

Volume 11, Issue 1 (Autumn 2025)
Health in Emergencies and Disasters Quarterly 2025, 11(1): 65-76 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Niaraees Zavare A S, Moazam E, Sohrabi K, Najafi Shahkoohi E, Najafi Shahkoohi A, Rezaei F. The Provision of Palliative Services in Iranian Hospitals During the COVID-19 Pandemic. Health in Emergencies and Disasters Quarterly 2025; 11 (1) :65-76
URL: http://hdq.uswr.ac.ir/article-1-608-en.html
URL: http://hdq.uswr.ac.ir/article-1-608-en.html
Asal Sadat Niaraees Zavare1 

 , Elham Moazam2 , Karim Sohrabi3 , Elaheh Najafi Shahkoohi4 , Atefeh Najafi Shahkoohi1 , Fatemeh Rezaei *5
, Elham Moazam2 , Karim Sohrabi3 , Elaheh Najafi Shahkoohi4 , Atefeh Najafi Shahkoohi1 , Fatemeh Rezaei *5
, Elham Moazam2 , Karim Sohrabi3 , Elaheh Najafi Shahkoohi4 , Atefeh Najafi Shahkoohi1 , Fatemeh Rezaei *5
1- Department of Health Economics, School of Health Management and Information Sciences, Iran University of Medical Sciences, Tehran, Iran.
2- Cancer Prevention Research Center, Isfahan University of Medical Sciences, Isfahan, Iran.
3- Department of Emergency Medicine, School of Medicine, Isfahan University of Medical Sciences, Isfahan, Iran.
4- Department of Health Management, Policy and Economics, School of Public Health, Tehran University of Medical Science, Tehran, Iran.
5- Department of Health in Disasters and Emergencies, Social Determinants of Health Research Center, School of Management and Medical Informatics, Isfahan University of Medical Science, Isfahan, Iran. ,f.rezaei.pro@gmail.com
2- Cancer Prevention Research Center, Isfahan University of Medical Sciences, Isfahan, Iran.
3- Department of Emergency Medicine, School of Medicine, Isfahan University of Medical Sciences, Isfahan, Iran.
4- Department of Health Management, Policy and Economics, School of Public Health, Tehran University of Medical Science, Tehran, Iran.
5- Department of Health in Disasters and Emergencies, Social Determinants of Health Research Center, School of Management and Medical Informatics, Isfahan University of Medical Science, Isfahan, Iran. ,
Full-Text [PDF 517 kb]
(605 Downloads)
| Abstract (HTML) (2308 Views)
Full-Text: (413 Views)
Introduction
The World Health Organization (WHO) defines palliative care as an approach aimed at enhancing the quality of life for patients, both adults and children, and their families facing challenges associated with life-threatening illnesses [1]. The primary goal of palliative care is to mitigate and prevent suffering through the timely identification, precise evaluation, and treatment of pain and other related issues, encompassing physical, psychosocial, and spiritual aspects [2]. Ensuring access to palliative care is crucial for providing comprehensive and compassionate support to patients and families throughout the disease trajectory, spanning from diagnosis to death and bereavement, across all care settings [3].
The COVID-19 pandemic has subjected patients, their families, and caregivers to multifaceted suffering, including physical, psychological, social, and spiritual dimensions. Palliative care services address many of these concerns and pressures. The incorporation of palliative care into emergency management strategies has been emphasized in response to the spread of infectious diseases, like COVID-19 [4]. Research conducted in various countries following the onset of the COVID-19 pandemic underscores the vital role of palliative care in addressing patients’ complex needs during this challenging period and has revealed several adaptations implemented by healthcare providers [5-9]. These approaches include home- and community-based palliative care integrated with telehealth and innovative virtual hubs [10-12].
Extensive research has established the importance of cultural factors, spirituality, and religious coping mechanisms in the context of serious illnesses [13]. The implementation of palliative care is influenced by numerous cultural elements, such as family dynamics, elder care practices, physician roles, health-related decision-making processes, and the acceptance of life-threatening diagnoses [13, 14].
As one of the first countries to face the challenges posed by the COVID-19 pandemic, Iran’s healthcare professionals developed measures and adaptations to address the disease within the constraints of their resources and cultural and religious context, despite limited experience in palliative care [15]. Insights from global innovators in palliative care within resource-limited settings offer valuable perspectives for nations grappling with the COVID-19 emergency [12]. This study aimed to investigate the provision of palliative services during the COVID-19 pandemic within the Iranian healthcare system. Our findings will contribute to the development of a unified vision among various institutions, fostering collaborative efforts to attract multilateral support. Additionally, this research will inform policy decisions, disseminate critical knowledge, drive quality improvement initiatives, and advocate for the essential role of palliative care in preserving patient dignity and comfort during public health emergencies, such as COVID-19.
Materials and Methods
This study constituted a conductive content analysis conducted in two primary phases in 2022. A two-phased approach was implemented to obtain a comprehensive understanding of palliative care services provided during the COVID-19 pandemic. The semi-structured interviews facilitated a thorough examination of individual experiences and insights, while the expert panels enabled collective validation and expansion of these findings through collaborative discussion among palliative care professionals. Initially, purposive sampling was employed, subsequently augmented by snowball sampling, to achieve data saturation. A total of 17 individuals were selected to participate in this study through the application of purposive sampling.
Two trained researchers conducted semi-structured interviews with the participants. The interviews addressed several key questions, including: 1) Please describe the measures you have taken in the field of palliative care for patients with COVID-19; 2) Please describe the measures you have taken in each of the following areas: Physical, psychological, social and spiritual care; 3) Please describe the measures that have been taken to provide support to the patient’s family and relatives; 4) In the case of patients who have died, have measures been taken to provide support to their families in the period of bereavement?; 5) Please describe the new medicine or procedure that has been used to relieve pain and improve the quality of life of patients; and 6) In the context of palliative care for patients with COVID-19, which measures have you identified as the most significant and impactful? Please provide a rationale for your selection.
The participants were professionals with a minimum of five years of experience, employed in various positions in hospitals. They all possessed at least a bachelor’s degree and had diverse roles and responsibilities related to providing services to patients diagnosed with COVID-19. Following the completion of five interviews, an interview guide was developed to facilitate further questioning and analysis based on the data obtained. Upon completion of 17 interviews, it was determined that data saturation had been achieved. Subsequently, each code was either added as a new code or integrated into the predefined categories. The interviews were transcribed and subjected to thematic analysis utilizing MAXQDA 2018.1. The initial codes were identified from the data and subsequently refined into themes through both independent analysis and consensus meetings conducted among the research team.
The findings from the initial phase were utilized to inform the structure and focus of the expert panels, thereby ensuring that the discussions were predicated on previously identified themes from the interviews. Subsequently, three expert panels were convened, and key informants in the field of palliative care were invited to participate. To ensure the quality and relevance of the expert panel members, the inclusion criteria were as follows: 1) Relevant education and specialization- a formal degree in palliative care, nursing, medicine, social work, or a related field with a strong emphasis on palliative care principles; 2) Professional experience- a minimum of five years of professional experience in palliative care or educational settings; 3) Familiarity with the Iranian health system- adequate knowledge and understanding of the Iranian health system. Those who were unable to commit the requisite time and to work within a diverse expert panel were excluded from participation.
The participants of the expert panels were not among those whom we interviewed. A facilitator was responsible for initiating and directing the discussion, with the objective of eliciting recommendations regarding the reorganization of the initially developed categories. The panels were conducted in the presence of researchers and five experts in the field of palliative care. Following the identification of the primary sub-categories, categories, and concepts, through a review of the panels’ experts’ input, the findings were refined to exclude themes and verbal codes that were not within the scope of palliative care services.
The coding was conducted with two independent analysts adopting a constant comparative analysis approach and utilizing MAXQDA 2018.1 software. Specific categories were developed based on recurring themes, and a consensus was reached through a process of collective deliberation during the research team meetings. To ensure the consistency and accuracy of the coding process, weekly meetings were held to evaluate the inter-rater reliability of the codes and create categories by data analysts. In instances where discrepancies arose between analysts, a third party with expertise in qualitative research and a registered member of the palliative care association was consulted to provide a final decision. The Kappa coefficient score in these instances reached 98%.
Subsequently, the data were integrated to provide health systems and health authorities with comprehensive palliative care, thereby enhancing the quality of patient care and introducing a range of adaptable palliative care measures that could be selected based on the specific circumstances of each hospital.
