

Volume 10, Issue 3 (Spring 2025)
Health in Emergencies and Disasters Quarterly 2025, 10(3): 167-176 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Vafaeenasab M, Sadat S J, Afrasiabifar A, Khorasani-Zavareh D, Khodayarian M. Exploring Barriers of Prehospital Logistics Support in Traffic Accidents With Mass Casualties: A Qualitative Research. Health in Emergencies and Disasters Quarterly 2025; 10 (3) :167-176
URL: http://hdq.uswr.ac.ir/article-1-615-en.html
URL: http://hdq.uswr.ac.ir/article-1-615-en.html
Mohammadreza Vafaeenasab1 

 , Seyed Javad Sadat *2 , Ardashir Afrasiabifar3 , Davoud Khorasani-Zavareh4 , Mahsa Khodayarian5
, Seyed Javad Sadat *2 , Ardashir Afrasiabifar3 , Davoud Khorasani-Zavareh4 , Mahsa Khodayarian5
, Seyed Javad Sadat *2 , Ardashir Afrasiabifar3 , Davoud Khorasani-Zavareh4 , Mahsa Khodayarian5
1- Yazd Accident Prevention and Crisis Research Center, Shahid Sadoughi University of Medical Sciences, Yazd, Iran., Shahid Sadoughi university of Medical Sciences, Yazd, lran
2- Department of Medical Surgical Nursing, School of Nursing, Yasuj University of Medical Sciences, Yasuj, Iran. & Department of Health in Emergencies and Disasters, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. ,sadatsaiedjavad@gmail.com
3- Department of Medical Surgical Nursing, School of Nursing, Yasuj University of Medical Sciences, Yasuj, Iran.
4- Safety Promotion and Injury Prevention Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran. & Department of Health in Emergencies and Disasters, School of Public Health and Safety, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
5- Department of Health Education, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
2- Department of Medical Surgical Nursing, School of Nursing, Yasuj University of Medical Sciences, Yasuj, Iran. & Department of Health in Emergencies and Disasters, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. ,
3- Department of Medical Surgical Nursing, School of Nursing, Yasuj University of Medical Sciences, Yasuj, Iran.
4- Safety Promotion and Injury Prevention Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran. & Department of Health in Emergencies and Disasters, School of Public Health and Safety, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
5- Department of Health Education, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Keywords: Prehospital, Logistics, Traffic accidents, Mass casualty incident (MCI), Emergency medical services (EMS)
Full-Text [PDF 510 kb]
(837 Downloads)
| Abstract (HTML) (3672 Views)
Full-Text: (440 Views)
Introduction
Mass casualty incidents (MCIs) can be caused by various factors, including mass gatherings; armed conflicts; terrorism; biological, geophysical, meteorological, disasters; and traffic accidents [1]. According to the World Health Organization (WHO), accidents with mass casualties are accidents in which the casualties cannot be managed with the current facilities and resources and the usual operational processes of organizations [2]. Traffic accidents are the ninth leading cause of death worldwide, resulting in 1.35 million deaths and 50 million injuries annually [3]. In Iran, road traffic deaths dropped from 32.1 to 20.5 per 100000 people between 2015 and 2018. In 2015, Iran ranked eighth globally in traffic accident fatalities. By 2018, its ranking had dropped to 53rd [4]. The results of a study by Razzak et al. showed that post-crash care could lead to a reduction in trauma mortality of up to 35% [5]. This care depends on the cooperation and support of other relief organizations, such as the Red Cross, the Police, and the Fire Department, in providing resources and logistics [6].
Logistics is the process of mobilizing resources, skills, and knowledge to help disaster victims [7]. Emergency logistics aims to achieve maximum efficiency in a short time and minimize MCI losses [8]. MCI may severely damage large geographic areas and populations. Therefore, logistics operations in emergency incidents have complex dimensions, including damage assessment, estimation of needs, allocation of different resources in a short period, organization of rescue operations, and evacuation of the injured [9]. Dealing with uncertainty, unpredictability, unexpected consequences of accidents with mass casualties, unconfirmed information, and lack of information, sometimes contradictory, blurs the exact nature of the accident and makes decisions more difficult [10]. The Furbee report found that 38% of emergency service organizations are confused about providing answers and allocating appropriate resources [11]. Active cooperation inside and outside relief organizations in logistics is the most important part of disaster management with mass injuries, but insufficient infrastructure, lack of cooperation, and inadequate communication among relief organizations can lead to problems in logistics activities [12].
As the most important part of the Iranian Medical Emergency and Accident Management Center, the prehospital emergency system provides vital medical services at the scene of accidents with mass injuries [13]. The report by Obermeyer et al. highlights the lack of logistics resources and the lack of specialized training provided to emergency care service providers in low- and middle-income countries [14]. Despite multiple MCIs worldwide, there is a limited number of academic studies in logistics. Logistics support is a crucial field of research that needs the attention and support of people, organizations, and the government. The government has the opportunity to increase its share in MCI by improving the areas of knowledge management, technology, and measurement [7]. Modeling and simulation are the most commonly used method in the studies [14, 15]. Qualitative research on logistics in Iran has rarely been done. Therefore, to understand the experience of the personnel of relief organizations involved in accidents with mass casualties and logistics support in Iran, this study was conducted to explore barriers to prehospital logistics support in traffic accidents with mass casualties.
Materials and Methods
The present qualitative study was conducted using conventional content analysis.
Study participants and data collection
This study was conducted with the participation of employees of relief organizations, including emergency medical technicians, police forces, and Red Crescent staff in Yazd, Fars, Kohgiluyeh and Boyer-Ahmad, and Qom provinces, Iran from June 2018 to September 2019. Participants were recruited from the prehospital emergency system, the Red Crescent, the Police, and the transportation department. The first participant was selected using a purposive sampling method. The other participants entered the qualitative interview process by snowball method, which included 28 men and 3 women: Emergency technicians (9 participants), emergency medicine experts (5 participants), head of Emergency Operations Center (3 participants), dispatch operator (3 participants), head of Medical Emergency and Accident Management Center (3 participants), the Police (3 participants), Red Crescent Relief (2 participants), Deputy Red Crescent Rescue (1 participant), emergency medicine specialist (1 participant) and head of Road Transport Organization (1 participant). The number of female participants is low because Iran’s prehospital emergency personnel and other relief organizations are only men, and women only work as operators at the Dispatch Center. The inclusion criteria were the willingness to conduct interviews, the ability to express experiences, and having at least 2 years of work experience. The unwillingness to continue the interview and not answering the questions were considered criteria for exclusion. The first four interviews were conducted utilizing unstructured in-depth interviews followed by 27 semi-structured interviews. Each interview began with a general question: “Describe your experiences with the MCI in which you participated?” This question was asked of employees of relief organizations. The prehospital emergency personnel were asked: “What factors contributed to prehospital logistics support in the MCI you were involved in.” Probing questions such as “What do you mean?” “Please explain further” and “give an example of your objective in your experience” are used to clarify information and collect additional data. During the interviews, deterrents and facilitators of prehospital logistics support with exploratory questions were explored. This process continued until data saturation was reached. The duration of the interviews varied between 25 and 100 minutes. There was a relationship between the time of the interviews and the expertise of the interviewees. So, the head of the Transportation Department and the users of the dispatch center had the shortest interviews, and the emergency medical personnel had the longest.
Data analysis
Since the researcher seeks to explore barriers to prehospital logistics support in traffic accidents with mass casualties, they chose the Elo et al. [16] approach for the current study. This approach involves open coding, creating categories, and abstraction [16-18]. One interviewer conducted all interviews. The interviews were recorded using mobile voice recorder software in a quiet and convenient environment and were accurately converted to textual data immediately after the interview. All interviews were implemented and transcribed on the first day after the interview. The participants’ feelings were noted, such as laughter, silence, tone, and speech. For a general understanding, the transcribed interview text was carefully studied several times. The participants’ own words and indicative codes (researcher’s perceptions of the statements) were used for the initial coding. Then, subsequent interviews were conducted. Semantic units were extracted from the main concepts, and each semantic unit was given a code. Different codes were placed in the main classes based on commonalities of meanings and concepts. Then, the classes were compared, and a theme emerged from the analysis and interpretation of the main classes.
