

Volume 10, Issue 1 (Autumn 2024)
Health in Emergencies and Disasters Quarterly 2024, 10(1): 59-66 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Shams N, Abbasi Dolatabadi Z, Haqqani S, Delkhosh M. Relationship Between COVID-19-related Anxiety and Changes in Lifestyle Behaviors Among Older Adults in Iran. Health in Emergencies and Disasters Quarterly 2024; 10 (1) :59-66
URL: http://hdq.uswr.ac.ir/article-1-565-en.html
URL: http://hdq.uswr.ac.ir/article-1-565-en.html



1- Department of Community Health and Geriatric Nursing, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran., دانشکده پرستاری و مامایی دانشگاه علوم پزشکی تهران
2- Department of Medical-Surgical Nursing, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran., دانشکده پرستاری و مامایی دانشگاه علوم پزشکی تهران
3- Nursing Care Research Center, School of Nursing and Midwifery, Iran University of Medical Sciences, Tehran, Iran., دانشكده پرستاري و مامايي، دانشگاه علوم پزشـكي ايـران
4- Department of Community Health and Geriatric Nursing, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran. ,delkhoshmarjan@gmail.com
2- Department of Medical-Surgical Nursing, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran., دانشکده پرستاری و مامایی دانشگاه علوم پزشکی تهران
3- Nursing Care Research Center, School of Nursing and Midwifery, Iran University of Medical Sciences, Tehran, Iran., دانشكده پرستاري و مامايي، دانشگاه علوم پزشـكي ايـران
4- Department of Community Health and Geriatric Nursing, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran. ,
Full-Text [PDF 593 kb]
(1002 Downloads)
| Abstract (HTML) (2713 Views)
Full-Text: (655 Views)
Introduction
COVID-19 has been a recent crisis that has affected people’s activities [1-3]. The World Health Organization (WHO) declared this disease a pandemic on March 11, 2020 [4, 5]. The high transmission and prevalence of this disease led to the creation of an unprecedented public health crisis in the world [6] and endangered the physical and mental health of humans [3, 7, 8]. One of the important consequences of the COVID-19 pandemic was the creation of social anxiety worldwide [9]. The emergence of this disease caused confusion and significant changes in people’s living conditions with devastating psychological effects such as anxiety [10, 11]. Epidemics and pandemics are widely understood as traumatic events and lead to a significant increase in anxiety, depression, and fear of people [12, 13]. The anxiety caused by COVID-19 was mainly due to reasons such as the unknown nature of the disease and insufficient information about it, the frequent appearance of new clinical symptoms, and the high infection rate [7, 14]. The pandemic led to obsessive behaviors and negative feelings even in people who had good mental health before the pandemic [10]. Older adults were more susceptible to COVID-19 infection and experienced adverse physical and mental consequences [15, 16]. The fear and anxiety caused by COVID-19 can lead to mental and psychological complications and weaken the immune system in vulnerable groups such as older adults [6, 17]. Anxiety is one of the most common mental problems among older adults. The outbreak of COVID-19 increased their anxiety [10], and they experienced a relatively high level of depression compared to other age groups [15, 18].
On the other hand, the anxiety caused by the COVID-19 pandemic and the implementation of preventive measures such as social distancing and self-quarantine affected people’s lifestyles in different countries and led to severe fundamental changes in their activities of daily living [11, 12]. One of the effects on people’s lifestyles was related to their nutritional habits [13]. On the other hand, home quarantine affected the sleep quality of people [12]. Several studies suggested that older adults are more likely to experience the negative effects of COVID-19 on their lifestyle [19-22]. Older adults may avoid buying foods during the pandemic because of anxiety and fear of infection [13]. In addition, their appetite may decline due to decreased physical activity, eating alone, anxiety, and stress caused by COVID-19 [23]. The COVID-19 pandemic negatively affected the physical activity of people, including older adults [18]. Such changes in the lifestyle of the elderly, along with their underlying health problems, can increase the serious complications of COVID-19 [14].
Since lifestyle guidelines for COVID-19 are not completely evidence-based and the information about how to deal with issues such as self-care, nutrition, physical activity, or sleep during the pandemic is incomplete, more studies are needed on the effects of the pandemic on the lifestyle behaviors of people. Observational studies on lifestyle behaviors during the pandemic are necessary to design effective public policies, especially among vulnerable groups such as older adults [19]. Therefore, this study aimed to evaluate the relationship between the anxiety caused by COVID-19 and the changes in lifestyle behaviors of older adults in Zanjan, Iran.
Materials and Methods
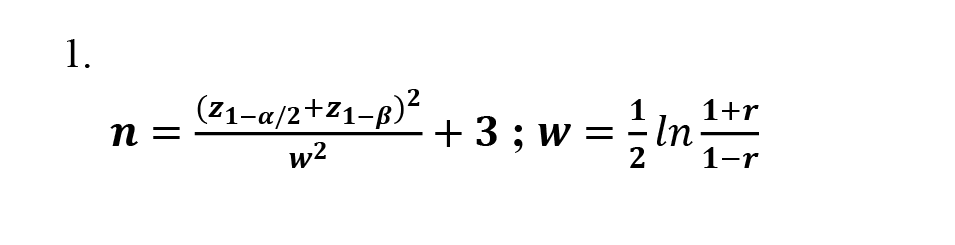
This descriptive-correlational study with a cross-sectional design was conducted in 2021. Participants were 265 older adults aged 60-74 years, covered by the comprehensive health centers in Zanjan. The sample size was determined using the Equation 1 at a 95% confidence level and considering 90% test power, a correlation coefficient (r) of 0.2 between anxiety caused by COVID-19 and changes in lifestyle behaviors, Z(1-α/2)=1.96, and Z(1-β)=1.28 (Equation 1):
Sampling was conducted using a multi-stage random sampling method. Considering the distribution of comprehensive health centers across the four regions of Zanjan, two centers were randomly selected from each region, i.e. a total of 8 centers out of 18. In this stage, the sample size for each center was determined separately based on the number of registered elderly people. Then, elderly people were selected using a convenience sampling method and based on the study inclusion criteria (age 60-74 years, not having psychological disorders according to a self-report, and willingness to participate in the research).
