

Volume 10, Issue 2 (Winter 2025)
Health in Emergencies and Disasters Quarterly 2025, 10(2): 107-114 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Delshad V, Khankeh H, Ebadi A, Bidzan M, Ghaedamini Harouni G, Stueck M. Measuring the Biopsychosocial Health of Emergency Medical Technicians in Tehran, Iran. Health in Emergencies and Disasters Quarterly 2025; 10 (2) :107-114
URL: http://hdq.uswr.ac.ir/article-1-593-en.html
URL: http://hdq.uswr.ac.ir/article-1-593-en.html
Vahid Delshad1 

 , Hamidreza Khankeh *2 , Abbas Ebadi3 , Mariola Bidzan4 , Gholamreza Ghaedamini Harouni5 , Marcus Stueck6
, Hamidreza Khankeh *2 , Abbas Ebadi3 , Mariola Bidzan4 , Gholamreza Ghaedamini Harouni5 , Marcus Stueck6
, Hamidreza Khankeh *2 , Abbas Ebadi3 , Mariola Bidzan4 , Gholamreza Ghaedamini Harouni5 , Marcus Stueck6
1- Health in Emergency and Disaster Research Center, Social Health Research Institute, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Health in Emergency and Disaster Research Center, Social Health Research Institute, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ,hrkhankeh@gmail.com
3- Nursing Care Research Center, Clinical Sciences Institute, Baqiyatallah University of Medical Sciences, Tehran, Iran.
4- Institute of Psychology, University of Gdansk, Gdansk, Poland.
5- Social Welfare Management Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ·
6- Group Academy of Work and Health, DPFA Academy, Leipzig, Germany.
2- Health in Emergency and Disaster Research Center, Social Health Research Institute, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ,
3- Nursing Care Research Center, Clinical Sciences Institute, Baqiyatallah University of Medical Sciences, Tehran, Iran.
4- Institute of Psychology, University of Gdansk, Gdansk, Poland.
5- Social Welfare Management Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ·
6- Group Academy of Work and Health, DPFA Academy, Leipzig, Germany.
Full-Text [PDF 529 kb]
(1074 Downloads)
| Abstract (HTML) (3624 Views)
Full-Text: (576 Views)
Introduction
Given the broad scope of health, its determinants are also diverse and include genetic, personal, environmental, lifestyle, and service quality factors [1]. Age, gender, job, social class, nutrition status, etc. play an important role in the health and well-being of people. Choosing a particular job often exposes individuals to risk factors of diseases tailored to the selected job. In addition, it indirectly affects social class, nutrition, housing status, and other activities of the person [1]. Most of people spend at least one-third of their life at work [2]. A person’s job has a role in shaping his/her social identity, meeting the needs in life, and creating social relationships. Changes in employment status, salary, benefits, position, etc. can put pressure on and cause stress and anxiety in individuals [3]. One of the fundamental problems that has arisen in recent decades due to the modernization of lifestyle, increased competition, and changes in occupational relationships is occupational stress. It is associated with reduced job satisfaction, anxiety, fatigue, depression, insomnia, errors, lack of concentration and calmness, difficulty thinking and decision-making, and serious physical problems in individuals [4]. Absenteeism, reduced job commitment, decreased performance and efficiency, increased incidence of accidents and unsafe work practices, increased complaints, and negative effects on employee recruitment are among the effects of occupational stress on the organization [5].
Pre-hospital emergency is one of the most stressful areas of the health system [6]. Occupational stress can negatively affect the health and well-being of emergency medical technicians (EMTs). They are often exposed to high levels of work-related stressors and traumatic situations. One of the main stressors for EMTs is high workload or work pressure. They have to make quick decisions to save the lives of injured people. The unpredictable nature of emergency calls, long working hours, and lack of breaks can also contribute to high occupational stress level in EMTs. In addition, they may face violent behaviors and critically ill patients and their families and witness distressing scenes, which can have a negative impact on their mental health. Moreover, shift work and irregular working hours can disrupt their sleep patterns and contribute to fatigue and exhaustion [7].
Adequate health levels, as well as a low level of occupational stress, can definitely reduce the incidence of occupational hazards [8]. Therefore, assessing the risk of occupational stress and its management is important to reduce the adverse psychological consequences of occupational stress [9]. Several studies have identified the effects of trauma and occupational stress on the mental health of EMTs [10, 11, 12, 13]. It has been demonstrated that organizational and occupational factors such as workload, job tasks, work shifts, little time to rest, and organizational supervision have a negative impact on EMTs [14-16]. For example, a study in Brazil showed that 90% of EMTs had emotional fatigue [17]. A study in Sweden showed that uncertain conditions of pre-hospital emergency services led to stress in EMTs [18]. In a study in the United States, EMTs perceived that life-threatening clinical conditions such as respiratory, cardiac, and trauma problems in children cause stress and anxiety in them [19]. In Iran, there are also studies on the stress level of EMTs. For example, Iranmanesh et al. in 2013 showed that 94% of EMTs had moderate post-traumatic stress disorder [20]. Delshad et al., in 2021, reported that biopsychosocial, occupational, and behavioral factors can affect the health of EMTs [1]. It is obvious that individuals who provide pre-hospital emergency services should be healthy in terms of biopsychosocial aspects so that patients can benefit from their quality services [21]. Addressing the occupational stress of EMTs is essential, not only for their own health and well-being but also for the effective delivery of emergency medical services to the patients. Therefore, this study aims to evaluate the biopsychosocial health of EMTs.
