

Volume 10, Issue 2 (Winter 2025)
Health in Emergencies and Disasters Quarterly 2025, 10(2): 85-94 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
khankeh H R, Farrokhi M, Hosseinabadi-farahani M, Saatchi M, Ahmadi S, Roudini J, et al . Challenges of Social Trust in Disaster Management Focusing on COVID-19 in Iran: Recommendations for Gaining it Again. Health in Emergencies and Disasters Quarterly 2025; 10 (2) :85-94
URL: http://hdq.uswr.ac.ir/article-1-588-en.html
URL: http://hdq.uswr.ac.ir/article-1-588-en.html
Hamid Reza Khankeh1 

 , Mehrdad Farrokhi1 , Mohammadjavad Hosseinabadi-farahani2 , Mohammad Saatchi1 , Sina Ahmadi3 , Juliet Roudini4 , Amin Rahmatali Khazaee1 , Mariye Jenabi Ghods2 , Elham Sepahvand5 , Maryam Ranjbar1 , Taleb Badri6 , Mohammad Pourebrahimi *7
, Mehrdad Farrokhi1 , Mohammadjavad Hosseinabadi-farahani2 , Mohammad Saatchi1 , Sina Ahmadi3 , Juliet Roudini4 , Amin Rahmatali Khazaee1 , Mariye Jenabi Ghods2 , Elham Sepahvand5 , Maryam Ranjbar1 , Taleb Badri6 , Mohammad Pourebrahimi *7
, Mehrdad Farrokhi1 , Mohammadjavad Hosseinabadi-farahani2 , Mohammad Saatchi1 , Sina Ahmadi3 , Juliet Roudini4 , Amin Rahmatali Khazaee1 , Mariye Jenabi Ghods2 , Elham Sepahvand5 , Maryam Ranjbar1 , Taleb Badri6 , Mohammad Pourebrahimi *7
1- Health in Emergency and Disaster Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Nursing, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Social Development and Health Promotion Research Center, Health Institute, Kermanshah University of Medical Sciences, Kermanshah, Iran.
4- Research Fellow-patient and Stakeholder Engagement, Berlin Institute of Health, Berlin, Germany.
5- Department of Nursing, School of Nursing and Midwifery, Lorestan University of Medical Sciences, Khoramabad, Iran.
6- Behavioral Sciences Research Center, Life Style Institute, Baqiyatallah University of Medical Sciences, Tehran, Iran.
7- Nursing Care Research Center, School of Nursing, Clinical Science Institute, Baqiyatallah University of Medical Sciences, Tehran, Iran. ,pourebrahimi62@gmail.com
2- Department of Nursing, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Social Development and Health Promotion Research Center, Health Institute, Kermanshah University of Medical Sciences, Kermanshah, Iran.
4- Research Fellow-patient and Stakeholder Engagement, Berlin Institute of Health, Berlin, Germany.
5- Department of Nursing, School of Nursing and Midwifery, Lorestan University of Medical Sciences, Khoramabad, Iran.
6- Behavioral Sciences Research Center, Life Style Institute, Baqiyatallah University of Medical Sciences, Tehran, Iran.
7- Nursing Care Research Center, School of Nursing, Clinical Science Institute, Baqiyatallah University of Medical Sciences, Tehran, Iran. ,
Full-Text [PDF 502 kb]
(788 Downloads)
| Abstract (HTML) (3317 Views)
Full-Text: (726 Views)
Introduction
Natural hazards threaten the lives of many people worldwide every year [1, 2]. Natural disasters accounted for 10,492 deaths, affected 101.8 million people, and caused approximately 252.1 billion US$ of economic losses [3, 4]. Iran, as a lower-middle-income country with a unique geopolitical position, has also been affected by disasters and their damage [5]. The number, variety, and severity of disasters in Iran have been increased in recent years [6, 7]. One of the recent disasters was the outbreak of COVID-19, which caused significant social problems [6, 7]. Iran experienced consecutive waves of COVID-19 [8, 9, 10]. In addition to its effects on the health system, it has many social consequences. The social management of such phenomenon requires the knowledge of its various aspects [11], proper inter-sectoral communication, and identification of factors affecting social trust, social health, and education [12, 13]. Early warning, proper planning, and timely responses can help considerably reduce the damage and adverse effects of unforeseen events like the COVID-19 pandemic [14]. It is necessary to have consensus and preparedness at all individual, social, and organizational levels to reduce the effects and damage caused by disasters [15].
Previous studies indicated that effective social communication is needed to understand the disaster risk [14, 16]. If such interaction can build social trust, it will create social cohesion and stability within a society. Social trust is an important aspect of individual and social relations and a prerequisite for proper social functioning, disaster risk perception, and effective communication for risk management. Social trust, a belief in the competence, honesty, or benevolence of the other party, is an important cause and consequence of functioning institutions [17] and controls human behaviors. Improvement in social trust is related to a proactive response to the crisis [18], and failure to do so can result in its deterioration. Siegrist and Zingg showed that trust in health services provider organizations and their managers positively affected people’s willingness to adopt recommended behavior [19]. Social Trust has a significant role in creating and maintaining order and social solidarity by facilitating social interactions [20-23].
Given that trust between community members and emergency and relief organizations is needed to build preparedness, it has become an important topic in the study of the impact of natural disasters [24]. People often act impulsively during disasters [25]. This makes it more difficult to provide the necessary aid to those in urgent need [26]. One study in Saudi Arabia conducted during the COVID-19 pandemic indicated that high levels of public trust in society are associated with increased success in disease prevention policies. Also, gender, age, marital status, and educational level were key predictors of precautionary practices [17]. The loss of social trust can exacerbate the psychological and social problems seen before the pandemic [17, 18]. Understanding the role of social trust in disasters and the related factors can help with community-based disaster risk management and reduce the burden of problems. Meanwhile, there is a lack of knowledge regarding social components and their role at the time of crisis. The COVID-19 pandemic and its consequences in Iran made it necessary to pay attention to social trust and its improvement in society. It is vital to measure the social trust status and the challenges facing Iranian society following disasters such as the COVID-19 pandemic to reduce vulnerability and improve resilience. Therefore, this study aims to investigate the challenges and provide recommendations for building social trust and preparedness against disasters such as COVID-19 in Iran.
Materials and Methods
Study design and participants
This is a qualitative study using a conventional content analysis method. Participants were lay people living in Tehran, the capital of Iran, who had experienced several disasters (n=20) and managers of emergency and relief organizations (n=7) who were willing to share their experiences (mean age=34.2 years). They were selected by purposive and snowball sampling methods with maximum diversity in terms of age, sex, level of education, and organizational position to explore perceptions and experiences of people from different angles (Table 1).