For data collection, three questionnaires were used:
Demographic form
This questionnaire surveys ten sociodemographic characteristics, including age, gender, educational level, marital status, income level, living arrangements, underlying diseases, and history of COVID-19 infection in the individual and in the family.
Coronavirus pandemic anxiety scale (CPAS-11): This tool, designed by Bernardo et al. (2020) for the age group of 18-79 years to measure anxiety in the past two weeks, has 11 items and two domains of somatic and non-somatic symptoms [20]. The items are rated on a 4-point Likert scale as 0 (not at all), 1 (several days), 2 (more than half the days), and 3 (nearly every day). The total score ranges 0-33, with scores >15 indicating a high level of anxiety. The Cronbach’s α for this tool is 0.87. In our study, after forward-backward translation, it was sent to the developer, and a correlation of 0.83 was reported between the main and Persian versions. To determine the face validity and content validity, the opinions of ten gerontology and community health professors were solicited, and their feedback was used to modify the items. The test re-test reliability was assessed at a two-week interval on 20 individuals who were not from the samples, resulting in an intraclass correlation coefficient of 0.81.
Lifestyle-related behavior changes scale during the COVID-19 pandemic: This tool, designed and validated by Kumari et al. (2020) [21], has 20 items measuring changes in lifestyle behaviors during the COVID-19 pandemic in terms of eating habits, exercise/physical activity, and sleep/rest quality. The questionnaire includes nine positive items indicating undesirable changes in lifestyle behaviors rated on a five-point Likert scale (significantly increased, slightly increased, grossly similar, slightly decreased, and significantly decreased) and nine negative items (indicating desirable changes in lifestyle behaviors) with reversed scoring. Items 3 and 18 are neutral. A higher score indicates more desirable changes in lifestyle behaviors during the COVID-19 pandemic, while a lower score indicates more undesirable changes. The Cronbach’s α for the reliability of the overall questionnaire is 0.72. This questionnaire was translated into Persian, and its validity (content and face) and reliability were calculated in our study. The content and face validity were confirmed based on the opinions of 10 experts in this field. For the reliability of the overall scale, a Cronbach’s α of 0.81 was obtained.
The researcher read the questions to those who visited in person and completed the questionnaires. For those contacted by phone, the answers were recorded. The collected data were analyzed using descriptive statistics (frequency, percentage, Mean±SD) and inferential statistics (Pearson correlation test) in SPSS software, version 16.
Results
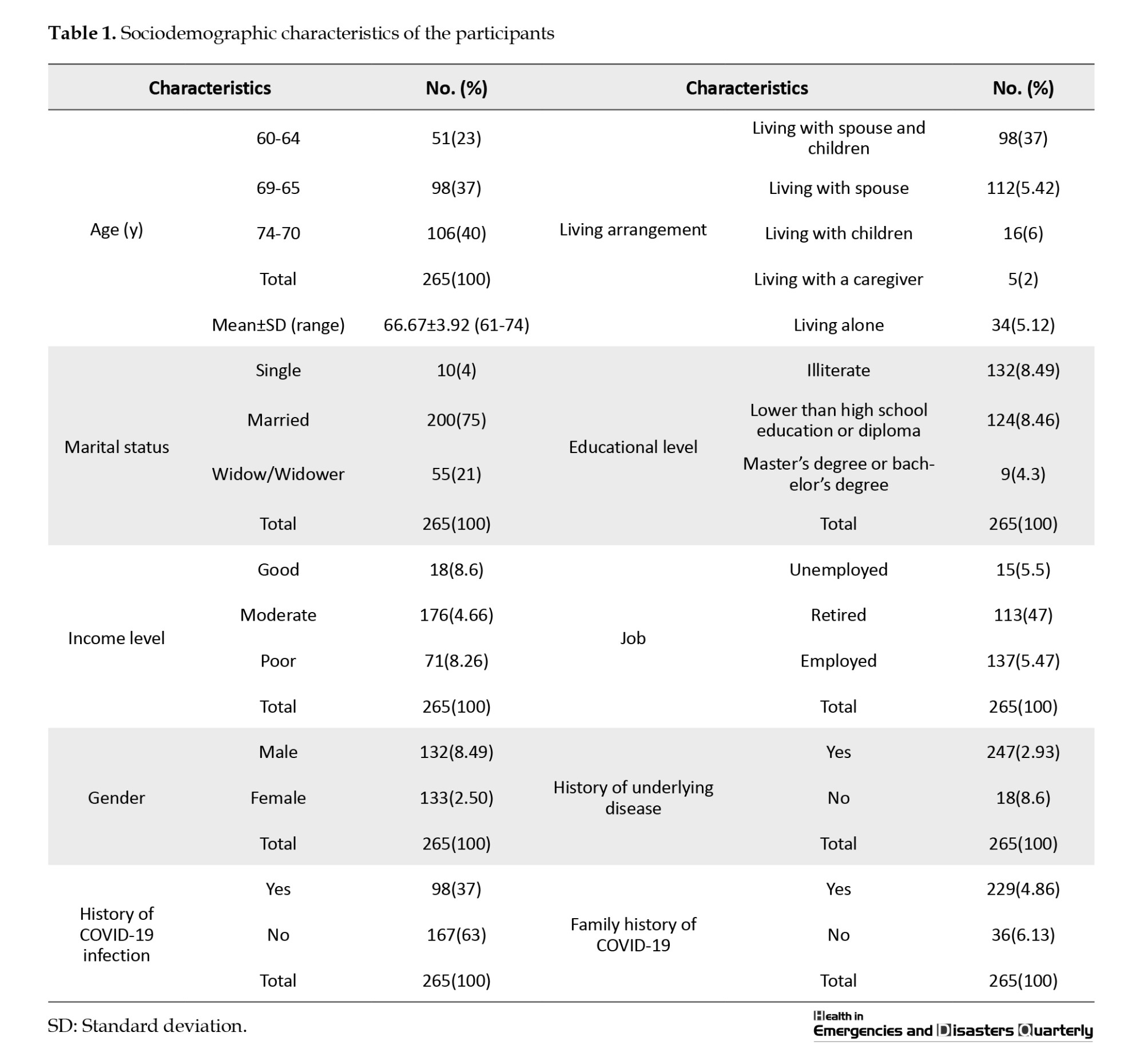
The mean age of participants was 66.67±3.92 years. Most were married (75%), illiterate (49.8%), and had a moderate income level (66.4%). Table 1 reports other demographic characteristics.
