

Volume 9, Issue 3 (Spring 2024)
Health in Emergencies and Disasters Quarterly 2024, 9(3): 221-238 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Naseri F, Khosravizadeh O, Shahrestanaki Y A. Identifying and Conceptualizing the Improvement Dimensions of Pre-hospital Emergency Time Indicators in Qazvin City, Iran: A Qualitative Study. Health in Emergencies and Disasters Quarterly 2024; 9 (3) :221-238
URL: http://hdq.uswr.ac.ir/article-1-569-en.html
URL: http://hdq.uswr.ac.ir/article-1-569-en.html



1- Student Research Committee, Qazvin University of Medical Sciences, Qazvin, Iran., 1. Student Research Committee, Qazvin University of Medical Sciences, Qazvin, Iran
2- Social Determinants of Health Research Center, Research Institute for Prevention of Non-Communicable Diseases, Qazvin University of Medical Sciences, Qazvin, Iran. ,omid.khosravizadeh@gmail.com
3- Social Determinants of Health Research Center, Research Institute for Prevention of Non-Communicable Diseases, Qazvin University of Medical Sciences, Qazvin, Iran., 2. Social Determinants of Health Research Center, Research Institute for Prevention of Non-Communicable Diseases, Qazvin University of Medical Sciences, Qazvin, Iran
2- Social Determinants of Health Research Center, Research Institute for Prevention of Non-Communicable Diseases, Qazvin University of Medical Sciences, Qazvin, Iran. ,
3- Social Determinants of Health Research Center, Research Institute for Prevention of Non-Communicable Diseases, Qazvin University of Medical Sciences, Qazvin, Iran., 2. Social Determinants of Health Research Center, Research Institute for Prevention of Non-Communicable Diseases, Qazvin University of Medical Sciences, Qazvin, Iran
Full-Text [PDF 702 kb]
(555 Downloads)
| Abstract (HTML) (2353 Views)
Full-Text: (489 Views)
Introduction
In response to the rising prevalence of illnesses, trauma, and cardiovascular conditions and the universal entitlement to healthcare, encompassing pre-hospital emergency medical services (EMS), the World Health Organization (WHO) advocates for the incorporation of EMS as an indispensable and vital constituent within the healthcare framework [1]. EMS goes beyond traditional, disease-focused areas to address a wide range of sudden illnesses and injuries that have a significant impact on mortality and disability, especially in economies with limited to moderate financial resources. Accordingly, providing prompt medical attention is an effective strategy for reducing the global burden of disease [2]. Baron Jean Laurie pioneered the arrangement and delivery of emergency services during the German-Austrian conflict with France. Similarly, in Iran, the inception of these services occurred after the tragic incident of the Mehrabad Airport roof collapse in 1978, resulting in multiple casualties [3]. In all nations, EMS is regarded as the primary component for delivering health and treatment services, and their definition is as follows: EMS constitutes an all-encompassing system that addresses the medical requirements of individuals who are injured or suffering from acute and emergent illnesses, beyond the confines of healthcare facilities, before and during their transition to a suitable medical facility [4]. The primary objective of the EMS system is to offer services that meet consumers’ expectations, optimize time efficiency, and fulfill the requirements of patients experiencing urgent and critical circumstances within the shortest timeframe possible while upholding safety standards [5]. In numerous global regions, particularly in low and middle-income nations, EMS infrastructure is less advanced, and the effectiveness of the healthcare system falls short of being satisfactory [6]. In Iran, despite notable advancements in this domain, such as the expansion of bases, the augmentation of ambulance fleets, the enhancement of equipment quality, the enlargement of the workforce, and the incorporation of air ambulances (helicopters), motorized ambulances, and ambulance buses, a multitude of issues and inadequacies persist [7]. In Iran, the pre-hospital services association is linked to the medical oversight hubs, the national emergency entity, and the Ministry of Health and Medical Education. By dialing 115, individuals can access these services. Currently, the national emergency agency holds the responsibility for devising comprehensive strategies, directives, and regulations about pre-hospital EMS [8]. The management centers for accidents and medical emergencies at the provincial level in Iran are overseen and supported by the respective provincial medical sciences universities. Nearly 80% to 85% of EMS in the country involves the transportation of individuals with acute medical conditions to healthcare facilities [9]. Pre-hospital emergency services serve as the first point of contact in the healthcare system for individuals experiencing acute and emergency conditions. They have a crucial frontline role in managing and responding to emergencies within the healthcare system [4, 9]. The primary responsibility of EMS is to oversee and regulate the care of patients facing acute and urgent circumstances. The efficient and timely management of emergency cases by EMS plays a vital role in reducing morbidity and mortality rates [10].Consequently, during instances of accidents and internal emergencies, these attentions commence at the patient’s side, offering suitable medical treatment at the correct location and moment, utilizing the accessible resources, and ultimately guiding the patient to the hospital’s emergency department [8]. Estimates from 40 countries indicate that emergency medical care can prevent 54% to 90% of fatalities and reduce the burden of disease by 900 million to 2.5 billion disability-adjusted life years in low- and middle-income countries [11]. The efficient functioning of medical emergency centers in terms of time is crucial for the management and control of emergency patients and medical emergencies. This reduces mortality and morbidity but also facilitates the burden on hospitals during times of crisis, emphasizing the significance of pre-hospital care. To enhance their capabilities and effectively respond to urgent situations, emergency medical centers must be cognizant of their performance during critical scenarios. They must gather this valuable information and use it as a foundation for improvement and preparedness in handling acute situations. This study is conducted considering the research conducted in this area and recognizing the significance of time factors within the pre-hospital emergency system. Nevertheless, despite the criticality of the matter, no prior investigations had been carried out in Qazvin Province, Iran. Therefore, employing a qualitative approach, we identified the influential factors that enhance the performance of pre-hospital emergency time indicators and proposed solutions to ameliorate the situation.
Materials and Methods
The objective of the current research is to identify and extract the key elements that contribute to enhancing the performance of six time-based metrics endorsed within pre-hospital emergency services. These metrics include seconds delay time, response time, scene time, total run time, transport time, and round trip time (the detailed explanations of the indicators are in Table 1).

Given that selecting a qualitative methodology for research is suitable when the intention is to explore a novel area using an exploratory technique or to approach it from an innovative angle, this study utilizes a qualitative approach alongside an analytical methodology to attain the objective of this study. The content that has been recommended is also integrated into the approach.
Study population
The key informants and experts in the field of pre-hospital emergency, including the officials of the emergency organization, academic staff members, technicians, and specialist doctors residing in the emergency departments of educational and treatment centers formed the research community. Furthermore, a purposive sampling technique was employed. Additionally, considering that qualitative studies do not adhere to a precise sample size criterion, the sampling process in the current study persisted until data saturation was achieved. The prerequisites for study participation included having substantial expertise and experience in pre-hospital emergency services, relevant work history, as well as a notable interest and motivation to partake in the research.
Data collection method
The instrument used for data collection was a semi-structured interview guide. To craft this guide, insights from educators and advisors, in addition to a review of pertinent literature, were harnessed. This guide encompassed broad inquiries to elicit open-ended responses (Figure 1).
 Upon receiving individuals’ consent, their verbal contributions were recorded and notes were written. Prior arrangements were made with the participants before the interview sessions. After furnishing comprehensive clarifications regarding the research objectives, the interviews were exclusively carried out following the acquisition of their informed agreement. Furthermore, all audio and written records were stored anonymously, and the identities of the interviewees were withheld in the research findings.
Upon receiving individuals’ consent, their verbal contributions were recorded and notes were written. Prior arrangements were made with the participants before the interview sessions. After furnishing comprehensive clarifications regarding the research objectives, the interviews were exclusively carried out following the acquisition of their informed agreement. Furthermore, all audio and written records were stored anonymously, and the identities of the interviewees were withheld in the research findings.
Data management and analysis process
To dissect the qualitative data procured from the interviews, the content analysis technique was employed. This approach was executed through a sequence of three phases, involving data condensation, data augmentation, and categorization, along with subsequent analysis. During this phase, the initial step involved transcribing all the interviews following attentive listening and thorough examination. Subsequently, the researcher proceeded with coding the statements and categorizing them. Ultimately, upon concluding this process, the outcome of this research stage materialized as the identification of dimensions and elements that impact the enhancement of pre-hospital emergency time metrics. These aspects were distilled into distinct themes through the analysis of the interview responses.
Results
In pursuit of the research objective, 10 principal sources of information were engaged in the interview process. Out of the interviewees, 9 individuals (90%) were male and the remaining 1 individual (10%) was female. All participants held at least a bachelor’s degree in terms of educational attainment. A majority of the interviewees occupied the role of foundational staff within the educational and medical establishments in Qazvin City, Iran (Table 2).