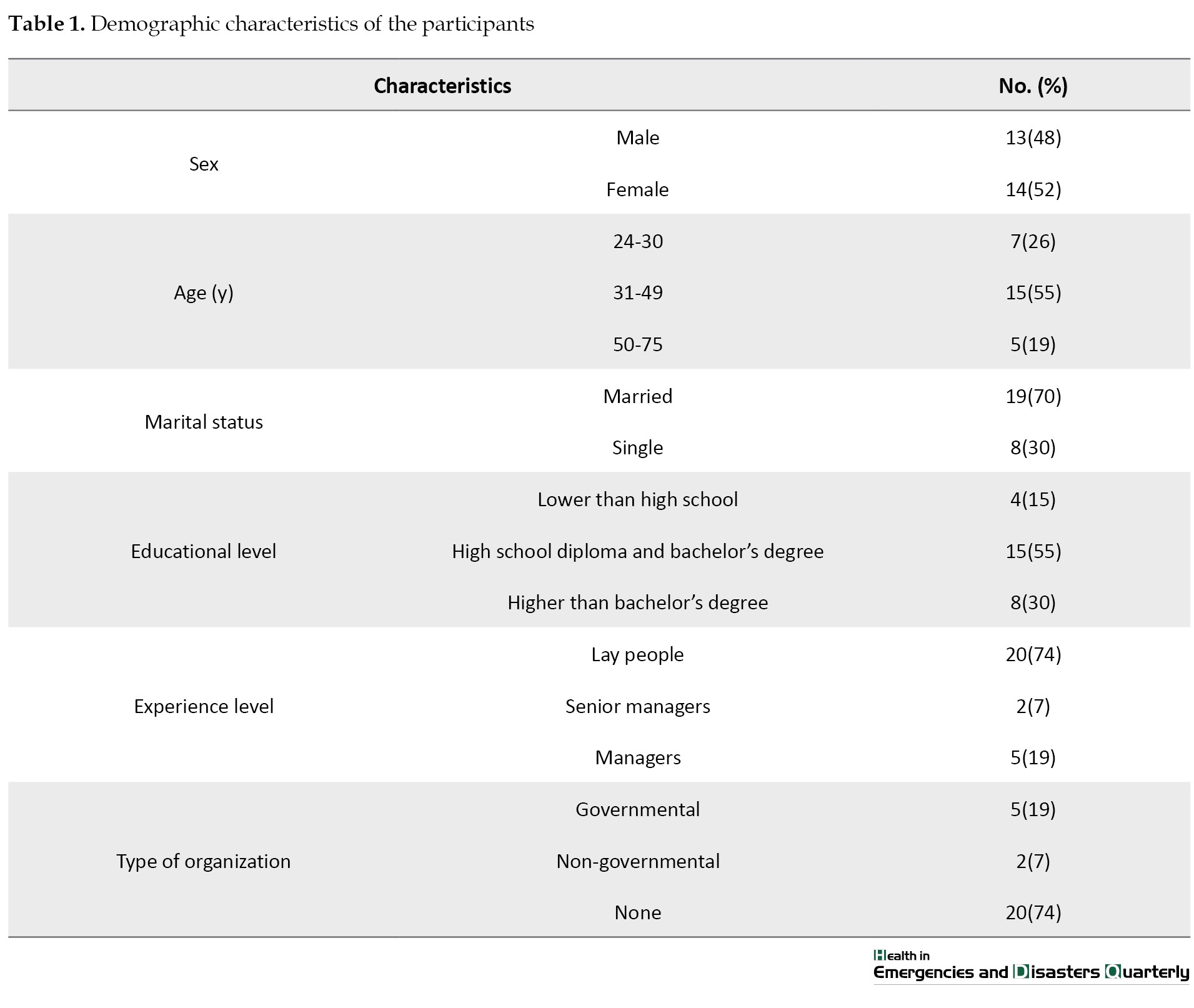
The inclusion criteria were age >24 years, ability to participate in interviews, and living in Tehran.
Data collection
After explaining the study objectives to the participants and obtaining their informed consent, data were collected using in-depth semi-structured interviews with each group until reaching theoretical saturation. Data collection lasted 4 months from June to September of 2020. The interview started with general and open-ended questions, such as “Have you experienced natural disasters in Tehran?”, “What do you think about the performance of emergency and relief organizations in Tehran?”, “How confident are you about the performance of emergency and relief organizations in disaster management?”, “How did you perceive the performance of health organizations during the COVID-19 pandemic?”, “What are the main challenges to managing disasters?” and “What do you recommend to improve the performance of these organizations?” Each interview also included probe and prompt questions, such as “Could you explain more about this?” and “What did you mean by saying this?” The focus of the questions then changed based on the participants’ answers. The participants chose the place and time for the interviews. The interviews were conducted face-to-face (n=16, in the workplace) or over the phone (n=11). In all face-to-face interviews, the researchers wore gloves and masks, and provided these safety items to the participants. The mean interview duration was 49 minutes (ranged 35-76 minutes). All interviews were recorded and transcribed verbatim.
Data analysis
The data were analyzed using the conventional content analysis method proposed by Graneheim and Lundman [27]. The transcriptions were read carefully. The significant semantic units were extracted, summarized, and coded. Multiple reading and note-taking during simultaneous interpretation helped identify the connections between the concepts extracted from the participants’ statements. The codes were classified based on similarities and differences, and the main themes (challenges and recommendations) were identified.
We used the four criteria proposed by Guba to assess the trustworthiness of collected data [28]. We tried to communicate well with the participants and increase the credibility of the data through long-term engagement and complete immersion in the data. In addition, we checked the accuracy in collaboration with participants (member checking). All interviews were recorded and transcribed verbatim to ensure the credibility of the data. To determine the dependability of the data, we recorded and reported all the steps and the made decisions so that others can follow and repeat the process, if necessary. To determine the transferability of the data, we tried to fully describe the research context by accurately describing the participant characteristics, research environment, sampling method, and time and place of interview.
Results
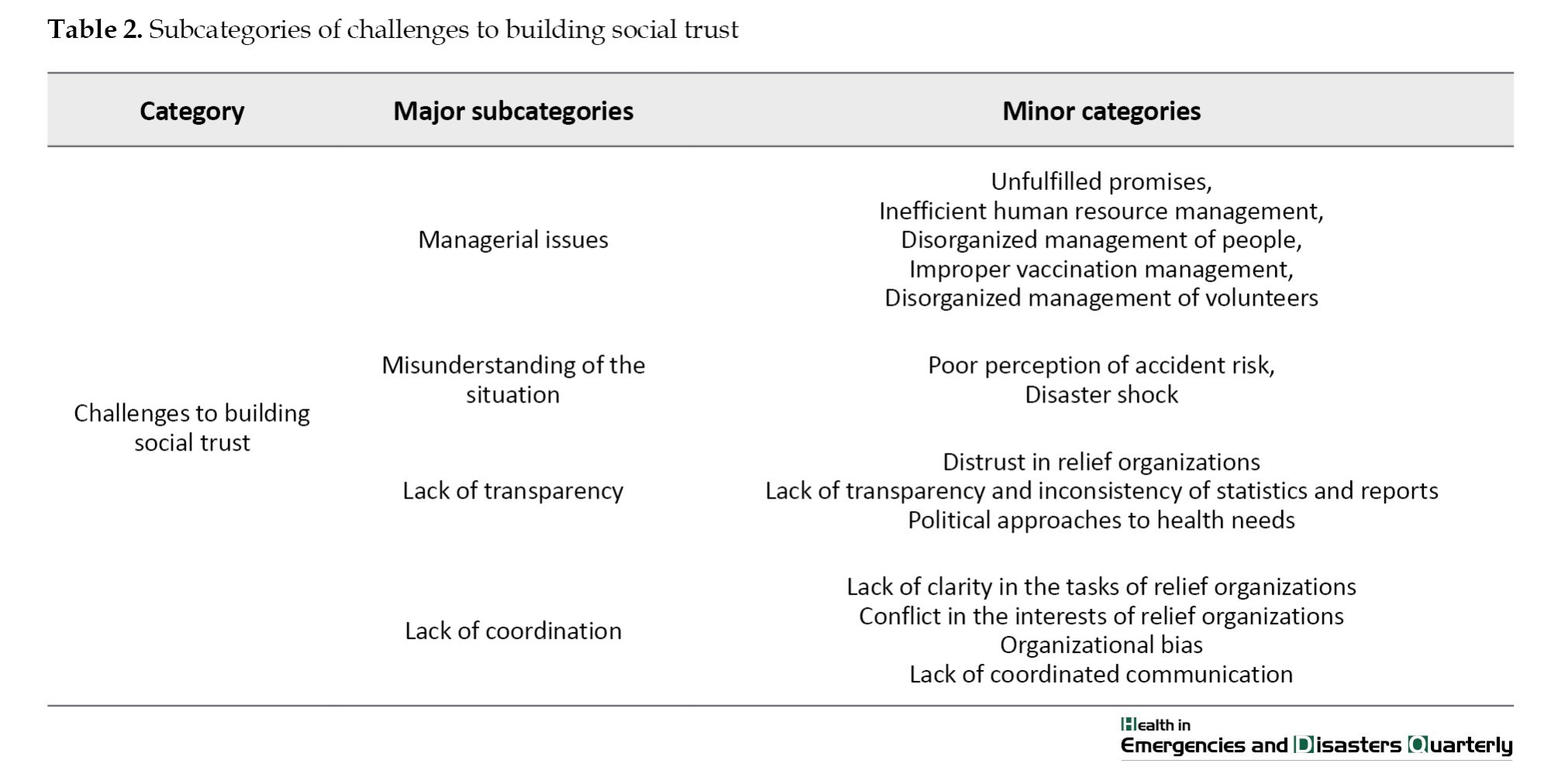
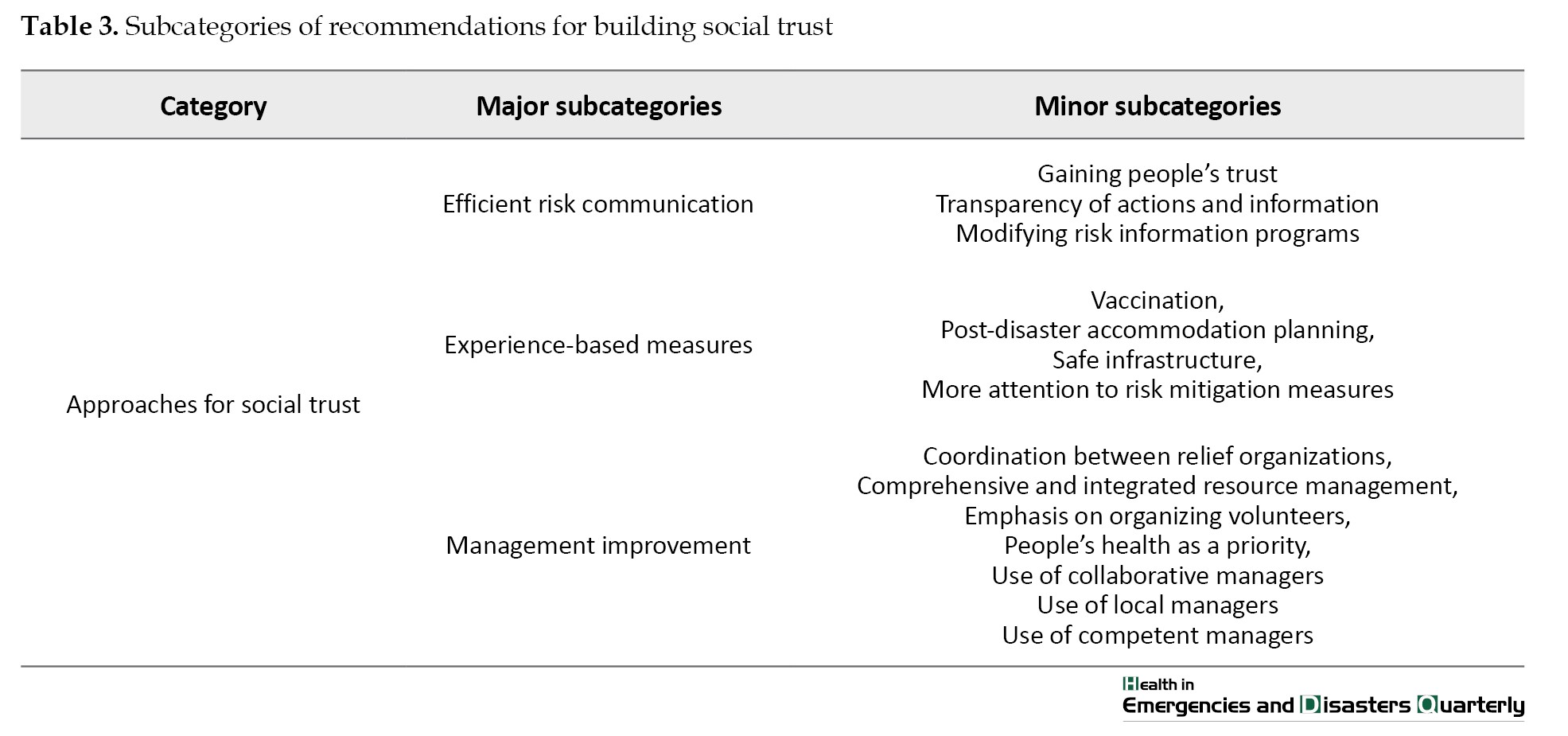
Four categories were found for the theme of “challenges to building social trust” and three categories for the theme of “recommendations for building social trust”, each with subcategories presented in Tables 2 and 3.
Challenges to building social trust
Managerial challenges