Results
Table 1 presents a comprehensive overview of the 17 participants, including their job titles, educational qualifications, age, gender, and city of work.
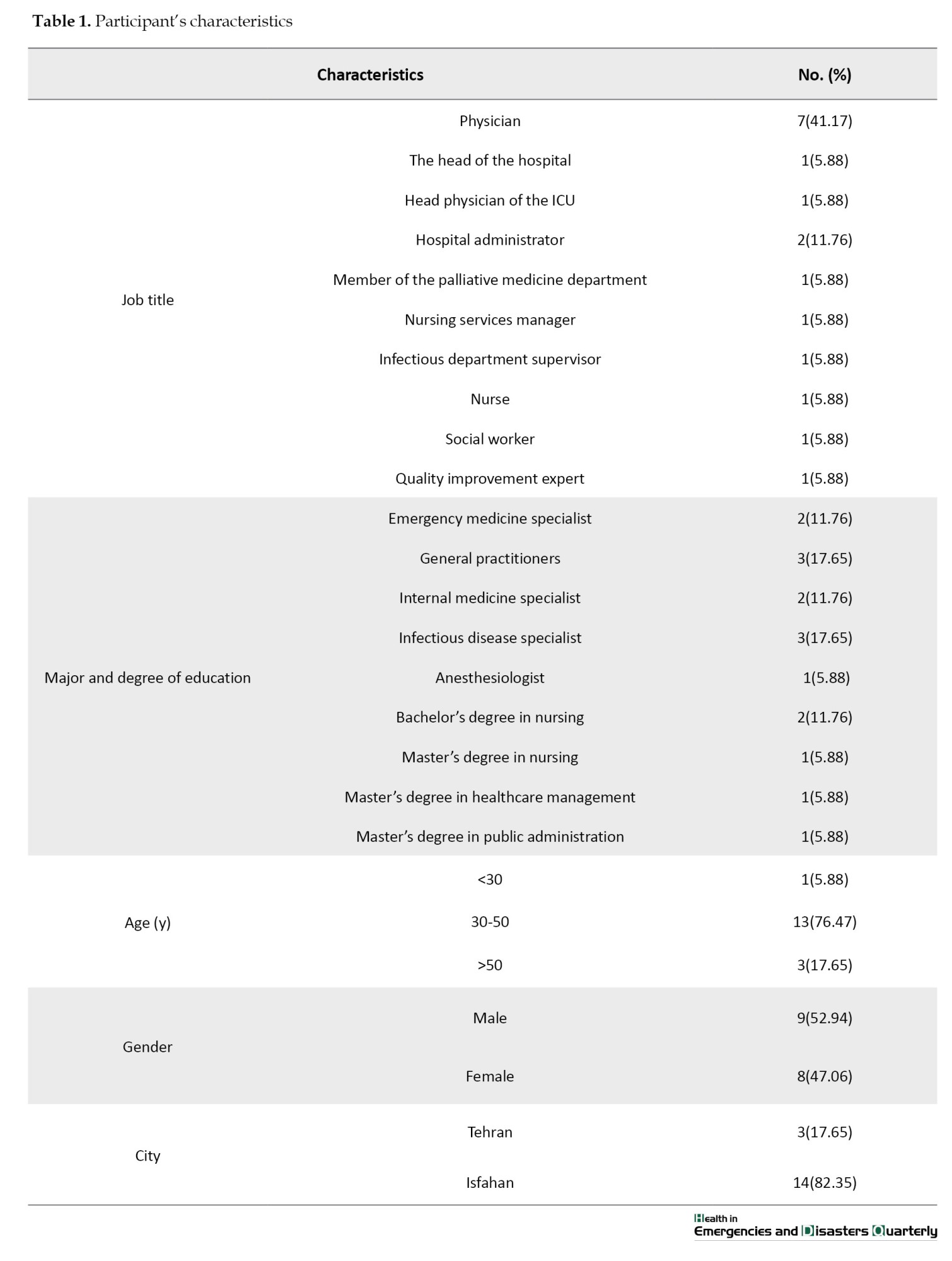
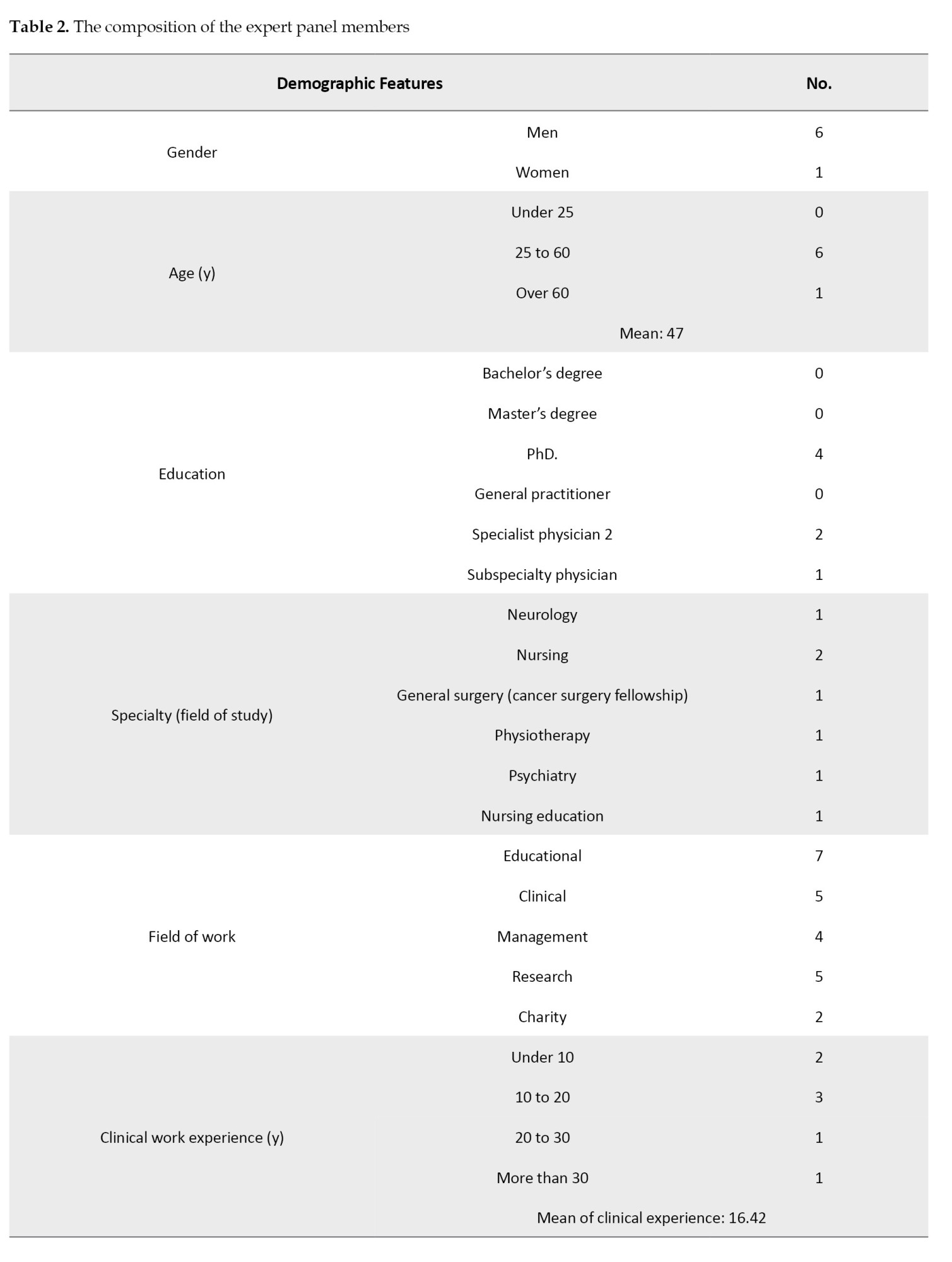
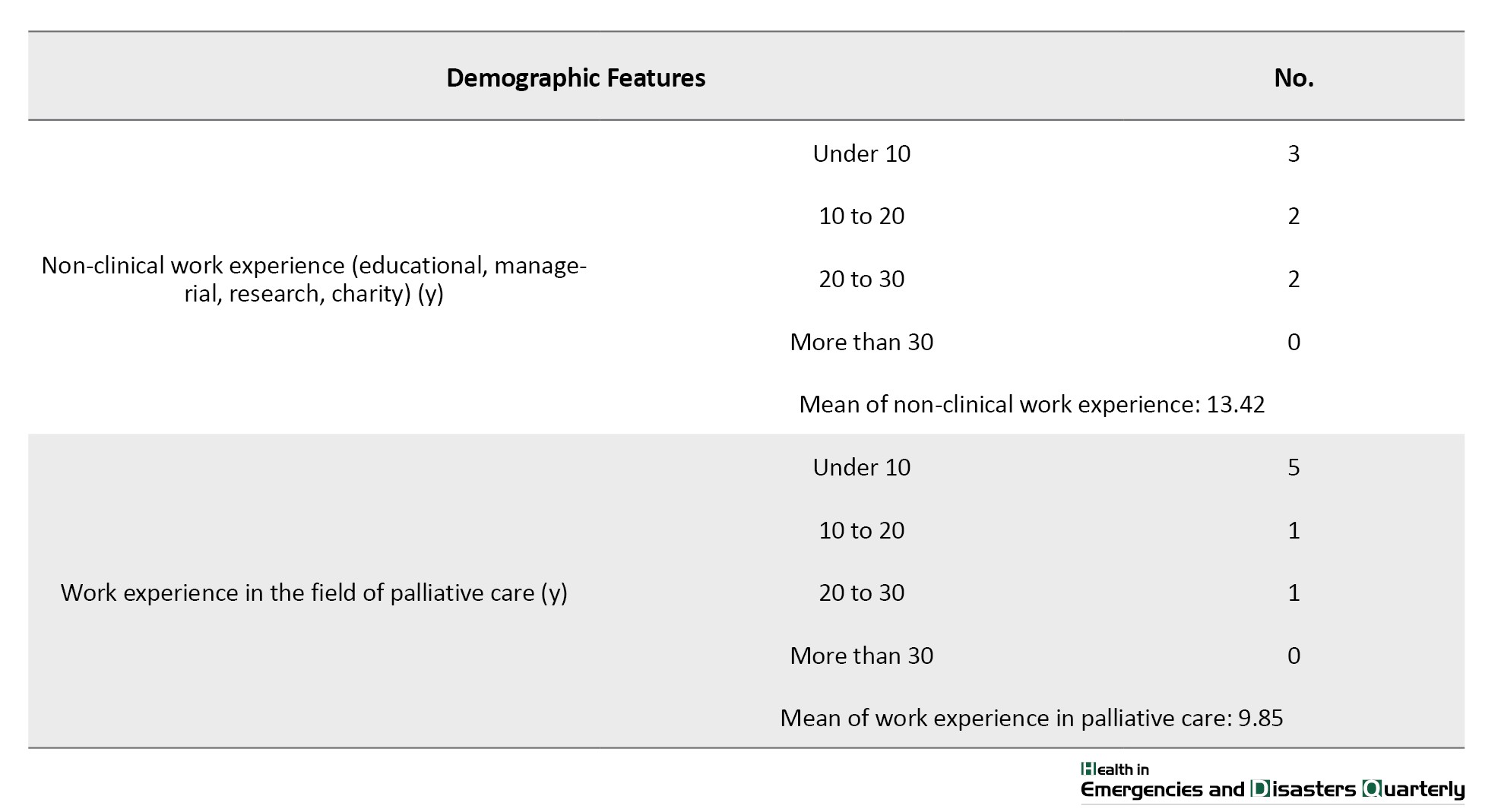
Table 2 provides a description of the characteristics of the expert panel members.
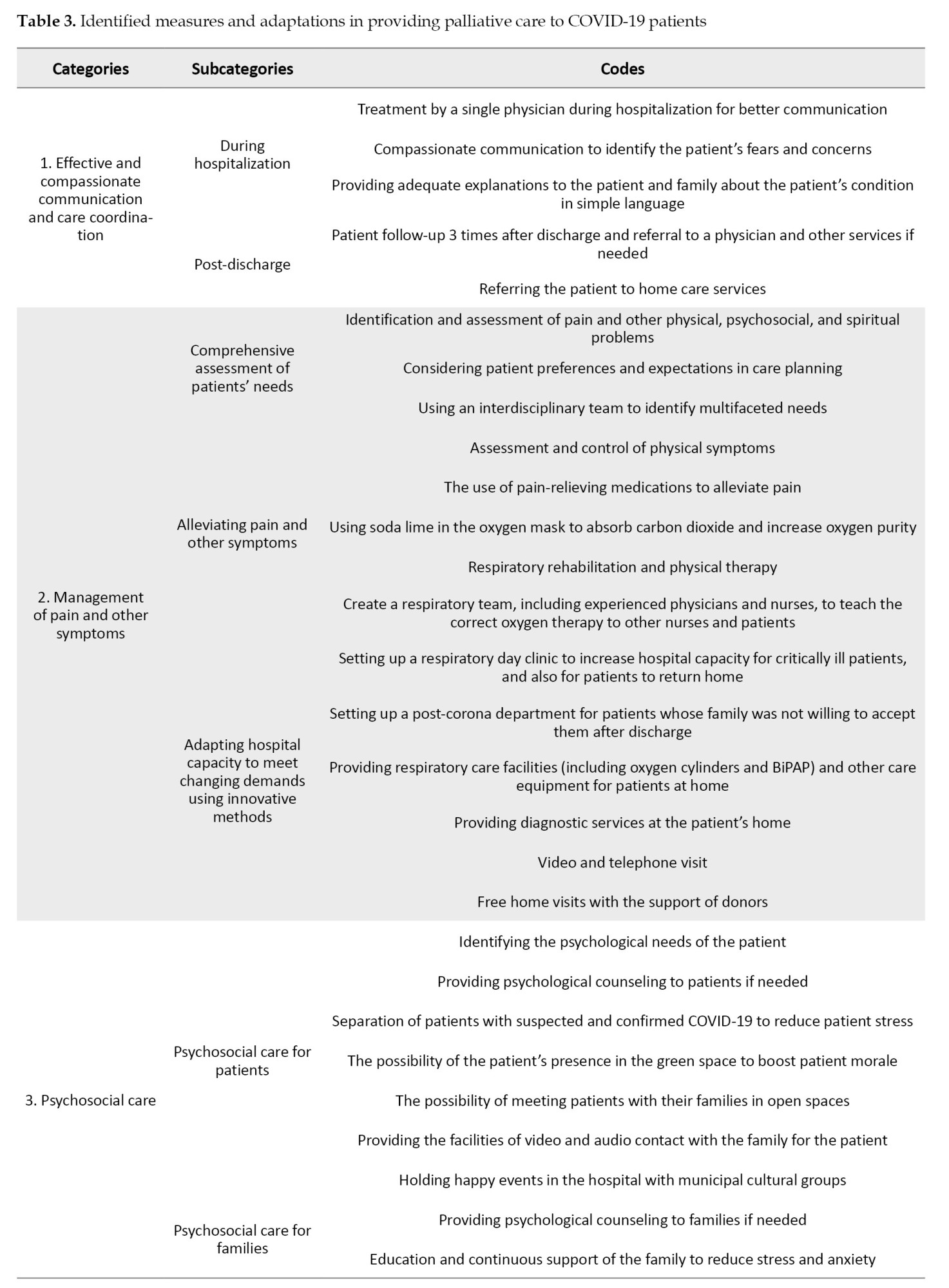
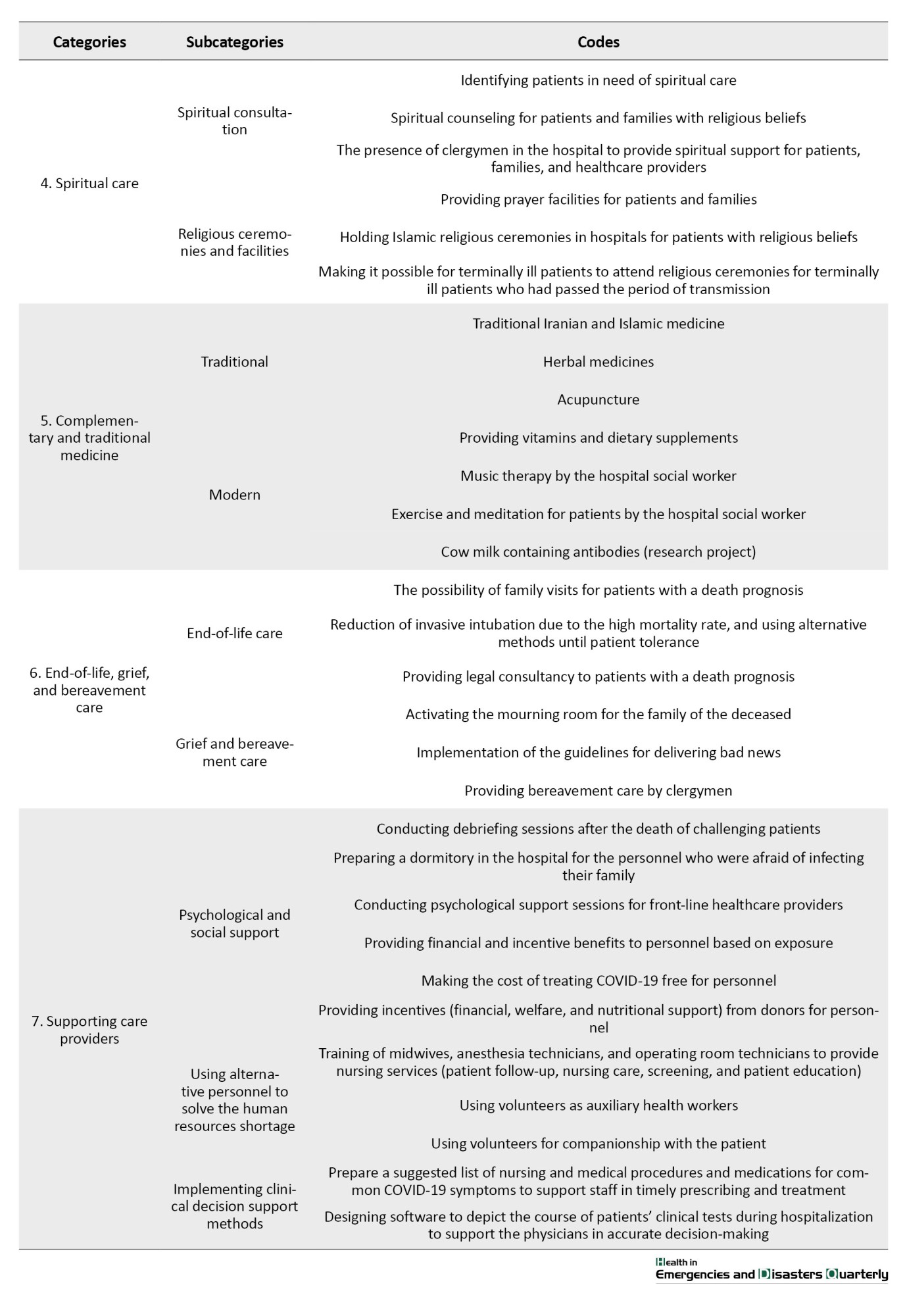
Following the integration of data from interviews and panel meetings, the adaptations made in palliative care for patients with COVID-19 were classified into seven principal categories, 16 subcategories, and 57 codes (Table 3).
The following section presents quotations pertaining to each concept.
Concept 1: Effective and compassionate communication and care coordination
The participants placed particular emphasis on the importance of two-way communication between healthcare providers and patients during the course of a patient’s hospitalization and subsequent discharge, especially while they were receiving healthcare services.
“We attempted to interact with patients in a compassionate manner, thereby enabling them to express their concerns and fears, allowing us to address their needs to the best of our abilities” (Participant No. 6 [P.6]).
“Even after discharge, we continued to monitor the patient and contacted them on three occasions at varying intervals” (P.3).
Concept 2: Management of pain and other symptoms
The participants indicated that the identification of pain and symptoms represents a pivotal aspect of palliative care for patients diagnosed with COVID-19. Furthermore, another significant challenge was adapting hospital capacity to accommodate surges in demand through the utilization of innovative methodologies. The heavy workloads undertaken by healthcare providers, coupled with the excessive admission of patients beyond capacity, made it challenging to identify and effectively manage pain and other symptoms.
“One of the initial objectives for the respiratory day clinic was to maintain the capacity of inpatient beds for critically ill patients who require 24/7 symptom control and to enhance the quality of services provided” (P.5).
“For a significant proportion of patients, symptoms, such as fever, pain, and even respiratory problems, could be effectively managed and controlled in a home setting” (P.12).
Concept 3: Psychosocial care