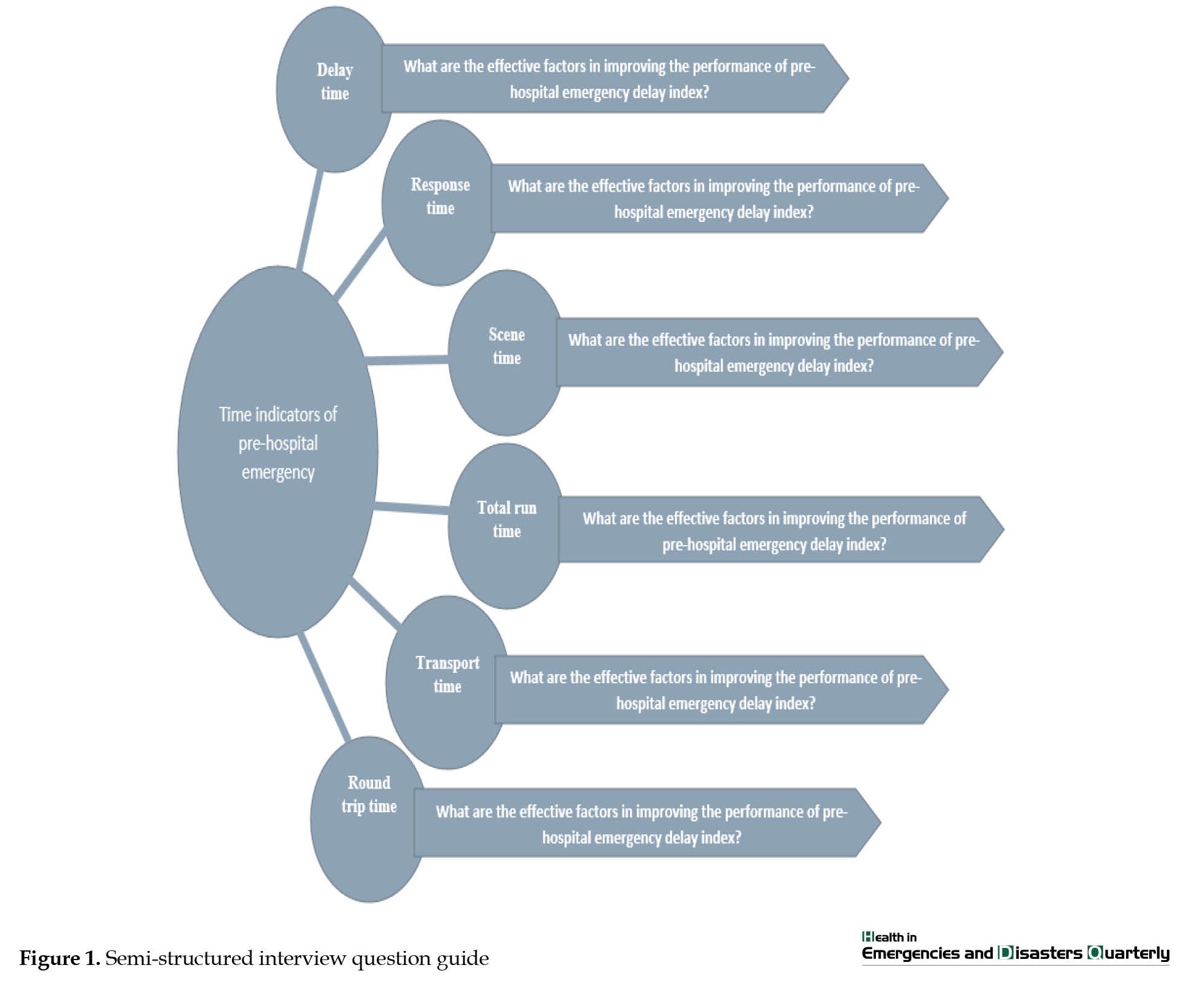
Initially, a comprehensive transcription of the interviews with prominent specialists was conducted, following attentive listening and thorough assessment. Subsequently, the qualitative findings of the study are written. The statements were elucidated and assigned codes, with the outcomes being presented as 14 dimensions and 41 influential constituents contributing to the enhancement of pre-hospital emergency time benchmarks (Table 3).
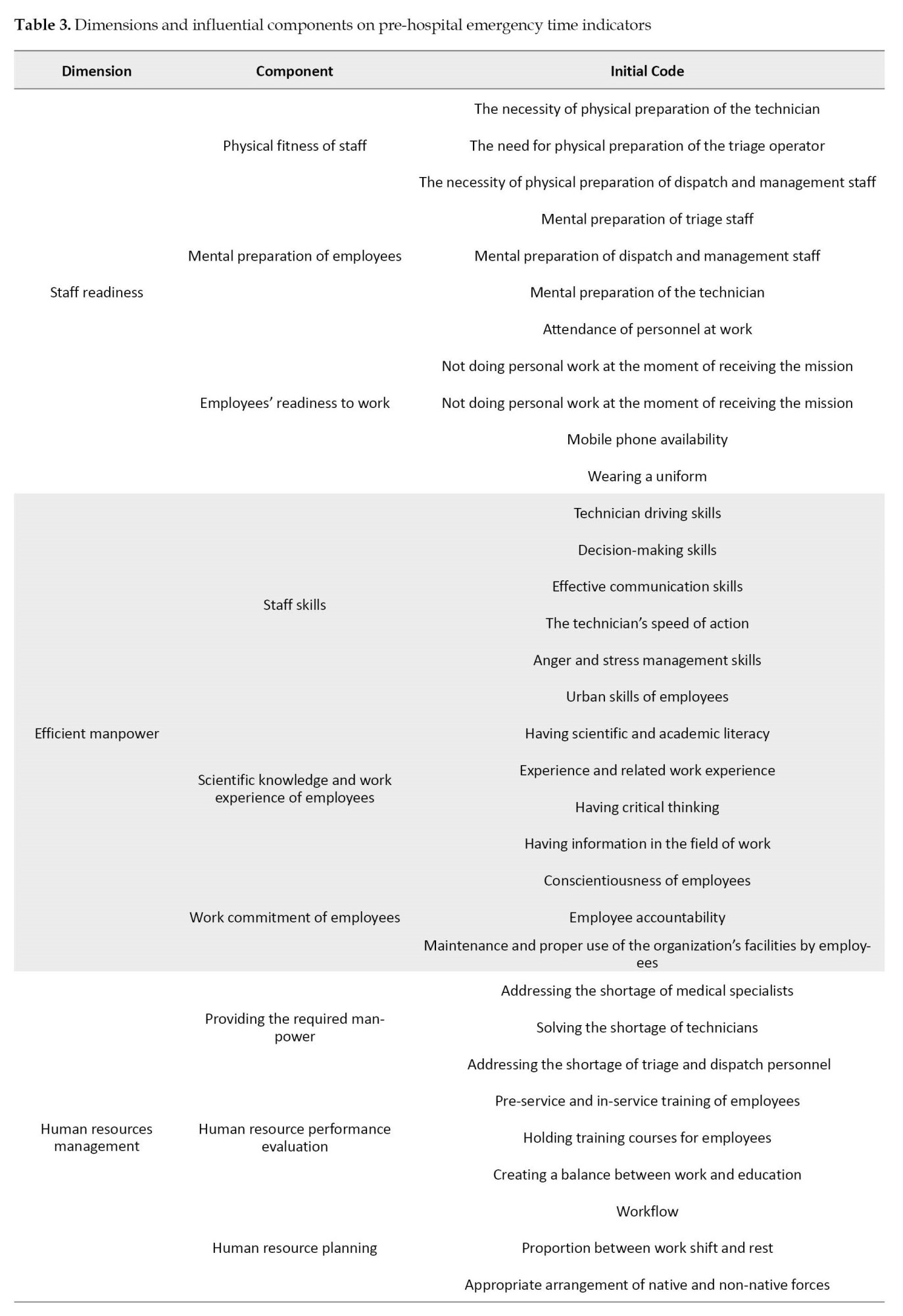

In the subsequent sections, discussions revolve around the themes and sub-themes derived from the interviews. A concise portrayal of their structure is provided, along with references to significant phrases associated with each aspect of the interviewees’ contributions.
Staff readiness
Every person interviewed shared the belief that the preparedness of the personnel is among the key elements contributing significantly to the enhancement of time measures in pre-hospital emergencies. In other words, the level of readiness exhibited by the on-duty personnel for prompt responsiveness. The staff’s preparedness to execute tasks entails various instances, such as when a mission is communicated to the base, but a technician is engaged in personal tasks, resulting in a delay for the ambulance to depart from the base. Consequently, employees must be prepared and abstain from personal tasks when they receive a mission. In this regard, experts pointed to components such as Physical fitness of staff Mental preparation of employees, and employees’ readiness to work.
Regarding this case, the interviewee P-9 maintained the following opinion
“Compiling health records can be beneficial. For example, a triage nurse in good physical and mental condition can manage the mission effectively, obtaining accurate addresses, ensuring smooth mission transfers, and facilitating clear communication between the technician and the patient. A technician experiencing issues, such as back pain or knee pain would face challenges in evacuating a patient from higher floors. Similarly, a technician with psychological distress is at a disadvantage in establishing effective communication and comprehending a patient’s pain and distress to provide adequate relief. This underscores the significance of upholding both the physical and mental well-being of the personnel”.
Efficient manpower
Each participant shared the view that effective personnel play a role in influencing time metrics. When discussing the efficacy of the workforce, it implies their capacity to competently manage tasks, possess educational proficiency alongside their skills and capabilities, and exhibit a strong commitment to the organization’s mission. In this dimension, the components, such as staff skills, scientific knowledge and work experience of employees, and work commitment of employees to the organization have been mentioned.
Regarding this dimension, the participant P-3 stated the following opinion
“Enhancing time indicators in medical emergencies relies on the effectiveness and dedication of human resources, as every moment and second holds immense value. The dedication of individuals plays a crucial role in saving patients' lives. Technicians, with their expertise, are the primary resource for assisting during critical moments. The level of dedication within an individual can be decisive in emergencies. Additionally, this commitment is influenced by various factors, such as compensation, salaries, benefits, and overall satisfaction with the organization, which are management-related aspects. It is believed that satisfied individuals are more likely to perform their job proficiently”.
Additionally, in this regard, the participant P-10 maintained the following opinion
“Proficiency in interacting with callers or their companions is a crucial skill in emergencies. In unique scenarios, these individuals may be restless, agitated, and under significant stress, demanding the dispatch of an ambulance without fully understanding the situation. The triage operator attempts to engage them by asking a series of questions; however, sometimes the caller becomes even more agitated and resorts to yelling. If the triage operator lacks skills in stress and anger management, as well as effective communication, the interaction can be disrupted, leading to a prolonged process. This elongation of time can be problematic considering the need for time management. Therefore, it is imperative to possess skills, such as anger management, stress management, effective communication, and academic proficiency in handling such situations”.
Human resources management
The participants reached a consensus on this measure, which essentially stands as one of the most effective approaches to enhance pre-hospital emergency time metrics. This consensus considers the shortage of personnel in connection with the realm of human resources management, emphasizing the necessity for resource provisioning and strategic human resources planning. The interviewees mentioned various components, such as providing the required manpower, human resource performance evaluation, and human resource planning.
In terms of this issue, interviewee P-3 stated the following opinion
“There is a shortage of personnel in various areas, including the triage unit, dispatch, and the count of technicians and physicians. Some individuals are forced to work consecutive shifts at the bases for two or three days, resulting in a decline in overall effectiveness. This decrease in work efficiency raises concerns about human resources. It is crucial to prioritize addressing this issue and finding a viable solution to alleviate the strain and ensure adequate staffing levels for optimal performance”.
Also, in confirmation of this dimension, the participant P-2 stated the following opinion
“We need to ensure that we allocate personnel in a manner that avoids extended shifts while maintaining efficiency as a priority. Our approach should involve offering amenities and support that coincide with minimized workloads for the staff, ultimately enabling us to deliver optimal services and cater to the workforce effectively”.
Infrastructure and organizational facilities
The participants held the viewpoint that infrastructure and organizational amenities constitute crucial elements in enhancing pre-hospital emergency time metrics. This is because even if resources are scarce, such as ambulances or equipment, expecting significant improvements in indicators would be unrealistic. They pointed to components, such as establishment facilities, efficient ambulance fleet, proportion of the number of bases to the population, and creating a suitable and low-stress environment for the communication center, which can be effective in improving these indicators.