According to the participants’ experiences, one of the main challenges to building social trust was managerial issues. Social trust in emergency and relief organizations has been reduced due to unrealized promises, mismanagement of human resources, improper distribution of staff/resources, and lack of attention to and planning for volunteers. The lack of comprehensive risk assessment, which caused a delay in the early stages, and the lack of a response plan for COVID-19 (including a vaccination program) worsened the situation. The reduced trust made people pessimistic about the health and social conditions of the community.
“Unfortunately, the slogan of meritocracy was never realized because of the ridiculous phenomenon of credentialism. The disaster management system was completely passive in managing the pandemic; all these problems happened because of this mismanagement.” (Participant No. 6 (P6), a 38-year-old male). “I do not trust the system and those dealing with the COVID-19 situation! I think these organizations are trying to show everything as being normal because of their failure to manage the disease. I think it is so difficult to eradicate this social distrust; it did not happen overnight! So it cannot be eliminated overnight. Many things were said at the beginning of the pandemic several times, but these were later proven wrong; many promises were made that were not fulfilled after months. All these things caused social distrust. Some officials made a promise that was broken later by other officials!”(P2, a 28-year-old female).
Misunderstanding of the situation
Lack of knowledge and awareness about disaster preparedness and lack of education about measures that should be taken during a disaster caused people to fail to take the proper action, thinking that the only correct action is to leave the affected area. “We did not know much about safety measures! No one really knew! There should be an expert in this field [to teach people]. Based on the previous experience, many people knew that an earthquake might happen since a powerful earthquake happened here several years ago, such that this place was completely destroyed and people came back and built houses on the ruins. What I wanted to say is that we do not have enough information” (P4, a 34-year-old female).
Lack of transparency
Another challenge was the lack of transparency in released reports and information. Contradictory information and statistics on social media caused citizens to consider the information distributed by the emergency and relief organizations unreliable, so they lost trust in them.
“The information they report about the casualties or deaths that may occur is vital. If the information is true, people will trust them more. What people said differed from what was reported. If we pay attention, we can certainly do a lot during these events. Regarding financial aid, officials often say that they paid a lot of money, while people say something else, which makes many people not trust the information and not help government organizations. People prefer to help the victims directly! It is not clear who is right! There is a lot of controversy, which can cause distrust”(P14, a 26-year-old female).
Lack of coordination
In most cases, the leadership and management of the disaster in Iran is the responsibility of the National Emergency Management Organization; the organizations such as the Red Crescent, the army, and law enforcement forces act as supporting agents. However, in many cases, the responsibilities of each organization and institution are not well defined, leading to chaos and waste of time and resources.