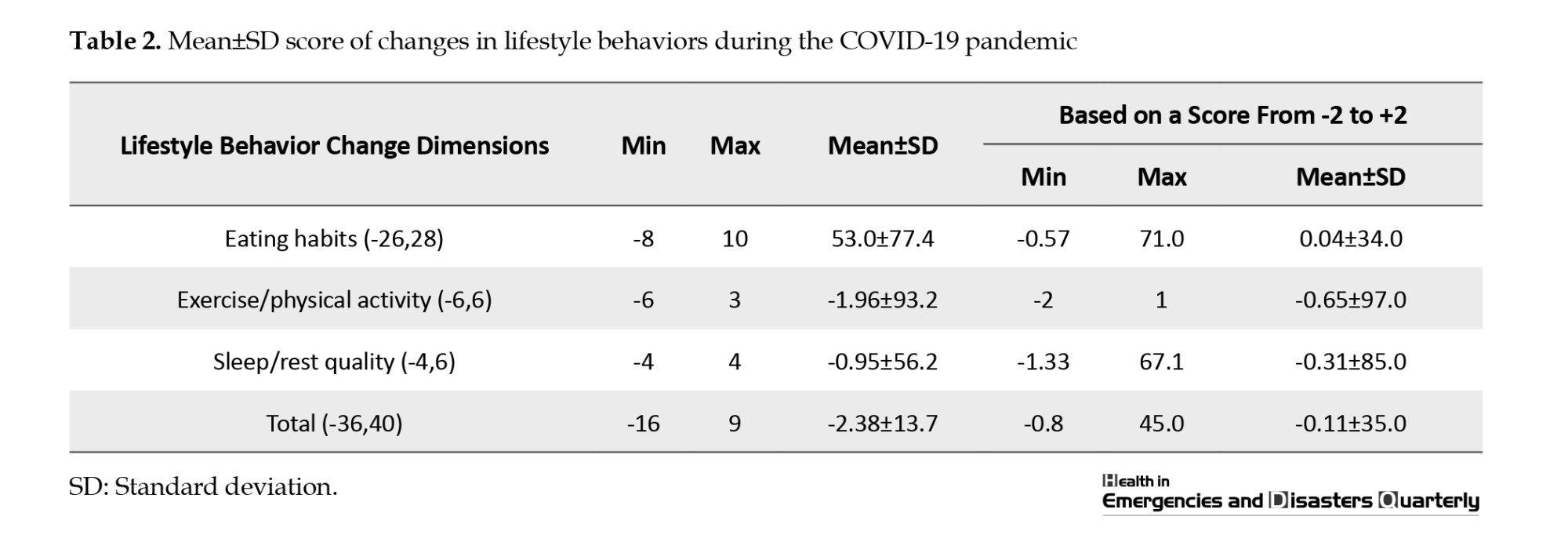
All participants experienced severe anxiety caused by COVID-19 (100%) with a mean total score of 22.23±3.47 (>15). The mean anxiety score for non-somatic symptoms was 11.55±2.34, and for somatic symptoms, it was 10.67±1.94. Regarding lifestyle behavior changes, the mean total score was -2.38±7.13, ranged from -40 to 36. The changes were slightly desirable only in terms of eating habits. In the dimensions of “exercise/physical activity” and “sleep/rest quality,” the changes were undesirable (Table 2).
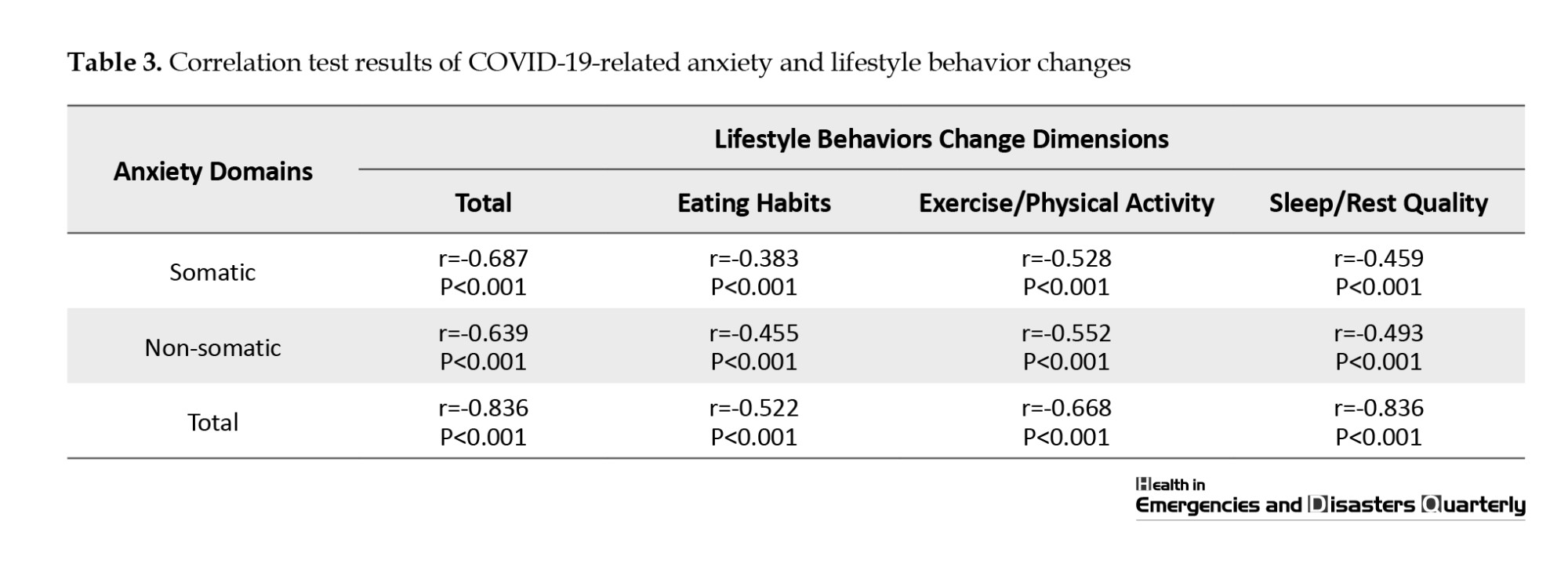
We found a significant negative correlation between COVID-19-related anxiety (somatic and non-somatic symptoms) and lifestyle behavior change and its dimensions (P<0.001). This indicates that the increase in COVID-19-related anxiety can lead to undesirable changes in the lifestyle behaviors of older adults (Table 3).