In confirmation of this statement, interviewee P-1 mentioned the following opinion
“The classification pertains to the organization, system, and arrangement. For instance, numerous bases lacked a designated parking area for ambulances. Lately, there are reports of new parking facilities being constructed; however, the functionality of these parking entrances becomes a concern, whether it is manual operation or electronic mechanisms”.
Regarding the given aspect, the participant P-4 stated the following opinion
“Enhancing indicator performance involves a crucial facet– the expansion of facilities. On the provincial level, there is a distinct lack of bases, and numerous factors are contingent upon this shortfall, stemming from a deficit in the base development strategy. For instance, Qazvin City (Iran) currently falls short of the latest population standard, which dictates the need for one base per 20 000 residents. Abiding by this guideline, Qazvin City faces a substantial shortage of around 10 to 12 bases, significantly influencing the situation”.
Communication and information technology management
The specialists thought that the configuration of the emergency communication center holds substantial potential for enhancing indicators, particularly the index related to time delays. This setup should encompass several tiers that can uphold ongoing connections in the event of a failure in one layer. They pointed to components, such as the first line of emergency response, radio communication system, telephone communication system, and the Internet communication system which can be effective in improving the indicators.
In this case, the interviewee P-4 stated the following opinion
“The integration of 115 response operators has contributed to the enhancement of pre-hospital emergency service efficiency. In the past, response times were more extended, compounded by the absence of skilled personnel at the bases. Only individuals with diplomas were available to assist, and this was especially problematic as female staff could not be employed at road bases. Moreover, centralization has also played a role in ameliorating time indicators”.
Also, regarding this dimension, the interviewee P-8 stated the following opinion
“The presence of multiple communication tiers is crucial in both pre-hospital and hospital operations. This includes landline, mobile phone, and internet communication. Enhancing wireless communication strengthens various systems, such as phone networks, the Asayar system, internet connectivity, and intranet capabilities. The current use of communication layers in the pre-hospital domain, including Asayar, internet, wireless, and telephone, is deemed insufficient. Transitioning from the internet platform to the intranet platform is the next step to enhance security. Expanding communication layers is essential to connect dispatch centers, bases, hospitals, and centers, ensuring effective communication among these entities”.
Smart automation
Specialists held the view that technology can play a significant role in enhancing indicators, as time is critical in emergencies, and the application of technology accelerates processes, thereby effectively contributing to the improvement of time metrics. They pointed to components, such as routing technologies and specialized application software.
Regarding this dimension, the interviewee P-3 stated the following opinion
“At present, there exists a set of software that can transmit the mission address location to ambulance smartphones; however, our progress in this aspect is still lacking. Current internet maps need to be advanced to display the precise real-time position of the ambulance while it is in transit. This involves software solutions and GPS technology, which need to be operational in ambulances”.
Additionally, in this case, the participant P-5 stated the following opinion
“Telemedicine was initially introduced into the emergency system for online electrocardiography recording and its primary function remains the same. Depending on the capabilities of the monitoring device, telemedicine enables remote monitoring of acute and critical patients during transit, including subjects with blood pressure concerns. These devices are equipped with digital features, such as pulse oximeters. While telemedicine is incorporated into ambulance protocols, the current capacity in Qazvin City does not allow for directly obtaining online electrocardiography readings”. “Initially introduced into the emergency system solely for online electrocardiography recording, telemedicine’s primary function remains consistent. Depending on the capabilities of the monitoring device, it can facilitate the remote monitoring of acute and critical patients during transit, encompassing individuals with blood pressure concerns. These devices are equipped with digital features including pulse oximeters. While telemedicine is incorporated into ambulance protocols, our current capacity in Qazvin City does not extend to directly obtaining online electrocardiography readings”.
Influential environmental factors
Specialists held the belief that external environmental factors beyond the organization play a crucial and impactful role in time indicators. The participants pointed to components, such as weather conditions, traffic situation, and distance and state of transportation routes.
The participant P-10 stated the following opinion
“One of the major challenges in Qazvin City is the traffic behavior on the roads, especially during specific periods, such as school closures and afternoon shopping. This constant issue makes navigating certain streets difficult, especially for ambulances trying to reach a location. Traffic patterns and people’s driving etiquette have a significant impact on response time. Moreover, the quality of the road surface in certain areas is crucial. Sometimes, the bases are located at a distance from the road, requiring the ambulance to find a parking spot before joining the main road. Unpaved roads, dirt tracks, and obstacles like elevated structures also contribute to longer travel distances. These factors collectively affect emergency response time indicators”.
Patient-related factors
Nearly all the specialists concurred that a range of factors associated with the patient and their condition exert an influence on time indicators. According to the interviewees, this aspect holds notable sway over the time index about arriving at the scene, as well as the time index related to any delays in providing information to the operator for collaboration. However, it bears the most substantial impact on the index concerning the attendance stage. They pointed to components, such as patient cooperation and clinical status.
Regarding this case, the interviewee P-1 mentioned the following opinion
“Consider this scenario, I am a technician, I have arrived at the scene, managed the situation, evaluated the patient’s condition, and completed all necessary tasks swiftly. I am ready to move the patient since, as a human technician, I can initiate patient transfer with appropriate authorization. Nevertheless, this is where the human element comes into play. Both the patient and individuals around them can influence this step. Sometimes, even the patients might resist or withhold permission for the transfer. Cultural nuances might also come into play, leading to debates. For instance, a patient might decline to transfer to the hospital, stating that their spouse needs to be informed first”.
Also, participant P-6 emphasized this dimension in the following opinion
“The timeframe differs based on the patient’s clinical state. For instance, in a critical situation, such as cardiac arrest, we might need to administer cardiopulmonary resuscitation for as long as 45 min. Conversely, a patient might have an issue necessitating treatment, such as administering serum therapy to elevate blood pressure, which could take around 20 min to observe improvement and subsequently facilitate transfer. Alternatively, if the patient has suffered trauma, a sequence of interventions might be necessary. In certain instances, immediate transfer might be imperative”.
Influential factors of stage management
According to specialists, the efficient handling of stages by technicians plays a pivotal role in enhancing time indicators. Every accident scene presents unique circumstances that need to be carefully considered, guiding decisions and actions accordingly. They mentioned components, such as security of the accident scene, safety of the accident scene, and unsettled atmosphere at the scene of the incident.
Regarding this case, the participant P-6 stated the following opinion
“During altercations, especially incidents involving gunfire, it is crucial to secure the scene before a technician can safely approach the patient. However, there is often a delay of approximately 30 min before the police arrive at the location to provide additional security. This delay extends the overall process, taking around 30 to 40 min before the scene is fully secured and the technician can attend to the patient”.
In confirmation of this issue, the participant P-9 stated the following opinion
“Our colleagues often face challenges when responding to accidents due to the excessive influx of people at the scene. This large gathering of individuals can hinder proper scene management and the technician’s ability to carry out effective triage. Triage involves quickly assessing patients to determine their need for immediate attention or lower priority. The noisy and agitated behavior of patients with lower priority (green category) can draw more attention, diverting resources from those in critical condition. Additionally, the emotional impact of a deceased patient tends to attract the crowd’s attention, even though they may not have the necessary medical knowledge to accurately assess the severity of patients’ conditions”.
Adherence to national guidelines
Every participant shared the perspective that national guidelines play a crucial role in enhancing pre-hospital emergency time indicators. These directives function as a navigational guide, offering recommended steps to follow in diverse scenarios. They mentioned various components, such as care protocols and star protocols.
In this regard, the participant P-2 stated the following opinion
“Protocols are in place for both on-scene conditions and telephone triage colleagues, and they diligently follow these protocols. The instructions guide the appropriate actions to take based on specific indicators. Similarly, technician colleagues also follow a set of offline and online protocols that dictate their actions upon arriving at the scene. These protocols ensure a systematic approach and consistent care throughout the process”.
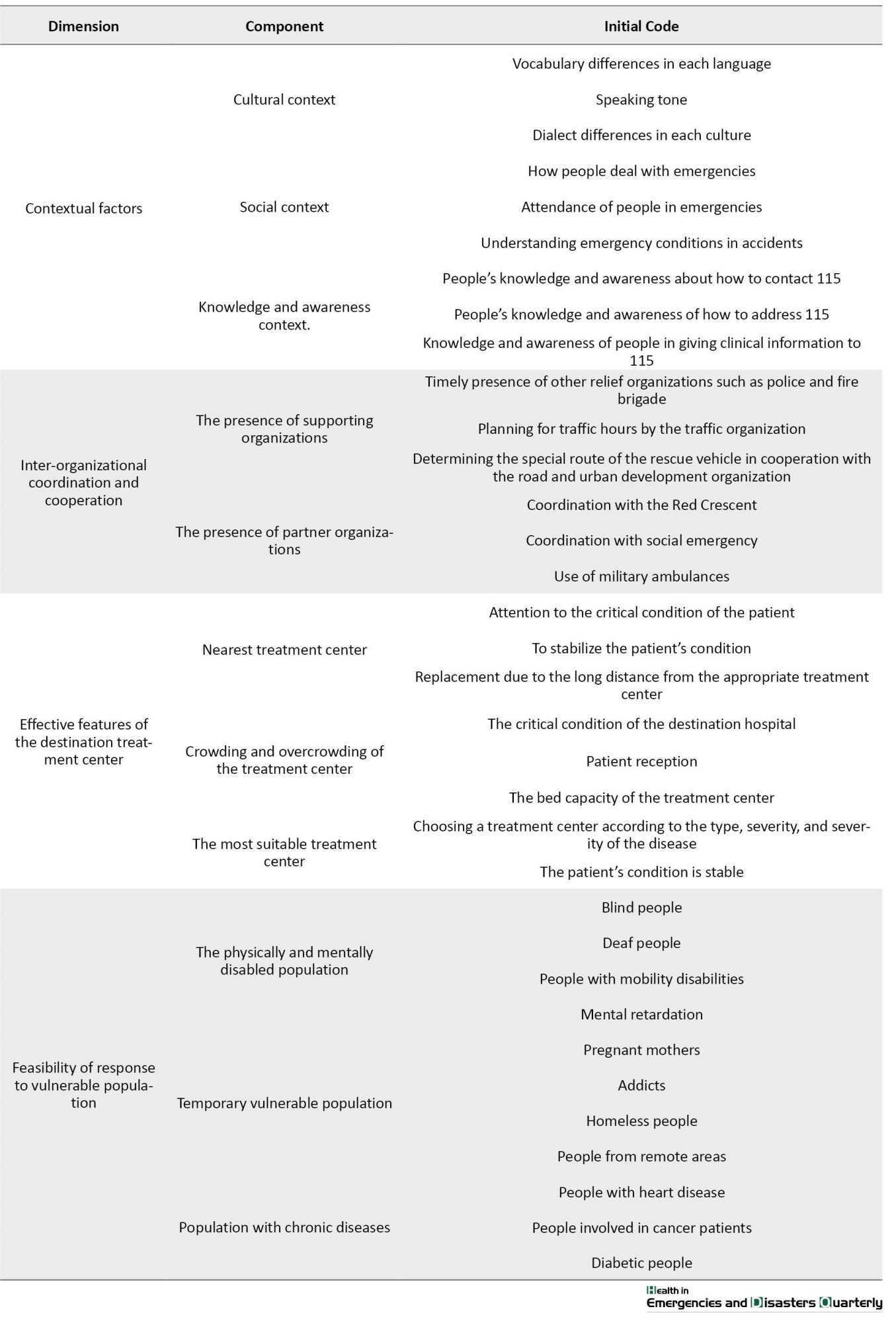
Contextual factors
According to the experts in this study, delivering EMS services is influenced by societal dynamics, cultural norms, and related matters. These aspects, known as contextual factors, play a pivotal role. This is because people’s conduct is shaped within the framework of society and culture. They mentioned components, such as cultural context, social context, and knowledge and awareness context.