A 31-year-old female participant said: “When a disaster happens, the members of the disaster management headquarters hold a meeting. To whom and where they sent all these relief items and volunteers or with whom they were coordinated is not clear! We see a volunteer who puts a bank account number on Instagram to collect money for the affected people!” (P12).
Recommendations for building social trust
Social trust is important for proper disaster risk management and is an element of social capital. Social trust is considered as the cause and effect of social capital. The category of “recommendations for building social trust” had three subcategories.
Effective risk communication
According to the participants, people need to know the risks and self-protection methods during disasters. Accurate and early provision of information in understandable languages and on the social networks people trust and use enables people to make correct decisions and take action to protect themselves against hazards. Therefore, real-time communication between experts, managers, and lay people is important to gain trust and be better prepared against disasters. People’s trust should be gradually gained to promote social participation, and officials should make promises based on their abilities and capacities. The participants in this study argued that effective risk communication could improve social trust and social participation; “The authorities do not have to say something when they do not know the exact situation of the affected area! The timely provision of information is crucial. There should be transparency. Databases should be identified. Relief organizations should be in contact with people.” (P10, a 52-year-old male)
Experience-based measures
Given that the important cities of Iran are prone to natural disasters such as earthquakes, risk mitigation is necessary and should be preferred over post-disaster response and recovery, which is costly. In other words, the experience and knowledge should be used wisely. Accordingly, the most fundamental task is to get prepared for emergencies in order to be able to take appropriate measures, such as providing shelter and relief items to the affected people. During the COVID-19 pandemic, the timely supply of safe and approved vaccines was one of the measures that increased social trust.
“The most important action that should be taken at the time of disasters is to provide all affected people with the basic needs and lifesaving services. Some actions may be postponed, but relief items, medicines, food, and water should be available to people. Quickly attending the scene and helping victims will make people trust the emergency system more.” (P 3, a 26-year-old female).
Management improvement
According to the participants, the use of competent and experienced managers in emergency and relief organizations creates trust in society. When people see the presence of meritocracy and capable managers, their trust in the emergency system can be increased. Since Iran has a large geographical area, the use of local authorities and volunteers that are more familiar with the conditions and culture of the affected region contributes to better disaster risk management. The participants suggested that health issues should be the main priority of the organizations and that political views should not affect people’s health.
“In my opinion, the most important and best action to better manage health issues is the use of professional and compassionate managers who really care about their country and people and do not think about their personal interests. Another factor that should be considered in the selection of competent managers is their experience in the international areas. The one with related education has much more capability to manage disaster-related issues.” (P6, a 38-year-old male). “The health of people should be considered as the priority.” (P 2, a 28-year-old female).
Discussion
According to our findings, the main challenges to building social trust in Iranian society during disasters were managerial issues, misunderstanding of the situation, lack of transparency, and lack of coordination. The managerial issues included the subcategories of unfulfilled promises, inefficient human resource management, disorganized management of people, Improper vaccination management, and disorganized management of volunteers. For the category of “misunderstanding of the situation”, the subcategories included poor perception of the risk and the disaster shock. For the category of “lack of transparency”, the subcategories included distrust in relief organizations, lack of transparency and inconsistency of statistics and reports, and political approaches to health needs. For the category of “lack of coordination, the subcategories included lack of clarity in duties of relief organizations, conflict in the interests of relief organizations, organizational bias, and lack of coordinated communication.
We also presented some recommendations to help promote social trust in three categories of effective risk communication, experience-based measures, and management improvement. In this regard, transparency of actions and information, modification of the risk information programs, risk communication management, securing infrastructure, special attention to the risk mitigation phase in risk management, coordination between relief organizations, comprehensive and integrated resource management, emphasis on organizing volunteers, use of local and capable managers were recommended.
Inefficient human resource management was one of the challenges related to managerial issues. Adequate human resources are essential for preparedness against disasters such as COVID-19, albeit simply increasing the resources is not enough; there should be competent human resources to improve the quality of provided services [23]. This result suggests that the inefficient human resources management and supply chain management during the COVID-19 pandemic reduced people’s trust in the government and organizations in charge of managing the disease. The results of one study on human resource management during the COVID-19 pandemic indicated that the pandemic affected recruitment, selection, training, performance appraisal and management, rewards, and participation of employees, in addition to organizational performance [29]. Therefore, governments and human resource managers should take effective measures to cope with COVID-19 by optimizing strengths and eliminating weaknesses and environmental threats. Since one of the most fundamental ways to restore public trust is efficient functioning of organizations, and given that poor management has caused irreparable damage to social trust during the pandemic and even before it [30], employing competent, capable, and well-educated managers and placing them in positions tailored to their expertise can provide better results and promote social trust.
Challenges related to the COVID-19 vaccination, such as unclear biosafety of the imported vaccines, insufficient stockpile for the vaccines, misinformation about vaccines, and poor supply chain management were other challenges related to management issues [31]. A study found that one of the underlying causes of the decline in COVID-19 vaccination in West Africa was the vaccine shortage. This is why high mortality and infection rates were reported in West Africa [32]. So, if the vaccination coverage was completed soon, it would restore a high degree of the lost social trust in authorities and would give people hope that the crisis was going to end soon [33]. Miyachi et al. also indicated that one of the essential criteria for public trust in the government and the health care system was the history of vaccination [34].
Lack of knowledge of the nature and risk of COVID-19 and how to prepare was another challenge to social trust in Iran. In this study, citizens of Tehran did not take safety measures to eliminate the risks in their place of residence due to the lack of awareness of the disease risk. There was misinformation or disinformation about the disease risk. According to Taylor and Snyder, risk perception is related to safety behavior and creates commitment to safety [35]. Therefore, reducing and eliminating these factors is necessary to be appropriately prepared for disasters and reduce post-disaster causalities. Keeping the infrastructure safe and secure and taking preventive measures were reported by the participants in this study as recommendations to promote social trust.
Statistics about disasters, including COVID-19, are usually presented via mass media. These statistics often estimate the situation; in most cases, accurate data is unavailable (e.g. only the deaths of people who tested positive are reported). In addition, the news media report only some aspects of the disaster [36]. In our study, one of the challenges to social trust was the lack of transparency and inconsistency of data released by different organizations. News or social media play an essential role in reducing the damage caused by disasters [37]. However, because the government in Iran controls the news media (Radio or TV), social trust in them has decreased and the tendency to use social media has increased [36]. This issue can be a reason for the contradictory news and statistics reported by unofficial and official media in Iran, which can reduce social trust.
According to our results, political interests sometimes affect the disaster risk management process, leading to ignoring the opinion of experts. Therefore, taking a political approach to manage the risk of disasters was considered as a challenge to building social trust in Iran. Due to international sanctions, there were insufficient vaccines and drug procurement in Iran; without the World Health Organization’s (WHO) support, it was impossible to supply vaccines [38, 39]. Therefore, the public belief that political issues had affected the management of the COVID-19 pandemic in Iran was deemed accurate. According to recommendations, to restore the lost trust, there is a need to pay attention to low-income people and provide appropriate social protection programs for all people, especially the vulnerable groups. According to Yin et al. [40], the financial status of individuals has a direct relationship with their level of trust in the government. Moreover, income inequality and insufficient social protection programs have an inverse relationship with social trust [40].
The lack of clarity regarding missions and tasks in relief organizations was identified as one of the critical challenges in building social trust in Iran. The tasks of these organizations should be clarified, and inter-organizational coordination is needed to prevent confusion at the time of disasters [41]. Balcik et al. also suggest that the policies, guidelines, and procedures should be uniform and integrated to help organizations react more efficiently to disasters [42].