In the context of psychosocial care, the primary objective was to identify and address the psychosocial needs of patients’ families while simultaneously prioritizing the preservation of patients’ mental health.
“When communicating with family members, it is essential to assess their emotional and social well-being. It is crucial to promote peace and stability within the family unit, emphasizing that their calmness can positively impact the patient’s condition. There is a direct relationship between the two” (P.11).
“One of the most prevalent concerns among patients was the result of their PCR test after hospital admission. The issue was addressed by differentiating between those who tested definitively positive and those who were merely suspected to be infected” (P.8).
Psychological counseling was provided, and psychologists attended to the patients’ families in person or via video connection, engaging in discussions with family members due to the unavailability of visitation hours (P.6).
Concept 4: Spiritual care
In all hospitals where the investigation was conducted, patients with a confirmed diagnosis of COVID-19 infection and their families were provided with spiritual care services and facilities. Some participants highlighted the significance of offering spiritual care to patients with religious beliefs.
“From the outset of the pandemic, religious leaders have been present in hospitals, conducting spiritual consultations for patients and their families” (P.1).
Concept 5: Complementary and traditional medicine
Participants reported that both traditional and modern forms of complementary medicine were available in hospitals. Nevertheless, all cases were treated in accordance with the physicians’ consent and their opinion regarding the safety of the proposed procedures.
“Some patients expressed a desire to utilize herbal medicines and supplements, which would be approved if the attending physician concurred” (P.7).
“The social worker of the hospital visited all the departments and played music for the patients to elevate their spirits” (P.17).
Concept 6: End-of-life, grief, and bereavement care
In light of the considerable number of fatalities among those infected with COVID-19, the provision of end-of-life, grief, and bereavement care in hospitals has been identified as a priority area for health authorities. However, the provision of sporadic grief and bereavement care services was identified as a shortcoming among the participants, with some centers also lacking experience in this field.