In this regard, the interviewee P-10 stated the following opinion
“The presence of a crowd at the accident site leads to disorderliness, often instigated by companions or bystanders. The technician’s efforts to carry out on-site assessments can be hampered due to threats and coercion, exerted through pressure tactics that compel rapid patient retrieval and departure. Individuals who lack medical knowledge tend to intervene, and their interference can disrupt the technician’s tasks”.
In this case, the participant P-8 stated the following opinion:
“An individual providing information as a patient offers basic details, and public awareness significantly aids the triage process by helping the triage assess whether the case is an emergency warranting an ambulance dispatch. If the informant possesses a range of general information, they can provide more accurate guidance. It could be beneficial for the emergency department to create educational pamphlets, organize informative radio programs, and other resources for the general public”.
Inter-organizational coordination and cooperation
The majority of experts shared the viewpoint that the effective enhancement of time indicators is influenced by the coordination and collaboration among emergency-related organizations. They mentioned various components, such as the presence of supporting organizations and the presence of partner organizations.
The participant P-5 stated the following opinion in this regard:
“When discussing collaboration with the Ministry of Roads and Urban Development, the focus shifts to roads and highways. For instance, on highways, a technician in an ambulance might find themselves in a traffic jam for two kilometers due to an accident ahead. Then, the question arises of how the ambulance can navigate this situation effectively. Here, the involvement of the Ministry of Roads and Urban Development becomes crucial. If designated lanes exclusive to emergency vehicles are established, where no other vehicles are allowed to pass, and stringent penalties are imposed for violations, the ambulance can utilize these lanes to bypass traffic congestion. This way, the ambulance can navigate through traffic effectively, benefiting from the special lane privileges”.
Regarding this dimension, the interviewee P-7 stated the following opinion:
“Concerning the interactions between the emergency organization and relevant entities, over the past three years, we have engaged in multiple discussions with the Red Crescent and the 123 hotline. In the realm of social emergency-related organizations, there should ideally be a comprehensive engagement, involving numerous entities. In some instances, the situation might not qualify as a critical emergency but requires assistance from social emergency services. Here, coordination is essential. In terms of collaboration with the Red Crescent, fortunately, there have been no issues, and our efforts have aligned seamlessly”.
Effective features of the destination treatment center
The specialists held the view that the attributes of the destination treatment facility, including proximity to the accident site, alignment with the patient’s clinical state, and the ability to accommodate the patient, contribute significantly to the enhancement of time indicators. They mentioned various components, such as the nearest treatment center, crowding, and overcrowding of the treatment center, and the most suitable treatment center.
Also, in this case, the participant P-1 stated the following opinion:
“The technician assesses the patient’s condition to determine the appropriate medical facility for comprehensive treatment. While initial care and treatment are provided at the scene, it is crucial to transport the patient to a specialized medical center for definitive treatment. For example, a cardiac patient would be transferred to a heart center, while a trauma case requires a trauma center. In cases where the patient has a combination of injuries, such as burns and trauma, the technician must identify the appropriate treatment center. The technician’s diagnosis is significant, as well as considering the distance between the accident site and the designated treatment center”.
Feasibility of response to vulnerable population
Certain specialists thought that implementing initiatives aimed at aiding the vulnerable population could prove efficacious in enhancing time indicators and elevating the pre-hospital emergency services’ efficacy. They mentioned components, such as physically and mentally disabled and temporarily vulnerable populations with chronic diseases.
About this subject, the interviewee P-10 maintained the following opinion:
“As someone actively involved in this field, I observe that we often overlook the marginalized segments of our society. It is important to clarify that when I mention minorities, I am not referring to religious minorities. Rather, I am addressing various marginalized groups within society, including individuals with distinct disabilities, like cognitive challenges or physical impairments. The pressing question is how we can facilitate their access to the emergency medical system and how we can ensure that they can effectively engage with and benefit from emergency services tailored to their specific needs”.
Discussion
In discussing the dimension of staff readiness, ensuring the physical, mental, and psychological preparedness of staff members is an essential and requisite characteristic of this profession. Creating health records can serve as a beneficial approach in this context. The physical and mental well-being of employees significantly impacts the performance of emergency services, spanning from the initiation of a mission to its completion. Additionally, the notion of employees’ preparedness for swift responses pertains to their availability at their designated workstations and their readiness to accept and execute missions promptly. Supporting this dimension, the work of Moradian et al. [12], and Bayrami et al. [13] substantiates these ideas, aligning with the current research. Regarding the efficient manpower dimension, it signifies that employees are proficient in managing their assigned responsibilities, and this proficiency, coupled with their skills, knowledge, quick decision-making, diligence, and sense of accountability, enhances the effectiveness and output of pre-hospital emergency operations. Within EMS, the competence of the workforce plays a crucial role in enhancing time-related performance metrics. These metrics are associated with individual capabilities, and the organization can enhance these capacities through the implementation of training sessions and hands-on exercises, such as simulations. This concept is supported by the research conducted by Seyyednozadi et al. [14], Khanke et al. [15], and Dadashzadeh et al. [16] as referenced. Regarding the conceptual dimension of human resources management, within the pre-hospital emergency system, it is crucial to recruit and employ personnel with both robust physical strength and mental well-being. Subsequently, after recruitment, consistent assessment of personnel performance by human resources management becomes imperative. Additionally, given the demanding nature of emergency work, adherence to proper work and rest standards is essential, and to counteract the attrition associated with emergency roles, a rotation system, such as the 115 job rotation should be implemented. This approach enhances the efficacy of staff engagement, thereby contributing to the improvement of time-related performance metrics in pre-hospital emergency services. This perspective is reinforced by Khanke et al.’s research [15], Yadollahi et al.’s study [17], and Azami-Aghdash et al.’s investigation [7], which all align with the concepts highlighted in the present study. In elucidating the dimension related to infrastructure and organizational facilities, the emergency organization holds the responsibility of furnishing the necessary infrastructure and amenities to enhance the efficiency of emergency services. This enhancement is a pivotal factor in reducing the duration of critical indicators. In this context, the availability of essential elements, such as 115 ambulance stations with dedicated parking spaces and emergency vehicles holds paramount importance. These vehicles play a critical role in swiftly transporting emergency responders to accident scenes and facilitating patient transfer to medical facilities. Ensuring the technical soundness of these vehicles is imperative. Furthermore, the physical workspace for employees should also be appropriately designed. Support for this perspective can be drawn from Moradian et al.’s study [12] and Sabouri et al.’s research [18], both of which align with the concepts presented in this study. Regarding communication and information technology management, emergency 115 operates with diverse communication tiers, facilitating information exchange through these levels. Employing contemporary and diverse communication technologies consistently can safeguard the organization’s information. In situations where one communication layer experiences disruption, the subsequent layer steps in seamlessly to ensure uninterrupted communication. Consequently, the proficient management of communication and information technology significantly contributes to the enhancement of time-related performance indicators. This view is corroborated by Ahmadi Dashtiyan et al.’s research [5] and is also echoed in Olave-Rojas et al.’s study [19] both aligning with the concepts highlighted in the present study. Concerning the make smart dimension, technology accelerates tasks and the proliferation of intelligent devices holds the potential to expedite operations. In the context of pre-hospital emergency services, leveraging specialized software, such as the Asayar system in place of traditional paper-based systems, utilizing GPS for optimized routing, and incorporating smart tools, including telemedicine can all contribute to enhancing time-related performance metrics. This viewpoint is reinforced by the research conducted by Gaeeni et al. [20], which aligns with Azami-Aghdash et al.’s study and Hajinabi et al.’s investigation, both of which resonate with the themes explored in the present study [7, 21]. In considering the interpretation of the influential environmental factors dimension, external environmental elements encompass influences on organizational performance that lie beyond the organization’s jurisdiction. Consequently, devising strategies and preparing to counteract these influences, while simultaneously aligning the organization to them, can assist in effectively addressing these external factors. Such preparedness contributes to the efficacy of enhancing pre-hospital emergency indicators. This perspective is supported by the research conducted by Ahmadi Dashtiyan et al. [5], and Seyyednozadi et al. [14], both of which substantiate the ideas explored in this study. Regarding the patient-related dimension, this factor exerts a more substantial influence on the on-scene presence indicator. The conduct of the patient’s companions and the demeanor of the patient upon initial interaction with the emergency staff can markedly affect the team’s morale and efficacy. Supporting this viewpoint, Alrazeeni, et al. [22], and Cui et al. [23] have addressed this facet, aligning with the current research. Continuing to discuss the influential factors of scene management, when dealing with an accident scene, an immediate and preliminary evaluation of various aspects is vital. This includes categorizing the nature of the incident, assessing its scale, estimating the extent of damage, and gauging the number of casualties. The insights gathered during this initial phase contribute to gauging the urgency of the situation, thereby impacting the time-related indicator for on-scene presence. Each accident scene presents its unique circumstances, necessitating thorough consideration and subsequent decision-making based on these specific conditions. Regarding the facet of Adherence to national guidelines, there exist prescribed protocols within pre-hospital emergency services. These protocols function as navigational tools in diverse scenarios, offering recommended actions to be undertaken. Consequently, abiding by these guidelines and implementing them can be impactful in enhancing time-related performance indicators. This perspective is corroborated by Alrazeeni et al.’s research, which aligns with the themes of the present study [22]. When discussing contextual factors, societal norms, cultural considerations, and matters linked to people’s awareness of EMS play a significant role. Various factors, such as the capacity to provide medical history and the propensity for cooperation with EMS are instrumental in augmenting the effectiveness of pre-hospital emergency services and related time-based benchmarks. Khanke et al.’s study [15] and Seyyednozadi et al.’s research [14] lend support to these aspects and align with the present study. The inter-organizational coordination and collaboration aspect pertains to the interaction between various entities concerning EMS. These entities can be categorized into two types as follows: Those directly aligned with emergency response and those providing auxiliary support to emergencies. When effective coordination and cooperation are established between emergency services and these organizations, it can positively impact the enhancement of time-related performance measures. Azami-Aghdash et al.’s study [7] and Khanke et al.’s research underscore this dimension, aligning with the themes addressed in the present study. In the subsequent exploration of effective features of the destination treatment center, when a patient is transferred to a treatment center, there is often limited information available about the conditions of that specific hospital. Therefore, the selection of the appropriate hospital based on the patient’s clinical condition and the hospital’s capacity becomes crucial for the patient’s acceptance and effective care. The promptness of patient admission to the treatment center is a significant factor, directly impacting the reduction of time-related indicators. This dimension was also highlighted by Seyyednozadi et al. [14] in their study, aligning with the themes addressed in the present research. Regarding the practicality of Feasibility of response to vulnerable populations, implementing a dedicated program targeted at these groups can significantly enhance both time-related indicators and the overall efficacy of pre-hospital emergency services.
