

Volume 10, Issue 4 (Summer 2025)
Health in Emergencies and Disasters Quarterly 2025, 10(4): 291-300 |
Back to browse issues page


Ethics code: IR.MAZUMS.REC.1401.536
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Jorbonyan A, Hosseinnataj A, Naseri F, Najafi H, Rezapour V, Alizadeh M et al . COVID-19 Risk Perception and Its Relationship With Quality of Life and Mental Health Conditions in Older Diabetic Woman. Health in Emergencies and Disasters Quarterly 2025; 10 (4) :291-300
URL: http://hdq.uswr.ac.ir/article-1-621-en.html
URL: http://hdq.uswr.ac.ir/article-1-621-en.html
Abdolhakim Jorbonyan1 

 , Abolfazl Hosseinnataj2 , Farzaneh Naseri3 , Hadi Najafi4 , Vahideh Rezapour5 , Mohammadreza Alizadeh6 , Shahab Papi *7
, Abolfazl Hosseinnataj2 , Farzaneh Naseri3 , Hadi Najafi4 , Vahideh Rezapour5 , Mohammadreza Alizadeh6 , Shahab Papi *7
, Abolfazl Hosseinnataj2 , Farzaneh Naseri3 , Hadi Najafi4 , Vahideh Rezapour5 , Mohammadreza Alizadeh6 , Shahab Papi *7
1- Department of Geriatric Health, Faculty of Health, Mazandaran University of Medical Sciences, Sari, Iran. & Health Sciences Research Center, Mazandaran University of Medical Sciences, Sari, Iran.
2- Department of Biostatistics and Epidemiology, Faculty of Health, Mazandaran University of Medical Sciences, Sari, Iran.
3- Student Research Committee, Faculty of Nursing and Midwifery, Mazandaran University of Medical Sciences, Sari, Iran.
4- Department of Geriatric Health, School of Rehabilitation, Tehran University of Medical Sciences, Tehran, Iran.
5- Department of Geriatric Health, Faculty of Health, Tabriz University of Medical Sciences, Tabriz, Iran.
6- Department of Geriatric Health, School of Public Health, Babol University of Medical Sciences, Babol, Iran.
7- Health Sciences Research Center, Mazandaran University of Medical Sciences, Sari, Iran. & Department of Nursing, School of Nursing and Midwifery, Lorestan University of Medical Sciences, Khorramabad, Iran. ,shahabpapi@yahoo.com
2- Department of Biostatistics and Epidemiology, Faculty of Health, Mazandaran University of Medical Sciences, Sari, Iran.
3- Student Research Committee, Faculty of Nursing and Midwifery, Mazandaran University of Medical Sciences, Sari, Iran.
4- Department of Geriatric Health, School of Rehabilitation, Tehran University of Medical Sciences, Tehran, Iran.
5- Department of Geriatric Health, Faculty of Health, Tabriz University of Medical Sciences, Tabriz, Iran.
6- Department of Geriatric Health, School of Public Health, Babol University of Medical Sciences, Babol, Iran.
7- Health Sciences Research Center, Mazandaran University of Medical Sciences, Sari, Iran. & Department of Nursing, School of Nursing and Midwifery, Lorestan University of Medical Sciences, Khorramabad, Iran. ,
Full-Text [PDF 561 kb]
(703 Downloads)
| Abstract (HTML) (3886 Views)
Full-Text: (561 Views)
Introduction
Health professionals describe risk perception as gathering, choosing and interpreting information regarding the negative impacts of diseases and events [1]. Risk perception is a fundamental element for behavior change. When exposed to a dangerous situation, two cognitive assessments are created in the human mind: Efficacy and threat assessments. These reactions can determine an individual’s behavior [2]. Research shows that increased risk perception can lead to preventive preparedness against disasters, effective response strategies, and increased resilience [3]. Risk perception is influenced by socioeconomic factors, personality traits and cultural dimensions of communities, which can play an essential role in disaster preparedness and risk reduction [4].
The COVID-19 pandemic is a natural disaster that has had far-reaching effects on different sectors, including healthcare, the economy, and social dynamics. Since its emergence, this virus has had a devastating impact on the global population, resulting in more than 167 million infections and at least three million deaths worldwide [5]. Although all age groups in society are at risk of contracting COVID-19, older adults are often more vulnerable due to their high vulnerability rate and multiple concurrent illnesses. The findings of a study conducted in Italy indicate that the average age of people who died due to COVID-19 was 79 for men and 82 for women. The results of this research also suggested that the course of COVID-19 in older adults with chronic diseases was very severe [6].