Methods
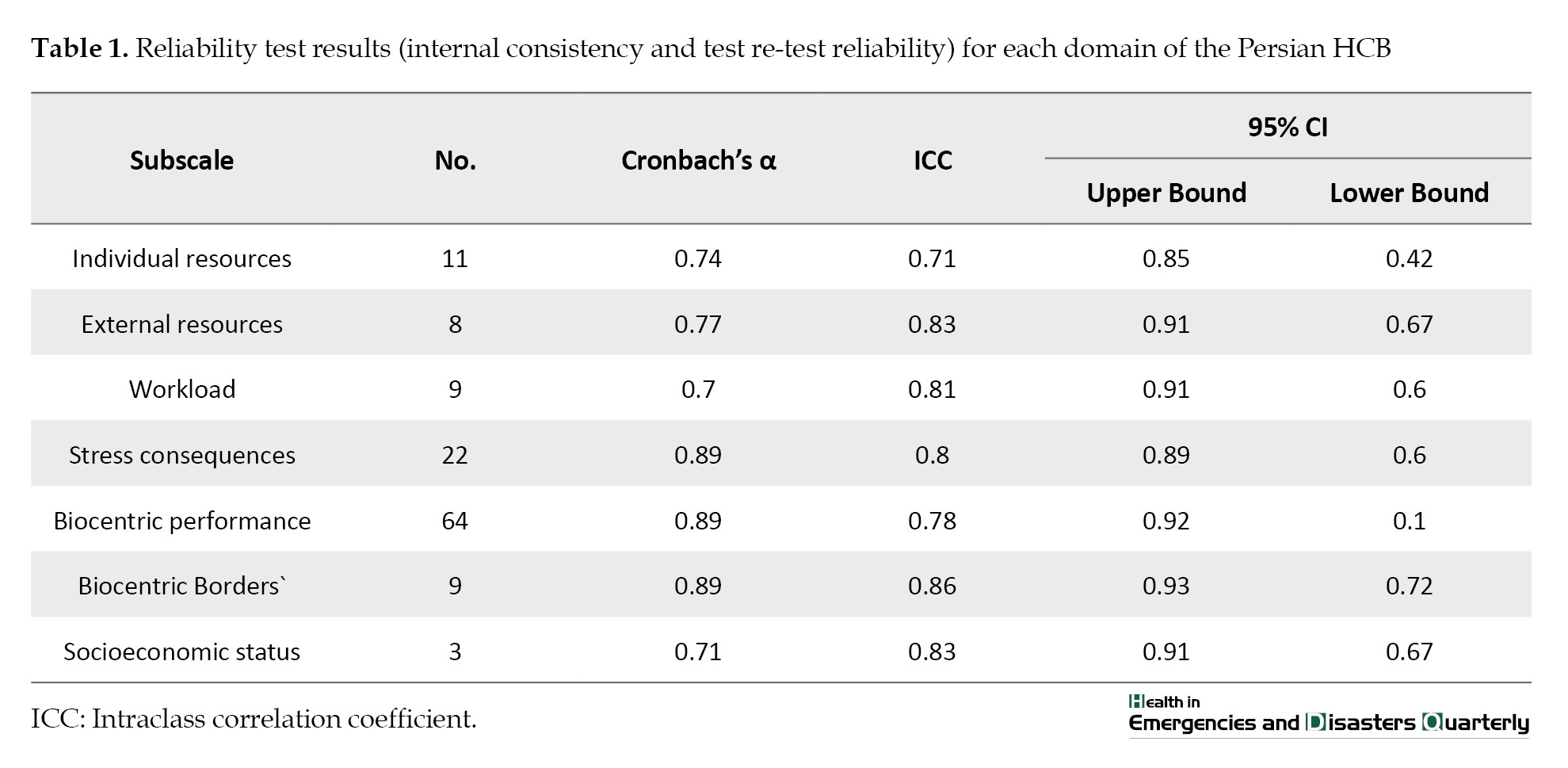
This is a descriptive cross-sectional study. The study population consists of the EMTs from six regions of Tehran, Iran, including north (n=266), south (n=334), east (n=312), west (n=363), central (n=286), and suburban (n=84) (total number=1645). Convenience sampling was used for selecting participants. The data collection tool was the health cube battery (HCB) developed by Stueck et al. based on the bio-centric health management model [22]. It is a self-assessment tool with 126 items for psychobiological risk assessment with domains of individual resources, external resources, workload, stress consequences, bio-centric performance, physiological reactions, and socioeconomic status. Since all participants were professionals with at least a university degree and had medical equipment for emergency services, their physiological reactions (e.g. blood pressure, pulse rate, and oxygen saturation) were self-assessed based on the guidelines. The calibration of assessment devices was done during field visits with the help of an emergency medical services supervisor, and the measurement of symptoms was assessed with the help of the emergency department and the managers from different regions and health centers. The HCB questionnaire was first translated using the forward-backward method based on the World Health Organization’s (WHO) translation and adaptation guideline [23]. Then, its face validity was assessed based on the opinions of 10 EMTs, and the content validity was assessed based on the opinions of 36 experts in pre-hospital emergency medical services, including psychologists, psychiatrists, psychiatric nurses, and emergency and disaster specialists. They were asked to assess the clarity, understandability, and necessity of each item. The necessity of each item was assessed based on a 3-point Likert scale (necessary, useful but not necessary, not necessary). The items with a content validity ratio (CVR) of <0.36 (according to the Lawshe table [24]) were excluded. Table 1 presents the results for internal consistency and test re-test reliability of the Persian version of HCB.
The data analysis was performed in Excel and SPSS software, version 22.
Results
The study population consists of 585 EMTs aged 20-60 years. The mean age of the population was 31.88±43.6 years, and the mean work experience in the emergency department was 14.7±73.5 years. As shown in Table 2, most of them were from the central region (40.9%), had an associate degree (59.5%), with an EMT/paramedics field of study (85.1%), and were ambulance drivers (65.3%), and male (97.9%).

Of 585 people, the females and operational managers, administrative staff, air rescuers, and dispatchers (n=22) were excluded from the study. Finally, data from 563 were used in the data analysis.
As shown in Table 3, the mean score of the biocentric performance was higher than other domains.