“The bereavement room was managed by our institution. In some instances, bereaved families were provided with grief counseling services” (P.10).
“Guidelines for the delivery of difficult news were in place, which were revised during the period of the COVID-19 pandemic” (P.11).
Concept 7: Supporting care providers
Those working in the healthcare sector frequently encounter experiences of loss, suffering, and burnout. Thus, healthcare professionals require adequate support to deliver the necessary, well-qualified, patient-centered services that can meet the physical, social, emotional, and spiritual needs of their patients.
“We entered into a contractual agreement. Classes were conducted in this field for the personnel, and psychologists endeavored to provide them with the required assistance, and the outcomes were satisfactory” (P.1).
“We provided training to midwifery, anesthesia, and operating room personnel and enlisted them to perform a series of nursing services, which resulted in a reduction of the burden on the nurses” (P.4).
Discussion
This study delineates the principal measures and adaptations implemented in the provision of palliative care during the COVID-19 pandemic in Iran, as perceived by healthcare professionals. The study identified seven primary categories, which were further subdivided into 16 subcategories and 57 codes. The primary categories encompassed effective communication, pain and symptom management, psychosocial care, spiritual care, complementary and traditional medicine, end-of-life care, and support for care providers. In the following section, we will discuss how each function of providing palliative care can be both effective and necessary in comparison to other findings.
Regarding the first category, compassionate communication between caregivers and patients should be institutionalized within the healthcare system during hospitalization and post-discharge. The COVID-19 pandemic introduced distinct communication challenges, including the absence of family members, time constraints, staff burnout, and the necessity of personal protective equipment (PPE) [16]. Technological interventions, workforce training, telehealth or video conferencing, digital literacy, medical applications, and increases in virtual consultations are among the adaptive measures employed to address these barriers [17, 18]. Our study highlighted that healthcare providers engaged in direct conversations with patients and their families rather than overly relying on communication technologies.