Rigor
Enworo’s criteria were used, which included the four criteria of acceptability or credibility, confirmability, dependability, and transferability. Data validation by participants, research team colleagues, and two faculty members outside the research team increased acceptability and credibility. Two research team members coded the interviews to determine dependability; there was much agreement between the opinions. Extreme care was also taken in collecting, implementing, and recording data and allocating sufficient time to collect data. In the field of transferability, the information obtained by two faculty members outside the research team and experts in the field of qualitative research was reviewed and confirmed. Authenticity was also shown through participants’ statements of the phenomenon and how the researcher analyzed the data [19].
Results
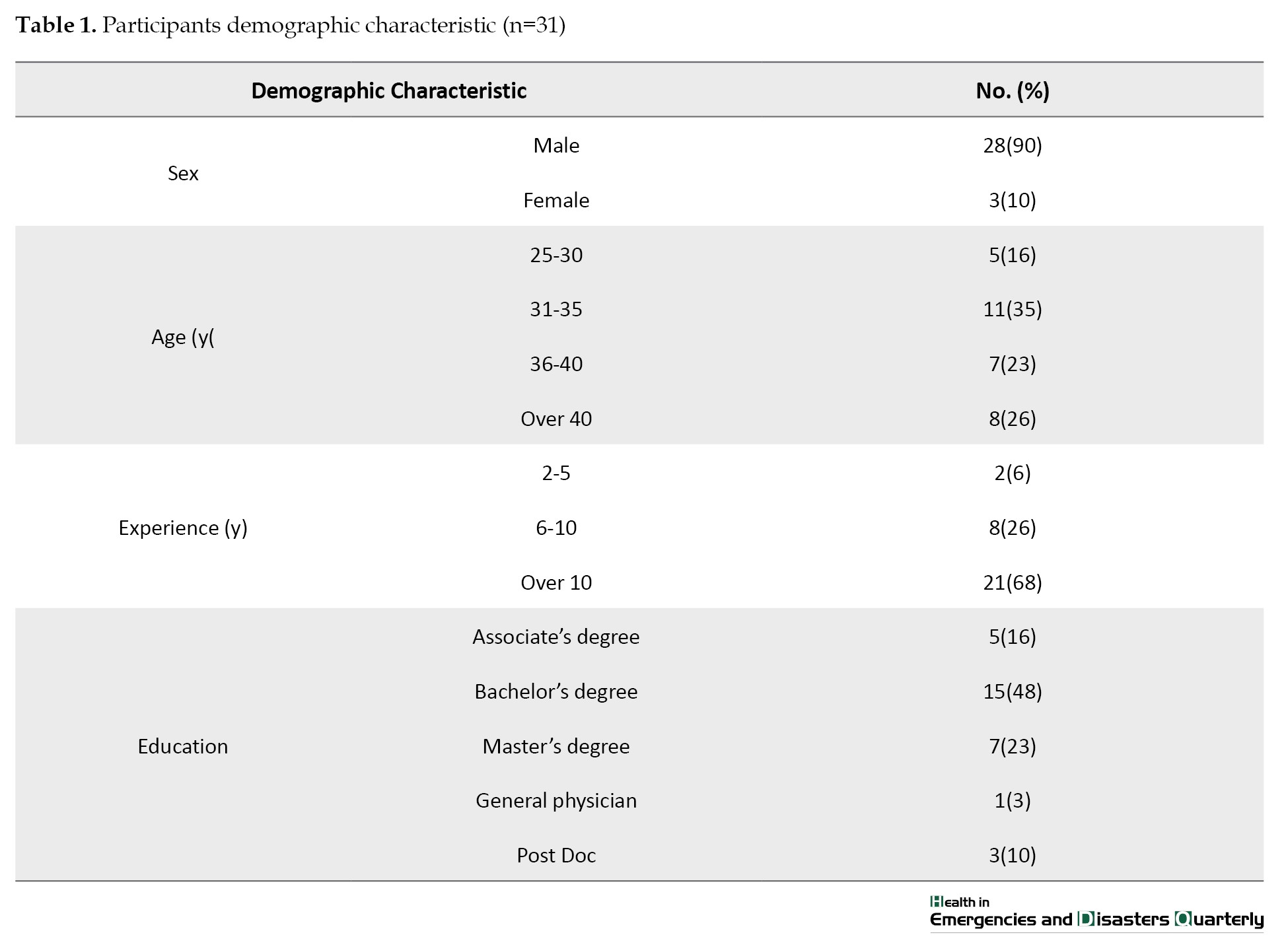
Twenty-seven participants were male, and 4 were female. The mean age of participants was 38 years, and their average work experience was 13 years (Table 1).
Three main categories were identified: Evaluation (with two subcategories: Incomplete assessment of the accident scene needs and inappropriate triage), resources and equipment (with two subcategories: Inadequate communication facilities and lack of professional equipment), and human resources (with two subcategories: Manpower challenges and inadequate staff skills as barriers. Establishing a command post and unified command on-site, participation of relief organizations in assessing the scene and triage of casualties, improving the quantity and quality of equipment, upgrading the communication system and using advanced communication technologies, and holding skills enhancement and training workshops to enhance staff skills in using equipment from other relief organizations are proposed solutions to facilitate prehospital logistics support in responding to traffic accidents with mass casualties (Table 2).

Evaluation
Incomplete assessment of the accident scene needs
The Dispatch Center assesses the scene over the phone by contacting those present. In some cases, the information obtained from the Dispatch Center was incomplete. The conditions of the accident scene, the type of injury, or the need for release have not been well assessed by the user of the Dispatch Center. Therefore, after the arrival of the personnel, the need for equipment and the release of the injured are determined. When emergency medical technician (EMT) personnel arrive at the scene, crowds prevent the activities of relief workers, especially scene assessments. EMT accuracy decreases when entering such a scene. They neglect to evaluate the scene when they see an injured person with a broken femur and subsequent heavy bleeding. After the technician evaluates the scene, the strangers move the injured to another place and create a crowded scene, which confuses the EMT and causes them to forget which one they evaluated.
“The patients we have evaluated, other people move to another place which disrupts the order and decision making. If we want to go back and evaluate all the patients, it will take us a long time.” (said EMT No. 3)
The involvement of relief organizations in scene evaluation should be planned. A joint inter-departmental team will conduct a thorough assessment of the accident scene and provide the basis for a better and more complete assessment of the scene, determining the number of injured, the needs of the accident scene, and the timely provision of relief services.
“A joint inter-departmental team of relief organization should assess the incident as part of the national response plan.” (said Head of Prehospital Emergency)
Improper triage
Prehospital emergency personnel lack the ability and power to decide on the triage of the injured when they are on the scene due to the large number of injured and the prevailing atmosphere. The injured, who should have been red during triage, were classified as yellow. It was not until after taking precautionary measures, being dispatched and re-triaged, that it had been realized that they had been mistakenly triaged. The red injured, who had to be taken care of quickly and transported to the medical center by ambulance, were triaged in the yellow group and taken to the ambulance bus. This response delays the provision of services to the injured needing urgent services and has sometimes resulted in irreparable damage. Occasionally, the injured were over-triaged, increasing the emergency department’s workload and congestion.
“When we enter the scene, we neglect triage and start treatment because of the atmosphere. In the same scene, we under-triage an injured person with high priority. When we see the injured person, he is bleeding, and his level of consciousness is reduced. We start medical treatment there, and in many cases, our triage remains incomplete.” (said EMT No. 8)
In triage, personnel should focus only on the outcome and efficiency of the operation, regardless of individual feelings and characteristics. The most difficult decision is about the injured who, despite being alive and receiving medical treatment, have no hope of being rescued, and eliminating them will increase the chances of survival and rescue of others. Triage on the scene is possible only with the relief organizations’ cooperation. Triage is done at the scene by trained personnel. Treatment measures at this stage are limited to rapid and pre-determined measures to help the patient survive.