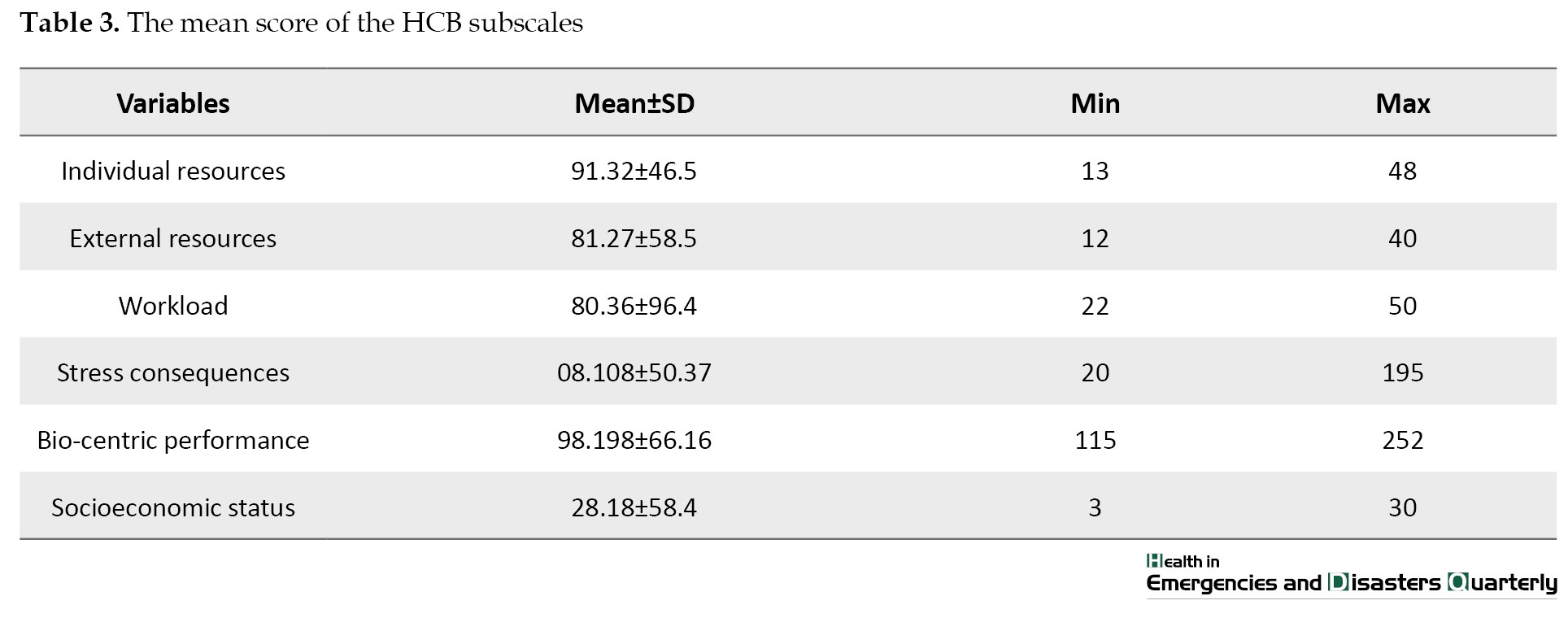
The mean scores of other domains were also higher than the average. However, in the domain of biocentric boundaries, the score was below average. As shown in Table 4, the mean levels of physiological conditions were within the normal range.
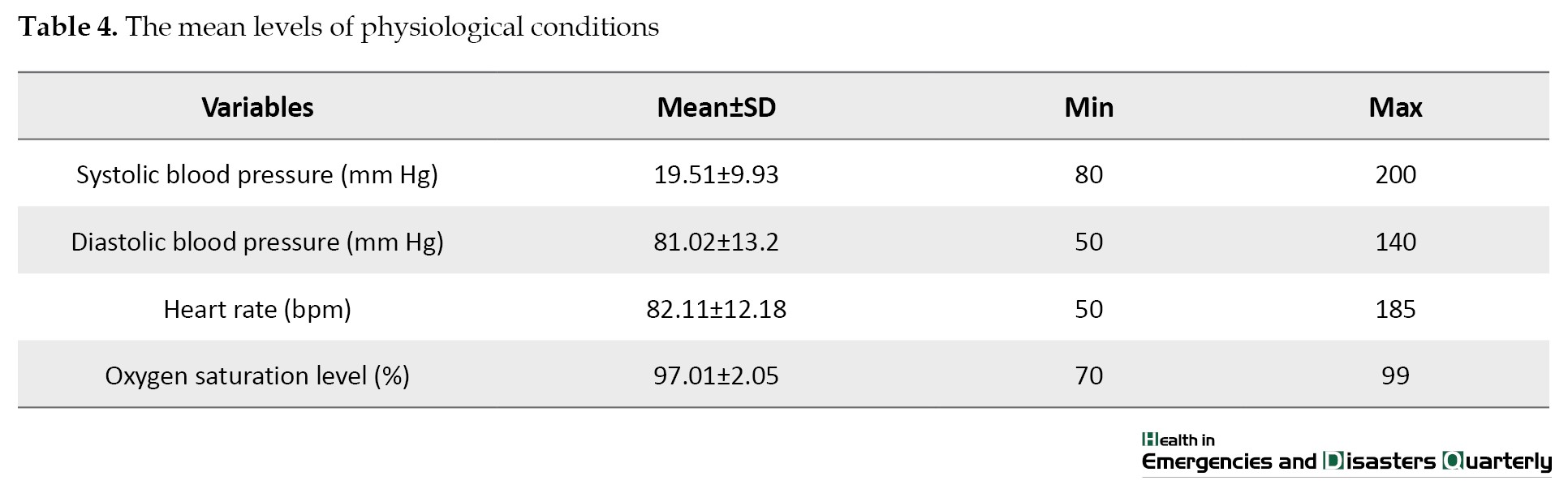
Table 5 presents the descriptive values of physiological conditions based on three levels of socioeconomic status (low, moderate, and high).