In contrast to patients with advanced chronic illnesses, those diagnosed with COVID-19 may exhibit symptoms, yet the outcomes of recovery or mortality may remain uncertain. Consequently, healthcare professionals may have been hesitant to actively address pain and symptoms due to concerns about potentially hindering the patient’s chances of recovery [12]. This hesitance occasionally led to patients experiencing unnecessary pain and discomfort. Based on our experiences, utilizing an interdisciplinary team to identify multifaceted needs, considering patient preferences and expectations, and administering adequate pain relief medications were essential. The establishment of supportive structures, such as a respiratory day clinic and post-COVID department to alleviate symptoms, along with the provision of respiratory care facilities and complimentary home visits, was also crucial. Inokuchi et al. conducted a review that highlighted barriers to participation due to limited resources, personnel, and a lack of coordination among hospitals, facilities, outpatient clinics, and home visits [19]. Focusing on the third category, psychological care should be provided for infected patients and their families. The psychological impact of COVID-19 on patients has been significant, with reports of increased stress, anxiety, depression, and frustration [20]. Rao, et al. [21] indicated that the inability to fulfill the psychosocial needs of families resulted in feelings of guilt and distress among caregivers. Consequently, we explored alternative approaches, such as organizing joyful gatherings in outdoor spaces aimed at enhancing patients’ psychological well-being, while prioritizing psychological counseling when deemed necessary.
Spiritual care represents an additional function of palliative care that should be addressed through religious consultation and ceremonies. However, it is important to recognize that each context has a specific religious background, which is a key factor in determining responsibilities and management of religious activities [12]. Spiritual care has long been acknowledged as one of the domains of quality palliative care. While the pandemic has highlighted significant weaknesses in various healthcare sectors, it has also emphasized the necessity of prioritizing spiritual care as a crucial component of holistic palliative care [22]. Walsman suggested that actively listening, acknowledging and validating reactions, employing empathic communication, and paying attention to dignity can help mitigate spiritual distress [23]. Consequently, spiritual volunteers were enlisted, religious counseling was incorporated, and religious ceremonies were organized for patients who expressed interest.
Another important concept pertains to complementary and traditional medicine for COVID-19 patients, which encompasses a range of both conventional and modern practices. During the COVID-19 pandemic, traditional and complementary interventions were widely accepted and utilized with comparatively high frequency [24, 25]. Karataş emphasized the need for improved education regarding complementary and traditional medicine, enhanced physician-patient communication, and access to reliable information to facilitate appropriate use of these therapies [26]. Our experience indicates the utilization of traditional Iranian and Islamic medicine. Furthermore, Dehghan et al. reported that over 80% of the general population engaged with at least one form of complementary and alternative medicine (CAM) during the COVID-19 outbreak in Iran [25].
Eisma et al. demonstrated that among the many unforeseen consequences of the COVID-19 pandemic, societies are now grappling with an increasing number of bereaved individuals facing complicated grief in its aftermath [27]. Moreover, caregivers may experience prolonged grief, particularly when they perceive the dying process as a result of regrettable care decisions [28]. In our context, clergymen are often deemed more acceptable than healthcare providers in offering support; Holland et al. suggested that the responsibility could also be delegated to a family caregiver, who encourages the family to engage in meaningful activities, such as planting flowers or preparing a favorite meal, in memory of their loved one [29].
While it is acknowledged that healthcare providers are at a higher risk of infection, it remains unacceptable for them to suffer fatal consequences due to their occupation. In response, authorities have sought alternative approaches, including telemedicine, remote monitoring, self-monitoring for patients, and the use of robots and donors to supply materials to isolation wards [30]. It is important to note that not all countries possess adequate knowledge of telemedicine technologies; thus, employing alternative sources, such as volunteers from other disciplines, is recommended. Similarly, psychosocial support was addressed at both organizational and individual levels. Organizations provided caregivers with sufficient PPE, rest, clear communication and guidelines, and quick access to occupational health and safety teams. Additionally, accommodations for high-risk caregivers, support for children’s needs, regular assessments of caregivers’ mental well-being, and the establishment of frameworks to offer psychological first aid and specialized services were recommended [30, 31]. The establishment of a dormitory within the hospital for staff members concerned about the risk of infecting their loved ones was particularly well received.
Limitations: This study investigating the provision of palliative care during the COVID-19 pandemic has several limitations. First, the use of purposive and snowball sampling methods may restrict the diversity of perspectives, potentially leading to a biased understanding of care, as these methods primarily involve certain medical personnel. Second, the semi-structured interview format introduces the possibility of interviewer bias, which may affect the depth and quality of the data collected. Although data saturation was achieved with 17 interviews, this sample size may not adequately capture the experiences of all healthcare providers across different regions in Iran. To mitigate this issue, expert panel recommendations were employed.
Moreover, the study’s exclusive focus on medical personnel may overlook vital insights from other stakeholders, including patients, families, and non-medical staff, thereby limiting a comprehensive understanding of palliative care services. Overall, these limitations indicate that while the study offers valuable insights, further research is essential to acquire a broader perspective on palliative care provision in diverse contexts.
Conclusion
This study contributes to the existing body of knowledge by examining the adaptations made by healthcare professionals in the provision of palliative care during the COVID-19 pandemic. However, it is essential to assess the efficacy and necessity of these adaptations in comparison to alternative options.
It is imperative that palliative care be incorporated into epidemic guidelines for healthcare practices to ensure the continuity of care for patients in the event of future crises. This integration will ensure that the knowledge gained and modifications implemented during the pandemic are preserved and incorporated into future emergency preparedness plans, thereby enabling healthcare systems to provide comprehensive care that addresses the physical, psychological, social, and spiritual needs of patients and their families during public health emergencies.
In light of the above, this research documents the adaptations in palliative care during the COVID-19 pandemic in Iran and emphasizes the ongoing need for innovation, research, and policy development in this critical area of healthcare.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Isfahan University of Medical Sciences, Isfahan, Iran (Code: IR.MUI.NUREMA.REC.1401.117). The research was conducted in accordance with the ethical guidelines to ensure the protection of the participants’ privacy and confidentiality. The participants were assured that their information would be kept confidential.
Funding
This study was supported by Isfahan University of Medical Sciences, Isfahan, Iran (Grant No.: 2401155).
Authors' contributions
Conceptualization, methodology and data analysis: Asal Sadat Niaraees Zavare, Fatemeh Rezaei and Elham Moazam; Investigation, data collection and writing the original draft: Asal Sadat Niaraees Zavare, Elaheh Najafi Shahkoohi and Atefeh Najafi Shahkoohi;Supervision, review and editing: Fatemeh Rezaei and Karim Sohrabi; Funding administration: Fatemeh Rezaei.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to express their profound gratitude to all members of the hospital staff who participated in this project, as well as to all the members of the expert panel. The expertise, commitment, and valuable insights of these individuals were instrumental in shaping the research.
The World Health Organization (WHO) defines palliative care as an approach aimed at enhancing the quality of life for patients, both adults and children, and their families facing challenges associated with life-threatening illnesses [1]. The primary goal of palliative care is to mitigate and prevent suffering through the timely identification, precise evaluation, and treatment of pain and other related issues, encompassing physical, psychosocial, and spiritual aspects [2]. Ensuring access to palliative care is crucial for providing comprehensive and compassionate support to patients and families throughout the disease trajectory, spanning from diagnosis to death and bereavement, across all care settings [3].
The COVID-19 pandemic has subjected patients, their families, and caregivers to multifaceted suffering, including physical, psychological, social, and spiritual dimensions. Palliative care services address many of these concerns and pressures. The incorporation of palliative care into emergency management strategies has been emphasized in response to the spread of infectious diseases, like COVID-19 [4]. Research conducted in various countries following the onset of the COVID-19 pandemic underscores the vital role of palliative care in addressing patients’ complex needs during this challenging period and has revealed several adaptations implemented by healthcare providers [5-9]. These approaches include home- and community-based palliative care integrated with telehealth and innovative virtual hubs [10-12].
Extensive research has established the importance of cultural factors, spirituality, and religious coping mechanisms in the context of serious illnesses [13]. The implementation of palliative care is influenced by numerous cultural elements, such as family dynamics, elder care practices, physician roles, health-related decision-making processes, and the acceptance of life-threatening diagnoses [13, 14].
As one of the first countries to face the challenges posed by the COVID-19 pandemic, Iran’s healthcare professionals developed measures and adaptations to address the disease within the constraints of their resources and cultural and religious context, despite limited experience in palliative care [15]. Insights from global innovators in palliative care within resource-limited settings offer valuable perspectives for nations grappling with the COVID-19 emergency [12]. This study aimed to investigate the provision of palliative services during the COVID-19 pandemic within the Iranian healthcare system. Our findings will contribute to the development of a unified vision among various institutions, fostering collaborative efforts to attract multilateral support. Additionally, this research will inform policy decisions, disseminate critical knowledge, drive quality improvement initiatives, and advocate for the essential role of palliative care in preserving patient dignity and comfort during public health emergencies, such as COVID-19.