Conclusion
In this qualitative study, different dimensions, including personnel readiness, organizational infrastructure, patient-related factors, inter-organizational coordination, receiving treatment facility attributes, and responsiveness to vulnerable populations have been examined and analyzed. The findings indicate that diverse dimensions, such as staff preparedness, communication technologies, facilities, cultural and social variations, inter-organizational collaboration, attributes of the receiving treatment center, and specialized programs for vulnerable communities play significant roles in improving pre-hospital emergency time indicators. Overall, the article underscores the importance of effective planning and management across these diverse dimensions, which can lead to notable enhancements in the performance and time indicators of pre-hospital emergency services. It is important to recognize that vulnerable populations vary across different contexts and domains. Consequently, it becomes essential to identify diverse vulnerable groups and assess their specific requirements for emergency services. This information serves as a basis for devising tailored strategies that cater to the distinct needs of these groups, ultimately ensuring their benefit from the provided services.
Future study suggestions
Given the significant impact of collaborative and supportive organizations in joint initiatives, it is advisable to organize joint programs, facilitate information exchange meetings, and establish communication pathways to enhance coordination with these entities.
Enhancing the provision of education and training courses for emergency personnel can lead to the augmentation of their capabilities and skills, thereby contributing to the enhancement of the emergency unit’s performance.
Allocating resources to sophisticated communication technologies like software solutions, visual communication systems, and GPS mapping has the potential to enhance real-time communication and boost operational efficiency.
Conducting further research and studies in critical domains concerning performance and time aspects can lead to sustained enhancements in the effectiveness of pre-hospital emergency services.
Implementing targeted initiatives and efficient strategies to address the requirements of susceptible communities can contribute to the enhancement of time and efficacy indicators in delivering emergency services.
Ethical Considerations
Compliance with ethical guidelines
The present study has been registered in the Ethics Committee of Qazvin University of Medical Sciences with the (Code: IR.QUMS.REC.1400.472). Before commencing each interview, implicit approval was acquired from the participants for the audio recording of their dialogue. Moreover, they were apprised that they retained the prerogative to abstain from cooperating or sharing their experiences at any point in the research process. Given that the confidentiality of data is mandatory in all research endeavors, this aspect was also meticulously upheld in the context of this study.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Study design: Omid Khosravizadeh; Research: Omid Khosravizadeh and Fariba Naseri; Data analysis: Yousof Akbari Shahrestanaki; Writing and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors expresses their gratitude to all the individuals who willingly dedicated their time to partake in the interviews for this study, openly discussing their experiences and viewpoints with the investigator.
References
In response to the rising prevalence of illnesses, trauma, and cardiovascular conditions and the universal entitlement to healthcare, encompassing pre-hospital emergency medical services (EMS), the World Health Organization (WHO) advocates for the incorporation of EMS as an indispensable and vital constituent within the healthcare framework [1]. EMS goes beyond traditional, disease-focused areas to address a wide range of sudden illnesses and injuries that have a significant impact on mortality and disability, especially in economies with limited to moderate financial resources. Accordingly, providing prompt medical attention is an effective strategy for reducing the global burden of disease [2]. Baron Jean Laurie pioneered the arrangement and delivery of emergency services during the German-Austrian conflict with France. Similarly, in Iran, the inception of these services occurred after the tragic incident of the Mehrabad Airport roof collapse in 1978, resulting in multiple casualties [3]. In all nations, EMS is regarded as the primary component for delivering health and treatment services, and their definition is as follows: EMS constitutes an all-encompassing system that addresses the medical requirements of individuals who are injured or suffering from acute and emergent illnesses, beyond the confines of healthcare facilities, before and during their transition to a suitable medical facility [4]. The primary objective of the EMS system is to offer services that meet consumers’ expectations, optimize time efficiency, and fulfill the requirements of patients experiencing urgent and critical circumstances within the shortest timeframe possible while upholding safety standards [5]. In numerous global regions, particularly in low and middle-income nations, EMS infrastructure is less advanced, and the effectiveness of the healthcare system falls short of being satisfactory [6]. In Iran, despite notable advancements in this domain, such as the expansion of bases, the augmentation of ambulance fleets, the enhancement of equipment quality, the enlargement of the workforce, and the incorporation of air ambulances (helicopters), motorized ambulances, and ambulance buses, a multitude of issues and inadequacies persist [7]. In Iran, the pre-hospital services association is linked to the medical oversight hubs, the national emergency entity, and the Ministry of Health and Medical Education. By dialing 115, individuals can access these services. Currently, the national emergency agency holds the responsibility for devising comprehensive strategies, directives, and regulations about pre-hospital EMS [8]. The management centers for accidents and medical emergencies at the provincial level in Iran are overseen and supported by the respective provincial medical sciences universities. Nearly 80% to 85% of EMS in the country involves the transportation of individuals with acute medical conditions to healthcare facilities [9]. Pre-hospital emergency services serve as the first point of contact in the healthcare system for individuals experiencing acute and emergency conditions. They have a crucial frontline role in managing and responding to emergencies within the healthcare system [4, 9]. The primary responsibility of EMS is to oversee and regulate the care of patients facing acute and urgent circumstances. The efficient and timely management of emergency cases by EMS plays a vital role in reducing morbidity and mortality rates [10].Consequently, during instances of accidents and internal emergencies, these attentions commence at the patient’s side, offering suitable medical treatment at the correct location and moment, utilizing the accessible resources, and ultimately guiding the patient to the hospital’s emergency department [8]. Estimates from 40 countries indicate that emergency medical care can prevent 54% to 90% of fatalities and reduce the burden of disease by 900 million to 2.5 billion disability-adjusted life years in low- and middle-income countries [11]. The efficient functioning of medical emergency centers in terms of time is crucial for the management and control of emergency patients and medical emergencies. This reduces mortality and morbidity but also facilitates the burden on hospitals during times of crisis, emphasizing the significance of pre-hospital care. To enhance their capabilities and effectively respond to urgent situations, emergency medical centers must be cognizant of their performance during critical scenarios. They must gather this valuable information and use it as a foundation for improvement and preparedness in handling acute situations. This study is conducted considering the research conducted in this area and recognizing the significance of time factors within the pre-hospital emergency system. Nevertheless, despite the criticality of the matter, no prior investigations had been carried out in Qazvin Province, Iran. Therefore, employing a qualitative approach, we identified the influential factors that enhance the performance of pre-hospital emergency time indicators and proposed solutions to ameliorate the situation.
Materials and Methods
The objective of the current research is to identify and extract the key elements that contribute to enhancing the performance of six time-based metrics endorsed within pre-hospital emergency services. These metrics include seconds delay time, response time, scene time, total run time, transport time, and round trip time (the detailed explanations of the indicators are in Table 1).
Given that selecting a qualitative methodology for research is suitable when the intention is to explore a novel area using an exploratory technique or to approach it from an innovative angle, this study utilizes a qualitative approach alongside an analytical methodology to attain the objective of this study. The content that has been recommended is also integrated into the approach.
Study population
The key informants and experts in the field of pre-hospital emergency, including the officials of the emergency organization, academic staff members, technicians, and specialist doctors residing in the emergency departments of educational and treatment centers formed the research community. Furthermore, a purposive sampling technique was employed. Additionally, considering that qualitative studies do not adhere to a precise sample size criterion, the sampling process in the current study persisted until data saturation was achieved. The prerequisites for study participation included having substantial expertise and experience in pre-hospital emergency services, relevant work history, as well as a notable interest and motivation to partake in the research.
Data collection method
The instrument used for data collection was a semi-structured interview guide. To craft this guide, insights from educators and advisors, in addition to a review of pertinent literature, were harnessed. This guide encompassed broad inquiries to elicit open-ended responses (Figure 1).
Data management and analysis process
To dissect the qualitative data procured from the interviews, the content analysis technique was employed. This approach was executed through a sequence of three phases, involving data condensation, data augmentation, and categorization, along with subsequent analysis. During this phase, the initial step involved transcribing all the interviews following attentive listening and thorough examination. Subsequently, the researcher proceeded with coding the statements and categorizing them. Ultimately, upon concluding this process, the outcome of this research stage materialized as the identification of dimensions and elements that impact the enhancement of pre-hospital emergency time metrics. These aspects were distilled into distinct themes through the analysis of the interview responses.
Results
In pursuit of the research objective, 10 principal sources of information were engaged in the interview process. Out of the interviewees, 9 individuals (90%) were male and the remaining 1 individual (10%) was female. All participants held at least a bachelor’s degree in terms of educational attainment. A majority of the interviewees occupied the role of foundational staff within the educational and medical establishments in Qazvin City, Iran (Table 2).
Initially, a comprehensive transcription of the interviews with prominent specialists was conducted, following attentive listening and thorough assessment. Subsequently, the qualitative findings of the study are written. The statements were elucidated and assigned codes, with the outcomes being presented as 14 dimensions and 41 influential constituents contributing to the enhancement of pre-hospital emergency time benchmarks (Table 3).
In the subsequent sections, discussions revolve around the themes and sub-themes derived from the interviews. A concise portrayal of their structure is provided, along with references to significant phrases associated with each aspect of the interviewees’ contributions.