Discussion
This study aimed to determine the relationship between the anxiety caused by COVID-19 and the changes in lifestyle-related behaviors of older adults living in Zanjan, Iran. The results showed an inverse and significant correlation between COVID-19-related anxiety (somatic and non-somatic) and changes in lifestyle behaviors (exercise/physical activity, eating habits, and sleep/rest). All elderly participants experienced severe anxiety.
Wang et al. compared the prevalence of anxiety among older adults before and during the COVID-19 pandemic in China and found that the prevalence of anxiety was about 4.95% before the outbreak, which increased by 10% during the pandemic [22]. Their results are consistent with the present study, although their study was conducted at the beginning of the pandemic in China. Our study was conducted after the initiation of vaccination and the reduction of restrictions for social gatherings in Iran. In Rashedi et al.’s study, it was also found that the prevalence of anxiety due to COVID-19 among older adults was 9% [23]. The results of Sirin et al. indicated that 31.7% of the participants experienced high levels of anxiety during the COVID-19 pandemic. Their study showed that during the pandemic, social distancing and quarantine were severe risk factors for the psychological well-being of older adults, causing high levels of anxiety among them [24]. The findings of our study are consistent with Sirin et al.’s study, both studies highlighting the negative effect of COVID-19 on the mental health of older adults. Ouanes et al. [25] examined the prevalence of depression, anxiety, and stress among older adults in quarantine during the COVID-19 pandemic in Qatar, and found no significant difference in the prevalence of these symptoms compared to a gender- and age-matched control group. They concluded that the elderly population, due to their high resilience and effective coping strategies developed over the years, did not experience significant psychological distress related to quarantine. In Iran, older adults did not receive specific support or interventions to cope with the psychological burden of the pandemic, leaving this vulnerable population exposed to high level of psychological distress during the pandemic. The results of the present study further underscore that older adults, when faced with crises, experience high levels of stress and anxiety and need to receive targeted, practical support, education, and counseling interventions.
Limited studies have been conducted regarding changes in lifestyle behaviors among older adults during the COVID-19 pandemic. Renzo et al. found that diet, physical activity, and the incidence of high-risk behaviors such as smoking among people over 12 years of age had essential changes during the pandemic. The desire to smoke increased among the population and physical activity declined [26]. This supports the results of the present study. We showed that, among lifestyle-related behaviors, exercise/physical activity experienced more negative changes [27]. Di Santo et al. also reported that most older adults reduced their physical activity, and nearly 70% reported increased immobility time. Adherence to the Mediterranean diet decreased in almost one-third of the respondents, and more than 35% reported weight gain. Social activities also declined in most of the participants, and they reduced their productive activities [18]. Hoffman et al. determined that about half of the elderly reported decreased physical activity and exercise due to the pandemic, and some also reported abnormal eating behaviors such as eating more snacks [28]. The results of these studies indicate that the COVID-19 pandemic caused changes in the diet and physical activity of older people. During the pandemic, quarantine, social distancing, fear of contracting the disease, and inactivity in enclosed environments are among the factors that limit people’s physical activity and exercise. The closure of educational, sports, and recreational centers also had role in limiting the physical activity of people in different age groups.
The results of the present study demonstrated a significant inverse correlation between anxiety caused by COVID-19 (somatic and non-somatic) and changes in lifestyle behaviors. Similarly, the study by Schuch et al. found the significant inverse correlation of diet and physical activity with the COVID-19-related anxiety and depression among the participants [29]. Creese et al. also identified that, compared to pre-COVID data, decreased physical activity was a risk factor for the worsening of mental health problems during the pandemic [30]. Furthermore, the study by Nagasu et al. showed that lifestyle-related factors such as insufficient rest, sleep, and nutritious meals were significantly associated with psychological disorders during the COVID-19 pandemic [31]. The findings emphasize the critical need for targeted, effective interventions to support, educate, and counsel older adults to mitigate the adverse effects of high anxiety and promote better lifestyle behaviors during pandemics.
A limitation of this study was the lack of evaluation of cognitive problems in older adults. It is recommended that a cognitive test should be used in future studies for investigation. Another limitation was that due to the conditions of the COVID-19 pandemic and the impossibility of older adults’ difficulty attending the health centers and completing the questionnaire in person, the questionnaires were completed by the researchers on their behalf (in person and by phone), which can cause a bias in the accuracy of the responses. Based on the findings of this study and similar studies, it is recommended that timely and appropriate education and psychological counseling for older adults should be systematically provided in health centers. Community health and geriatric nurses, specialists, and caregivers should be enlisted to help modify various lifestyle behaviors of older adults. It is also recommended to conduct similar studies in other cities to examine the potential correlation between lifestyle changes and other mental health problems in older adults during the pandemic. The self-efficacy of older adults and its relationship with their anxiety should also be investigated.