Materials and Methods
This study constituted a conductive content analysis conducted in two primary phases in 2022. A two-phased approach was implemented to obtain a comprehensive understanding of palliative care services provided during the COVID-19 pandemic. The semi-structured interviews facilitated a thorough examination of individual experiences and insights, while the expert panels enabled collective validation and expansion of these findings through collaborative discussion among palliative care professionals. Initially, purposive sampling was employed, subsequently augmented by snowball sampling, to achieve data saturation. A total of 17 individuals were selected to participate in this study through the application of purposive sampling.
Two trained researchers conducted semi-structured interviews with the participants. The interviews addressed several key questions, including: 1) Please describe the measures you have taken in the field of palliative care for patients with COVID-19; 2) Please describe the measures you have taken in each of the following areas: Physical, psychological, social and spiritual care; 3) Please describe the measures that have been taken to provide support to the patient’s family and relatives; 4) In the case of patients who have died, have measures been taken to provide support to their families in the period of bereavement?; 5) Please describe the new medicine or procedure that has been used to relieve pain and improve the quality of life of patients; and 6) In the context of palliative care for patients with COVID-19, which measures have you identified as the most significant and impactful? Please provide a rationale for your selection.
The participants were professionals with a minimum of five years of experience, employed in various positions in hospitals. They all possessed at least a bachelor’s degree and had diverse roles and responsibilities related to providing services to patients diagnosed with COVID-19. Following the completion of five interviews, an interview guide was developed to facilitate further questioning and analysis based on the data obtained. Upon completion of 17 interviews, it was determined that data saturation had been achieved. Subsequently, each code was either added as a new code or integrated into the predefined categories. The interviews were transcribed and subjected to thematic analysis utilizing MAXQDA 2018.1. The initial codes were identified from the data and subsequently refined into themes through both independent analysis and consensus meetings conducted among the research team.
The findings from the initial phase were utilized to inform the structure and focus of the expert panels, thereby ensuring that the discussions were predicated on previously identified themes from the interviews. Subsequently, three expert panels were convened, and key informants in the field of palliative care were invited to participate. To ensure the quality and relevance of the expert panel members, the inclusion criteria were as follows: 1) Relevant education and specialization- a formal degree in palliative care, nursing, medicine, social work, or a related field with a strong emphasis on palliative care principles; 2) Professional experience- a minimum of five years of professional experience in palliative care or educational settings; 3) Familiarity with the Iranian health system- adequate knowledge and understanding of the Iranian health system. Those who were unable to commit the requisite time and to work within a diverse expert panel were excluded from participation.
The participants of the expert panels were not among those whom we interviewed. A facilitator was responsible for initiating and directing the discussion, with the objective of eliciting recommendations regarding the reorganization of the initially developed categories. The panels were conducted in the presence of researchers and five experts in the field of palliative care. Following the identification of the primary sub-categories, categories, and concepts, through a review of the panels’ experts’ input, the findings were refined to exclude themes and verbal codes that were not within the scope of palliative care services.
The coding was conducted with two independent analysts adopting a constant comparative analysis approach and utilizing MAXQDA 2018.1 software. Specific categories were developed based on recurring themes, and a consensus was reached through a process of collective deliberation during the research team meetings. To ensure the consistency and accuracy of the coding process, weekly meetings were held to evaluate the inter-rater reliability of the codes and create categories by data analysts. In instances where discrepancies arose between analysts, a third party with expertise in qualitative research and a registered member of the palliative care association was consulted to provide a final decision. The Kappa coefficient score in these instances reached 98%.
Subsequently, the data were integrated to provide health systems and health authorities with comprehensive palliative care, thereby enhancing the quality of patient care and introducing a range of adaptable palliative care measures that could be selected based on the specific circumstances of each hospital.
Results
Table 1 presents a comprehensive overview of the 17 participants, including their job titles, educational qualifications, age, gender, and city of work.
Table 2 provides a description of the characteristics of the expert panel members.
Following the integration of data from interviews and panel meetings, the adaptations made in palliative care for patients with COVID-19 were classified into seven principal categories, 16 subcategories, and 57 codes (Table 3).
The following section presents quotations pertaining to each concept.
Concept 1: Effective and compassionate communication and care coordination
The participants placed particular emphasis on the importance of two-way communication between healthcare providers and patients during the course of a patient’s hospitalization and subsequent discharge, especially while they were receiving healthcare services.
“We attempted to interact with patients in a compassionate manner, thereby enabling them to express their concerns and fears, allowing us to address their needs to the best of our abilities” (Participant No. 6 [P.6]).
“Even after discharge, we continued to monitor the patient and contacted them on three occasions at varying intervals” (P.3).
Concept 2: Management of pain and other symptoms
The participants indicated that the identification of pain and symptoms represents a pivotal aspect of palliative care for patients diagnosed with COVID-19. Furthermore, another significant challenge was adapting hospital capacity to accommodate surges in demand through the utilization of innovative methodologies. The heavy workloads undertaken by healthcare providers, coupled with the excessive admission of patients beyond capacity, made it challenging to identify and effectively manage pain and other symptoms.
“One of the initial objectives for the respiratory day clinic was to maintain the capacity of inpatient beds for critically ill patients who require 24/7 symptom control and to enhance the quality of services provided” (P.5).
“For a significant proportion of patients, symptoms, such as fever, pain, and even respiratory problems, could be effectively managed and controlled in a home setting” (P.12).
Concept 3: Psychosocial care
In the context of psychosocial care, the primary objective was to identify and address the psychosocial needs of patients’ families while simultaneously prioritizing the preservation of patients’ mental health.
“When communicating with family members, it is essential to assess their emotional and social well-being. It is crucial to promote peace and stability within the family unit, emphasizing that their calmness can positively impact the patient’s condition. There is a direct relationship between the two” (P.11).
“One of the most prevalent concerns among patients was the result of their PCR test after hospital admission. The issue was addressed by differentiating between those who tested definitively positive and those who were merely suspected to be infected” (P.8).
Psychological counseling was provided, and psychologists attended to the patients’ families in person or via video connection, engaging in discussions with family members due to the unavailability of visitation hours (P.6).
Concept 4: Spiritual care
In all hospitals where the investigation was conducted, patients with a confirmed diagnosis of COVID-19 infection and their families were provided with spiritual care services and facilities. Some participants highlighted the significance of offering spiritual care to patients with religious beliefs.
“From the outset of the pandemic, religious leaders have been present in hospitals, conducting spiritual consultations for patients and their families” (P.1).
Concept 5: Complementary and traditional medicine
Participants reported that both traditional and modern forms of complementary medicine were available in hospitals. Nevertheless, all cases were treated in accordance with the physicians’ consent and their opinion regarding the safety of the proposed procedures.
“Some patients expressed a desire to utilize herbal medicines and supplements, which would be approved if the attending physician concurred” (P.7).
“The social worker of the hospital visited all the departments and played music for the patients to elevate their spirits” (P.17).
Concept 6: End-of-life, grief, and bereavement care
In light of the considerable number of fatalities among those infected with COVID-19, the provision of end-of-life, grief, and bereavement care in hospitals has been identified as a priority area for health authorities. However, the provision of sporadic grief and bereavement care services was identified as a shortcoming among the participants, with some centers also lacking experience in this field.
“The bereavement room was managed by our institution. In some instances, bereaved families were provided with grief counseling services” (P.10).
“Guidelines for the delivery of difficult news were in place, which were revised during the period of the COVID-19 pandemic” (P.11).
Concept 7: Supporting care providers
Those working in the healthcare sector frequently encounter experiences of loss, suffering, and burnout. Thus, healthcare professionals require adequate support to deliver the necessary, well-qualified, patient-centered services that can meet the physical, social, emotional, and spiritual needs of their patients.
“We entered into a contractual agreement. Classes were conducted in this field for the personnel, and psychologists endeavored to provide them with the required assistance, and the outcomes were satisfactory” (P.1).
“We provided training to midwifery, anesthesia, and operating room personnel and enlisted them to perform a series of nursing services, which resulted in a reduction of the burden on the nurses” (P.4).
Discussion
This study delineates the principal measures and adaptations implemented in the provision of palliative care during the COVID-19 pandemic in Iran, as perceived by healthcare professionals. The study identified seven primary categories, which were further subdivided into 16 subcategories and 57 codes. The primary categories encompassed effective communication, pain and symptom management, psychosocial care, spiritual care, complementary and traditional medicine, end-of-life care, and support for care providers. In the following section, we will discuss how each function of providing palliative care can be both effective and necessary in comparison to other findings.