Staff readiness
Every person interviewed shared the belief that the preparedness of the personnel is among the key elements contributing significantly to the enhancement of time measures in pre-hospital emergencies. In other words, the level of readiness exhibited by the on-duty personnel for prompt responsiveness. The staff’s preparedness to execute tasks entails various instances, such as when a mission is communicated to the base, but a technician is engaged in personal tasks, resulting in a delay for the ambulance to depart from the base. Consequently, employees must be prepared and abstain from personal tasks when they receive a mission. In this regard, experts pointed to components such as Physical fitness of staff Mental preparation of employees, and employees’ readiness to work.
Regarding this case, the interviewee P-9 maintained the following opinion
“Compiling health records can be beneficial. For example, a triage nurse in good physical and mental condition can manage the mission effectively, obtaining accurate addresses, ensuring smooth mission transfers, and facilitating clear communication between the technician and the patient. A technician experiencing issues, such as back pain or knee pain would face challenges in evacuating a patient from higher floors. Similarly, a technician with psychological distress is at a disadvantage in establishing effective communication and comprehending a patient’s pain and distress to provide adequate relief. This underscores the significance of upholding both the physical and mental well-being of the personnel”.
Efficient manpower
Each participant shared the view that effective personnel play a role in influencing time metrics. When discussing the efficacy of the workforce, it implies their capacity to competently manage tasks, possess educational proficiency alongside their skills and capabilities, and exhibit a strong commitment to the organization’s mission. In this dimension, the components, such as staff skills, scientific knowledge and work experience of employees, and work commitment of employees to the organization have been mentioned.
Regarding this dimension, the participant P-3 stated the following opinion
“Enhancing time indicators in medical emergencies relies on the effectiveness and dedication of human resources, as every moment and second holds immense value. The dedication of individuals plays a crucial role in saving patients' lives. Technicians, with their expertise, are the primary resource for assisting during critical moments. The level of dedication within an individual can be decisive in emergencies. Additionally, this commitment is influenced by various factors, such as compensation, salaries, benefits, and overall satisfaction with the organization, which are management-related aspects. It is believed that satisfied individuals are more likely to perform their job proficiently”.
Additionally, in this regard, the participant P-10 maintained the following opinion
“Proficiency in interacting with callers or their companions is a crucial skill in emergencies. In unique scenarios, these individuals may be restless, agitated, and under significant stress, demanding the dispatch of an ambulance without fully understanding the situation. The triage operator attempts to engage them by asking a series of questions; however, sometimes the caller becomes even more agitated and resorts to yelling. If the triage operator lacks skills in stress and anger management, as well as effective communication, the interaction can be disrupted, leading to a prolonged process. This elongation of time can be problematic considering the need for time management. Therefore, it is imperative to possess skills, such as anger management, stress management, effective communication, and academic proficiency in handling such situations”.
Human resources management
The participants reached a consensus on this measure, which essentially stands as one of the most effective approaches to enhance pre-hospital emergency time metrics. This consensus considers the shortage of personnel in connection with the realm of human resources management, emphasizing the necessity for resource provisioning and strategic human resources planning. The interviewees mentioned various components, such as providing the required manpower, human resource performance evaluation, and human resource planning.
In terms of this issue, interviewee P-3 stated the following opinion
“There is a shortage of personnel in various areas, including the triage unit, dispatch, and the count of technicians and physicians. Some individuals are forced to work consecutive shifts at the bases for two or three days, resulting in a decline in overall effectiveness. This decrease in work efficiency raises concerns about human resources. It is crucial to prioritize addressing this issue and finding a viable solution to alleviate the strain and ensure adequate staffing levels for optimal performance”.
Also, in confirmation of this dimension, the participant P-2 stated the following opinion
“We need to ensure that we allocate personnel in a manner that avoids extended shifts while maintaining efficiency as a priority. Our approach should involve offering amenities and support that coincide with minimized workloads for the staff, ultimately enabling us to deliver optimal services and cater to the workforce effectively”.
Infrastructure and organizational facilities
The participants held the viewpoint that infrastructure and organizational amenities constitute crucial elements in enhancing pre-hospital emergency time metrics. This is because even if resources are scarce, such as ambulances or equipment, expecting significant improvements in indicators would be unrealistic. They pointed to components, such as establishment facilities, efficient ambulance fleet, proportion of the number of bases to the population, and creating a suitable and low-stress environment for the communication center, which can be effective in improving these indicators.
In confirmation of this statement, interviewee P-1 mentioned the following opinion
“The classification pertains to the organization, system, and arrangement. For instance, numerous bases lacked a designated parking area for ambulances. Lately, there are reports of new parking facilities being constructed; however, the functionality of these parking entrances becomes a concern, whether it is manual operation or electronic mechanisms”.
Regarding the given aspect, the participant P-4 stated the following opinion
“Enhancing indicator performance involves a crucial facet– the expansion of facilities. On the provincial level, there is a distinct lack of bases, and numerous factors are contingent upon this shortfall, stemming from a deficit in the base development strategy. For instance, Qazvin City (Iran) currently falls short of the latest population standard, which dictates the need for one base per 20 000 residents. Abiding by this guideline, Qazvin City faces a substantial shortage of around 10 to 12 bases, significantly influencing the situation”.
Communication and information technology management
The specialists thought that the configuration of the emergency communication center holds substantial potential for enhancing indicators, particularly the index related to time delays. This setup should encompass several tiers that can uphold ongoing connections in the event of a failure in one layer. They pointed to components, such as the first line of emergency response, radio communication system, telephone communication system, and the Internet communication system which can be effective in improving the indicators.
In this case, the interviewee P-4 stated the following opinion
“The integration of 115 response operators has contributed to the enhancement of pre-hospital emergency service efficiency. In the past, response times were more extended, compounded by the absence of skilled personnel at the bases. Only individuals with diplomas were available to assist, and this was especially problematic as female staff could not be employed at road bases. Moreover, centralization has also played a role in ameliorating time indicators”.
Also, regarding this dimension, the interviewee P-8 stated the following opinion
“The presence of multiple communication tiers is crucial in both pre-hospital and hospital operations. This includes landline, mobile phone, and internet communication. Enhancing wireless communication strengthens various systems, such as phone networks, the Asayar system, internet connectivity, and intranet capabilities. The current use of communication layers in the pre-hospital domain, including Asayar, internet, wireless, and telephone, is deemed insufficient. Transitioning from the internet platform to the intranet platform is the next step to enhance security. Expanding communication layers is essential to connect dispatch centers, bases, hospitals, and centers, ensuring effective communication among these entities”.
Smart automation
Specialists held the view that technology can play a significant role in enhancing indicators, as time is critical in emergencies, and the application of technology accelerates processes, thereby effectively contributing to the improvement of time metrics. They pointed to components, such as routing technologies and specialized application software.
Regarding this dimension, the interviewee P-3 stated the following opinion
“At present, there exists a set of software that can transmit the mission address location to ambulance smartphones; however, our progress in this aspect is still lacking. Current internet maps need to be advanced to display the precise real-time position of the ambulance while it is in transit. This involves software solutions and GPS technology, which need to be operational in ambulances”.
Additionally, in this case, the participant P-5 stated the following opinion
“Telemedicine was initially introduced into the emergency system for online electrocardiography recording and its primary function remains the same. Depending on the capabilities of the monitoring device, telemedicine enables remote monitoring of acute and critical patients during transit, including subjects with blood pressure concerns. These devices are equipped with digital features, such as pulse oximeters. While telemedicine is incorporated into ambulance protocols, the current capacity in Qazvin City does not allow for directly obtaining online electrocardiography readings”. “Initially introduced into the emergency system solely for online electrocardiography recording, telemedicine’s primary function remains consistent. Depending on the capabilities of the monitoring device, it can facilitate the remote monitoring of acute and critical patients during transit, encompassing individuals with blood pressure concerns. These devices are equipped with digital features including pulse oximeters. While telemedicine is incorporated into ambulance protocols, our current capacity in Qazvin City does not extend to directly obtaining online electrocardiography readings”.
Influential environmental factors
Specialists held the belief that external environmental factors beyond the organization play a crucial and impactful role in time indicators. The participants pointed to components, such as weather conditions, traffic situation, and distance and state of transportation routes.
The participant P-10 stated the following opinion
“One of the major challenges in Qazvin City is the traffic behavior on the roads, especially during specific periods, such as school closures and afternoon shopping. This constant issue makes navigating certain streets difficult, especially for ambulances trying to reach a location. Traffic patterns and people’s driving etiquette have a significant impact on response time. Moreover, the quality of the road surface in certain areas is crucial. Sometimes, the bases are located at a distance from the road, requiring the ambulance to find a parking spot before joining the main road. Unpaved roads, dirt tracks, and obstacles like elevated structures also contribute to longer travel distances. These factors collectively affect emergency response time indicators”.
Patient-related factors
Nearly all the specialists concurred that a range of factors associated with the patient and their condition exert an influence on time indicators. According to the interviewees, this aspect holds notable sway over the time index about arriving at the scene, as well as the time index related to any delays in providing information to the operator for collaboration. However, it bears the most substantial impact on the index concerning the attendance stage. They pointed to components, such as patient cooperation and clinical status.
Regarding this case, the interviewee P-1 mentioned the following opinion
“Consider this scenario, I am a technician, I have arrived at the scene, managed the situation, evaluated the patient’s condition, and completed all necessary tasks swiftly. I am ready to move the patient since, as a human technician, I can initiate patient transfer with appropriate authorization. Nevertheless, this is where the human element comes into play. Both the patient and individuals around them can influence this step. Sometimes, even the patients might resist or withhold permission for the transfer. Cultural nuances might also come into play, leading to debates. For instance, a patient might decline to transfer to the hospital, stating that their spouse needs to be informed first”.
Also, participant P-6 emphasized this dimension in the following opinion
“The timeframe differs based on the patient’s clinical state. For instance, in a critical situation, such as cardiac arrest, we might need to administer cardiopulmonary resuscitation for as long as 45 min. Conversely, a patient might have an issue necessitating treatment, such as administering serum therapy to elevate blood pressure, which could take around 20 min to observe improvement and subsequently facilitate transfer. Alternatively, if the patient has suffered trauma, a sequence of interventions might be necessary. In certain instances, immediate transfer might be imperative”.
Influential factors of stage management
According to specialists, the efficient handling of stages by technicians plays a pivotal role in enhancing time indicators. Every accident scene presents unique circumstances that need to be carefully considered, guiding decisions and actions accordingly. They mentioned components, such as security of the accident scene, safety of the accident scene, and unsettled atmosphere at the scene of the incident.
Regarding this case, the participant P-6 stated the following opinion
“During altercations, especially incidents involving gunfire, it is crucial to secure the scene before a technician can safely approach the patient. However, there is often a delay of approximately 30 min before the police arrive at the location to provide additional security. This delay extends the overall process, taking around 30 to 40 min before the scene is fully secured and the technician can attend to the patient”.