Conclusion
There is a significant negative relationship between somatic and non-somatic domains of COVID-19-related anxiety and the changes in lifestyle behaviors of older adults in Zajnajn, Iran. Timely educational, supportive, and counseling programs for older adults during the pandemic can potentially prevent them from developing anxiety and unhealthy lifestyle behaviors. Health system managers and policymakers need to develop and implement these supportive and counseling programs for the elderly to prevent psychological disorders in this vulnerable group.
Ethical Considerations
Compliance with ethical guidelines
All participants signed a written informed consent form. They were assured that their information would remain confidential. This study obtained its ethical approval from the Ethics Committee of the School of Nursing and Midwifery, Tehran University of Medical Sciences (Code: IR.TUMS.FNM.REC.1400.188).
Funding
This study was extracted from master’s thesis of Navid Shams, approved by Department of Geriatrics and Community Health Centers, School of Nursing and Midwifery, Tehran University of Medical Sciences.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors would like to thank all participants for their cooperation in this study.
References
COVID-19 has been a recent crisis that has affected people’s activities [1-3]. The World Health Organization (WHO) declared this disease a pandemic on March 11, 2020 [4, 5]. The high transmission and prevalence of this disease led to the creation of an unprecedented public health crisis in the world [6] and endangered the physical and mental health of humans [3, 7, 8]. One of the important consequences of the COVID-19 pandemic was the creation of social anxiety worldwide [9]. The emergence of this disease caused confusion and significant changes in people’s living conditions with devastating psychological effects such as anxiety [10, 11]. Epidemics and pandemics are widely understood as traumatic events and lead to a significant increase in anxiety, depression, and fear of people [12, 13]. The anxiety caused by COVID-19 was mainly due to reasons such as the unknown nature of the disease and insufficient information about it, the frequent appearance of new clinical symptoms, and the high infection rate [7, 14]. The pandemic led to obsessive behaviors and negative feelings even in people who had good mental health before the pandemic [10]. Older adults were more susceptible to COVID-19 infection and experienced adverse physical and mental consequences [15, 16]. The fear and anxiety caused by COVID-19 can lead to mental and psychological complications and weaken the immune system in vulnerable groups such as older adults [6, 17]. Anxiety is one of the most common mental problems among older adults. The outbreak of COVID-19 increased their anxiety [10], and they experienced a relatively high level of depression compared to other age groups [15, 18].
On the other hand, the anxiety caused by the COVID-19 pandemic and the implementation of preventive measures such as social distancing and self-quarantine affected people’s lifestyles in different countries and led to severe fundamental changes in their activities of daily living [11, 12]. One of the effects on people’s lifestyles was related to their nutritional habits [13]. On the other hand, home quarantine affected the sleep quality of people [12]. Several studies suggested that older adults are more likely to experience the negative effects of COVID-19 on their lifestyle [19-22]. Older adults may avoid buying foods during the pandemic because of anxiety and fear of infection [13]. In addition, their appetite may decline due to decreased physical activity, eating alone, anxiety, and stress caused by COVID-19 [23]. The COVID-19 pandemic negatively affected the physical activity of people, including older adults [18]. Such changes in the lifestyle of the elderly, along with their underlying health problems, can increase the serious complications of COVID-19 [14].
Since lifestyle guidelines for COVID-19 are not completely evidence-based and the information about how to deal with issues such as self-care, nutrition, physical activity, or sleep during the pandemic is incomplete, more studies are needed on the effects of the pandemic on the lifestyle behaviors of people. Observational studies on lifestyle behaviors during the pandemic are necessary to design effective public policies, especially among vulnerable groups such as older adults [19]. Therefore, this study aimed to evaluate the relationship between the anxiety caused by COVID-19 and the changes in lifestyle behaviors of older adults in Zanjan, Iran.
Materials and Methods
This descriptive-correlational study with a cross-sectional design was conducted in 2021. Participants were 265 older adults aged 60-74 years, covered by the comprehensive health centers in Zanjan. The sample size was determined using the Equation 1 at a 95% confidence level and considering 90% test power, a correlation coefficient (r) of 0.2 between anxiety caused by COVID-19 and changes in lifestyle behaviors, Z(1-α/2)=1.96, and Z(1-β)=1.28 (Equation 1):
Sampling was conducted using a multi-stage random sampling method. Considering the distribution of comprehensive health centers across the four regions of Zanjan, two centers were randomly selected from each region, i.e. a total of 8 centers out of 18. In this stage, the sample size for each center was determined separately based on the number of registered elderly people. Then, elderly people were selected using a convenience sampling method and based on the study inclusion criteria (age 60-74 years, not having psychological disorders according to a self-report, and willingness to participate in the research).
For data collection, three questionnaires were used:
Demographic form
This questionnaire surveys ten sociodemographic characteristics, including age, gender, educational level, marital status, income level, living arrangements, underlying diseases, and history of COVID-19 infection in the individual and in the family.
Coronavirus pandemic anxiety scale (CPAS-11): This tool, designed by Bernardo et al. (2020) for the age group of 18-79 years to measure anxiety in the past two weeks, has 11 items and two domains of somatic and non-somatic symptoms [20]. The items are rated on a 4-point Likert scale as 0 (not at all), 1 (several days), 2 (more than half the days), and 3 (nearly every day). The total score ranges 0-33, with scores >15 indicating a high level of anxiety. The Cronbach’s α for this tool is 0.87. In our study, after forward-backward translation, it was sent to the developer, and a correlation of 0.83 was reported between the main and Persian versions. To determine the face validity and content validity, the opinions of ten gerontology and community health professors were solicited, and their feedback was used to modify the items. The test re-test reliability was assessed at a two-week interval on 20 individuals who were not from the samples, resulting in an intraclass correlation coefficient of 0.81.