“In the triage, the injured person gets a black tag, and his companions insist we take vital measures for him. If we want to start resuscitation for this person, other injured people who need urgent services will be in danger. We have to do triage in the simulated scene to master.” (said EMT No. 9)
Resources and equipment
Inadequate communication facilities
EMT personnel should be able to report the number, condition, and severity of injuries to the dispatch center at the accident scene so that relief personnel, ambulance, and equipment can be sent to the scene according to the accident situation. In difficult-to-reach areas, personnel cannot communicate the scene’s needs due to radio and mobile communication problems. They ask the occupants of passing vehicles to report scene information to Center 115 where possible.
“There are also places where we do not have radio communications. We have to travel a few kilometers to call for relief personnel to announce the need for release or more ambulances to the center.” (said EMT No. 7)
In the preparation phase, relief organizations must specify how to communicate with each other by radio within the framework of the national response program. Having a common communication center and communication number, as well as the use of communication and monitoring systems with high technology, such as telecommunication satellites, will promote the cooperation of organizations in the response phase. Successful operations require a continuous flow of information between relief organizations. Communication systems and related equipment must be constantly upgraded and updated.
“If I have a pre-determined plan for how to communicate with organizations and connect to police and Red Crescent relief organizations in an emergency, and the use of high-tech communication and surveillance systems such as telecommunications satellites can improve cooperation of other relief organizations with the prehospital emergency.” (said the Head of Prehospital Emergency)
Lack of professional equipment
According to the participants, the lack of equipment and infrastructure facilities is one of the main concerns of the prehospital emergency system. When accidents occur with many injured people, there is no physical space to receive the injured, including a crisis shelter. On the other hand, the number of hospital beds does not meet the large number of patients and increases the hospital’s workload. Sometimes, even the lack of prehospital and hospital equipment and facilities delays medical services. If the return of the splint or long backboard used by the prehospital emergency personnel to transport the injured to the hospital is delayed, then this delays the return of the prehospital personnel to their place of work. The lack of up-to-date and specialized helicopters is the biggest weakness of the relief organizations’ equipment in the prehospital area. None of the organizations has a suitable helicopter. Emergency prehospital helicopters are not specialized and are rented, and the Police and the Red Crescent lack the right helicopters to carry out missions. Economic sanctions have prevented the provision of up-to-date helicopters for relief organizations. It is also impossible to fly at night with the available helicopters.
“Our weakness in the field of helicopter equipment is that we do not have up-to-date helicopters for any of the organizations. Emergency helicopters are all rented and not specialized. Red Crescent helicopters also have problems. The Police are very weak in helicopters, and sanctions on this case have been very impressive.” (said the Head of Prehospital Emergency)
In accidents with mass casualties, due to the needs of the injured, the equipment in an ambulance is not enough, and the equipment is used only for the injured who are likely to survive. In the accident management center, one of the fields has equipped a vehicle with the required equipment called an MCI trailer, which covers all the equipment needed for the accident scene.
“When I have several injured people, I can do fixation for only one patient. We need extra equipment for three to four patients. We use the MCI trailer for MCI scenes.” (said EMT No. 9).
Human resources
Manpower challenges
Most participants noted the lack of two EMTs for the first ambulance to arrive at the scene with mass casualties. One EMT is not enough for critically injured people who need cardiopulmonary resuscitation or respiratory care such as suctioning, and the accident commander has used Red Crescent personnel to address this deficiency. In some cases, due to the small number of police personnel and the overcrowding, the police force has not been able to secure the scene, or the heavy, tedious, and vital work of cutting the columns of the accidental vehicle has been delayed due to lack of Red Crescent personnel.
“Two people are really not enough for the scene with many casualties. I have given one of my personnel to the emergency personnel many times to help him cope with the critically ill patient.” (Red Crescent Deputy of Relief and Rescue)
One of the ways to provide the human resources needed at the scene of the accident is to use the people present at the scene. People at the scene of the accident often obstruct the services of relief organizations by creating hustle and bustle. It is challenging to prevent people from entering the scene of an accident, and the intervention of the security forces alone does not work. With public first aid training, people-centered management, and the use of people’s participation, this challenge can be turned into an opportunity, and people’s participation and potential can be used to provide relief services. In human resources, our most important challenge is people-centered management, and people’s participation in scene management and response to events are our main challenges and weaknesses.
“We have not been able to organize, educate and inform people in a timely manner so that they can help us instead of harassing and gathering.” (Head of Prehospital Emergency)
Inadequate staff skills
The high skill and experience of the emergency medical technician at the accident scene accelerates medical services delivery and saves the lives of the injured at a golden time. The inability of the EMT to provide vital care, especially to open the airway and stabilize the spine, not only does not help the casualty but also causes irreparable damage. For example, a technician who is unable to open the injured airway has caused the patient to suffocate and die due to a wrong action.
“My teammate had given the laryngeal mask airways (LMA) to the patient, but the cuff did not inflate, or in another case, it had been reversed and caused the patient to suffocate, whereas if he put the airway and ambo in the same position, the injured would have survived.” (said EMT No. 7).
One of the most important issues in relief organizations is strengthening existing human resources. The purpose of reinforcement is to increase their abilities, skills, and motivations to increase the efficiency of personnel in accidents. Most participants noted the large gap between the knowledge and skills of relief workers. Achieving the desired level of skill requires holding scientific and practical courses. Training in communicating well with people, improving skills in providing relief services, and careful work planning so that personnel cover each other’s skills gap will improve personnel performance at the accident scene. The weakness of employees’ skills has shown the need to empower them.
“If the technician is tough, he can communicate properly and justify people well on stage. Staff skills need to be increased to function properly. The forces must work in rotation between crowded and secluded places so that you can see all the scenes, and the forces are arranged in such a way that they complement each other and cover each other’s weaknesses.” (said EMT No. 9).
Discussion
This study aimed to explore barriers to prehospital logistics support in traffic accidents with mass casualties. The results of this study showed that barriers to prehospital logistics support include evaluation (incomplete assessment of the accident scene needs and inappropriate triage), resources and equipment (inadequate communication facilities and lack of professional equipment), and human resources (manpower challenges and inadequate staff skills). The proposed solutions for improving prehospital logistics included establishing a command post and unified command on-site, participation of relief organizations in scene assessment and triage of casualties, improving the quantity and quality of equipment, utilizing advanced technologies to upgrade communication systems, and conducting training workshops to enhance staff skills in using equipment from other relief organizations.
The results of this study showed that by assessing the scene of the accident, scene safety, number of injured, type of injury, mechanism of injury, number of vehicles involved, and the need for the injured to be released in the car, the risk of overturning and explosion of the car was also assessed. One of the obstacles to determining the needs was the incomplete assessment of the accident scene by the relief personnel. Insufficient experience of relief personnel, crowds on the scene, and the large number of injured people have been the main reasons for the incomplete assessment of the accident scene. In addition, triage was not well performed by EMT personnel, who placed the red casualties in the yellow (delayed) group, which resulted in irreparable injuries. In this regard, the study of the Iraqi pilgrims’ bus accident showed that due to the lack of a plan and protocol for the call, relief organizations were not sent simultaneously. Traffic, crowds at the scene, and filming of some people present at the scene disrupted the scene, so much that a 12-year-old child was found at the scene after the rescue service ended. The triage process of the injured gets complicated due to the involvement of those present at the scene, so the injured of the green triage group are taken to the hospital with a red label [20]. Another study shows that due to the collapse of the stadium roof and the lack of access to the stage, EMT staff could not obtain accurate information on the number of injured, the type of injury, and the mechanism of injury. The lack of an accident command post and coordination of relief organizations to create an advanced medical post caused a lack of triage at the scene. The information about the injured was not recorded, and EMT staff did not have a specific plan to transfer the injured to the medical center [21]. Also, the assessment of the accident scene at the Yurt mine explosion showed that the response structure, command structure, and scene support were unsuccessful [22]. However, another study showed that the Emergency Medical Center contacted the scene to investigate the incident, including the number of injured, the severity of the injury, the number of vehicles involved, the mechanism of injury, and the safety of the scene, and then sent rescue teams and equipment appropriate to the scene. Triage was performed at the accident scene, and the injured were classified according to the severity of the injury and transferred to the nearest medical centers with priority [23].