One of these chronic conditions is diabetes in older adults [7]. Studies have estimated the prevalence of COVID-19 in older adults with diabetes to be 14.5%, which is still increasing [8]. Diabetes is one of the most common metabolic disorders in older adults. The prevalence of this disease is higher, especially in older women, and its side effects affect almost all aspects of older adults’ lives [9]. This condition is exacerbated by concurrent COVID-19 infection, such as increased mental disorders, namely depression, anxiety, and stress, which we are witnessing today in many patients with diabetes [10]. Many older adults are exposed to psychological threats during and after the pandemic, affected by home quarantine conditions, feelings of loneliness, and loss of loved ones [11]. These conditions have aggravated the psychological problems of these individuals, and they may experience various psychological complications such as depression, anxiety, severe nervous attacks, physical symptoms, nervous shocks and posttraumatic stress symptoms, delirium, psychosis, and even suicide attempts [12].
In this regard, Souza et al. (2021) investigated the mental health of individuals with diabetes during the COVID-19 pandemic. The findings of this study showed that 37.7%, 43.3% and 51.1% of patients had stress, anxiety, and depression, respectively. Additionally, being female, low income and education levels, loneliness, history of mental disorders, lack of physical activity, and smoking were among the factors that increased mental disorders in patients with diabetes [13]. Moreover, patients with diabetes may experience periods of low quality of life due to their limitations. The outbreak of COVID-19 and home quarantine led to reduced social connections and difficult access to doctors and medications in many patients with diabetes, resulting in disease recurrence and reduced quality of life for these patients [14]. In a separate study that investigated how the COVID-19 pandemic affected the quality of life for individuals with diabetes, it was discovered that stress and anxiety about contracting COVID-19 are significant factors contributing to a decline in the quality of life for many diabetic patients.
In contrast, awareness, social support, medical care, and physical activity increase the quality of life of patients with diabetes [15]. The quality of life for older adults can be easily compromised due to the deterioration in both physical and mental capabilities [16]. Consequently, it is crucial to identify and analyze factors that could enhance the quality of life for older adults, particularly during the COVID-19 pandemic [17]. Evidence indicates that engaging in protective behaviors, such as practicing good hygiene, utilizing masks and gloves, maintaining social distancing, avoiding unnecessary travel, and thoroughly washing hands with soap and water for at least 20 seconds, can significantly lower the risk of contracting COVID-19 and mitigate its effects [18]. However, following such protective and care programs requires individuals’ understanding of the risk of contracting the disease, which is an essential factor in people’s intention to adopt health behaviors [13].
Although we are now facing a significant reduction in mortality and risks compared to the peak of the COVID-19 outbreak, vulnerable groups, especially older adults with chronic diseases, are still at risk of contracting it and its consequences. Thus, considering what was discussed, older adults, particularly older women with diabetes, are at an increased risk of contracting this disease, which can lead to mental health disorders and a decline in quality of life. Evaluating the risk perception of COVID-19 in these individuals may aid in understanding their mental attitudes and subsequently facilitate educational interventions to promote behavior change. Therefore, the present study aimed to determine the relationship between COVID-19 risk perception and quality of life, stress, anxiety, and depression in older women with diabetes. Considering the high prevalence of diabetes and the aging population in Mazandaran Province, Iran, this research was conducted on older women with diabetes who visited health centers in Sari City, Mazandaran Province, in 2023.
Materials and Methods
Sample size and inclusion and exclusion criteria
The present study was a descriptive-analytical and correlational study conducted among older women with diabetes referring to Sari City (Iran) healthcare centers in 2023. The sample size of 250 (a 10% dropout rate was estimated) older adults was calculated based on Bastani et al.’s study [19] and using Equation 1:
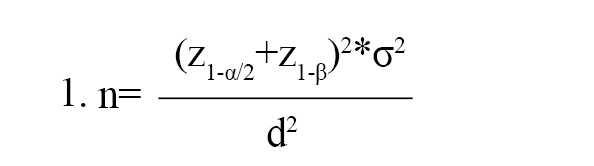
Considering the type 1 error of 5%, the power of 80%, and the measurement error d=2. The inclusion criteria for entering the study were as follows: Having diabetes (based on medical records), being a woman, being at least 60 years old, and lacking a history of known psychiatric disorders (such as depression, anxiety, etc.) based on individual’s statements, presenting medical documents and willingness to participate in the research, not contracting COVID-19 during the study period, not being hospitalized and providing informed consent. The exclusion criterion included not completing the questionnaire (>5%).