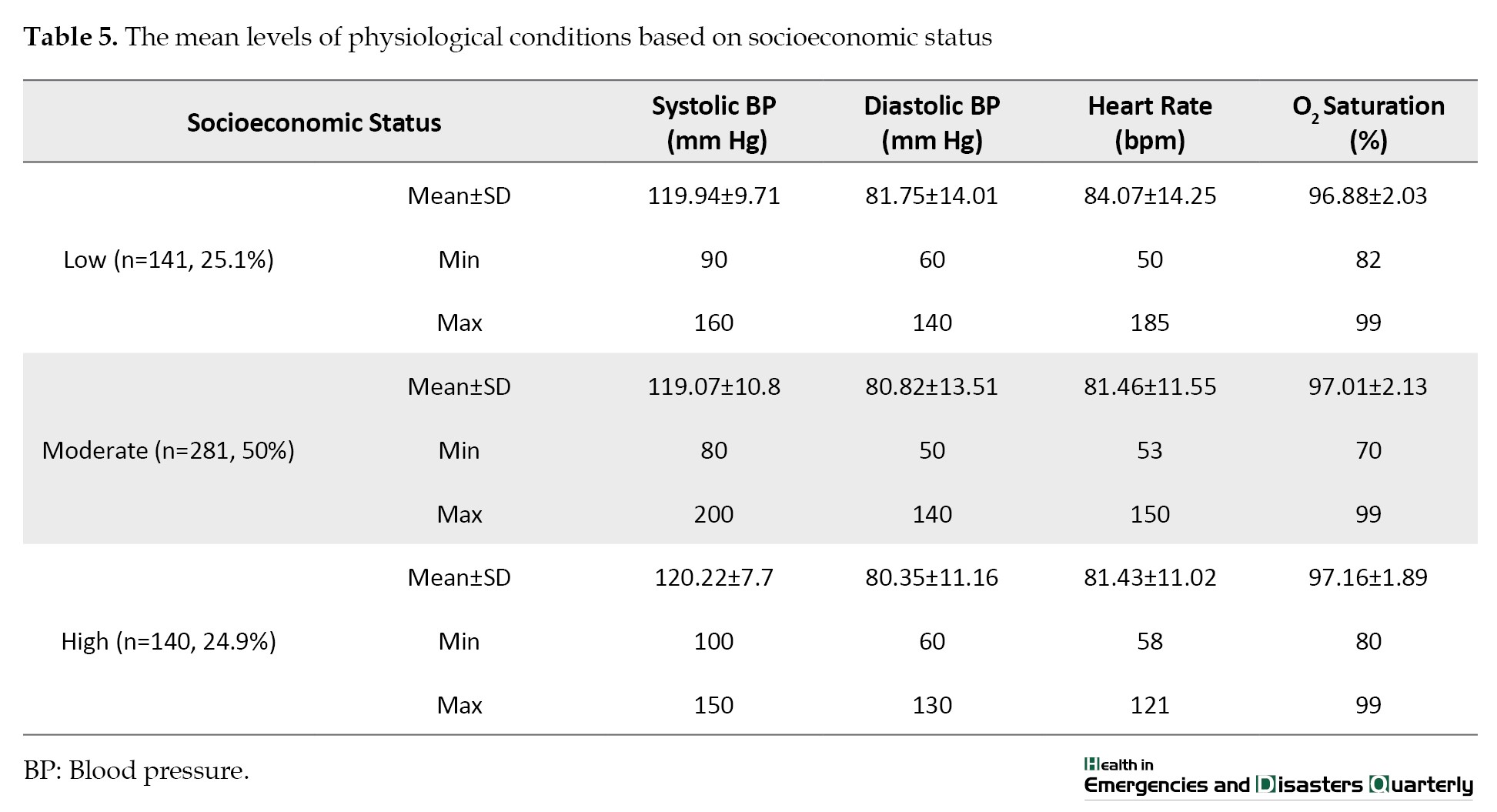
Overall, 50% of the participants reported moderate socioeconomic status, and there was no significant difference in terms of physiological conditions among the three socioeconomic groups, although there were noticeable differences in the minimum and maximum values.
Discussion
In the present study, the health status and socioeconomic conditions of EMTs in Tehran, Iran, were investigated. According to the findings, half of them had a moderate socioeconomic status. Those with higher socioeconomic status had higher performance and better physiological conditions.
In Nino et al.’s study in 2020 on the socio-psychological conditions of healthcare workers, it was reported that healthcare workers had different physical, psychological, social, biological, and individual characteristics. Factors such as increased mental workload, job fatigue, and lack of communication had negative effects on healthcare workers’ socio-psychological conditions [25]. Adam et al. in 2015, using an interpretative phenomenological analysis of stress and social health levels in EMTs [26], and Coxon et al in 2016, by examining the experiences of emergency operations center personnel, found that the nature of fast-paced work and job demands does not allow technicians to have physical rest and analyze incidents, which creates a vicious cycle for responders, ambulance clinical staff [27], ambulance volunteers, and dispatch personnel, resulting in an undesirable balance between work and life and poor recovery after shifts [28].
The main physical concern reported by EMTs is musculoskeletal injuries, especially back pain, due to patient handling and working in challenging environments. Other health concern is communicable diseases, which are more common in inexperienced staff. Some studies have reported that due to shift work and lack of exercise facilities in the workplace, EMTs find it difficult to maintain or improve their physical health and nutrition [29, 30], which is somewhat consistent with the present study. Most of the EMTs in our study had a moderate socioeconomic status. A study conducted in 2009 by Takeyama et al. in Japan showed that a modified ambulance night shift system can reduce fatigue and improve the physiological function of EMTs [31]. Their results are not consistent with the results of the present study, may be due to difference in the assessment of the function variable. In this study, the function was assessed using a self-report tool, whereas Takeyama et al. [31] measured the physiological function.