To quickly assess the accidents with mass casualties, it is recommended that more ambulances or ambulance buses be dispatched to the scene instead of sending one ambulance. Scene crowds and inadequate EMT skills lead to inadequate triage. Establishing a single command post and an integrated on-site command is essential to facilitate effective coordination between relief organizations [20]. Also, quickly determining the accident location using global positioning system (GPS) and satellite tools helps determine the accident location and faster relief [24]. Access to information such as injury severity, number of casualties, and prehospital and inpatient resources will help decision-makers better understand and manage MCI [25].
Another finding of this study was resources and equipment. In this study, the lack of appropriate communication facilities to exchange information on the accident scene with the prehospital emergency center and Emergency Operations Center has caused delays in calling rescue organizations, dispatching personnel and facilities to the accident scene, and disrupting services to the injured. Similar to these findings, the systematic review study showed that in 5 out of 8 MCI reports, problems in the communication system, including wireless system malfunction, poor coverage, overload, and communication center confusion, led to receiving incomplete scene information and consequently different strategies of relief organizations in responding to MCI [26]. Also, in the Marathon bombings’ MCI response, while most centers were aware of the incident through the media, radio communication between relief workers was disrupted [27]. This study showed that the lack of professional equipment and infrastructure facilities such as crisis shelters, ambulances, medical equipment, splints, long backboards, and protective equipment delayed providing prehospital and hospital emergency systems services. In this regard, the results of a study show that due to the lack of logistics resources, such as protective equipment and first aid kits, as well as the lack of equipment use skills, EMT staff faced challenges in maintaining safety and providing medical services [28]. Other studies have reported a lack of access to ambulances due to the insufficient number of ambulances, technical defects, and fuel shortages [29, 30]. Making timely and effective decisions during rapid changes in events depends on the knowledge of available resources and the situation at the accident scene [31]. Increasing the quantity and quality of equipment and reserving ambulances to transport the injured in MCI [28], upgrading the communication system, and using advanced communication technologies will lead to better coverage of the personnel of relief organizations and their better cooperation with the prehospital emergency [26].
Human resources are another finding of this study. The availability of specialized trained personnel and effective human resource management ensures the continuation of prehospital logistical support to trauma victims in MCI [32]. In this study, manpower challenges are another barrier to providing services at the scene of an accident that has disrupted the care of critically injured. In this regard, several studies consider the lack of human resources as the most important barrier to providing care in MCI [13, 23] and the cause of delay in prehospital logistics support [33, 34]. Because in accidents with mass casualties, human resources, and equipment do not meet the number of injured and their needs for prehospital logistics support [35], increasing the number of emergency medical personnel and relief bases reduces access time at the scene, improves prehospital emergency system efficiency and reduces mortality due to delayed MCI [34]. The results of this study show that the insufficient skills of employees confuse them in providing timely medical services to the injured. In this regard, the study of preventable deaths in road accidents shows that EMT personnel do not have sufficient knowledge and skills to perform appropriate clinical care, which results in secondary injury to the injured [36]. One of the obstacles to prehospital care in traffic accidents in Iran is insufficient EMT skills, the main reasons for which are inadequate practical training, poor training programs, and insufficient motivation to attend training courses. It is necessary to improve the knowledge and ability of employees by holding skills enhancement and training workshops [37]. The results of another study show that improving the efficiency of staff and management of managers can reduce the time of access to the injured, accelerate the support of prehospital logistics, and reduce mortality [34].
Conclusion
To overcome the barriers to prehospital logistical support in response to traffic accidents with mass casualties, a more thorough assessment of the accident scene is required to ensure that the necessary human resources and equipment are deployed to the site appropriately and in a timely manner. Establishing a command post and unified command at the scene of the accident, participation of relief organizations in scene assessment and triage of casualties, improving the quantity and quality of equipment, increasing the number of personnel and aid stations, using advanced technologies, such as satellites and drones to assess the scene of the accident, upgrading the communication system and holding educational and skill-building workshops accelerates the provision of prehospital logistics support. Providing logistical services following the needs of the incident scene, improving the knowledge and skills of relief organization organizations from each other’s logistics resources, and sharing logistics resources will prevent their confusion in providing prehospital services, accelerate the support of prehospital logistics, and reduce injuries and deaths.
Limitations and strengths of the study
One of the strengths of this study is using the experiences of emergency personnel in four provinces, especially Qom, whose emergency forces have good experience in MCIs because the traffic load from most provinces toward Tehran passes through Qom. Some participants did not respond to follow-up phone interviews, while others responded. It is suggested that, given that the resources, equipment, and manpower of relief organizations vary according to their structure and objectives, barriers and facilitators of logistics sharing under a single command in accidents with mass casualties should be investigated. Examining strategies to improve the efficiency of managers and employees of relief organizations also improves the quality and quantity of prehospital logistics support.
Ethical Considerations
Compliance with ethical guidelines
The current study was approved by Shahid Sadoughi University of Medical Sciences, Yazd, Iran (Code: IR.SSU.SPH.REC.1397.020). Permission was granted to interview by receiving an introduction letter from the Faculty of Health and presenting it to the Medical Emergency and Accident Management Center of Universities of Medical Sciences in Yazd, Fars, Kohgiluyeh, Boyer-Ahmad, and Qom provinces. Written consent was obtained from the study participants. The participants were notified of the confidentiality of the interview and their right to withdraw from the study at any time. The interview time was decided at the participants’ will.
Funding
This article was extracted from the PhD dissertation of Seyed Javad Sadat, approved by the Faculty of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. This study was funded by Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Authors' contributions
Conceptualization and supervision: Mohammadreza Vafaeenasab and Mahsa Khodayarian; Methodology: Seyed Javad Sadat, and Davoud Khorasani-Zavareh; Data collection: Seyed Javad Sadat, Data analysis: Davoud Khorasani-Zavareh and Seyed Javad Sadat; Investigation, funding acquisition, resources and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the Vice-Chancellor for Research and Technology of Shahid Sadoughi University of Medical Sciences, Yazd, Iran, for the financial support and all relief organization staff who participated in this study for their cooperation.
References
Mass casualty incidents (MCIs) can be caused by various factors, including mass gatherings; armed conflicts; terrorism; biological, geophysical, meteorological, disasters; and traffic accidents [1]. According to the World Health Organization (WHO), accidents with mass casualties are accidents in which the casualties cannot be managed with the current facilities and resources and the usual operational processes of organizations [2]. Traffic accidents are the ninth leading cause of death worldwide, resulting in 1.35 million deaths and 50 million injuries annually [3]. In Iran, road traffic deaths dropped from 32.1 to 20.5 per 100000 people between 2015 and 2018. In 2015, Iran ranked eighth globally in traffic accident fatalities. By 2018, its ranking had dropped to 53rd [4]. The results of a study by Razzak et al. showed that post-crash care could lead to a reduction in trauma mortality of up to 35% [5]. This care depends on the cooperation and support of other relief organizations, such as the Red Cross, the Police, and the Fire Department, in providing resources and logistics [6].
Logistics is the process of mobilizing resources, skills, and knowledge to help disaster victims [7]. Emergency logistics aims to achieve maximum efficiency in a short time and minimize MCI losses [8]. MCI may severely damage large geographic areas and populations. Therefore, logistics operations in emergency incidents have complex dimensions, including damage assessment, estimation of needs, allocation of different resources in a short period, organization of rescue operations, and evacuation of the injured [9]. Dealing with uncertainty, unpredictability, unexpected consequences of accidents with mass casualties, unconfirmed information, and lack of information, sometimes contradictory, blurs the exact nature of the accident and makes decisions more difficult [10]. The Furbee report found that 38% of emergency service organizations are confused about providing answers and allocating appropriate resources [11]. Active cooperation inside and outside relief organizations in logistics is the most important part of disaster management with mass injuries, but insufficient infrastructure, lack of cooperation, and inadequate communication among relief organizations can lead to problems in logistics activities [12].