Recruitment
The sampling method in the present study was divided into two stages: cluster random sampling and simple random sampling. According to the distribution of the population, the healthcare centers of Sari City were divided into four clusters in four geographical directions (north, south, west and east) and according to the size of each cluster, several healthcare centers were randomly selected (cluster random sampling). Then, according to the population covered by each healthcare center, older women with diabetes were recruited in the research (simple random sampling). It is worth mentioning that if the selected older women did not meet the criteria for entering the research, the sampling continued until the desired sample size was reached.
Data collection and research instruments
Data collection was carried out through the use of questionnaires. Given the differing literacy levels among the elderly participants, the researcher directly asked the respondents questions.
The risk perception questionnaire of COVID-19
Developed by Jahangiry et al. (2020), the risk perception questionnaire of COVID-19 consists of 38 items divided into three subscales: Efficacy (self-efficacy and perceived response efficacy), defensive responses, and perceived threat. It was designed based on the parallel process model to assess risk perception related to COVID-19. The efficacy subscale includes 15 items that evaluate participants’ beliefs regarding their capability to implement recommended COVID-19 responses and the effectiveness of these preventive measures. The defensive responses subscale, which encompasses denial, reaction, and avoidance, contains 8 items measuring individuals’ perceptions of the risk of contracting COVID-19. The perceived threat dimension includes 8 items that assess beliefs about the severity and sensitivity of COVID-19 and the associated risk of infection. Responses are scored on a 5-point Likert scale ranging from completely disagree (1 point) to completely agree (5 points). Lower scores reflect a reduced risk perception, while higher scores indicate an elevated risk perception. This questionnaire has demonstrated strong validity and reliability within Iranian society, with the Cronbach α coefficients ranging from 0.69 to 0.79, indicating acceptable internal consistency. Additionally, the reliability assessed through the intracluster correlation coefficient (ICC) among 195 Iranian participants yielded favorable results, ranging from 0.71 to 0.80 [20].
Depression anxiety and stress scale (21-item) (DASS-21)
Developed in 1995 by Parkitny et al. [21], DASS-21 consists of 21 items that evaluate each of the psychological constructs of “depression,” “anxiety” and “stress,” with 7 items [21]. This scale measures the severity of the main symptoms of depression, anxiety and stress. The final score of each subscale is obtained through the sum of the scores of the related questions. Responses range from “never” to “always.” For each option (never, little, sometimes, and always), a score of 1, 2, or 3 is assigned. The sum of the accumulated scores is interpreted as normal anxiety, depression, and stress up to a very severe level. This questionnaire has been validated by Sahibi et al. [22] for the Iranian population. The Cronbach α was reported as 0.94 for depression, 0.92 for anxiety and 0.82 for stress [22]. In the present study, the Cronbach α coefficients for the subscales of anxiety, depression, and stress were obtained as 0.75, 0.70 and 0.75, respectively. At the same time, the overall scale yielded a coefficient of 0.90, indicating the high reliability of the instrument.
Diabetes quality of life (DQOL) questionnaire
The DQOL was developed by Thomas and evaluates the quality of life of type 1 and 2 diabetic patients. This 60-item questionnaire was shortened to a 15-item questionnaire by Burroughs [23]. The items in this questionnaire relate to patient care behaviors and satisfaction regarding disease management. It employs a 5-point Likert scale for scoring, ranging from entirely dissatisfied (1 point) to completely satisfied (5 points). The minimum possible score is 15, while the maximum is 75. Higher scores reflect a better quality of life, whereas lower scores indicate a diminished quality of life. Specifically, a score between 0 and 18 signifies minimal quality of life, 19 to 37 indicates poor quality, 38 to 56 represents average quality, and 57 to 75 denotes good quality [24]. The internal consistency and the Cronbach α coefficient for the Iranian version of this tool was 0.77, which shows its appropriate validity in Iranian society [25].
Sociodemographic and clinical characteristics
Participants completed a questionnaire that included sociodemographic and clinical characteristics, such as gender, marital status, economic status, education level, occupational status, living arrangements, medical conditions, smoking and alcohol history, as well as a history of drug addiction.