Several studies have confirmed the importance of systolic and diastolic blood pressure as physiological variables associated with health risks [32-35]. The fatigue and stress in healthcare workers can have a negative impact on their physical and mental health. Operational factors such as performance indicators, allocations, operational standards, response time, and expectations are factors that need to be managed by EMTs in addition to clinical roles and daily challenges [28]. Most studies on the sociopsychological conditions and resilience of EMTs have shown the effects of occupational stress. The EMTs use some strategies to cope with their work-related problems. One strategy used is the compartmentalization or segmentation of events and associated emotions to manage emergency demands and provide emergency services, which may be effective in the short term but may have negative effects in the long term (e.g. emotional distancing from the patient). Avoidance and information-seeking strategies are often used by nurses to regain a sense of control and manage demands [35].
The effects of occupational stress on the biopsychosocial health of EMTs can have an impact on their relationships with others. According to studies, stress is associated with individual characteristics. Evaluating stress and individual characteristics is essential for developing stress management programs. The EMTs are often faced with critical situations. Their emotional, cognitive, and behavioral responses to events are different before and after such situations [36]. Delshad et al. in 2021 showed that health management, biopsychosocial, occupational, and behavioral factors can affect the promotion of EMTs [1]. The EMTS and their families are under sociopsychological pressure. There should be a balance between work and receiving proper support and training for health management. Their study are consistent with the present study in terms of the necessity of examining sociopsychological factors and their impact on EMTs’ health.
Conclusion
The EMTs with better socioeconomic status can have better performance and physiological health. This highlights the need for more attention to the economic and social concerns of emergency workers, as it is considered an investment and not an expense. This investment has a direct impact on employee performance and indirect effects on their health, as well as costs such as sick leave, treatment, and replacement of workforce. It naturally affects the overall health of the community receiving emergency services.
Limitations
Due to the COVID-19 pandemic, it was not possible to assess all physiological variables. The physiological variables were assessed by a self-report tool, which was another limitation of the study. However, these limitations were partially controlled due to the large sample size and the use of standard operating procedures and random evaluations. This study was conducted in the Emergency Department of Tehran, with a high number and diversity of personnel. Given the impact of ethnicity, culture, climate, and location, it is recommended that further studies be conducted on more biological and physiological factors in different ethnic groups in Iran.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Code: IR.USWR.REC.1398.145).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Hamidreza Khankeh, Abbas Ebadi, Mariola Bidzan and Marcus Stueck; Methodology: Hamidreza Khankeh, Abbas Ebadi, Gholamreza Ghaedamini Harouni and Marcus Stueck; Software: Vahid Delshad, Abbas Ebadi, and Gholamreza Ghaedamini Harouni; Validation: Vahid Delshad and Hamidreza Khankeh; Investigation, data curation and writing: Vahid Delshad; Visualization: Vahid Delshad and Mariola Bidzan: Formal analysis: Vahid Delshad and Abbas Ebadi; Supervision and project administration|: Hamidreza Khankeh, Mariola Bidzan, and Marcus Stueck
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors would also like to extend their appreciation to the staff of Pre-Hospital Emergency Medical Services at Tehran.
References
Given the broad scope of health, its determinants are also diverse and include genetic, personal, environmental, lifestyle, and service quality factors [1]. Age, gender, job, social class, nutrition status, etc. play an important role in the health and well-being of people. Choosing a particular job often exposes individuals to risk factors of diseases tailored to the selected job. In addition, it indirectly affects social class, nutrition, housing status, and other activities of the person [1]. Most of people spend at least one-third of their life at work [2]. A person’s job has a role in shaping his/her social identity, meeting the needs in life, and creating social relationships. Changes in employment status, salary, benefits, position, etc. can put pressure on and cause stress and anxiety in individuals [3]. One of the fundamental problems that has arisen in recent decades due to the modernization of lifestyle, increased competition, and changes in occupational relationships is occupational stress. It is associated with reduced job satisfaction, anxiety, fatigue, depression, insomnia, errors, lack of concentration and calmness, difficulty thinking and decision-making, and serious physical problems in individuals [4]. Absenteeism, reduced job commitment, decreased performance and efficiency, increased incidence of accidents and unsafe work practices, increased complaints, and negative effects on employee recruitment are among the effects of occupational stress on the organization [5].
Pre-hospital emergency is one of the most stressful areas of the health system [6]. Occupational stress can negatively affect the health and well-being of emergency medical technicians (EMTs). They are often exposed to high levels of work-related stressors and traumatic situations. One of the main stressors for EMTs is high workload or work pressure. They have to make quick decisions to save the lives of injured people. The unpredictable nature of emergency calls, long working hours, and lack of breaks can also contribute to high occupational stress level in EMTs. In addition, they may face violent behaviors and critically ill patients and their families and witness distressing scenes, which can have a negative impact on their mental health. Moreover, shift work and irregular working hours can disrupt their sleep patterns and contribute to fatigue and exhaustion [7].