Regarding the first category, compassionate communication between caregivers and patients should be institutionalized within the healthcare system during hospitalization and post-discharge. The COVID-19 pandemic introduced distinct communication challenges, including the absence of family members, time constraints, staff burnout, and the necessity of personal protective equipment (PPE) [16]. Technological interventions, workforce training, telehealth or video conferencing, digital literacy, medical applications, and increases in virtual consultations are among the adaptive measures employed to address these barriers [17, 18]. Our study highlighted that healthcare providers engaged in direct conversations with patients and their families rather than overly relying on communication technologies.
In contrast to patients with advanced chronic illnesses, those diagnosed with COVID-19 may exhibit symptoms, yet the outcomes of recovery or mortality may remain uncertain. Consequently, healthcare professionals may have been hesitant to actively address pain and symptoms due to concerns about potentially hindering the patient’s chances of recovery [12]. This hesitance occasionally led to patients experiencing unnecessary pain and discomfort. Based on our experiences, utilizing an interdisciplinary team to identify multifaceted needs, considering patient preferences and expectations, and administering adequate pain relief medications were essential. The establishment of supportive structures, such as a respiratory day clinic and post-COVID department to alleviate symptoms, along with the provision of respiratory care facilities and complimentary home visits, was also crucial. Inokuchi et al. conducted a review that highlighted barriers to participation due to limited resources, personnel, and a lack of coordination among hospitals, facilities, outpatient clinics, and home visits [19]. Focusing on the third category, psychological care should be provided for infected patients and their families. The psychological impact of COVID-19 on patients has been significant, with reports of increased stress, anxiety, depression, and frustration [20]. Rao, et al. [21] indicated that the inability to fulfill the psychosocial needs of families resulted in feelings of guilt and distress among caregivers. Consequently, we explored alternative approaches, such as organizing joyful gatherings in outdoor spaces aimed at enhancing patients’ psychological well-being, while prioritizing psychological counseling when deemed necessary.
Spiritual care represents an additional function of palliative care that should be addressed through religious consultation and ceremonies. However, it is important to recognize that each context has a specific religious background, which is a key factor in determining responsibilities and management of religious activities [12]. Spiritual care has long been acknowledged as one of the domains of quality palliative care. While the pandemic has highlighted significant weaknesses in various healthcare sectors, it has also emphasized the necessity of prioritizing spiritual care as a crucial component of holistic palliative care [22]. Walsman suggested that actively listening, acknowledging and validating reactions, employing empathic communication, and paying attention to dignity can help mitigate spiritual distress [23]. Consequently, spiritual volunteers were enlisted, religious counseling was incorporated, and religious ceremonies were organized for patients who expressed interest.
Another important concept pertains to complementary and traditional medicine for COVID-19 patients, which encompasses a range of both conventional and modern practices. During the COVID-19 pandemic, traditional and complementary interventions were widely accepted and utilized with comparatively high frequency [24, 25]. Karataş emphasized the need for improved education regarding complementary and traditional medicine, enhanced physician-patient communication, and access to reliable information to facilitate appropriate use of these therapies [26]. Our experience indicates the utilization of traditional Iranian and Islamic medicine. Furthermore, Dehghan et al. reported that over 80% of the general population engaged with at least one form of complementary and alternative medicine (CAM) during the COVID-19 outbreak in Iran [25].
Eisma et al. demonstrated that among the many unforeseen consequences of the COVID-19 pandemic, societies are now grappling with an increasing number of bereaved individuals facing complicated grief in its aftermath [27]. Moreover, caregivers may experience prolonged grief, particularly when they perceive the dying process as a result of regrettable care decisions [28]. In our context, clergymen are often deemed more acceptable than healthcare providers in offering support; Holland et al. suggested that the responsibility could also be delegated to a family caregiver, who encourages the family to engage in meaningful activities, such as planting flowers or preparing a favorite meal, in memory of their loved one [29].
While it is acknowledged that healthcare providers are at a higher risk of infection, it remains unacceptable for them to suffer fatal consequences due to their occupation. In response, authorities have sought alternative approaches, including telemedicine, remote monitoring, self-monitoring for patients, and the use of robots and donors to supply materials to isolation wards [30]. It is important to note that not all countries possess adequate knowledge of telemedicine technologies; thus, employing alternative sources, such as volunteers from other disciplines, is recommended. Similarly, psychosocial support was addressed at both organizational and individual levels. Organizations provided caregivers with sufficient PPE, rest, clear communication and guidelines, and quick access to occupational health and safety teams. Additionally, accommodations for high-risk caregivers, support for children’s needs, regular assessments of caregivers’ mental well-being, and the establishment of frameworks to offer psychological first aid and specialized services were recommended [30, 31]. The establishment of a dormitory within the hospital for staff members concerned about the risk of infecting their loved ones was particularly well received.
Limitations: This study investigating the provision of palliative care during the COVID-19 pandemic has several limitations. First, the use of purposive and snowball sampling methods may restrict the diversity of perspectives, potentially leading to a biased understanding of care, as these methods primarily involve certain medical personnel. Second, the semi-structured interview format introduces the possibility of interviewer bias, which may affect the depth and quality of the data collected. Although data saturation was achieved with 17 interviews, this sample size may not adequately capture the experiences of all healthcare providers across different regions in Iran. To mitigate this issue, expert panel recommendations were employed.
Moreover, the study’s exclusive focus on medical personnel may overlook vital insights from other stakeholders, including patients, families, and non-medical staff, thereby limiting a comprehensive understanding of palliative care services. Overall, these limitations indicate that while the study offers valuable insights, further research is essential to acquire a broader perspective on palliative care provision in diverse contexts.
Conclusion
This study contributes to the existing body of knowledge by examining the adaptations made by healthcare professionals in the provision of palliative care during the COVID-19 pandemic. However, it is essential to assess the efficacy and necessity of these adaptations in comparison to alternative options.
It is imperative that palliative care be incorporated into epidemic guidelines for healthcare practices to ensure the continuity of care for patients in the event of future crises. This integration will ensure that the knowledge gained and modifications implemented during the pandemic are preserved and incorporated into future emergency preparedness plans, thereby enabling healthcare systems to provide comprehensive care that addresses the physical, psychological, social, and spiritual needs of patients and their families during public health emergencies.
In light of the above, this research documents the adaptations in palliative care during the COVID-19 pandemic in Iran and emphasizes the ongoing need for innovation, research, and policy development in this critical area of healthcare.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Isfahan University of Medical Sciences, Isfahan, Iran (Code: IR.MUI.NUREMA.REC.1401.117). The research was conducted in accordance with the ethical guidelines to ensure the protection of the participants’ privacy and confidentiality. The participants were assured that their information would be kept confidential.
Funding
This study was supported by Isfahan University of Medical Sciences, Isfahan, Iran (Grant No.: 2401155).
Authors' contributions
Conceptualization, methodology and data analysis: Asal Sadat Niaraees Zavare, Fatemeh Rezaei and Elham Moazam; Investigation, data collection and writing the original draft: Asal Sadat Niaraees Zavare, Elaheh Najafi Shahkoohi and Atefeh Najafi Shahkoohi;Supervision, review and editing: Fatemeh Rezaei and Karim Sohrabi; Funding administration: Fatemeh Rezaei.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to express their profound gratitude to all members of the hospital staff who participated in this project, as well as to all the members of the expert panel. The expertise, commitment, and valuable insights of these individuals were instrumental in shaping the research.