In confirmation of this issue, the participant P-9 stated the following opinion
“Our colleagues often face challenges when responding to accidents due to the excessive influx of people at the scene. This large gathering of individuals can hinder proper scene management and the technician’s ability to carry out effective triage. Triage involves quickly assessing patients to determine their need for immediate attention or lower priority. The noisy and agitated behavior of patients with lower priority (green category) can draw more attention, diverting resources from those in critical condition. Additionally, the emotional impact of a deceased patient tends to attract the crowd’s attention, even though they may not have the necessary medical knowledge to accurately assess the severity of patients’ conditions”.
Adherence to national guidelines
Every participant shared the perspective that national guidelines play a crucial role in enhancing pre-hospital emergency time indicators. These directives function as a navigational guide, offering recommended steps to follow in diverse scenarios. They mentioned various components, such as care protocols and star protocols.
In this regard, the participant P-2 stated the following opinion
“Protocols are in place for both on-scene conditions and telephone triage colleagues, and they diligently follow these protocols. The instructions guide the appropriate actions to take based on specific indicators. Similarly, technician colleagues also follow a set of offline and online protocols that dictate their actions upon arriving at the scene. These protocols ensure a systematic approach and consistent care throughout the process”.
Contextual factors
According to the experts in this study, delivering EMS services is influenced by societal dynamics, cultural norms, and related matters. These aspects, known as contextual factors, play a pivotal role. This is because people’s conduct is shaped within the framework of society and culture. They mentioned components, such as cultural context, social context, and knowledge and awareness context.
In this regard, the interviewee P-10 stated the following opinion
“The presence of a crowd at the accident site leads to disorderliness, often instigated by companions or bystanders. The technician’s efforts to carry out on-site assessments can be hampered due to threats and coercion, exerted through pressure tactics that compel rapid patient retrieval and departure. Individuals who lack medical knowledge tend to intervene, and their interference can disrupt the technician’s tasks”.
In this case, the participant P-8 stated the following opinion:
“An individual providing information as a patient offers basic details, and public awareness significantly aids the triage process by helping the triage assess whether the case is an emergency warranting an ambulance dispatch. If the informant possesses a range of general information, they can provide more accurate guidance. It could be beneficial for the emergency department to create educational pamphlets, organize informative radio programs, and other resources for the general public”.
Inter-organizational coordination and cooperation
The majority of experts shared the viewpoint that the effective enhancement of time indicators is influenced by the coordination and collaboration among emergency-related organizations. They mentioned various components, such as the presence of supporting organizations and the presence of partner organizations.
The participant P-5 stated the following opinion in this regard:
“When discussing collaboration with the Ministry of Roads and Urban Development, the focus shifts to roads and highways. For instance, on highways, a technician in an ambulance might find themselves in a traffic jam for two kilometers due to an accident ahead. Then, the question arises of how the ambulance can navigate this situation effectively. Here, the involvement of the Ministry of Roads and Urban Development becomes crucial. If designated lanes exclusive to emergency vehicles are established, where no other vehicles are allowed to pass, and stringent penalties are imposed for violations, the ambulance can utilize these lanes to bypass traffic congestion. This way, the ambulance can navigate through traffic effectively, benefiting from the special lane privileges”.
Regarding this dimension, the interviewee P-7 stated the following opinion:
“Concerning the interactions between the emergency organization and relevant entities, over the past three years, we have engaged in multiple discussions with the Red Crescent and the 123 hotline. In the realm of social emergency-related organizations, there should ideally be a comprehensive engagement, involving numerous entities. In some instances, the situation might not qualify as a critical emergency but requires assistance from social emergency services. Here, coordination is essential. In terms of collaboration with the Red Crescent, fortunately, there have been no issues, and our efforts have aligned seamlessly”.
Effective features of the destination treatment center
The specialists held the view that the attributes of the destination treatment facility, including proximity to the accident site, alignment with the patient’s clinical state, and the ability to accommodate the patient, contribute significantly to the enhancement of time indicators. They mentioned various components, such as the nearest treatment center, crowding, and overcrowding of the treatment center, and the most suitable treatment center.
Also, in this case, the participant P-1 stated the following opinion:
“The technician assesses the patient’s condition to determine the appropriate medical facility for comprehensive treatment. While initial care and treatment are provided at the scene, it is crucial to transport the patient to a specialized medical center for definitive treatment. For example, a cardiac patient would be transferred to a heart center, while a trauma case requires a trauma center. In cases where the patient has a combination of injuries, such as burns and trauma, the technician must identify the appropriate treatment center. The technician’s diagnosis is significant, as well as considering the distance between the accident site and the designated treatment center”.
Feasibility of response to vulnerable population
Certain specialists thought that implementing initiatives aimed at aiding the vulnerable population could prove efficacious in enhancing time indicators and elevating the pre-hospital emergency services’ efficacy. They mentioned components, such as physically and mentally disabled and temporarily vulnerable populations with chronic diseases.
About this subject, the interviewee P-10 maintained the following opinion:
“As someone actively involved in this field, I observe that we often overlook the marginalized segments of our society. It is important to clarify that when I mention minorities, I am not referring to religious minorities. Rather, I am addressing various marginalized groups within society, including individuals with distinct disabilities, like cognitive challenges or physical impairments. The pressing question is how we can facilitate their access to the emergency medical system and how we can ensure that they can effectively engage with and benefit from emergency services tailored to their specific needs”.
Discussion
In discussing the dimension of staff readiness, ensuring the physical, mental, and psychological preparedness of staff members is an essential and requisite characteristic of this profession. Creating health records can serve as a beneficial approach in this context. The physical and mental well-being of employees significantly impacts the performance of emergency services, spanning from the initiation of a mission to its completion. Additionally, the notion of employees’ preparedness for swift responses pertains to their availability at their designated workstations and their readiness to accept and execute missions promptly. Supporting this dimension, the work of Moradian et al. [12], and Bayrami et al. [13] substantiates these ideas, aligning with the current research. Regarding the efficient manpower dimension, it signifies that employees are proficient in managing their assigned responsibilities, and this proficiency, coupled with their skills, knowledge, quick decision-making, diligence, and sense of accountability, enhances the effectiveness and output of pre-hospital emergency operations. Within EMS, the competence of the workforce plays a crucial role in enhancing time-related performance metrics. These metrics are associated with individual capabilities, and the organization can enhance these capacities through the implementation of training sessions and hands-on exercises, such as simulations. This concept is supported by the research conducted by Seyyednozadi et al. [14], Khanke et al. [15], and Dadashzadeh et al. [16] as referenced. Regarding the conceptual dimension of human resources management, within the pre-hospital emergency system, it is crucial to recruit and employ personnel with both robust physical strength and mental well-being. Subsequently, after recruitment, consistent assessment of personnel performance by human resources management becomes imperative. Additionally, given the demanding nature of emergency work, adherence to proper work and rest standards is essential, and to counteract the attrition associated with emergency roles, a rotation system, such as the 115 job rotation should be implemented. This approach enhances the efficacy of staff engagement, thereby contributing to the improvement of time-related performance metrics in pre-hospital emergency services. This perspective is reinforced by Khanke et al.’s research [15], Yadollahi et al.’s study [17], and Azami-Aghdash et al.’s investigation [7], which all align with the concepts highlighted in the present study. In elucidating the dimension related to infrastructure and organizational facilities, the emergency organization holds the responsibility of furnishing the necessary infrastructure and amenities to enhance the efficiency of emergency services. This enhancement is a pivotal factor in reducing the duration of critical indicators. In this context, the availability of essential elements, such as 115 ambulance stations with dedicated parking spaces and emergency vehicles holds paramount importance. These vehicles play a critical role in swiftly transporting emergency responders to accident scenes and facilitating patient transfer to medical facilities. Ensuring the technical soundness of these vehicles is imperative. Furthermore, the physical workspace for employees should also be appropriately designed. Support for this perspective can be drawn from Moradian et al.’s study [12] and Sabouri et al.’s research [18], both of which align with the concepts presented in this study. Regarding communication and information technology management, emergency 115 operates with diverse communication tiers, facilitating information exchange through these levels. Employing contemporary and diverse communication technologies consistently can safeguard the organization’s information. In situations where one communication layer experiences disruption, the subsequent layer steps in seamlessly to ensure uninterrupted communication. Consequently, the proficient management of communication and information technology significantly contributes to the enhancement of time-related performance indicators. This view is corroborated by Ahmadi Dashtiyan et al.’s research [5] and is also echoed in Olave-Rojas et al.’s study [19] both aligning with the concepts highlighted in the present study. Concerning the make smart dimension, technology accelerates tasks and the proliferation of intelligent devices holds the potential to expedite operations. In the context of pre-hospital emergency services, leveraging specialized software, such as the Asayar system in place of traditional paper-based systems, utilizing GPS for optimized routing, and incorporating smart tools, including telemedicine can all contribute to enhancing time-related performance metrics. This viewpoint is reinforced by the research conducted by Gaeeni et al. [20], which aligns with Azami-Aghdash et al.’s study and Hajinabi et al.’s investigation, both of which resonate with the themes explored in the present study [7, 21]. In considering the interpretation of the influential environmental factors dimension, external environmental elements encompass influences on organizational performance that lie beyond the organization’s jurisdiction. Consequently, devising strategies and preparing to counteract these influences, while simultaneously aligning the organization to them, can assist in effectively addressing these external factors. Such preparedness contributes to the efficacy of enhancing pre-hospital emergency indicators. This perspective is supported by the research conducted by Ahmadi Dashtiyan et al. [5], and Seyyednozadi et al. [14], both of which substantiate the ideas explored in this study. Regarding the patient-related dimension, this factor exerts a more substantial influence on the on-scene presence indicator. The conduct of the patient’s companions and the demeanor of the patient upon initial interaction with the emergency staff can markedly affect the team’s morale and efficacy. Supporting this viewpoint, Alrazeeni, et al. [22], and Cui et al. [23] have addressed this facet, aligning with the current research. Continuing to discuss the influential factors of scene management, when dealing with an accident scene, an immediate and preliminary evaluation of various aspects is vital. This includes categorizing the nature of the incident, assessing its scale, estimating the extent of damage, and gauging the number of casualties. The insights gathered during this initial phase contribute to gauging the urgency of the situation, thereby impacting the time-related indicator for on-scene presence. Each accident scene presents its unique circumstances, necessitating thorough consideration and subsequent decision-making based on these specific conditions. Regarding the facet of Adherence to national guidelines, there exist prescribed protocols within pre-hospital emergency services. These protocols function as navigational tools in diverse scenarios, offering recommended actions to be undertaken. Consequently, abiding by these guidelines and implementing them can be impactful in enhancing time-related performance indicators. This perspective is corroborated by Alrazeeni et al.’s research, which aligns with the themes of the present study [22]. When discussing contextual factors, societal norms, cultural considerations, and matters linked to people’s awareness of EMS play a significant role. Various factors, such as the capacity to provide medical history and the propensity for cooperation with EMS are instrumental in augmenting the effectiveness of pre-hospital emergency services and related time-based benchmarks. Khanke et al.’s study [15] and Seyyednozadi et al.’s research [14] lend support to these aspects and align with the present study. The inter-organizational coordination and collaboration aspect pertains to the interaction between various entities concerning EMS. These entities can be categorized into two types as follows: Those directly aligned with emergency response and those providing auxiliary support to emergencies. When effective coordination and cooperation are established between emergency services and these organizations, it can positively impact the enhancement of time-related performance measures. Azami-Aghdash et al.’s study [7] and Khanke et al.’s research underscore this dimension, aligning with the themes addressed in the present study. In the subsequent exploration of effective features of the destination treatment center, when a patient is transferred to a treatment center, there is often limited information available about the conditions of that specific hospital. Therefore, the selection of the appropriate hospital based on the patient’s clinical condition and the hospital’s capacity becomes crucial for the patient’s acceptance and effective care. The promptness of patient admission to the treatment center is a significant factor, directly impacting the reduction of time-related indicators. This dimension was also highlighted by Seyyednozadi et al. [14] in their study, aligning with the themes addressed in the present research. Regarding the practicality of Feasibility of response to vulnerable populations, implementing a dedicated program targeted at these groups can significantly enhance both time-related indicators and the overall efficacy of pre-hospital emergency services.