Adequate health levels, as well as a low level of occupational stress, can definitely reduce the incidence of occupational hazards [8]. Therefore, assessing the risk of occupational stress and its management is important to reduce the adverse psychological consequences of occupational stress [9]. Several studies have identified the effects of trauma and occupational stress on the mental health of EMTs [10, 11, 12, 13]. It has been demonstrated that organizational and occupational factors such as workload, job tasks, work shifts, little time to rest, and organizational supervision have a negative impact on EMTs [14-16]. For example, a study in Brazil showed that 90% of EMTs had emotional fatigue [17]. A study in Sweden showed that uncertain conditions of pre-hospital emergency services led to stress in EMTs [18]. In a study in the United States, EMTs perceived that life-threatening clinical conditions such as respiratory, cardiac, and trauma problems in children cause stress and anxiety in them [19]. In Iran, there are also studies on the stress level of EMTs. For example, Iranmanesh et al. in 2013 showed that 94% of EMTs had moderate post-traumatic stress disorder [20]. Delshad et al., in 2021, reported that biopsychosocial, occupational, and behavioral factors can affect the health of EMTs [1]. It is obvious that individuals who provide pre-hospital emergency services should be healthy in terms of biopsychosocial aspects so that patients can benefit from their quality services [21]. Addressing the occupational stress of EMTs is essential, not only for their own health and well-being but also for the effective delivery of emergency medical services to the patients. Therefore, this study aims to evaluate the biopsychosocial health of EMTs.
Methods
This is a descriptive cross-sectional study. The study population consists of the EMTs from six regions of Tehran, Iran, including north (n=266), south (n=334), east (n=312), west (n=363), central (n=286), and suburban (n=84) (total number=1645). Convenience sampling was used for selecting participants. The data collection tool was the health cube battery (HCB) developed by Stueck et al. based on the bio-centric health management model [22]. It is a self-assessment tool with 126 items for psychobiological risk assessment with domains of individual resources, external resources, workload, stress consequences, bio-centric performance, physiological reactions, and socioeconomic status. Since all participants were professionals with at least a university degree and had medical equipment for emergency services, their physiological reactions (e.g. blood pressure, pulse rate, and oxygen saturation) were self-assessed based on the guidelines. The calibration of assessment devices was done during field visits with the help of an emergency medical services supervisor, and the measurement of symptoms was assessed with the help of the emergency department and the managers from different regions and health centers. The HCB questionnaire was first translated using the forward-backward method based on the World Health Organization’s (WHO) translation and adaptation guideline [23]. Then, its face validity was assessed based on the opinions of 10 EMTs, and the content validity was assessed based on the opinions of 36 experts in pre-hospital emergency medical services, including psychologists, psychiatrists, psychiatric nurses, and emergency and disaster specialists. They were asked to assess the clarity, understandability, and necessity of each item. The necessity of each item was assessed based on a 3-point Likert scale (necessary, useful but not necessary, not necessary). The items with a content validity ratio (CVR) of <0.36 (according to the Lawshe table [24]) were excluded. Table 1 presents the results for internal consistency and test re-test reliability of the Persian version of HCB.
The data analysis was performed in Excel and SPSS software, version 22.
Results
The study population consists of 585 EMTs aged 20-60 years. The mean age of the population was 31.88±43.6 years, and the mean work experience in the emergency department was 14.7±73.5 years. As shown in Table 2, most of them were from the central region (40.9%), had an associate degree (59.5%), with an EMT/paramedics field of study (85.1%), and were ambulance drivers (65.3%), and male (97.9%).
Of 585 people, the females and operational managers, administrative staff, air rescuers, and dispatchers (n=22) were excluded from the study. Finally, data from 563 were used in the data analysis.
As shown in Table 3, the mean score of the biocentric performance was higher than other domains.
The mean scores of other domains were also higher than the average. However, in the domain of biocentric boundaries, the score was below average. As shown in Table 4, the mean levels of physiological conditions were within the normal range.
Table 5 presents the descriptive values of physiological conditions based on three levels of socioeconomic status (low, moderate, and high).
Overall, 50% of the participants reported moderate socioeconomic status, and there was no significant difference in terms of physiological conditions among the three socioeconomic groups, although there were noticeable differences in the minimum and maximum values.
Discussion
In the present study, the health status and socioeconomic conditions of EMTs in Tehran, Iran, were investigated. According to the findings, half of them had a moderate socioeconomic status. Those with higher socioeconomic status had higher performance and better physiological conditions.
In Nino et al.’s study in 2020 on the socio-psychological conditions of healthcare workers, it was reported that healthcare workers had different physical, psychological, social, biological, and individual characteristics. Factors such as increased mental workload, job fatigue, and lack of communication had negative effects on healthcare workers’ socio-psychological conditions [25]. Adam et al. in 2015, using an interpretative phenomenological analysis of stress and social health levels in EMTs [26], and Coxon et al in 2016, by examining the experiences of emergency operations center personnel, found that the nature of fast-paced work and job demands does not allow technicians to have physical rest and analyze incidents, which creates a vicious cycle for responders, ambulance clinical staff [27], ambulance volunteers, and dispatch personnel, resulting in an undesirable balance between work and life and poor recovery after shifts [28].
The main physical concern reported by EMTs is musculoskeletal injuries, especially back pain, due to patient handling and working in challenging environments. Other health concern is communicable diseases, which are more common in inexperienced staff. Some studies have reported that due to shift work and lack of exercise facilities in the workplace, EMTs find it difficult to maintain or improve their physical health and nutrition [29, 30], which is somewhat consistent with the present study. Most of the EMTs in our study had a moderate socioeconomic status. A study conducted in 2009 by Takeyama et al. in Japan showed that a modified ambulance night shift system can reduce fatigue and improve the physiological function of EMTs [31]. Their results are not consistent with the results of the present study, may be due to difference in the assessment of the function variable. In this study, the function was assessed using a self-report tool, whereas Takeyama et al. [31] measured the physiological function.
Several studies have confirmed the importance of systolic and diastolic blood pressure as physiological variables associated with health risks [32-35]. The fatigue and stress in healthcare workers can have a negative impact on their physical and mental health. Operational factors such as performance indicators, allocations, operational standards, response time, and expectations are factors that need to be managed by EMTs in addition to clinical roles and daily challenges [28]. Most studies on the sociopsychological conditions and resilience of EMTs have shown the effects of occupational stress. The EMTs use some strategies to cope with their work-related problems. One strategy used is the compartmentalization or segmentation of events and associated emotions to manage emergency demands and provide emergency services, which may be effective in the short term but may have negative effects in the long term (e.g. emotional distancing from the patient). Avoidance and information-seeking strategies are often used by nurses to regain a sense of control and manage demands [35].
