neyshabur University of Medical Sciences for the financial support.
References
- García-Suárez M, Méndez-Martínez C, Martínez-Isasi S, Gómez-Salgado J, Fernández-García D. Basic life support training methods for health science students: A systematic review. International Journal of Environmental Research and Public Health. 2019; 16(5):768. [DOI:10.3390/ijerph16050768] [PMID]
- Malekzadeh J, Mazlom SR, Assarroudi A, Rasouly Sangany M. Comparison of the effects of three different counting methods on cardiopulmonary resuscitation quality and rescuer fatigue. Evidence Based Care. 2017; 7(1):35-42. [DOI: 10.22038/EBCJ.2017.19821.1478]
- Papi M, Hakim A, Bahrami H. Basic life support knowledge and skills in emergency medical services, Islamic Republic of Iran. Eastern Mediterranean Health Journal. 2020; 26(10):1193-9. [DOI: 10.26719/emhj.19.018] [PMID]
- Hernández-Padilla J, Suthers F, Fernández-Sola C, Granero-Molina J. Development and psychometric assessment of the Basic Resuscitation Skills Self-Efficacy Scale. European Journal of Cardiovascular Nursing. 2016; 15(3):e10-8. [DOI:10.1177/1474515114562130] [PMID]
- Assarroudi A, Heshmati Nabavi F, Ebadi A, Esmaily H. Professional Rescuers’ experiences of motivation for cardiopulmonary resusCitation A qualitative study. Nursing & Health Sciences. 2017; 19(2):237-43. [DOI:10.1111/nhs.12336] [PMID]
- Kleinman ME, Brennan EE, Goldberger ZD, Swor RA, Terry M, Bobrow BJ, et al. Part 5: Adult basic life support and cardiopulmonary resuscitation quality: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015; 132(18 Suppl 2):S414-35. [PMID]
- Lee SY, Hong KJ, Shin SD, Ro YS, Song KJ, Park JH, et al. The effect of dispatcher-assisted cardiopulmonary resuscitation on early defibrillation and return of spontaneous circulation with survival. Resuscitation. 2019; 135:21-9. [DOI:10.1016/j.resuscitation.2019.01.004] [PMID]
- Eberhard KE, Linderoth G, Gregers MCT, Lippert F, Folke F. Impact of dispatcher-assisted cardiopulmonary resuscitation on neurologically intact survival in out-of-hospital cardiac arrest: A systematic review. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine. 2021; 29(1):70. [DOI:10.1186/s13049-021-00875-5] [PMID]
- Limkakeng AT, Ye JJ, Staton C, Ng YY, Leong BSH, Shahidah N, et al. Impact of dispatcher-assisted cardiopulmonary resuscitation on performance of termination of resuscitation criteria. Resuscitation. 2022; 170:160-6. [DOI:10.1016/j.resuscitation.2021.11.034] [PMID]
- Roppolo LP, Pepe PE, Cimon N, Gay M, Patterson B, Yancey A, et al. Modified cardiopulmonary resuscitation (CPR) instruction protocols for emergency medical dispatchers: Rationale and recommendations. Resuscitation. 2005; 65(2):203-10. [DOI:10.1016/j.resuscitation.2004.11.025] [PMID]
- Zachariah BS, Pepe PE. The development of emergency medical dispatch in the USA: A historical perspective. European Journal of Emergency Medicine. 1995; 2(3):109-12. [PMID]
- Bohm K, Vaillancourt C, Charette ML, Dunford J, Castrén M. In patients with out-of-hospital cardiac arrest, does the provision of dispatch cardiopulmonary resuscitation instructions as opposed to no instructions improve outcome: A systematic review of the literature. Resuscitation. 2011; 82(12):1490-5. [DOI:10.1016/j.resuscitation.2011.09.004] [PMID]
- Harjanto S, Na MX, Hao Y, Ng YY, Doctor N, Goh ES, et al. A before-after interventional trial of dispatcher-assisted cardio-pulmonary resuscitation for out-of-hospital cardiac arrests in Singapore. Resuscitation. 2016; 102:85-93. [DOI:10.1016/j.resuscitation.2016.02.014] [PMID]
- Rea TD, Eisenberg MS, Culley LL, Becker L. Dispatcher-assisted cardiopulmonary resuscitation and survival in cardiac arrest. Circulation. 2001; 104(21):2513-6. [DOI:10.1161/hc4601.099468] [PMID]
- Bobrow BJ, Spaite DW, Vadeboncoeur TF, Hu C, Mullins T, Tormala W, et al. Implementation of a regional telephone cardiopulmonary resuscitation program and outcomes after out-of-hospital cardiac arrest. JAMA Cardiology. 2016; 1(3):294-302. [DOI:10.1001/jamacardio.2016.0251] [PMID]
- Ro YS, Shin SD, Lee YJ, Lee SC, Song KJ, Ryoo HW, et al. Effect of dispatcher-assisted cardiopulmonary resuscitation program and location of out-of-hospital cardiac arrest on survival and neurologic outcome. Annals of Emergency Medicine. 2017; 69(1):52-61.e1. [DOI:10.1016/j.annemergmed.2016.07.028] [PMID]
- Wu Z, Panczyk M, Spaite DW, Hu C, Fukushima H, Langlais B, et al. Telephone cardiopulmonary resuscitation is independently associated with improved survival and improved functional outcome after out-of-hospital cardiac arrest. Resuscitation. 2018; 122:135-40. [DOI:10.1016/j.resuscitation.2017.07.016] [PMID]
- Bahadori M, Nasiripur A, Tofighi S, Gohari M. Emergency medical services in Iran: An overview. Australasian Medical Journal. 2010; 3(6):335-9. [Link]