Lifestyle-related behavior changes scale during the COVID-19 pandemic: This tool, designed and validated by Kumari et al. (2020) [21], has 20 items measuring changes in lifestyle behaviors during the COVID-19 pandemic in terms of eating habits, exercise/physical activity, and sleep/rest quality. The questionnaire includes nine positive items indicating undesirable changes in lifestyle behaviors rated on a five-point Likert scale (significantly increased, slightly increased, grossly similar, slightly decreased, and significantly decreased) and nine negative items (indicating desirable changes in lifestyle behaviors) with reversed scoring. Items 3 and 18 are neutral. A higher score indicates more desirable changes in lifestyle behaviors during the COVID-19 pandemic, while a lower score indicates more undesirable changes. The Cronbach’s α for the reliability of the overall questionnaire is 0.72. This questionnaire was translated into Persian, and its validity (content and face) and reliability were calculated in our study. The content and face validity were confirmed based on the opinions of 10 experts in this field. For the reliability of the overall scale, a Cronbach’s α of 0.81 was obtained.
The researcher read the questions to those who visited in person and completed the questionnaires. For those contacted by phone, the answers were recorded. The collected data were analyzed using descriptive statistics (frequency, percentage, Mean±SD) and inferential statistics (Pearson correlation test) in SPSS software, version 16.
Results
The mean age of participants was 66.67±3.92 years. Most were married (75%), illiterate (49.8%), and had a moderate income level (66.4%). Table 1 reports other demographic characteristics.
All participants experienced severe anxiety caused by COVID-19 (100%) with a mean total score of 22.23±3.47 (>15). The mean anxiety score for non-somatic symptoms was 11.55±2.34, and for somatic symptoms, it was 10.67±1.94. Regarding lifestyle behavior changes, the mean total score was -2.38±7.13, ranged from -40 to 36. The changes were slightly desirable only in terms of eating habits. In the dimensions of “exercise/physical activity” and “sleep/rest quality,” the changes were undesirable (Table 2).
We found a significant negative correlation between COVID-19-related anxiety (somatic and non-somatic symptoms) and lifestyle behavior change and its dimensions (P<0.001). This indicates that the increase in COVID-19-related anxiety can lead to undesirable changes in the lifestyle behaviors of older adults (Table 3).
Discussion
This study aimed to determine the relationship between the anxiety caused by COVID-19 and the changes in lifestyle-related behaviors of older adults living in Zanjan, Iran. The results showed an inverse and significant correlation between COVID-19-related anxiety (somatic and non-somatic) and changes in lifestyle behaviors (exercise/physical activity, eating habits, and sleep/rest). All elderly participants experienced severe anxiety.
Wang et al. compared the prevalence of anxiety among older adults before and during the COVID-19 pandemic in China and found that the prevalence of anxiety was about 4.95% before the outbreak, which increased by 10% during the pandemic [22]. Their results are consistent with the present study, although their study was conducted at the beginning of the pandemic in China. Our study was conducted after the initiation of vaccination and the reduction of restrictions for social gatherings in Iran. In Rashedi et al.’s study, it was also found that the prevalence of anxiety due to COVID-19 among older adults was 9% [23]. The results of Sirin et al. indicated that 31.7% of the participants experienced high levels of anxiety during the COVID-19 pandemic. Their study showed that during the pandemic, social distancing and quarantine were severe risk factors for the psychological well-being of older adults, causing high levels of anxiety among them [24]. The findings of our study are consistent with Sirin et al.’s study, both studies highlighting the negative effect of COVID-19 on the mental health of older adults. Ouanes et al. [25] examined the prevalence of depression, anxiety, and stress among older adults in quarantine during the COVID-19 pandemic in Qatar, and found no significant difference in the prevalence of these symptoms compared to a gender- and age-matched control group. They concluded that the elderly population, due to their high resilience and effective coping strategies developed over the years, did not experience significant psychological distress related to quarantine. In Iran, older adults did not receive specific support or interventions to cope with the psychological burden of the pandemic, leaving this vulnerable population exposed to high level of psychological distress during the pandemic. The results of the present study further underscore that older adults, when faced with crises, experience high levels of stress and anxiety and need to receive targeted, practical support, education, and counseling interventions.
Limited studies have been conducted regarding changes in lifestyle behaviors among older adults during the COVID-19 pandemic. Renzo et al. found that diet, physical activity, and the incidence of high-risk behaviors such as smoking among people over 12 years of age had essential changes during the pandemic. The desire to smoke increased among the population and physical activity declined [26]. This supports the results of the present study. We showed that, among lifestyle-related behaviors, exercise/physical activity experienced more negative changes [27]. Di Santo et al. also reported that most older adults reduced their physical activity, and nearly 70% reported increased immobility time. Adherence to the Mediterranean diet decreased in almost one-third of the respondents, and more than 35% reported weight gain. Social activities also declined in most of the participants, and they reduced their productive activities [18]. Hoffman et al. determined that about half of the elderly reported decreased physical activity and exercise due to the pandemic, and some also reported abnormal eating behaviors such as eating more snacks [28]. The results of these studies indicate that the COVID-19 pandemic caused changes in the diet and physical activity of older people. During the pandemic, quarantine, social distancing, fear of contracting the disease, and inactivity in enclosed environments are among the factors that limit people’s physical activity and exercise. The closure of educational, sports, and recreational centers also had role in limiting the physical activity of people in different age groups.
The results of the present study demonstrated a significant inverse correlation between anxiety caused by COVID-19 (somatic and non-somatic) and changes in lifestyle behaviors. Similarly, the study by Schuch et al. found the significant inverse correlation of diet and physical activity with the COVID-19-related anxiety and depression among the participants [29]. Creese et al. also identified that, compared to pre-COVID data, decreased physical activity was a risk factor for the worsening of mental health problems during the pandemic [30]. Furthermore, the study by Nagasu et al. showed that lifestyle-related factors such as insufficient rest, sleep, and nutritious meals were significantly associated with psychological disorders during the COVID-19 pandemic [31]. The findings emphasize the critical need for targeted, effective interventions to support, educate, and counsel older adults to mitigate the adverse effects of high anxiety and promote better lifestyle behaviors during pandemics.