The effects of occupational stress on the biopsychosocial health of EMTs can have an impact on their relationships with others. According to studies, stress is associated with individual characteristics. Evaluating stress and individual characteristics is essential for developing stress management programs. The EMTs are often faced with critical situations. Their emotional, cognitive, and behavioral responses to events are different before and after such situations [36]. Delshad et al. in 2021 showed that health management, biopsychosocial, occupational, and behavioral factors can affect the promotion of EMTs [1]. The EMTS and their families are under sociopsychological pressure. There should be a balance between work and receiving proper support and training for health management. Their study are consistent with the present study in terms of the necessity of examining sociopsychological factors and their impact on EMTs’ health.
Conclusion
The EMTs with better socioeconomic status can have better performance and physiological health. This highlights the need for more attention to the economic and social concerns of emergency workers, as it is considered an investment and not an expense. This investment has a direct impact on employee performance and indirect effects on their health, as well as costs such as sick leave, treatment, and replacement of workforce. It naturally affects the overall health of the community receiving emergency services.
Limitations
Due to the COVID-19 pandemic, it was not possible to assess all physiological variables. The physiological variables were assessed by a self-report tool, which was another limitation of the study. However, these limitations were partially controlled due to the large sample size and the use of standard operating procedures and random evaluations. This study was conducted in the Emergency Department of Tehran, with a high number and diversity of personnel. Given the impact of ethnicity, culture, climate, and location, it is recommended that further studies be conducted on more biological and physiological factors in different ethnic groups in Iran.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (Code: IR.USWR.REC.1398.145).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Hamidreza Khankeh, Abbas Ebadi, Mariola Bidzan and Marcus Stueck; Methodology: Hamidreza Khankeh, Abbas Ebadi, Gholamreza Ghaedamini Harouni and Marcus Stueck; Software: Vahid Delshad, Abbas Ebadi, and Gholamreza Ghaedamini Harouni; Validation: Vahid Delshad and Hamidreza Khankeh; Investigation, data curation and writing: Vahid Delshad; Visualization: Vahid Delshad and Mariola Bidzan: Formal analysis: Vahid Delshad and Abbas Ebadi; Supervision and project administration|: Hamidreza Khankeh, Mariola Bidzan, and Marcus Stueck
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors would also like to extend their appreciation to the staff of Pre-Hospital Emergency Medical Services at Tehran.
References
- Delshad V, Stueck M, Ebadi A, Bidzan M, Khankeh H. Bio-psycho-social health assessment in prehospital emergency technicians: A systematic review. Journal of Education and Health Promotion. 2022; 11:41. [DOI:10.4103/jehp.jehp_498_21] [PMID]
- Fathizadeh A, Khoshouei MS. The relationship between self-regulation and personality traits with job stress in University of Isfahan employees. Journal of Fundamentals of Mental Health. 2016; 19(1):14-21. [Link]
- Khatooni M, Mollahasan M, Khoainiha S. Job stress and its related factors in accountant employees of Qazvin University of Medical Sciences. Iran Occupational Health Journal. 2011; 8(2):66-76. [Link]
- Kushal A, Gupta S, Metha M, Singh MM. Study of stress among health care professionals: A systemic review. International Journal of Research Foundation of Hospital & Healthcare Administration. 2018; 6(1):6-11. [DOI:10.5005/jp-journals-10035-1084]
- Leka S, Griffiths A, Cox T. Work Organisation and stress, protecting workers health series No. 3. Geneva: World Health Organisation; 2003. [Link]
- Donnelly E. Work-related stress and posttraumatic stress in emergency medical services. Prehospital Emergency Care. 2012; 16(1):76-85. [DOI:10.3109/10903127.2011.621044] [PMID]
- Emergency Medical Services Agency. Occupational stress and mental health among pre-hospital emergency personnel: A review of the literature [internet]. 2021 [updated 2021 December 12].