As the most important part of the Iranian Medical Emergency and Accident Management Center, the prehospital emergency system provides vital medical services at the scene of accidents with mass injuries [13]. The report by Obermeyer et al. highlights the lack of logistics resources and the lack of specialized training provided to emergency care service providers in low- and middle-income countries [14]. Despite multiple MCIs worldwide, there is a limited number of academic studies in logistics. Logistics support is a crucial field of research that needs the attention and support of people, organizations, and the government. The government has the opportunity to increase its share in MCI by improving the areas of knowledge management, technology, and measurement [7]. Modeling and simulation are the most commonly used method in the studies [14, 15]. Qualitative research on logistics in Iran has rarely been done. Therefore, to understand the experience of the personnel of relief organizations involved in accidents with mass casualties and logistics support in Iran, this study was conducted to explore barriers to prehospital logistics support in traffic accidents with mass casualties.
Materials and Methods
The present qualitative study was conducted using conventional content analysis.
Study participants and data collection
This study was conducted with the participation of employees of relief organizations, including emergency medical technicians, police forces, and Red Crescent staff in Yazd, Fars, Kohgiluyeh and Boyer-Ahmad, and Qom provinces, Iran from June 2018 to September 2019. Participants were recruited from the prehospital emergency system, the Red Crescent, the Police, and the transportation department. The first participant was selected using a purposive sampling method. The other participants entered the qualitative interview process by snowball method, which included 28 men and 3 women: Emergency technicians (9 participants), emergency medicine experts (5 participants), head of Emergency Operations Center (3 participants), dispatch operator (3 participants), head of Medical Emergency and Accident Management Center (3 participants), the Police (3 participants), Red Crescent Relief (2 participants), Deputy Red Crescent Rescue (1 participant), emergency medicine specialist (1 participant) and head of Road Transport Organization (1 participant). The number of female participants is low because Iran’s prehospital emergency personnel and other relief organizations are only men, and women only work as operators at the Dispatch Center. The inclusion criteria were the willingness to conduct interviews, the ability to express experiences, and having at least 2 years of work experience. The unwillingness to continue the interview and not answering the questions were considered criteria for exclusion. The first four interviews were conducted utilizing unstructured in-depth interviews followed by 27 semi-structured interviews. Each interview began with a general question: “Describe your experiences with the MCI in which you participated?” This question was asked of employees of relief organizations. The prehospital emergency personnel were asked: “What factors contributed to prehospital logistics support in the MCI you were involved in.” Probing questions such as “What do you mean?” “Please explain further” and “give an example of your objective in your experience” are used to clarify information and collect additional data. During the interviews, deterrents and facilitators of prehospital logistics support with exploratory questions were explored. This process continued until data saturation was reached. The duration of the interviews varied between 25 and 100 minutes. There was a relationship between the time of the interviews and the expertise of the interviewees. So, the head of the Transportation Department and the users of the dispatch center had the shortest interviews, and the emergency medical personnel had the longest.
Data analysis
Since the researcher seeks to explore barriers to prehospital logistics support in traffic accidents with mass casualties, they chose the Elo et al. [16] approach for the current study. This approach involves open coding, creating categories, and abstraction [16-18]. One interviewer conducted all interviews. The interviews were recorded using mobile voice recorder software in a quiet and convenient environment and were accurately converted to textual data immediately after the interview. All interviews were implemented and transcribed on the first day after the interview. The participants’ feelings were noted, such as laughter, silence, tone, and speech. For a general understanding, the transcribed interview text was carefully studied several times. The participants’ own words and indicative codes (researcher’s perceptions of the statements) were used for the initial coding. Then, subsequent interviews were conducted. Semantic units were extracted from the main concepts, and each semantic unit was given a code. Different codes were placed in the main classes based on commonalities of meanings and concepts. Then, the classes were compared, and a theme emerged from the analysis and interpretation of the main classes.
Rigor
Enworo’s criteria were used, which included the four criteria of acceptability or credibility, confirmability, dependability, and transferability. Data validation by participants, research team colleagues, and two faculty members outside the research team increased acceptability and credibility. Two research team members coded the interviews to determine dependability; there was much agreement between the opinions. Extreme care was also taken in collecting, implementing, and recording data and allocating sufficient time to collect data. In the field of transferability, the information obtained by two faculty members outside the research team and experts in the field of qualitative research was reviewed and confirmed. Authenticity was also shown through participants’ statements of the phenomenon and how the researcher analyzed the data [19].
Results
Twenty-seven participants were male, and 4 were female. The mean age of participants was 38 years, and their average work experience was 13 years (Table 1).
Three main categories were identified: Evaluation (with two subcategories: Incomplete assessment of the accident scene needs and inappropriate triage), resources and equipment (with two subcategories: Inadequate communication facilities and lack of professional equipment), and human resources (with two subcategories: Manpower challenges and inadequate staff skills as barriers. Establishing a command post and unified command on-site, participation of relief organizations in assessing the scene and triage of casualties, improving the quantity and quality of equipment, upgrading the communication system and using advanced communication technologies, and holding skills enhancement and training workshops to enhance staff skills in using equipment from other relief organizations are proposed solutions to facilitate prehospital logistics support in responding to traffic accidents with mass casualties (Table 2).
Evaluation
Incomplete assessment of the accident scene needs
The Dispatch Center assesses the scene over the phone by contacting those present. In some cases, the information obtained from the Dispatch Center was incomplete. The conditions of the accident scene, the type of injury, or the need for release have not been well assessed by the user of the Dispatch Center. Therefore, after the arrival of the personnel, the need for equipment and the release of the injured are determined. When emergency medical technician (EMT) personnel arrive at the scene, crowds prevent the activities of relief workers, especially scene assessments. EMT accuracy decreases when entering such a scene. They neglect to evaluate the scene when they see an injured person with a broken femur and subsequent heavy bleeding. After the technician evaluates the scene, the strangers move the injured to another place and create a crowded scene, which confuses the EMT and causes them to forget which one they evaluated.
“The patients we have evaluated, other people move to another place which disrupts the order and decision making. If we want to go back and evaluate all the patients, it will take us a long time.” (said EMT No. 3)
The involvement of relief organizations in scene evaluation should be planned. A joint inter-departmental team will conduct a thorough assessment of the accident scene and provide the basis for a better and more complete assessment of the scene, determining the number of injured, the needs of the accident scene, and the timely provision of relief services.
“A joint inter-departmental team of relief organization should assess the incident as part of the national response plan.” (said Head of Prehospital Emergency)
Improper triage
Prehospital emergency personnel lack the ability and power to decide on the triage of the injured when they are on the scene due to the large number of injured and the prevailing atmosphere. The injured, who should have been red during triage, were classified as yellow. It was not until after taking precautionary measures, being dispatched and re-triaged, that it had been realized that they had been mistakenly triaged. The red injured, who had to be taken care of quickly and transported to the medical center by ambulance, were triaged in the yellow group and taken to the ambulance bus. This response delays the provision of services to the injured needing urgent services and has sometimes resulted in irreparable damage. Occasionally, the injured were over-triaged, increasing the emergency department’s workload and congestion.
“When we enter the scene, we neglect triage and start treatment because of the atmosphere. In the same scene, we under-triage an injured person with high priority. When we see the injured person, he is bleeding, and his level of consciousness is reduced. We start medical treatment there, and in many cases, our triage remains incomplete.” (said EMT No. 8)
In triage, personnel should focus only on the outcome and efficiency of the operation, regardless of individual feelings and characteristics. The most difficult decision is about the injured who, despite being alive and receiving medical treatment, have no hope of being rescued, and eliminating them will increase the chances of survival and rescue of others. Triage on the scene is possible only with the relief organizations’ cooperation. Triage is done at the scene by trained personnel. Treatment measures at this stage are limited to rapid and pre-determined measures to help the patient survive.