Conclusion
Managerial issues, misunderstanding of the situation, lack of transparency, and lack of coordination were the main challenges to building social trust in the emergency or relief organizations in Iran during the COVID-19 pandemic. The recommendations to improve social trust are the use of efficient risk communication methods, experience-based interventions, and managerial approaches. In this regard, focusing more on disaster risk mitigation by developing an early warning system and improving national surveillance system, capacity building, risk communication, public education for improving risk perception, transparency in organizational tasks and management of organizational conflicts, accurate and timely information through the trusted media, and mass vaccination focusing on vulnerable groups are some practical recommendations to increase social trust in Iran. Further quantitative studies are recommended to assess the relationship between social trust and community preparedness for disasters in Iran.
Limitations
There were some limitations in this research. The time of data collection coincided with the COVID-19 pandemic. Furthermore, our results have limited generalizability due to the qualitative design of this study. Another limitation was the unwillingness of some participants to continue participation in the face-to-face interviews amid the COVID-19 pandemic. In this regard, the in-depth interviews were conducted over the phone or Skype.
Ethical Considerations
Compliance with ethical guidelines
The study obtained ethical approval from the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Code: IR.USWR.REC.1399.065). Before the interviews, participants gave informed consent to participate in the study. Furthermore, the confidentiality of their information was observed.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and Supervision: Hamid Reza khankeh, Mehrdad Farrokhi and Juliet Roudini; Methodology: Hamid Reza khankeh, Mohammadjavad Hosseinabadi-farahani, and Mohammad Saatchi; Data collection: Amin Rahmatali Khazaee, Mariye Jenabi Ghods, Elham Sepahvand; Data analysis: Maryam Ranjbar, Taleb Badri; Writing the original draft: Sina Ahmadi, Mohammad Pourebrahimi, Maryam Ranjbar, and Amin Rahmatali Khazaee; Review, editing and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
Natural hazards threaten the lives of many people worldwide every year [1, 2]. Natural disasters accounted for 10,492 deaths, affected 101.8 million people, and caused approximately 252.1 billion US$ of economic losses [3, 4]. Iran, as a lower-middle-income country with a unique geopolitical position, has also been affected by disasters and their damage [5]. The number, variety, and severity of disasters in Iran have been increased in recent years [6, 7]. One of the recent disasters was the outbreak of COVID-19, which caused significant social problems [6, 7]. Iran experienced consecutive waves of COVID-19 [8, 9, 10]. In addition to its effects on the health system, it has many social consequences. The social management of such phenomenon requires the knowledge of its various aspects [11], proper inter-sectoral communication, and identification of factors affecting social trust, social health, and education [12, 13]. Early warning, proper planning, and timely responses can help considerably reduce the damage and adverse effects of unforeseen events like the COVID-19 pandemic [14]. It is necessary to have consensus and preparedness at all individual, social, and organizational levels to reduce the effects and damage caused by disasters [15].
Previous studies indicated that effective social communication is needed to understand the disaster risk [14, 16]. If such interaction can build social trust, it will create social cohesion and stability within a society. Social trust is an important aspect of individual and social relations and a prerequisite for proper social functioning, disaster risk perception, and effective communication for risk management. Social trust, a belief in the competence, honesty, or benevolence of the other party, is an important cause and consequence of functioning institutions [17] and controls human behaviors. Improvement in social trust is related to a proactive response to the crisis [18], and failure to do so can result in its deterioration. Siegrist and Zingg showed that trust in health services provider organizations and their managers positively affected people’s willingness to adopt recommended behavior [19]. Social Trust has a significant role in creating and maintaining order and social solidarity by facilitating social interactions [20-23].
Given that trust between community members and emergency and relief organizations is needed to build preparedness, it has become an important topic in the study of the impact of natural disasters [24]. People often act impulsively during disasters [25]. This makes it more difficult to provide the necessary aid to those in urgent need [26]. One study in Saudi Arabia conducted during the COVID-19 pandemic indicated that high levels of public trust in society are associated with increased success in disease prevention policies. Also, gender, age, marital status, and educational level were key predictors of precautionary practices [17]. The loss of social trust can exacerbate the psychological and social problems seen before the pandemic [17, 18]. Understanding the role of social trust in disasters and the related factors can help with community-based disaster risk management and reduce the burden of problems. Meanwhile, there is a lack of knowledge regarding social components and their role at the time of crisis. The COVID-19 pandemic and its consequences in Iran made it necessary to pay attention to social trust and its improvement in society. It is vital to measure the social trust status and the challenges facing Iranian society following disasters such as the COVID-19 pandemic to reduce vulnerability and improve resilience. Therefore, this study aims to investigate the challenges and provide recommendations for building social trust and preparedness against disasters such as COVID-19 in Iran.
Materials and Methods
Study design and participants
This is a qualitative study using a conventional content analysis method. Participants were lay people living in Tehran, the capital of Iran, who had experienced several disasters (n=20) and managers of emergency and relief organizations (n=7) who were willing to share their experiences (mean age=34.2 years). They were selected by purposive and snowball sampling methods with maximum diversity in terms of age, sex, level of education, and organizational position to explore perceptions and experiences of people from different angles (Table 1).
The inclusion criteria were age >24 years, ability to participate in interviews, and living in Tehran.
Data collection
After explaining the study objectives to the participants and obtaining their informed consent, data were collected using in-depth semi-structured interviews with each group until reaching theoretical saturation. Data collection lasted 4 months from June to September of 2020. The interview started with general and open-ended questions, such as “Have you experienced natural disasters in Tehran?”, “What do you think about the performance of emergency and relief organizations in Tehran?”, “How confident are you about the performance of emergency and relief organizations in disaster management?”, “How did you perceive the performance of health organizations during the COVID-19 pandemic?”, “What are the main challenges to managing disasters?” and “What do you recommend to improve the performance of these organizations?” Each interview also included probe and prompt questions, such as “Could you explain more about this?” and “What did you mean by saying this?” The focus of the questions then changed based on the participants’ answers. The participants chose the place and time for the interviews. The interviews were conducted face-to-face (n=16, in the workplace) or over the phone (n=11). In all face-to-face interviews, the researchers wore gloves and masks, and provided these safety items to the participants. The mean interview duration was 49 minutes (ranged 35-76 minutes). All interviews were recorded and transcribed verbatim.
Data analysis
The data were analyzed using the conventional content analysis method proposed by Graneheim and Lundman [27]. The transcriptions were read carefully. The significant semantic units were extracted, summarized, and coded. Multiple reading and note-taking during simultaneous interpretation helped identify the connections between the concepts extracted from the participants’ statements. The codes were classified based on similarities and differences, and the main themes (challenges and recommendations) were identified.
We used the four criteria proposed by Guba to assess the trustworthiness of collected data [28]. We tried to communicate well with the participants and increase the credibility of the data through long-term engagement and complete immersion in the data. In addition, we checked the accuracy in collaboration with participants (member checking). All interviews were recorded and transcribed verbatim to ensure the credibility of the data. To determine the dependability of the data, we recorded and reported all the steps and the made decisions so that others can follow and repeat the process, if necessary. To determine the transferability of the data, we tried to fully describe the research context by accurately describing the participant characteristics, research environment, sampling method, and time and place of interview.
Results
Four categories were found for the theme of “challenges to building social trust” and three categories for the theme of “recommendations for building social trust”, each with subcategories presented in Tables 2 and 3.
Challenges to building social trust
Managerial challenges
According to the participants’ experiences, one of the main challenges to building social trust was managerial issues. Social trust in emergency and relief organizations has been reduced due to unrealized promises, mismanagement of human resources, improper distribution of staff/resources, and lack of attention to and planning for volunteers. The lack of comprehensive risk assessment, which caused a delay in the early stages, and the lack of a response plan for COVID-19 (including a vaccination program) worsened the situation. The reduced trust made people pessimistic about the health and social conditions of the community.