- Dianati M, Assari-Maraghi A, Paravar M, Gilasi HR. [Bystander’s cardiopulmonary resuscitation rate and related factors in Kashan, Iran in 2014 (Persian)]. Feyz Medical Sciences Journal. 2015; 19(4):341-8. [Link]
- Bhanji F, Mancini ME, Sinz E, Rodgers DL, McNeil MA, Hoadley TA, et al. Part 16: Education, implementation, and teams: 2010 American Heart Association Guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010; 122(18 Suppl 3):S920-33. [PMID]
- Malta Hansen C, Rosenkranz SM, Folke F, Zinckernagel L, Tjørnhøj-Thomsen T, Torp-Pedersen C, et al. Lay Bystanders’ perspectives on what facilitates cardiopulmonary resuscitation and use of automated external defibrillators in real cardiac arrests. Journal of the American Heart Association. 2017; 6(3):e004572. [DOI:10.1161/JAHA.116.004572] [PMID]
- Shams A, Raad M, Chams N, Chams S, Bachir R, El Sayed MJ. Community involvement in out of hospital cardiac arrest: A cross-sectional study assessing cardiopulmonary resuscitation awareness and barriers among the Lebanese youth. Medicine. 2016; 95(43):e5091. [DOI:10.1097/MD.0000000000005091] [PMID]
- Park JH, Ro YS, Shin SD, Song KJ, Hong KJ, Kong SY. Dispatcher-assisted bystander cardiopulmonary resuscitation in rural and urban areas and survival outcomes after out-of-hospital cardiac arrest. Resuscitation. 2018; 125:1-7. [DOI:10.1016/j.resuscitation.2018.01.026] [PMID]
- Gräsner JT, Herlitz J, Koster RW, Rosell-Ortiz F, Stamatakis L, Bossaert L. Quality management in resuscitation--towards a European cardiac arrest registry (EuReCa). Resuscitation. 2011; 82(8):989-94. [DOI:10.1016/j.resuscitation.2011.02.047] [PMID]
- Chang I, Lee SC, Shin SD, Song KJ, Ro YS, Park JH, et al. Effects of dispatcher-assisted bystander cardiopulmonary resuscitation on neurological recovery in paediatric patients with out-of-hospital cardiac arrest based on the pre-hospital emergency medical service response time interval. Resuscitation. 2018; 130:49-56. [DOI:10.1016/j.resuscitation.2018.06.029] [PMID]
- Nagao K, Nonogi H, Yonemoto N, Gaieski DF, Ito N, Takayama M, et al. Duration of prehospital resuscitation efforts after out-of-hospital cardiac arrest. Circulation. 2016; 133(14):1386-96. [DOI:10.1161/CIRCULATIONAHA.115.018788] [PMID]
- Viereck S, Møller TP, Ersbøll AK, Bækgaard JS, Claesson A, Hollenberg J, et al. Recognising out-of-hospital cardiac arrest during emergency calls increases bystander cardiopulmonary resuscitation and survival. Resuscitation. 2017; 115:141-7. [DOI:10.1016/j.resuscitation.2017.04.006] [PMID]
- Srinivasan Gandhi JK. A study to evaluate effectiveness of triaging the triage: Reducing waiting time to triage in the command post to emergency department in selected hospitals. International Journal of Nursing Education. 2019; 11(4):149-53. [DOI:10.5958/0974-9357.2019.00108.9]
- Vu DH, Hoang BH, Do NS, Do GP, Dao XD, Nguyen HH, et al. Why Bystanders did not perform cardiopulmonary resuscitation on out-of-hospital cardiac arrest patients: A multi-center study in Hanoi (Vietnam). Prehospital and Disaster Medicine. 2022; 37(1):101-5. [DOI:10.1017/S1049023X21001369] [PMID]
- Sarchahi Z, Ghodsi, H, lakziyan R, Froutan R. Exploring the challenges of prehospital emergency personnel in COVID-19 Pandemic: A qualitative study. Asia Pacific Journal of Health Management. 2022; 17(1). [DOI:10.24083/apjhm.v17i1.1285]
- Brown LE, Halperin H. CPR training in the United States: The need for a new gold standard (and the gold to create it). Circulation Research. 2018; 123(8):950-2. [DOI:10.1161/CIRCRESAHA.118.313157] [PMID]
- Hansen CM, Lippert FK, Wissenberg M, Weeke P, Zinckernagel L, Ruwald MH, et al. Temporal trends in coverage of historical cardiac arrests using a volunteer-based network of automated external defibrillators accessible to laypersons and emergency dispatch centers. Circulation. 2014; 130(21):1859-67. [DOI:10.1161/CIRCULATIONAHA.114.008850] [PMID]
- Chaleepad S, Impool T, Lertsinudom S, Chadbunchachai W, Nakahara S. First-responder training based on existing healthcare system in Thailand. Resuscitation. 2020; 148:1-2. [DOI:10.1016/j.resuscitation.2019.12.028] [PMID]
- Hoang BH, Nakahara S, Nguyen HT. Training of potential trainers on lay-people CPR in Vietnam. Resuscitation. 2019; 136:149-50. [DOI:10.1016/j.resuscitation.2019.01.030] [PMID]
Type of Study: Research |
Subject:
Emergency
Received: 2023/06/28 | Accepted: 2023/01/21 | Published: 2024/01/1
Received: 2023/06/28 | Accepted: 2023/01/21 | Published: 2024/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Health in Emergencies and Disasters Quarterly
Health in Emergencies & Disasters Research Center, University of Social Welfare and Rehabilitation Sciences, Evin, Kudakyar Ave, Tehran, Iran.
Journal Tel: +9821 71732816 (2816)
Publisher Tel: +9821 4535 5555 - 4535 5000