“In the triage, the injured person gets a black tag, and his companions insist we take vital measures for him. If we want to start resuscitation for this person, other injured people who need urgent services will be in danger. We have to do triage in the simulated scene to master.” (said EMT No. 9)
Resources and equipment
Inadequate communication facilities
EMT personnel should be able to report the number, condition, and severity of injuries to the dispatch center at the accident scene so that relief personnel, ambulance, and equipment can be sent to the scene according to the accident situation. In difficult-to-reach areas, personnel cannot communicate the scene’s needs due to radio and mobile communication problems. They ask the occupants of passing vehicles to report scene information to Center 115 where possible.
“There are also places where we do not have radio communications. We have to travel a few kilometers to call for relief personnel to announce the need for release or more ambulances to the center.” (said EMT No. 7)
In the preparation phase, relief organizations must specify how to communicate with each other by radio within the framework of the national response program. Having a common communication center and communication number, as well as the use of communication and monitoring systems with high technology, such as telecommunication satellites, will promote the cooperation of organizations in the response phase. Successful operations require a continuous flow of information between relief organizations. Communication systems and related equipment must be constantly upgraded and updated.
“If I have a pre-determined plan for how to communicate with organizations and connect to police and Red Crescent relief organizations in an emergency, and the use of high-tech communication and surveillance systems such as telecommunications satellites can improve cooperation of other relief organizations with the prehospital emergency.” (said the Head of Prehospital Emergency)
Lack of professional equipment
According to the participants, the lack of equipment and infrastructure facilities is one of the main concerns of the prehospital emergency system. When accidents occur with many injured people, there is no physical space to receive the injured, including a crisis shelter. On the other hand, the number of hospital beds does not meet the large number of patients and increases the hospital’s workload. Sometimes, even the lack of prehospital and hospital equipment and facilities delays medical services. If the return of the splint or long backboard used by the prehospital emergency personnel to transport the injured to the hospital is delayed, then this delays the return of the prehospital personnel to their place of work. The lack of up-to-date and specialized helicopters is the biggest weakness of the relief organizations’ equipment in the prehospital area. None of the organizations has a suitable helicopter. Emergency prehospital helicopters are not specialized and are rented, and the Police and the Red Crescent lack the right helicopters to carry out missions. Economic sanctions have prevented the provision of up-to-date helicopters for relief organizations. It is also impossible to fly at night with the available helicopters.
“Our weakness in the field of helicopter equipment is that we do not have up-to-date helicopters for any of the organizations. Emergency helicopters are all rented and not specialized. Red Crescent helicopters also have problems. The Police are very weak in helicopters, and sanctions on this case have been very impressive.” (said the Head of Prehospital Emergency)
In accidents with mass casualties, due to the needs of the injured, the equipment in an ambulance is not enough, and the equipment is used only for the injured who are likely to survive. In the accident management center, one of the fields has equipped a vehicle with the required equipment called an MCI trailer, which covers all the equipment needed for the accident scene.
“When I have several injured people, I can do fixation for only one patient. We need extra equipment for three to four patients. We use the MCI trailer for MCI scenes.” (said EMT No. 9).
Human resources
Manpower challenges
Most participants noted the lack of two EMTs for the first ambulance to arrive at the scene with mass casualties. One EMT is not enough for critically injured people who need cardiopulmonary resuscitation or respiratory care such as suctioning, and the accident commander has used Red Crescent personnel to address this deficiency. In some cases, due to the small number of police personnel and the overcrowding, the police force has not been able to secure the scene, or the heavy, tedious, and vital work of cutting the columns of the accidental vehicle has been delayed due to lack of Red Crescent personnel.
“Two people are really not enough for the scene with many casualties. I have given one of my personnel to the emergency personnel many times to help him cope with the critically ill patient.” (Red Crescent Deputy of Relief and Rescue)
One of the ways to provide the human resources needed at the scene of the accident is to use the people present at the scene. People at the scene of the accident often obstruct the services of relief organizations by creating hustle and bustle. It is challenging to prevent people from entering the scene of an accident, and the intervention of the security forces alone does not work. With public first aid training, people-centered management, and the use of people’s participation, this challenge can be turned into an opportunity, and people’s participation and potential can be used to provide relief services. In human resources, our most important challenge is people-centered management, and people’s participation in scene management and response to events are our main challenges and weaknesses.
“We have not been able to organize, educate and inform people in a timely manner so that they can help us instead of harassing and gathering.” (Head of Prehospital Emergency)
Inadequate staff skills
The high skill and experience of the emergency medical technician at the accident scene accelerates medical services delivery and saves the lives of the injured at a golden time. The inability of the EMT to provide vital care, especially to open the airway and stabilize the spine, not only does not help the casualty but also causes irreparable damage. For example, a technician who is unable to open the injured airway has caused the patient to suffocate and die due to a wrong action.
“My teammate had given the laryngeal mask airways (LMA) to the patient, but the cuff did not inflate, or in another case, it had been reversed and caused the patient to suffocate, whereas if he put the airway and ambo in the same position, the injured would have survived.” (said EMT No. 7).
One of the most important issues in relief organizations is strengthening existing human resources. The purpose of reinforcement is to increase their abilities, skills, and motivations to increase the efficiency of personnel in accidents. Most participants noted the large gap between the knowledge and skills of relief workers. Achieving the desired level of skill requires holding scientific and practical courses. Training in communicating well with people, improving skills in providing relief services, and careful work planning so that personnel cover each other’s skills gap will improve personnel performance at the accident scene. The weakness of employees’ skills has shown the need to empower them.
“If the technician is tough, he can communicate properly and justify people well on stage. Staff skills need to be increased to function properly. The forces must work in rotation between crowded and secluded places so that you can see all the scenes, and the forces are arranged in such a way that they complement each other and cover each other’s weaknesses.” (said EMT No. 9).
Discussion
This study aimed to explore barriers to prehospital logistics support in traffic accidents with mass casualties. The results of this study showed that barriers to prehospital logistics support include evaluation (incomplete assessment of the accident scene needs and inappropriate triage), resources and equipment (inadequate communication facilities and lack of professional equipment), and human resources (manpower challenges and inadequate staff skills). The proposed solutions for improving prehospital logistics included establishing a command post and unified command on-site, participation of relief organizations in scene assessment and triage of casualties, improving the quantity and quality of equipment, utilizing advanced technologies to upgrade communication systems, and conducting training workshops to enhance staff skills in using equipment from other relief organizations.
The results of this study showed that by assessing the scene of the accident, scene safety, number of injured, type of injury, mechanism of injury, number of vehicles involved, and the need for the injured to be released in the car, the risk of overturning and explosion of the car was also assessed. One of the obstacles to determining the needs was the incomplete assessment of the accident scene by the relief personnel. Insufficient experience of relief personnel, crowds on the scene, and the large number of injured people have been the main reasons for the incomplete assessment of the accident scene. In addition, triage was not well performed by EMT personnel, who placed the red casualties in the yellow (delayed) group, which resulted in irreparable injuries. In this regard, the study of the Iraqi pilgrims’ bus accident showed that due to the lack of a plan and protocol for the call, relief organizations were not sent simultaneously. Traffic, crowds at the scene, and filming of some people present at the scene disrupted the scene, so much that a 12-year-old child was found at the scene after the rescue service ended. The triage process of the injured gets complicated due to the involvement of those present at the scene, so the injured of the green triage group are taken to the hospital with a red label [20]. Another study shows that due to the collapse of the stadium roof and the lack of access to the stage, EMT staff could not obtain accurate information on the number of injured, the type of injury, and the mechanism of injury. The lack of an accident command post and coordination of relief organizations to create an advanced medical post caused a lack of triage at the scene. The information about the injured was not recorded, and EMT staff did not have a specific plan to transfer the injured to the medical center [21]. Also, the assessment of the accident scene at the Yurt mine explosion showed that the response structure, command structure, and scene support were unsuccessful [22]. However, another study showed that the Emergency Medical Center contacted the scene to investigate the incident, including the number of injured, the severity of the injury, the number of vehicles involved, the mechanism of injury, and the safety of the scene, and then sent rescue teams and equipment appropriate to the scene. Triage was performed at the accident scene, and the injured were classified according to the severity of the injury and transferred to the nearest medical centers with priority [23].