References
- Faull C. The context and principles of palliative care. In: Kitchen R, Faull Ch, Russell S, Wilson J, editors. Handbook of palliative care. New Jersey: John Wiley & Sons Ltd; 2024. [Link]
- Dzierżanowski T. Definitions of palliative care-narrative review and new proposal. Medycyna Paliatywna/Palliative Medicine. 2021; 13(4):187-200. [DOI:10.5114/pm.2021.114495]
- Wantonoro W, Suryaningsih EK, Anita DC, Nguyen TV. Palliative Care: A concept analysis review. SAGE Open Nursing. 2022; 8:23779608221117379. [DOI:10.1177/23779608221117379] [PMID]
- Fadul N, Elsayem AF, Bruera E. Integration of palliative care into COVID-19 pandemic planning. BMJ Supportive & Palliative Care. 2021; (1):40-4. [DOI:10.1136/bmjspcare-2020-002364] [PMID]
- Aaronson EL, Petrillo L, Stoltenberg M, Jacobsen J, Wilson E, Bowman J, et al. The experience of emergency department providers with embedded palliative care during COVID. Journal of Pain and Symptom Management. 2020; 60(5):e35-43. [DOI:10.1016/j.jpainsymman.2020.08.007] [PMID]
- Dunleavy L, Preston N, Bajwah S, Bradshaw A, Cripps R, Fraser LK, et al. 'Necessity is the mother of invention': Specialist palliative care service innovation and practice change in response to COVID-19. Results from a multinational survey (CovPall). Palliative Medicine. 2021; 35(5):814-29. [DOI:10.1177/02692163211000660] [PMID]
- Heath L, Yates S, Carey M, Miller M. Palliative care during COVID-19: Data and visits from loved ones. The American Journal of Hospice & Palliative Care. 2020; 37(11):988-91. [DOI:10.1177/1049909120943577] [PMID]
- Hetherington L, Johnston B, Kotronoulas G, Finlay F, Keeley P, McKeown A. COVID-19 and hospital palliative care - a service evaluation exploring the symptoms and outcomes of 186 patients and the impact of the pandemic on specialist hospital palliative care. Palliative Medicine. 2020; 34(9):1256-62. [DOI:10.1177/0269216320949786] [PMID]
- Lopez S, Finuf KD, Marziliano A, Sinvani L, Burns EA. Palliative care consultation in hospitalized patients with COVID-19: A retrospective study of characteristics, outcomes, and unmet needs. Journal of Pain and Symptom Management. 2021; 62(2):267-76. [DOI:10.1016/j.jpainsymman.2020.12.015] [PMID]
- Mojtahedi Z, Shen JJ. Home palliative care during the covid-19 pandemic: A scoping review. The American Journal of Hospice & Palliative Care. 2023; 40(2):216-24. [DOI:10.1177/10499091221093314] [PMID]
- Eastman P, Dowd A, White J, Carter J, Ely M. Telehealth: Rapid adoption in community palliative care due to COVID-19: Patient and professional evaluation. BMJ Supportive & Palliative Care. 2021; 14(1):438-42. [DOI:10.1136/bmjspcare-2021-002987] [PMID]
- Knights D, Knights F, Lawrie I. Upside down solutions: Palliative care and COVID-19. BMJ Supportive & Palliative Care. 2024; 14(e1):e583-e7. [DOI:10.1136/bmjspcare-2020-002385] [PMID]
- Laabar TD, Saunders C, Auret K, Johnson CE. Socially, culturally and spiritually sensitive public health palliative care models in the lower-income countries: An integrative literature review. Indian Journal of Palliative Care. 2023; 29(1):15. [DOI:10.25259/IJPC_92_2022] [PMID]
- Mathew-Geevarughese SE, Corzo O, Figuracion E. Cultural, religious, and spiritual issues in palliative care. Primary Care. 2019; 46(3):399-413. [DOI:10.1016/j.pop.2019.05.006] [PMID]
- Ahmadi S, Irandoost SF, Ahmadi A, Yoosefi Lebni J, Mohammadi Gharehghani MA, Baba Safari N. Explaining experiences, challenges and adaptation strategies in COVID-19 Patients: A qualitative study in Iran. Frontiers in Public Health. 2022; 9:778026. [DOI:10.3389/fpubh.2021.778026] [PMID]
- Wittenberg E, Goldsmith JV, Chen C, Prince-Paul M, Johnson RR. Opportunities to improve COVID-19 provider communication resources: A systematic review. Patient Education and Counseling. 2021; 104(3):438-51. [DOI:10.1016/j.pec.2020.12.031] [PMID]
- Xu X, Ho MH, Lin CC. Telehealth in palliative care during the COVID-19 pandemic: A systematic mixed studies review. Worldviews on Evidence-Based Nursing. 2023; 20(5):476-91. [DOI:10.1111/wvn.12637] [PMID]
- Patra M, Hamiduzzaman M, McLaren H, Siddiquee NA. A scoping review of changes to patient-doctor communication during COVID-19. Health Communication. 2024; 39(1):25-48. [DOI:10.1080/10410236.2022.2152225] [PMID]
- Inokuchi R, Hanari K, Shimada K, Iwagami M, Sakamoto A, Sun Y, et al. Barriers to and facilitators of advance care planning implementation for medical staff after the COVID-19 pandemic: An overview of reviews. BMJ Open. 2023; 13(10):e075969. [DOI:10.1136/bmjopen-2023-075969] [PMID]
- Diana L, Regazzoni R, Sozzi M, Piconi S, Borghesi L, Lazzaroni E, et al. Monitoring cognitive and psychological alterations in COVID-19 patients: A longitudinal neuropsychological study. Journal of The Neurological Sciences. 2023; 444:120511. [DOI:10.1016/j.jns.2022.120511] [PMID]
- Rao SR, Spruijt O, Sunder P, Daniel S, Chittazhathu RK, Nair S, et al. Psychosocial aspects of COVID-19 in the context of palliative care - A quick review. Indian Journal of Palliative Care. 2020; 26(Suppl 1):S116-20. [DOI:10.4103/IJPC.IJPC_183_20] [PMID]
- Ferrell BR, Handzo G, Picchi T, Puchalski C, Rosa WE. The urgency of spiritual care: COVID-19 and the critical need for whole-person palliation. Journal of Pain and Symptom Management. 2020; 60(3):e7-11. [DOI:10.1016/j.jpainsymman.2020.06.034] [PMID]
- Waldman E, Glass M. A field manual for palliative care in humanitarian crises. Oxford: Oxford University Press; 2019. [DOI:10.1093/med/9780190066529.001.0001]
- Kim TH, Kang JW, Jeon SR, Ang L, Lee HW, Lee MS. Use of traditional, complementary and integrative medicine during the covid-19 pandemic: A systematic review and meta-analysis. Frontiers in Medicine. 2022; 9:884573. [DOI:10.3389/fmed.2022.884573] [PMID]
- Dehghan M, Ghanbari A, Ghaedi Heidari F, Mangolian Shahrbabaki P, Zakeri MA. Use of complementary and alternative medicine in general population during COVID-19 outbreak: A survey in Iran. Journal of Integrative Medicine. 2022; 20(1):45-51. [DOI:10.1016/j.joim.2021.11.004] [PMID]
- Karataş Y, Khan Z, Bilen Ç, Boz A, Özagil ESG, Abussuutoğlu AB, et al. Traditional and complementary medicine use and beliefs during COVID-19 outbreak: A cross-sectional survey among the general population in Turkey. Advances in Integrative Medicine. 2021; 8(4):261-6. [DOI:10.1016/j.aimed.2021.09.002] [PMID]
- Eisma MC, Boelen PA, Lenferink LIM. Prolonged grief disorder following the coronavirus (COVID-19) pandemic. Psychiatry Research. 2020; 288:113031. [DOI:10.1016/j.psychres.2020.113031] [PMID]
- Supiano KP, Luptak M, Andersen T, Beynon C, Iacob E, Wong B. If we knew then what we know now: The preparedness experience of pre-loss and post-loss dementia caregivers. Death Studies. 2022; 46(2):369-80. [DOI:10.1080/07481187.2020.1731014] [PMID]
- Holland DE, Vanderboom CE, Dose AM, Moore D, Robinson KV, Wild E, et al. Death and grieving for family caregivers of loved ones with life-limiting illnesses in the era of COVID-19: Considerations for case managers. Professional Case Management. 2021; 26(2):53-61. [DOI:10.1097/NCM.0000000000000485] [PMID]
- Willis KD, Rao SR, Normen M, de Groot J, Calman L, Bahcivan O, et al. Same storm, different boat: The global impact of COVID-19 on palliative care. Psychooncology. 2023; 32(1):148-54. [DOI:10.1002/pon.5995] [PMID]
- Spoorthy MS, Pratapa SK, Mahant S. Mental health problems faced by healthcare workers due to the COVID-19 pandemic-A review. Asian Journal of Psychiatry. 2020; 51:102119. [DOI:10.1016/j.ajp.2020.102119] [PMID]
Type of article: Research |
Subject:
Qualitative
Received: 2024/02/23 | Accepted: 2025/02/15 | Published: 2025/10/1
Received: 2024/02/23 | Accepted: 2025/02/15 | Published: 2025/10/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