Conclusion
In this qualitative study, different dimensions, including personnel readiness, organizational infrastructure, patient-related factors, inter-organizational coordination, receiving treatment facility attributes, and responsiveness to vulnerable populations have been examined and analyzed. The findings indicate that diverse dimensions, such as staff preparedness, communication technologies, facilities, cultural and social variations, inter-organizational collaboration, attributes of the receiving treatment center, and specialized programs for vulnerable communities play significant roles in improving pre-hospital emergency time indicators. Overall, the article underscores the importance of effective planning and management across these diverse dimensions, which can lead to notable enhancements in the performance and time indicators of pre-hospital emergency services. It is important to recognize that vulnerable populations vary across different contexts and domains. Consequently, it becomes essential to identify diverse vulnerable groups and assess their specific requirements for emergency services. This information serves as a basis for devising tailored strategies that cater to the distinct needs of these groups, ultimately ensuring their benefit from the provided services.
Future study suggestions
Given the significant impact of collaborative and supportive organizations in joint initiatives, it is advisable to organize joint programs, facilitate information exchange meetings, and establish communication pathways to enhance coordination with these entities.
Enhancing the provision of education and training courses for emergency personnel can lead to the augmentation of their capabilities and skills, thereby contributing to the enhancement of the emergency unit’s performance.
Allocating resources to sophisticated communication technologies like software solutions, visual communication systems, and GPS mapping has the potential to enhance real-time communication and boost operational efficiency.
Conducting further research and studies in critical domains concerning performance and time aspects can lead to sustained enhancements in the effectiveness of pre-hospital emergency services.
Implementing targeted initiatives and efficient strategies to address the requirements of susceptible communities can contribute to the enhancement of time and efficacy indicators in delivering emergency services.
Ethical Considerations
Compliance with ethical guidelines
The present study has been registered in the Ethics Committee of Qazvin University of Medical Sciences with the (Code: IR.QUMS.REC.1400.472). Before commencing each interview, implicit approval was acquired from the participants for the audio recording of their dialogue. Moreover, they were apprised that they retained the prerogative to abstain from cooperating or sharing their experiences at any point in the research process. Given that the confidentiality of data is mandatory in all research endeavors, this aspect was also meticulously upheld in the context of this study.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Study design: Omid Khosravizadeh; Research: Omid Khosravizadeh and Fariba Naseri; Data analysis: Yousof Akbari Shahrestanaki; Writing and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors expresses their gratitude to all the individuals who willingly dedicated their time to partake in the interviews for this study, openly discussing their experiences and viewpoints with the investigator.
References
- Abuzeyad FH, Al Qasim G, Alqasem L, Al Farras MI. Evolution of emergency medical services in the Kingdom of Bahrain. International Journal of Emergency Medicine. 2020; 13(1):55. [DOI:10.1186/s12245-020-00315-8] [PMID]
- Burkholder TW, Hill K, Calvello Hynes EJ. Developing emergency care systems: A human rights-based approach. Bulletin of the World Health Organization. 2019; 97(9):612-19. [DOI:10.2471/BLT.18.226605] [PMID]
- Vafaeinasab M, Fatehpanah A, Jahangiri K, Namdari M. [An evaluating on performance of pre-hospital emergency stations in Yazd, based on essential time for attending at patient’s bedside (Year-2013) (Persian)]. Tolooebehdasht. 2017;15(5):122-31. [Link]
- Namdar P, Kazemifar AM, Mohammadi M. The accuracy of diagnosis and treatment made by pre-hospital emergency medical technicians in patients admitted to hospitals in Qazvin, Iran. The Journal of Qazvin University of Medical Sciences. 2021; 24(6):510-9. [DOI:10.32598/JQUMS.24.6.3]
- Ahmadi Dashtiyan A, Masoudi Asl I, Riahi L, Mahmoodi M. [Prioritizing effective factors in the implementation of pre-Hospital Emergency Center using Analytical Network Process (ANP) method (Persian)]. Journal of Health Promotion Management. 2019; 8(3):1-9. [Link]
- Kotwal RS, Howard JT, Orman JA, Tarpey BW, Bailey JA, Champion HR, et al. The effect of a golden hour policy on the morbidity and mortality of combat casualties. JAMA Surgery. 2016; 151(1):15-24. [DOI:10.1001/jamasurg.2015.3104] [PMID]
- Azami-Aghdash S, Moosavi A, Gharaee H, Sadeghi G, Mousavi Isfahani H, Ghasemi Dastgerdi A, et al. Development of quality indicators to measure pre-hospital emergency medical services for road traffic injury. BMC Health Services Research. 2021; 21(1):235. [DOI:10.1186/s12913-021-06238-1] [PMID]
- Zeraatchi A, Rostami B, Rostami A. [Time indices of emergency medical services; a cross-sectional study (Persian)]. Iranian Journal of Emergency Medicine. 2018; 5(1):e8. [Link]
- Heydari H, Kamran A, Zali ME, Novinmehr N, Safari M. Customers' satisfaction about prehospital emergency medical services in Lorestan, Iran. Electronic Physician. 2017; 9(3):3974. [DOI:10.19082/3974] [PMID]
- Rungratmaneemas C, Lorsuwannarat T. Effectiveness of emergency medical services networks. Annals of the Romanian Society for Cell Biology. 2021; 5579-95. [Link]
- Chang CY, Abujaber S, Reynolds TA, Camargo CA Jr, Obermeyer Z. Burden of emergency conditions and emergency care usage: New estimates from 40 countries. Emergency Medicine Journal. 2016; 33(11):794-800. [DOI:10.1136/emermed-2016-205709] [PMID]
- Moradian M J, Rastegarfar B, Fooladband F. [Time indicators of pre-hospital emergency services in stroke patients of Fars/ Iran (Persian)]. Health_Based Research. 2019; 5(2):165-74. [Link]
- Bayrami R, Ebrahimipour H, Rezazadeh A. [Challenges in Pre hospital emergency medical service in Mashhad: A qualitative study (Persian)]. Journal of Hospital. 2017; 16(2):82-90. [Link]
- Seyyednozadi M, Jarahi L, Erfanian MR, Shakeri MT. Pre-hospital emergency medical services: An epidemiological survey in Mashhad, Iran. Journal of Patient Safety & Quality Improvement. 2017; 5(3):572-6. [DOI:10.22038/psj.2017.9040]
- Khankeh H, Alinia S, Masoumi G, Khorasani zavareh D, Ranjbar M, Daddoost L, et al. [Prehospital services by focus on road traffic accidents: Assessment developed and developing countries (Persian)]. Journal of Health Promotion Management. 2013; 2(2):71-9. [Link]
- Dadashzadeh A, Dehghannejhad J, Shams S, Sadegi H, Hassanzadeh F, Soheili A, et al. Situation of response and transport time in pre-hospital traumatic patients from scene to hospital in Tabriz – Iran. Nursing and Midwifery Journal. 2016; 14(8):728-37. [Link]
- Yadollahi S. [Evaluation of prehospital emergency performance services in Shahrekord city in 2016 (Persian)]. Quarterly Scientific Journal of Rescue and Relief. 2018; 10(4):100-11. [Link]
- Sabouri E, NADERI MM, Saburie O, Mohammadi Y, Tavakkoli F. [The evaluation of prehospital emergency performance indicators in Birjand, 2015 (Persian)]. Iranian Journal of Emergency Care. 2017; 1(1):61-8. [Link]
- Olave-Rojas D, Nickel S. Modeling a pre-hospital emergency medical service using hybrid simulation and a machine learning approach. Simulation Modelling Practice and Theory. 2021; 109:102302. [DOI:10.1016/j.simpat.2021.102302]
- Gaeeni M, Ranjbar Vernosfadarani M, Parvaresh Massoud M, Hemta A. [Comparison of time indicators and outcome of pre-hospital emergency operations in two methods of electronic registration with asayar program and paper registration (Persian)]. Qom University of Medical Sciences Journal. 2021; 14(12):22-31. [DOI:10.52547/qums.14.12.22]
- Hajinabi K, Riahi L, Varki HG. [The relationship between prehospital time indices and on-scene death rate in traffic accidents in the 22 regions of Tehran (Persian)]. Health Information Management. 2014; 11(3):353-61. [Link]
- Alrazeeni DM. Relationship between nonconveyed cases and on-scene time intervals for emergency medical services. Journal of Multidisciplinary Healthcare. 2020; 13:1895-904. [DOI:10.2147/JMDH.S279693] [PMID]
- Cui ER, Fernandez AR, Zegre-Hemsey JK, Grover JM, Honvoh G, Brice JH, et al. Disparities in emergency medical services time intervals for patients with suspected acute coronary syndrome: Findings from the North Carolina Prehospital Medical Information System. Journal of the American Heart Association. 2021; 10(15):e019305. [DOI:10.1161/JAHA.120.019305] [PMID]
Type of Study: Research |
Subject:
Qualitative
Received: 2023/12/12 | Accepted: 2024/02/2 | Published: 2024/04/1
Received: 2023/12/12 | Accepted: 2024/02/2 | Published: 2024/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