A limitation of this study was the lack of evaluation of cognitive problems in older adults. It is recommended that a cognitive test should be used in future studies for investigation. Another limitation was that due to the conditions of the COVID-19 pandemic and the impossibility of older adults’ difficulty attending the health centers and completing the questionnaire in person, the questionnaires were completed by the researchers on their behalf (in person and by phone), which can cause a bias in the accuracy of the responses. Based on the findings of this study and similar studies, it is recommended that timely and appropriate education and psychological counseling for older adults should be systematically provided in health centers. Community health and geriatric nurses, specialists, and caregivers should be enlisted to help modify various lifestyle behaviors of older adults. It is also recommended to conduct similar studies in other cities to examine the potential correlation between lifestyle changes and other mental health problems in older adults during the pandemic. The self-efficacy of older adults and its relationship with their anxiety should also be investigated.
Conclusion
There is a significant negative relationship between somatic and non-somatic domains of COVID-19-related anxiety and the changes in lifestyle behaviors of older adults in Zajnajn, Iran. Timely educational, supportive, and counseling programs for older adults during the pandemic can potentially prevent them from developing anxiety and unhealthy lifestyle behaviors. Health system managers and policymakers need to develop and implement these supportive and counseling programs for the elderly to prevent psychological disorders in this vulnerable group.
Ethical Considerations
Compliance with ethical guidelines
All participants signed a written informed consent form. They were assured that their information would remain confidential. This study obtained its ethical approval from the Ethics Committee of the School of Nursing and Midwifery, Tehran University of Medical Sciences (Code: IR.TUMS.FNM.REC.1400.188).
Funding
This study was extracted from master’s thesis of Navid Shams, approved by Department of Geriatrics and Community Health Centers, School of Nursing and Midwifery, Tehran University of Medical Sciences.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors would like to thank all participants for their cooperation in this study.
References
- Gao Q, Hu Y, Dai Z, Xiao F, Wang J, Wu J. The epidemiological characteristics of 2019 novel coronavirus diseases (COVID-19) in Jingmen, Hubei, China. Medicine. 2020; 99(23):e20605. [DOI:10.1097/MD.0000000000020605] [PMID] [PMCID]
- Abbasi Dolatabadi Z, Shali M, Nabi Foodani M, Delkhosh M, Shahmari M, Nikbakhtnasrabadi A. Experiences and lessons learned by clinical nurse managers during covid-19 pandemic in Iran. Journal of Nursing and Midwifery Sciences. 2023; 10(2):e138161. [Link]
- Nabi Foodani M, Mohamadnejad Ostad F, Navab E, Bahrampouri S, Abbasi Dolatabadi Z. Self-care and standard precaution observance in intensive care nurses during COVID 19. Health Education and Health Promotion. 2023; 11(1):3-10. [Link]
- Benksim A, Rachid A, Cherkaoui M. Vulnerability and fragility expose older adults to the potential dangers of COVID-19 pandemic. Iranian Journal of Public Health. 2020; 49(Suppl 1):122. [DOI:10.18502/ijph.v49iS1.3682]
- Roser M, Ritchie H, Ortiz-Ospina E, Hasell J. Coronavirus disease (COVID-19)-Statistics and research. Published Online at OurWorldInData.org. 2020. [Link]
- Noroozian M. The elderly population in iran: an ever growing concern in the health system. Iranian Journal of Psychiatry and Behavioral Sciences. 2012; 6(2):1-6. [PMID]
- Bajema KL, Oster AM, McGovern OL, Lindstrom S, Stenger MR, Anderson TC, et al. Persons evaluated for 2019 novel coronavirus-United States, January 2020. Morbidity and Mortality Weekly Report. 2020; 69(6):166-70. [DOI:10.15585/mmwr.mm6906e1] [PMID] [PMCID]
- Miresmaeeli SS, Esmaeili N, Sadeghi Ashlaghi S, Abbasi Dolatabadi Z. Disaster risk assessment among Iranian exceptional schools. Disaster Medicine and Public Health Preparedness. 2022; 16(2):678-82. [DOI:10.1017/dmp.2020.425] [PMID]
- Coelho CM, Suttiwan P, Arato N, Zsido AN. On the nature of fear and anxiety triggered by COVID-19. Frontiers in Psychology. 2020; 11:581314. [DOI:10.3389/fpsyg.2020.581314] [PMID] [PMCID]
- Shahyad S, Mohammadi MT. [Psychological impacts of Covid-19 outbreak on the mental health status of society individuals: A narrative review (Persian)]. Journal of Military Medicine. 2020; 22(2):184-92. [Link]
- Foodani MN, Abdulhusein M, Imanipour M, Bahrampouri S, Dolatabadi ZA. The relationship between professional quality of life and COVID-19 anxiety among nurses of emergency and intensive care units in najaf, Iraq. Journal of Nursing and Midwifery Sciences. 2023; 10(2):e135972. [Link]
- Riad A, Huang Y, Zheng L, Elavsky S. COVID-19 induced anxiety and protective behaviors during COVID-19 outbreak: Scale development and validation. MedRxiv. 2020. [Link]
- Mohammadpour M, Ghorbani V, Moradi S, Khaki Z, Foroughi AA, Rezaei MR. [Psychometric properties of the Iranian version of the coronavirus anxiety scale (Persian)]. Iranian Journal of Psychiatry and Clinical Psychology. 2020; 26(3):374-87. [DOI:10.32598/ijpcp.26.3482.1]