“Unfortunately, the slogan of meritocracy was never realized because of the ridiculous phenomenon of credentialism. The disaster management system was completely passive in managing the pandemic; all these problems happened because of this mismanagement.” (Participant No. 6 (P6), a 38-year-old male). “I do not trust the system and those dealing with the COVID-19 situation! I think these organizations are trying to show everything as being normal because of their failure to manage the disease. I think it is so difficult to eradicate this social distrust; it did not happen overnight! So it cannot be eliminated overnight. Many things were said at the beginning of the pandemic several times, but these were later proven wrong; many promises were made that were not fulfilled after months. All these things caused social distrust. Some officials made a promise that was broken later by other officials!”(P2, a 28-year-old female).
Misunderstanding of the situation
Lack of knowledge and awareness about disaster preparedness and lack of education about measures that should be taken during a disaster caused people to fail to take the proper action, thinking that the only correct action is to leave the affected area. “We did not know much about safety measures! No one really knew! There should be an expert in this field [to teach people]. Based on the previous experience, many people knew that an earthquake might happen since a powerful earthquake happened here several years ago, such that this place was completely destroyed and people came back and built houses on the ruins. What I wanted to say is that we do not have enough information” (P4, a 34-year-old female).
Lack of transparency
Another challenge was the lack of transparency in released reports and information. Contradictory information and statistics on social media caused citizens to consider the information distributed by the emergency and relief organizations unreliable, so they lost trust in them.
“The information they report about the casualties or deaths that may occur is vital. If the information is true, people will trust them more. What people said differed from what was reported. If we pay attention, we can certainly do a lot during these events. Regarding financial aid, officials often say that they paid a lot of money, while people say something else, which makes many people not trust the information and not help government organizations. People prefer to help the victims directly! It is not clear who is right! There is a lot of controversy, which can cause distrust”(P14, a 26-year-old female).
Lack of coordination
In most cases, the leadership and management of the disaster in Iran is the responsibility of the National Emergency Management Organization; the organizations such as the Red Crescent, the army, and law enforcement forces act as supporting agents. However, in many cases, the responsibilities of each organization and institution are not well defined, leading to chaos and waste of time and resources.
A 31-year-old female participant said: “When a disaster happens, the members of the disaster management headquarters hold a meeting. To whom and where they sent all these relief items and volunteers or with whom they were coordinated is not clear! We see a volunteer who puts a bank account number on Instagram to collect money for the affected people!” (P12).
Recommendations for building social trust
Social trust is important for proper disaster risk management and is an element of social capital. Social trust is considered as the cause and effect of social capital. The category of “recommendations for building social trust” had three subcategories.
Effective risk communication
According to the participants, people need to know the risks and self-protection methods during disasters. Accurate and early provision of information in understandable languages and on the social networks people trust and use enables people to make correct decisions and take action to protect themselves against hazards. Therefore, real-time communication between experts, managers, and lay people is important to gain trust and be better prepared against disasters. People’s trust should be gradually gained to promote social participation, and officials should make promises based on their abilities and capacities. The participants in this study argued that effective risk communication could improve social trust and social participation; “The authorities do not have to say something when they do not know the exact situation of the affected area! The timely provision of information is crucial. There should be transparency. Databases should be identified. Relief organizations should be in contact with people.” (P10, a 52-year-old male)
Experience-based measures
Given that the important cities of Iran are prone to natural disasters such as earthquakes, risk mitigation is necessary and should be preferred over post-disaster response and recovery, which is costly. In other words, the experience and knowledge should be used wisely. Accordingly, the most fundamental task is to get prepared for emergencies in order to be able to take appropriate measures, such as providing shelter and relief items to the affected people. During the COVID-19 pandemic, the timely supply of safe and approved vaccines was one of the measures that increased social trust.
“The most important action that should be taken at the time of disasters is to provide all affected people with the basic needs and lifesaving services. Some actions may be postponed, but relief items, medicines, food, and water should be available to people. Quickly attending the scene and helping victims will make people trust the emergency system more.” (P 3, a 26-year-old female).
Management improvement
According to the participants, the use of competent and experienced managers in emergency and relief organizations creates trust in society. When people see the presence of meritocracy and capable managers, their trust in the emergency system can be increased. Since Iran has a large geographical area, the use of local authorities and volunteers that are more familiar with the conditions and culture of the affected region contributes to better disaster risk management. The participants suggested that health issues should be the main priority of the organizations and that political views should not affect people’s health.
“In my opinion, the most important and best action to better manage health issues is the use of professional and compassionate managers who really care about their country and people and do not think about their personal interests. Another factor that should be considered in the selection of competent managers is their experience in the international areas. The one with related education has much more capability to manage disaster-related issues.” (P6, a 38-year-old male). “The health of people should be considered as the priority.” (P 2, a 28-year-old female).
Discussion
According to our findings, the main challenges to building social trust in Iranian society during disasters were managerial issues, misunderstanding of the situation, lack of transparency, and lack of coordination. The managerial issues included the subcategories of unfulfilled promises, inefficient human resource management, disorganized management of people, Improper vaccination management, and disorganized management of volunteers. For the category of “misunderstanding of the situation”, the subcategories included poor perception of the risk and the disaster shock. For the category of “lack of transparency”, the subcategories included distrust in relief organizations, lack of transparency and inconsistency of statistics and reports, and political approaches to health needs. For the category of “lack of coordination, the subcategories included lack of clarity in duties of relief organizations, conflict in the interests of relief organizations, organizational bias, and lack of coordinated communication.
We also presented some recommendations to help promote social trust in three categories of effective risk communication, experience-based measures, and management improvement. In this regard, transparency of actions and information, modification of the risk information programs, risk communication management, securing infrastructure, special attention to the risk mitigation phase in risk management, coordination between relief organizations, comprehensive and integrated resource management, emphasis on organizing volunteers, use of local and capable managers were recommended.
Inefficient human resource management was one of the challenges related to managerial issues. Adequate human resources are essential for preparedness against disasters such as COVID-19, albeit simply increasing the resources is not enough; there should be competent human resources to improve the quality of provided services [23]. This result suggests that the inefficient human resources management and supply chain management during the COVID-19 pandemic reduced people’s trust in the government and organizations in charge of managing the disease. The results of one study on human resource management during the COVID-19 pandemic indicated that the pandemic affected recruitment, selection, training, performance appraisal and management, rewards, and participation of employees, in addition to organizational performance [29]. Therefore, governments and human resource managers should take effective measures to cope with COVID-19 by optimizing strengths and eliminating weaknesses and environmental threats. Since one of the most fundamental ways to restore public trust is efficient functioning of organizations, and given that poor management has caused irreparable damage to social trust during the pandemic and even before it [30], employing competent, capable, and well-educated managers and placing them in positions tailored to their expertise can provide better results and promote social trust.
Challenges related to the COVID-19 vaccination, such as unclear biosafety of the imported vaccines, insufficient stockpile for the vaccines, misinformation about vaccines, and poor supply chain management were other challenges related to management issues [31]. A study found that one of the underlying causes of the decline in COVID-19 vaccination in West Africa was the vaccine shortage. This is why high mortality and infection rates were reported in West Africa [32]. So, if the vaccination coverage was completed soon, it would restore a high degree of the lost social trust in authorities and would give people hope that the crisis was going to end soon [33]. Miyachi et al. also indicated that one of the essential criteria for public trust in the government and the health care system was the history of vaccination [34].