- Wang PC, Delp L. Health status, job stress and work-related injury among Los Angeles taxi drivers. Work. 2014; 49(4):705-12. [DOI:10.3233/WOR-131696] [PMID]
- Stueck M, Delshad V, Roudini J, Khankeh H, Ranjbar M, Reschke K, et al. Health cube with school of empathy and stress reduction for Iranian Drivers: New tools for traffic psychology and biocentric health management in Iran. Modern Care Journal. 2019; 16(2):e90632. [DOI:10.5812/modernc.90632]
- Donnelly E, medicine DS-P and disaster, 2009 undefined. Occupational risk factors in the emergency medical services. cambridge.org. [DOI:10.1017/S1049023X00007251] [PMID]
- Gist R, Taylor VH. Occupational and organizational issues in emergency medical services behavioral health. Journal of Workplace Behavioral Health. 2008; 23(3):309-30. [DOI:10.1080/15555240802243120]
- Klimley KE, Van Hasselt VB, Stripling AM. Posttraumatic stress disorder in police, firefighters, and emergency dispatchers. Aggression and Violent Behavior. 2018; 43:33-44. [DOI:10.1016/j.avb.2018.08.005]
- Sterud T, Ekeberg Ø, Hem E. Health status in the ambulance services: A systematic review.BMC Health Services Research. 2006; 6:82. [DOI:10.1186/1472-6963-6-82] [PMID]
- Lanza A, Roysircar G, Rodgers S. First responder mental healthcare: Evidence-based prevention, postvention, and treatment. Professional Psychology: Research and Practice. 2018; 49(3):193–204. [DOI:10.1037/pro0000192]
- Lewis-Schroeder NF, Kieran K, Murphy BL, Wolff JD, Robinson MA, Kaufman ML. Conceptualization, assessment, and treatment of traumatic stress in first responders: A review of critical issues. Harvard Review of Psychiatry. 2018; 26(4):216-27. [DOI:10.1097/HRP.0000000000000176] [PMID]
- Cheng MK, Joseph J, Ferguson D. A cognitive behavioral model of first responder posttraumatic stress disorder. Journal of Cognitive Psychotherapy. 2018; 32(3):184-91. [DOI:10.1891/0889-8391.32.3.184] [PMID]
- França SP, De Martino MM, Aniceto EV, Silva LL. Predictors of burnout syndrome in nurses in the prehospital emergency services. Acta Paulista de Enfermagem. 2012; 25(1):68-73. [DOI:10.1590/S0103-21002012000100012]
- Bohström D, Carlström E, Sjöström N. Managing stress in prehospital care: Strategies used by ambulance nurses. International Emergency Nursing. 2017; 32:28-33. [DOI:10.1016/j.ienj.2016.08.004] [PMID]
- Guise JM, Hansen M, O'Brien K, Dickinson C, Meckler G, Engle P, et al. Emergency medical services responders› perceptions of the effect of stress and anxiety on patient safety in the out-of-hospital emergency care of children: A qualitative study. BMJ Open. 2017; 7(2):e014057. [DOI:10.1136/bmjopen-2016-014057] [PMID]
- Iranmanesh S, Tirgari B, Bardsiri HS. Post-traumatic stress disorder among paramedic and hospital emergency personnel in south-east Iran. World Journal of Emergency Medicine. 2013; 4(1):26-31. [DOI:10.5847/wjem.j.issn.1920-8642.2013.01.005] [PMID]
- Aringhieri R, Bruni ME, Khodaparasti S, van Essen JT. Emergency medical services and beyond: Addressing new challenges through a wide literature review. Computers & Operations Research. 2017; 78:349-68. [DOI:10.1016/j.cor.2016.09.016]
- Stueck, M. The pandemic management theory. COVID-19 and biocentric development. Health Psychology Report. 2021; 9(2): 101–28. [DOI: 10.5114/hpr.2021.103123] [PMID]
- Lawshe, C. A quantitative approach to content validity. Personnel Psychology. 1975; 28(4): 563-75. [DOI: 10.1111/j.1744-6570. 1975.tb01393.x]
- Delshad V, Khankeh H, Ebadi A, Bidzan M, Harouni G, Stueck M. Psychobiological risk assessment in emergency medical service drivers: Study protocol for structural equation modeling. Health Psychology Report. 2020; 8(4):453-61. [DOI:10.5114/hpr.2020.99455]
- Nino L, Marchak F, Claudio D. Physical and mental workload interactions in a sterile processing department. International Journal of Industrial Ergonomics. 2020; 76:102902. [DOI:10.1016/j.ergon.2019.102902]
- Adams K, Shakespeare-Finch J, Armstrong D. An interpretative phenomenological analysis of stress and well-being in emergency medical dispatchers. Journal of Loss and Trauma. 2015; 20(5):430-48. [DOI:10.1080/15325024.2014.949141]
- Coxon A, Cropley M, Schofield P, Start K, Horsfield C, Quinn T. ‹You›re never making just one decision›: Exploring the lived experiences of ambulance Emergency Operations Centre personnel. Emergency Medicine Journal. 2016; 33(9):645-51. [DOI:10.1136/emermed-2015-204841] [PMID]
- Gallagher S, McGilloway S. Living in critical times: The impact of critical incidents on frontline ambulance personnel: A qualitative perspective. International Journal of Emergency Mental Health. 2007; 9(3):215-23. [PMID]
- Flannery RB. Treating psychological trauma in first responders: A multi-modal paradigm. The Psychiatric Quarterly. 2015; 86(2):261-7. [DOI:10.1007/s11126-014-9329-z] [PMID]
- Rice V, Glass N, Ogle K, Parsian N. Exploring physical health perceptions, fatigue and stress among health care professionals. Journal of Multidisciplinary Healthcare. 2014; 7:155-61. [DOI:10.2147/JMDH.S59462] [PMID]
- Takeyama H, Itani T, Tachi N, Sakamura O, Murata K, Inoue T, et al. Effects of a modified ambulance night shift system on fatigue and physiological function among ambulance paramedics. Journal of Occupational Health. 2009; 51(3):204-9. [DOI:10.1539/joh.L7040] [PMID]
- Stueck M, Rigotti T, Roudini J, Galindo E, Utami DS. Relationship between blood pressure and psychological features of experience and behaviour among teachers. Health Psychology Report. 2015; 4(2):128-36. [DOI:10.5114/hpr.2016.56853]
- Pushpa K, Kanchana R. Comparison of waist-hip ratio, prehypertension, and hypertension in young male bus drivers and non-drivers of Bengaluru city. National Journal of Physiology, Pharmacy and Pharmacology. 2019; 9(1):90-4. [Link]
- Balzer HU, Hecht K. Chronobiologische Aspekte des Schlafverhaltens. In: Hecht K, Engfer A, Peter JH, Poppei M, editors. Schlaf, Gesundheit, Leistungsfähigkeit. Berlin: Springer ; 1993. [DOI:10.1007/978-3-642-77111-8_7]
- Barzideh M, Choobineh A,.Job stress dimensions and their relationship to general health status in nurses. Tibbi-i-kar. 2012; 4(3):17-27. [Link]
- Donnelly EA, Bennett M. Development of a critical incident stress inventory for the emergency medical services. Traumatology: An International Journal. 2014; 20(1):1-8. [DOI:10.1177/1534765613496646]
Type of article: Research |
Subject:
Emergency
Received: 2023/12/4 | Accepted: 2024/07/29 | Published: 2025/01/1
Received: 2023/12/4 | Accepted: 2024/07/29 | Published: 2025/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