- Khademi F, Moayedi S, Golitaleb M, Karbalaie N. The COVID-19 pandemic and death anxiety in the elderly. International Journal of Mental Health Nursing. 2020; 30(1):346-9. [DOI:10.1111/inm.12824] [PMID] [PMCID]
- Meng H, Xu Y, Dai J, Zhang Y, Liu B, Yang H. Analyze the psychological impact of COVID-19 among the elderly population in China and make corresponding suggestions. Psychiatry Research. 2020; 289:112983. [DOI:10.1016/j.psychres.2020.112983] [PMID] [PMCID]
- Liu S, Yang L, Zhang C, Xiang YT, Liu Z, Hu S, et al. Online mental health services in China during the COVID-19 outbreak. The Lancet Psychiatry. 2020; 7(4):e17-8. [DOI:10.1016/S2215-0366(20)30077-8] [PMID]
- Scacchi A, Catozzi D, Boietti E, Bert F, Siliquini R. COVID-19 lockdown and self-perceived changes of food choice, waste, impulse buying and their determinants in Italy: QuarantEat, a cross-sectional study. Foods. 2021; 10(2):306. [DOI:10.3390/foods10020306] [PMID] [PMCID]
- Di Santo SG, Franchini F, Filiputti B, Martone A, Sannino S. The effects of COVID-19 and quarantine measures on the lifestyles and mental health of people over 60 at increased risk of dementia. Front Psychiatry. 2020; 11:578628. [DOI: 10.3389/fpsyt.2020.578628] [PMID]
- Balanzá-Martínez V, Atienza-Carbonell B, Kapczinski F, De Boni RB. Lifestyle behaviours during the COVID-19-time to connect. Acta Psychiatrica Scandinavica. 2020; 141(5):399-400. [DOI:10.1111/acps.13177] [PMID] [PMCID]
- Bernardo ABI, Mendoza NB, Simon PD, Cunanan ALP, Dizon JIWT, Tarroja MCH, et al. Coronavirus Pandemic Anxiety Scale (CPAS-11): Development and initial validation. Current Psychology. 2022; 41(8):5703-11. [PMID]
- Kumari A, Ranjan P, Vikram NK, Kaur D, Sahu A, Dwivedi SN, et al. A short questionnaire to assess changes in lifestyle-related behaviour during COVID 19 pandemic. Diabetes & Metabolic Syndrome. 2020; 14(6):1697-701. [DOI:10.1016/j.dsx.2020.08.020] [PMID] [PMCID]
- Wang ZH, Qi SG, Zhang H, Mao PX, He YL, Li J, et al. [Impact of the COVID-19 epidemic on anxiety among the elderly in community (Chinese)]. Zhonghua Yi Xue Za Zhi. 2020; 100(40):3179-85. [PMID]
- Rashedi V, Roshanravan M, Borhaninejad V, Mohamadzadeh M. [Coronavirus anxiety and obsession, depression and activities of daily living among older adults in Mane and Semelghan, 2021 (Persian)]. Salmand: Iranian Journal of Ageing. 2022; 17(2):186-201. [DOI:10.32598/sija.2022.1857.2]
- Sirin H, Ahmadi AA, Ketrez G, Ozbeyaz C, Dikmen AU, Ozkan S. Assessment of anxiety in elderly population during the COVID-19 pandemic and the impact of compulsory home-stay in the central districts of Ankara, Turkey: A quantitative, qualitative mixed method study. International Journal of Geriatric Psychiatry. 2021; 36(11):1785-94. [DOI:10.1002/gps.5600] [PMID] [PMCID]
- Ouanes S, Kumar R, Doleh ESI, Smida M, Al-Kaabi A, Al-Shahrani AM, et al. Mental health, resilience, and religiosity in the elderly under COVID-19 quarantine in Qatar. Archives of Gerontology and Geriatrics. 2021; 96:104457. [DOI:10.1016/j.archger.2021.104457] [PMID] [PMCID]
- Di Renzo L, Gualtieri P, Pivari F, Soldati L, Attinà A, Cinelli G, et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. Journal of Translational Medicine. 2020; 18(1):229. [DOI:10.1186/s12967-020-02399-5] [PMID] [PMCID]
- Robinson E, Boyland E, Chisholm A, Harrold J, Maloney NG, Marty L, et al. Obesity, eating behavior and physical activity during COVID-19 lockdown: A study of UK adults. Appetite. 2021; 156:104853. [DOI:10.1016/j.appet.2020.104853] [PMID] [PMCID]
- Hofman A, Limpens MAM, de Crom TOE, Ikram MA, Luik AI, Voortman T. Trajectories and determinants of physical activity during covid-19 pandemic: A population-based study of middle-aged and elderly individuals in the Netherlands. Nutrients. 2021; 13(11):3832. [DOI:10.3390/nu13113832] [PMID] [PMCID]
- Schuch FB, Bulzing RA, Meyer J, Vancampfort D, Firth J, Stubbs B, et al. Associations of moderate to vigorous physical activity and sedentary behavior with depressive and anxiety symptoms in self-isolating people during the COVID-19 pandemic: A cross-sectional survey in Brazil. Psychiatry Research. 2020; 292:113339. [DOI:10.1016/j.psychres.2020.113339] [PMID] [PMCID]
- Creese B, Khan Z, Henley W, O'Dwyer S, Corbett A, Vasconcelos Da Silva M, et al. Loneliness, physical activity, and mental health during COVID-19: A longitudinal analysis of depression and anxiety in adults over the age of 50 between 2015 and 2020. International Psychogeriatrics. 2021; 33(5):505-14. [DOI:10.1017/S1041610220004135] [PMID] [PMCID]
- Nagasu M, Muto K, Yamamoto I. Impacts of anxiety and socioeconomic factors on mental health in the early phases of the COVID-19 pandemic in the general population in Japan: A web-based survey. Plos One. 2021; 16(3):e0247705. [DOI:10.1371/journal.pone.0247705] [PMID] [PMCID]
- Goethals L, Barth N, Guyot J, Hupin D, Celarier T, Bongue B. Impact of Home Quarantine on physical activity among older adults living at home during the covid-19 pandemic: Qualitative interview study. Jmir Aging. 2020; 3(1):e19007. [DOI:10.2196/19007] [PMID] [PMCID]
Type of article: Research |
Subject:
Quantitative
Received: 2023/08/25 | Accepted: 2024/05/25 | Published: 2024/10/1
Received: 2023/08/25 | Accepted: 2024/05/25 | Published: 2024/10/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