Lack of knowledge of the nature and risk of COVID-19 and how to prepare was another challenge to social trust in Iran. In this study, citizens of Tehran did not take safety measures to eliminate the risks in their place of residence due to the lack of awareness of the disease risk. There was misinformation or disinformation about the disease risk. According to Taylor and Snyder, risk perception is related to safety behavior and creates commitment to safety [35]. Therefore, reducing and eliminating these factors is necessary to be appropriately prepared for disasters and reduce post-disaster causalities. Keeping the infrastructure safe and secure and taking preventive measures were reported by the participants in this study as recommendations to promote social trust.
Statistics about disasters, including COVID-19, are usually presented via mass media. These statistics often estimate the situation; in most cases, accurate data is unavailable (e.g. only the deaths of people who tested positive are reported). In addition, the news media report only some aspects of the disaster [36]. In our study, one of the challenges to social trust was the lack of transparency and inconsistency of data released by different organizations. News or social media play an essential role in reducing the damage caused by disasters [37]. However, because the government in Iran controls the news media (Radio or TV), social trust in them has decreased and the tendency to use social media has increased [36]. This issue can be a reason for the contradictory news and statistics reported by unofficial and official media in Iran, which can reduce social trust.
According to our results, political interests sometimes affect the disaster risk management process, leading to ignoring the opinion of experts. Therefore, taking a political approach to manage the risk of disasters was considered as a challenge to building social trust in Iran. Due to international sanctions, there were insufficient vaccines and drug procurement in Iran; without the World Health Organization’s (WHO) support, it was impossible to supply vaccines [38, 39]. Therefore, the public belief that political issues had affected the management of the COVID-19 pandemic in Iran was deemed accurate. According to recommendations, to restore the lost trust, there is a need to pay attention to low-income people and provide appropriate social protection programs for all people, especially the vulnerable groups. According to Yin et al. [40], the financial status of individuals has a direct relationship with their level of trust in the government. Moreover, income inequality and insufficient social protection programs have an inverse relationship with social trust [40].
The lack of clarity regarding missions and tasks in relief organizations was identified as one of the critical challenges in building social trust in Iran. The tasks of these organizations should be clarified, and inter-organizational coordination is needed to prevent confusion at the time of disasters [41]. Balcik et al. also suggest that the policies, guidelines, and procedures should be uniform and integrated to help organizations react more efficiently to disasters [42].
Conclusion
Managerial issues, misunderstanding of the situation, lack of transparency, and lack of coordination were the main challenges to building social trust in the emergency or relief organizations in Iran during the COVID-19 pandemic. The recommendations to improve social trust are the use of efficient risk communication methods, experience-based interventions, and managerial approaches. In this regard, focusing more on disaster risk mitigation by developing an early warning system and improving national surveillance system, capacity building, risk communication, public education for improving risk perception, transparency in organizational tasks and management of organizational conflicts, accurate and timely information through the trusted media, and mass vaccination focusing on vulnerable groups are some practical recommendations to increase social trust in Iran. Further quantitative studies are recommended to assess the relationship between social trust and community preparedness for disasters in Iran.
Limitations
There were some limitations in this research. The time of data collection coincided with the COVID-19 pandemic. Furthermore, our results have limited generalizability due to the qualitative design of this study. Another limitation was the unwillingness of some participants to continue participation in the face-to-face interviews amid the COVID-19 pandemic. In this regard, the in-depth interviews were conducted over the phone or Skype.
Ethical Considerations
Compliance with ethical guidelines
The study obtained ethical approval from the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Code: IR.USWR.REC.1399.065). Before the interviews, participants gave informed consent to participate in the study. Furthermore, the confidentiality of their information was observed.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and Supervision: Hamid Reza khankeh, Mehrdad Farrokhi and Juliet Roudini; Methodology: Hamid Reza khankeh, Mohammadjavad Hosseinabadi-farahani, and Mohammad Saatchi; Data collection: Amin Rahmatali Khazaee, Mariye Jenabi Ghods, Elham Sepahvand; Data analysis: Maryam Ranjbar, Taleb Badri; Writing the original draft: Sina Ahmadi, Mohammad Pourebrahimi, Maryam Ranjbar, and Amin Rahmatali Khazaee; Review, editing and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
- Charney RL, Rebmann T, Esguerra CR, Lai CW, Dalawari P. Public perceptions of hospital responsibilities to those presenting without medical injury or illness during a disaster. The Journal of Emergency Medicine. 2013; 45(4):578-84. [DOI:10.1016/j.jemermed.2013.05.010] [PMID]
- Dewar B, Barr I, Robinson P. Hospital capacity and management preparedness for pandemic influenza in Victoria. Australian and New Zealand Journal of Public Health. 2014; 38(2):184-90. [DOI:10.1111/1753-6405.12170] [PMID]
- Frankenberg E, Sumantri C, Thomas D. Effects of a natural disaster on mortality risks over the longer term. Nature Sustainability. 2020; 3(8):614-9. [DOI:10.1038/s41893-020-0536-3] [PMID]
- Chen YE, Li C, Chang CP, Zheng M. Identifying the influence of natural disasters on technological innovation. Economic Analysis and Policy. 2021; 70:22-36. [DOI:10.1016/j.eap.2021.01.016]
- Ainehvand S, Raeissi P, Ravaghi H, Maleki M. Natural disasters and challenges toward achieving food security response in Iran. Journal of Education and Health Promotion. 2019; 8:51. [DOI:10.4103/jehp.jehp_256_18] [PMID]
- Ibrion M, Mokhtari M, Nadim F. Earthquake disaster risk reduction in Iran: Lessons and “lessons learned” from three large earthquake disasters-Tabas 1978, Rudbar 1990, and Bam 2003. International Journal of Disaster Risk Science. 2015; 6:415-27. [DOI:10.1007/s13753-015-0074-1]
- Najafi M, Ardalan A, Akbarisari A, Noorbala AA, Jabbari H. Demographic determinants of disaster preparedness behaviors amongst Tehran inhabitants, Iran. Plos Currents. 2015; 7:ecurrents.dis.976b0ab9c9d9941cbbae3775a6c5fbe6.[DOI:10.1371/currents.dis.976b0ab9c9d9941cbbae3775a6c5fbe6] [PMID]
- Yoosefi Lebni J, Irandoost SF, Safari H, Xosravi T, Ahmadi S, Soofizad G, et al. Lived experiences and challenges of the families of COVID-19 victims: A qualitative phenomenological study in Tehran, Iran. Inquiry: A Journal of Medical Care Organization, Provision and Financing. 2022; 59:469580221081405. [DOI:10.1177/00469580221081405] [PMID]