To quickly assess the accidents with mass casualties, it is recommended that more ambulances or ambulance buses be dispatched to the scene instead of sending one ambulance. Scene crowds and inadequate EMT skills lead to inadequate triage. Establishing a single command post and an integrated on-site command is essential to facilitate effective coordination between relief organizations [20]. Also, quickly determining the accident location using global positioning system (GPS) and satellite tools helps determine the accident location and faster relief [24]. Access to information such as injury severity, number of casualties, and prehospital and inpatient resources will help decision-makers better understand and manage MCI [25].
Another finding of this study was resources and equipment. In this study, the lack of appropriate communication facilities to exchange information on the accident scene with the prehospital emergency center and Emergency Operations Center has caused delays in calling rescue organizations, dispatching personnel and facilities to the accident scene, and disrupting services to the injured. Similar to these findings, the systematic review study showed that in 5 out of 8 MCI reports, problems in the communication system, including wireless system malfunction, poor coverage, overload, and communication center confusion, led to receiving incomplete scene information and consequently different strategies of relief organizations in responding to MCI [26]. Also, in the Marathon bombings’ MCI response, while most centers were aware of the incident through the media, radio communication between relief workers was disrupted [27]. This study showed that the lack of professional equipment and infrastructure facilities such as crisis shelters, ambulances, medical equipment, splints, long backboards, and protective equipment delayed providing prehospital and hospital emergency systems services. In this regard, the results of a study show that due to the lack of logistics resources, such as protective equipment and first aid kits, as well as the lack of equipment use skills, EMT staff faced challenges in maintaining safety and providing medical services [28]. Other studies have reported a lack of access to ambulances due to the insufficient number of ambulances, technical defects, and fuel shortages [29, 30]. Making timely and effective decisions during rapid changes in events depends on the knowledge of available resources and the situation at the accident scene [31]. Increasing the quantity and quality of equipment and reserving ambulances to transport the injured in MCI [28], upgrading the communication system, and using advanced communication technologies will lead to better coverage of the personnel of relief organizations and their better cooperation with the prehospital emergency [26].
Human resources are another finding of this study. The availability of specialized trained personnel and effective human resource management ensures the continuation of prehospital logistical support to trauma victims in MCI [32]. In this study, manpower challenges are another barrier to providing services at the scene of an accident that has disrupted the care of critically injured. In this regard, several studies consider the lack of human resources as the most important barrier to providing care in MCI [13, 23] and the cause of delay in prehospital logistics support [33, 34]. Because in accidents with mass casualties, human resources, and equipment do not meet the number of injured and their needs for prehospital logistics support [35], increasing the number of emergency medical personnel and relief bases reduces access time at the scene, improves prehospital emergency system efficiency and reduces mortality due to delayed MCI [34]. The results of this study show that the insufficient skills of employees confuse them in providing timely medical services to the injured. In this regard, the study of preventable deaths in road accidents shows that EMT personnel do not have sufficient knowledge and skills to perform appropriate clinical care, which results in secondary injury to the injured [36]. One of the obstacles to prehospital care in traffic accidents in Iran is insufficient EMT skills, the main reasons for which are inadequate practical training, poor training programs, and insufficient motivation to attend training courses. It is necessary to improve the knowledge and ability of employees by holding skills enhancement and training workshops [37]. The results of another study show that improving the efficiency of staff and management of managers can reduce the time of access to the injured, accelerate the support of prehospital logistics, and reduce mortality [34].
Conclusion
To overcome the barriers to prehospital logistical support in response to traffic accidents with mass casualties, a more thorough assessment of the accident scene is required to ensure that the necessary human resources and equipment are deployed to the site appropriately and in a timely manner. Establishing a command post and unified command at the scene of the accident, participation of relief organizations in scene assessment and triage of casualties, improving the quantity and quality of equipment, increasing the number of personnel and aid stations, using advanced technologies, such as satellites and drones to assess the scene of the accident, upgrading the communication system and holding educational and skill-building workshops accelerates the provision of prehospital logistics support. Providing logistical services following the needs of the incident scene, improving the knowledge and skills of relief organization organizations from each other’s logistics resources, and sharing logistics resources will prevent their confusion in providing prehospital services, accelerate the support of prehospital logistics, and reduce injuries and deaths.
Limitations and strengths of the study
One of the strengths of this study is using the experiences of emergency personnel in four provinces, especially Qom, whose emergency forces have good experience in MCIs because the traffic load from most provinces toward Tehran passes through Qom. Some participants did not respond to follow-up phone interviews, while others responded. It is suggested that, given that the resources, equipment, and manpower of relief organizations vary according to their structure and objectives, barriers and facilitators of logistics sharing under a single command in accidents with mass casualties should be investigated. Examining strategies to improve the efficiency of managers and employees of relief organizations also improves the quality and quantity of prehospital logistics support.
Ethical Considerations
Compliance with ethical guidelines
The current study was approved by Shahid Sadoughi University of Medical Sciences, Yazd, Iran (Code: IR.SSU.SPH.REC.1397.020). Permission was granted to interview by receiving an introduction letter from the Faculty of Health and presenting it to the Medical Emergency and Accident Management Center of Universities of Medical Sciences in Yazd, Fars, Kohgiluyeh, Boyer-Ahmad, and Qom provinces. Written consent was obtained from the study participants. The participants were notified of the confidentiality of the interview and their right to withdraw from the study at any time. The interview time was decided at the participants’ will.
Funding
This article was extracted from the PhD dissertation of Seyed Javad Sadat, approved by the Faculty of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. This study was funded by Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Authors' contributions
Conceptualization and supervision: Mohammadreza Vafaeenasab and Mahsa Khodayarian; Methodology: Seyed Javad Sadat, and Davoud Khorasani-Zavareh; Data collection: Seyed Javad Sadat, Data analysis: Davoud Khorasani-Zavareh and Seyed Javad Sadat; Investigation, funding acquisition, resources and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the Vice-Chancellor for Research and Technology of Shahid Sadoughi University of Medical Sciences, Yazd, Iran, for the financial support and all relief organization staff who participated in this study for their cooperation.