- Kang SH, Skidmore M. The effects of natural disasters on social trust: Evidence from South Korea. Sustainability. 2018; 10(9):2973. [DOI:10.3390/su10092973]
- Karimi SE, Ahmadi S, SoleimanvandiAzar N. Inequities as a social determinant of health: Responsibility in paying attention to the poor and vulnerable at risk of COVID-19. Journal of Public Health Research. 2021; 10(1):1904. [DOI:10.4081/jphr.2021.1904] [PMID]
- Nejad FN, Mohammadi Gharehghani MA, Ahmadi S. Collective and individual rationality dilemma and the failure of anti-Covid-19 policies: Why some people don’t wear masks? International Journal of Surgery. 2022; 105:106866. [DOI:10.1016/j.ijsu.2022.106866] [PMID]
- Khankeh H, Farrokhi M, Roudini J, Pourvakhshoori N, Ahmadi S, Abbasabadi-Arab M, et al. Challenges to manage pandemic of coronavirus disease (COVID-19) in Iran with a special situation: A qualitative multi-method study. BMC Public Health. 2021; 21(1):1919. [DOI:10.1186/s12889-021-11973-5] [PMID]
- Brüssow H, Timmis K. COVID-19: Long covid and its societal consequences. Environmental Microbiology. 2021; 23(8):4077-91. [DOI:10.1111/1462-2920.15634] [PMID]
- Rundmo T. Is it possible to prevent unforeseen events? In: Glenn-Egil T, editor. Interaction:’Samhandling’under risk. Oslo: Cappelen Damm Akademisk/NOASP (Nordic Open Access Scholarly Publishing); 2018. [Link]
- Gencer EA, Gencer EA. Natural disasters, urban vulnerability, and risk management: A theoretical overview. In: Gencer EA, editor.The interplay between urban development, vulnerability, and risk management: A case study of the Istanbul Metropolitan Area. Berlin: Springer; 2013. [DOI:10.1007/978-3-642-29470-9_2]
- Becker J, Johnston D, Paton D, Ronan K. How people use earthquake information and its influence on household preparedness in New Zealand. Journal of Civil Engineering and Architecture. 2012; 6(6):673-81. [Link]
- Almutairi AF, BaniMustafa Aa, Alessa YM, Almutairi SB, Almaleh Y. Public trust and compliance with the precautionary measures against COVID-19 employed by authorities in Saudi Arabia. Risk Management and Healthcare Policy. 2020:753-60. [DOI: 10.2147/RMHP.S257287]
- Thoresen S, Blix I, Wentzel-Larsen T, Birkeland MS. Trust and social relationships in times of the COVID-19 pandemic. European Journal of Psychotraumatology. 2021;12(sup1):1866418. [DOI: 10.1080/20008198.2020.1866418]
- Siegrist M, Zingg A. The role of public trust during pandemics. European psychologist. 2014. [DOI: 10.1027/1016-9040/a000169]
- Cvetkovich G. Social trust and the management of risk.London: Routledge; 2013. [DOI:10.4324/9781315071350]
- Haynes K, Barclay J, Pidgeon N. The issue of trust and its influence on risk communication during a volcanic crisis. Bulletin of Volcanology. 2008; 70:605-21. [DOI:10.1007/s00445-007-0156-z]
- Bostrom A, Atkinson E. Trust and Risk in Smallpox Vaccination. In: Earle tc (editor). Trust in cooperative risk management: Uncertainty and scepticism in the public mind. Abingdon: Routledge: 2007. [Link]
- Xue K, Guo S, Liu Y, Liu S, Xu D. Social networks, trust, and disaster-risk perceptions of rural residents in a multi-disaster environment: Evidence from Sichuan, China. International Journal of Environmental Research and Public Health. 2021; 18(4):2106. [DOI:10.3390/ijerph18042106] [PMID]
- McIvor D, Paton D, Johnston D. Modelling community preparation for natural hazards: understanding hazard cognitions. Journal of Pacific Rim Psychology. 2009; 3(2):39-46. [DOI:10.1375/prp.3.2.39]
- Asgarizadeh Z, Rafieian M, Dadashpour H. [The evaluation and analysis of empirical model of earthquake mitigation behaviors in Tehran households (Persian)]. Geography and Environmental Hazards. 2015; 4(3):39-60. [DOI:10.22067/geo.v4i3.41900]
- Camacho-Vallejo JF, González-Rodríguez E, Almaguer FJ, González-Ramírez RG. A bi-level optimization model for aid distribution after the occurrence of a disaster. Journal of Cleaner Production. 2015; 105:134-45. [DOI:10.1016/j.jclepro.2014.09.069]
- Graneheim UH, Lundman B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Education Today. 2004; 24(2):105-12. [DOI:10.1016/j.nedt.2003.10.001] [PMID]
- Guba EG. Criteria for assessing the trustworthiness of naturalistic inquiries. Educational Communication and Technology. 1981; 29:75-91. [DOI:10.1007/BF02766777]
- Tomčíková L, Svetozarovová N, Cocuľová J, Daňková Z. The impact of the global Covid-19 pandemic on the selected practices of human resources management in the relationship to the performance of tourism companies. GeoJournal of Tourism and Geosites. 2021; 35(2):525-30. [DOI:10.30892/gtg.35233-680]
- Büssing A, Baumann K, Surzykiewicz J. Loss of faith and decrease in trust in a higher source during COVID-19 in Germany. Journal of Religion and Health. 2022; 61(1):741-66. [DOI:10.1007/s10943-021-01493-2] [PMID]
- Mathivathanan K. Will COVID-19 vaccine equity be possible in India? Vaccine. 2021; 39(35):4928-9. [DOI:10.1016/j.vaccine.2021.07.049] [PMID]
- Afolabi MO, Wariri O, Saidu Y, Otu A, Omoleke SA, Ebenso B, et al. Tracking the uptake and trajectory of COVID-19 vaccination coverage in 15 West African countries: An interim analysis. BMJ Global Health. 2021; 6(12):e007518. [DOI:10.1136/bmjgh-2021-007518] [PMID]
- Khankeh HR, Farrokhi M, Khanjani MS, Momtaz YA, Forouzan AS, Norouzi M, et al. The barriers, challenges, and strategies of COVID-19 (SARS-CoV-2) vaccine acceptance: A concurrent mixed-method study in Tehran City, Iran. Vaccines. 2021; 9(11):1248. [DOI:10.3390/vaccines9111248] [PMID]
- Miyachi T, Takita M, Senoo Y, Yamamoto K. Lower trust in national government links to no history of vaccination. The Lancet. 2020; 395(10217):31-2. [DOI:10.1016/S0140-6736(19)32686-8] [PMID]
- Taylor WD, Snyder LA. The influence of risk perception on safety: A laboratory study. Safety Science. 2017; 95:116-24. [DOI:10.1016/j.ssci.2017.02.011]
- Anwar A, Malik M, Raees V, Anwar A. Role of mass media and public health communications in the COVID-19 pandemic. Cureus. 2020; 12(9):e10453. [DOI:10.7759/cureus.10453]
- Bridgman A, Merkley E, Loewen PJ, Owen T, Ruths D, Teichmann L, et al. The causes and consequences of COVID-19 misperceptions: Understanding the role of news and social media. Harvard Kennedy School Misinformation Review. 2020; 1(3). [Link]
- Abdoli A. Iran, sanctions, and the COVID-19 crisis. Journal of Medical Economics. 2020; 23(12):1461-5. [DOI:10.1080/13696998.2020.1856855] [PMID]
- Pormasoumi H, Rostami D, Jamebozorgi K, Mirshekarpour H, Heshmatnia J. COVID-19 management in Iran and international sanctions. European Journal of Translational Myology. 2022; 32(4). [DOI:10.4081/ejtm.2022.10777]
- Yin W, Kirkulak-Uludag B, Matthews K. Financialization, religion, and social trust in rural China. Plos One. 2020; 15(10):e0240114. [DOI:10.1371/journal.pone.0240114] [PMID]
- Dwivedi YK, Shareef MA, Mukerji B, Rana NP, Kapoor KK. Involvement in emergency supply chain for disaster management: A cognitive dissonance perspective. International Journal of Production Research. 2018; 56(21):6758-73. [DOI:10.1080/00207543.2017.1378958]
- Balcik B, Beamon BM, Krejci CC, Muramatsu KM, Ramirez M. Coordination in humanitarian relief chains: Practices, challenges and opportunities. International Journal of Production Economics. 2010; 126(1):22-34. [DOI:10.1016/j.ijpe.2009.09.008]
Type of article: Research |
Subject:
Qualitative
Received: 2023/11/27 | Accepted: 2024/07/7 | Published: 2025/01/1
Received: 2023/11/27 | Accepted: 2024/07/7 | Published: 2025/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