References
- Gabbe BJ, Veitch W, Curtis K, Martin K, Gomez D, Civil I, et al. Survey of major trauma centre preparedness for mass casualty incidents in Australia, Canada, England and New Zealand. EClinicalMedicine. 2020; 21:100322. [DOI:10.1016/j.eclinm.2020.100322] [PMID] [PMCID]
- Mohanty CR, Radhakrishnan RV, Stephen S, Jain M, Shetty AP, Issac A, et al. Epidemiology of mass casualty incidents in a tertiary care trauma center in eastern India: A retrospective observational study. Turkish Journal of Emergency Medicine. 2022; 22(2):96-103. [DOI:10.4103/2452-2473.342806] [PMID] [PMCID]
- Hylander J, Saveman BI, Björnstig U, Gyllencreutz L, Westman A. Time-efficiency factors in road tunnel rescue as perceived by Swedish operative personnel-an interview study. International Journal of Emergency Services. 2022; 11(2):312-24. [Link]
- World Health Organization. Global status report on road safety 2018. Geneva: World Health Organization; 2018. [Link]
- Razzak JA, Bhatti J, Wright K, Nyirenda M, Tahir MR, Hyder AA. Improvement in trauma care for road traffic injuries: an assessment of the effect on mortality in low-income and middle-income countries. The Lancet. 2022; 400(10348):329-36. [DOI:10.1016/S0140-6736(22)00887-X] [PMID]
- Karagiannis GM. A socio-technical systems approach for the analysis of emergency services [MA thesis]. Patras: Hellenic Open University; 2017. [Link]
- Raillani HA, Hammadi LA, Samed MA, EL Ballouti AB, Barbu VS. Humanitarian logistics in the disaster relief supply chain: state of the art. In: Syngellakis S, Fabbri A, editors. Risk Analysis XII. Southampton: WIT Press; 2020. [Link]
- Daud MS, Hussein MZ, Nasir ME, Abdullah R, Kassim R, Suliman MS, et al. Humanitarian logistics and its challenges: The literature review. International Journal of Supply Chain Management. 2016; 5(3):107-10. [Link]
- Xu H, Fang D, Jin Y. Emergency logistics theory, model and method: A review and further research directions. Proceedings of the 2018 3rd International Conference on Communications, Information Management and Network Security (CIMNS 2018). Dordrecht: Atlantis Press; 2018. [DOI:10.2991/cimns-18.2018.42]
- Jiang Y, Yuan Y. Emergency logistics in a large-scale disaster context: Achievements and challenges. International Journal of Environmental Research and Public Health. 2019; 16(5):779. [DOI:10.3390/ijerph16050779] [PMID] [PMCID]
- Furbee PM, Coben JH, Smyth SK, Manley WG, Summers DE, Sanddal ND, et al. Realities of rural emergency medical services disaster preparedness. Prehospital and Disaster Medicine. 2006; 21(2):64-70. [DOI:10.1017/s1049023x0000337x] [PMID]
- Manley WG, Furbee PM, Coben JH, Smyth SK, Summers DE, Althouse RC, et al. Realities of disaster preparedness in rural hospitals. Disaster Management & Response: DMR: An Official Publication of the Emergency Nurses Association. 2006; 4(3):80-7. [DOI:10.1016/j.dmr.2006.05.001] [PMID]
- Koseoglu AM, Yıldırımlı H. The role of logistics in disaster management and disaster logistics issues. Journal of Teaching and Education. 2015; 4(3):377-88. [Link]
- Obermeyer Z, Abujaber S, Makar M, Stoll S, Kayden SR, Wallis LA, et al. Emergency care in 59 low-and middle-income countries: A systematic review. Bulletin of The World Health Organization. 2015; 93(8):577-86G. [DOI:10.2471/BLT.14.148338] [PMID] [PMCID]
- Dashtiyan AA, Masoudi Asl I, Riahi L, Mahmoodi M. Developing a Model for the Establishment of Pre-Hospital Emergency Medicine Bases in the Northern Provinces of Iran. Farmeconomia Health Economics and Therapeutic Pathways. 2019; 20(1). [DOI:10.7175/fe.v20i1.1381]
- Elo S, Kääriäinen M, Kanste O, Pölkki T, Utriainen K, Kyngäs H. Qualitative content analysis: A focus on trustworthiness. SAGE Open. 2014; 4(1):2158244014522633. [DOI:10.1177/2158244014522633]
- Adiguzel S. Logistics management in disaster. Journal of Management Marketing and Logistics. 2019; 6(4):212-24. [Link]
- Sadat S, Khodayarian M, Vafaeenasab M. Factors affecting the skill and efficiency of emergency medical service staff in mass casualty road traffic incidents: A qualitative study. Journal of Clinical Care and Skills. 2022; 3(3):97-104. [DOI:10.52547/jccs.3.3.97]
- Enworo OC. Application of Guba and Lincoln's parallel criteria to assess trustworthiness of qualitative research on indigenous social protection systems. Qualitative Research Journal. 2023; 23(4):372-84. [Link]
- Speziale HS, Carpenter DR. Qualitative research in nursing: Advancing the humanistic imperative. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2011.[Link]
- Safi Keykaleh M, Sohrabizadeh S. The Emergency Medical System (EMS) response to Iraqi pilgrims’ bus crash in Iran: A case report. BMC Emergency Medicine. 2019; 19(1):38. [DOI:10.1186/s12873-019-0253-2] [PMID] [PMCID]
- Cha MI, Kim GW, Kim CH, Choa M, Choi DH, Kim I, Wang SJ, et al. A study on the disaster medical response during the Mauna Ocean Resort Gymnasium collapse. Clinical and Experimental Emergency Medicine. 2016;3 (3):165-74. [PMID]
- Raeisi AR, Mohajervatan A, Mehraein Nazdik Z. Mass casualty response to mine explosion: A case report in Iran. Health in Emergencies and Disasters. 2019; 4(3):173-8. [DOI:10.32598/hdq.4.3.173]
- Lee HY, Lee JI, Kim OH, Lee KH, Kim HT, Youk H. Assessment of the disaster medical response system through an investigation of a 43-vehicle mass collision on Jung-ang expressway. Accident Analysis & Prevention. 2019; 123:60-8. [DOI:10.1016/j.aap.2018.11.004] [PMID]
- Kolifarhood G, Khorasani-Zavareh D, Salarilak S, Shoghli A, Khosravi N. Spatial and non-spatial determinants of successful tuberculosis treatment outcomes: An implication of Geographical Information Systems in health policy-making in a developing country. Journal of Epidemiology and Global Health. 2015; 5(3):221-30. [DOI:10.1016/j.jegh.2014.11.001] [PMID] [PMCID]
- Dean MD, Nair SK. Mass-casualty triage: Distribution of victims to multiple hospitals using the SAVE model. European Journal of Operational Research. 2014; 238(1):363-73. [DOI:10.1016/j.ejor.2014.03.028]
- Hardy S, Fattah S, Wisborg T, Raatiniemi L, Staff T, Rehn M. Systematic reporting to improve the emergency medical response to major incidents: A pilot study. BMC Emergency Medicine. 2018; 18(1):6. [PMID]
- Ahmad S. Mass casualty incident management. Missouri Medicine. 2018; 115(5):451-5. [PMID]
- Lukumay GG, Outwater AH, Mkoka DA, Ndile ML, Saveman BI. Traffic police officers’ experience of post-crash care to road traffic injury victims: A qualitative study in Tanzania”. BMC Emergency Medicine. 2019; 19(1):51. [DOI:10.1186/s12873-019-0274-x] [PMID] [PMCID]
- Wesson HK, Stevens KA, Bachani AM, Mogere S, Akungah D, Nyamari J, et al. Trauma systems in Kenya: A qualitative analysis at the district level. Qualitative Health Research. 2015; 25(5):589-99. [DOI:10.1177/1049732314562890] [PMID]
- Sidney K, Ryan K, Diwan V, De Costa A. Utilization of a state run public private emergency transportation service exclusively for childbirth: The Janani (maternal) Express program in Madhya Pradesh, India. PLoS One. 2014; 9(5):e96287. [DOI:10.1371/journal.pone.0096287] [PMID] [PMCID]
- Marres GM, Taal L, Bemelman M, Bouman J, Leenen LP. Online victim tracking and tracing system (ViTTS) for major incident casualties. Prehospital and Disaster Medicine. 2013; 28(5):445-53. [DOI:10.1017/S1049023X13003567] [PMID]
- Hosseini SH, Amanat N, Ghanbari V, Nakhaee M, Abbasabadi M, Najafi M, et al. Community-based management challenges in disaster risk reduction: A content analysis in Iran. Health in Emergencies and Disasters. 2017; 2(2):63-70. [DOI:10.18869/nrip.hdq.2.2.63]
- Hong W, Kim I, Wang SJ. Experiences and lessons of the disaster medical assistance in Korea. Journal of The Korean Medical Association. 2014; 57(12):999-1007. [Link]
- Yu W, Lv Y, Hu C, Liu X, Chen H, Xue C, et al. Research of an emergency medical system for mass casualty incidents in Shanghai, China: A system dynamics model. Patient Preference and Adherence. 2018; 12:207-22. [DOI:10.2147/PPA.S155603] [PMID] [PMCID]
- Leow J, Brundage S, Kushner A, Kamara T, Hanciles E, Muana A, et al. Mass casualty incident training in a resource-limited environment. The British Journal of Surgery. 2012; 99(3):356-61. [DOI:10.1002/bjs.7762] [PMID]
- Eftekhari A, DehghaniTafti A, Nasiriani K, Hajimaghsoudi M, Fallahzadeh H, Khorasani-Zavareh D. Management of preventable deaths due to road traffic injuries in prehospital phase; a qualitative study. Archives of Academic Emergency Medicine. 2019; 7(1):32. [PMID]
Type of article: Research |
Subject:
Qualitative
Received: 2024/04/25 | Accepted: 2024/12/10 | Published: 2025/04/1
Received: 2024/04/25 | Accepted: 2024/12/10 | Published: 2025/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