Statistical analysis
In this study, SPSS software, version 24 was used to classify and analyze the data. Data were described using descriptive statistics, including frequency distribution table, Mean±SD. The Kolmogorov-Smirnov statistical test was used to determine the normal distribution of the data. According to the normal distribution of data (P≤0.05), parametric tests, analysis of variance (comparing the mean of more than two groups), and the Pearson correlation (relationship between two quantitative variables) were used. In addition, multiple linear regression was used to investigate the simultaneous relationship of variables with stress, depression, anxiety and quality of life. A significance level of <0.05 was considered significant.
Results
Participants characteristics
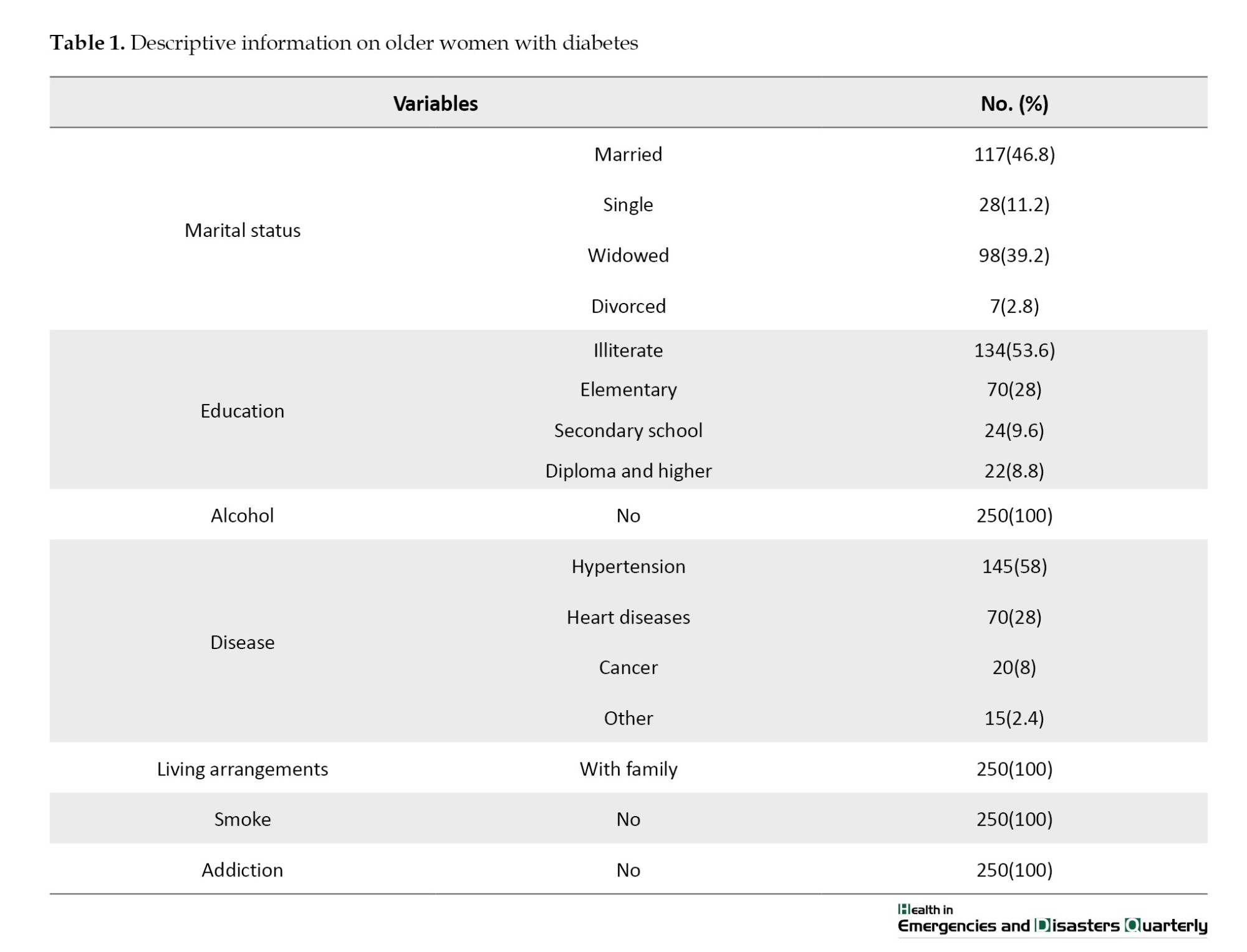
A total of 250 individuals participated in this study. Participants had a mean age of 67.04±6.26 years. Most of them were married (46.8%), illiterate (53.6%) and suffering from high blood pressure (58%). Other demographic information of the participants is shown in Table 1.
The mean quality of life score for older women with diabetes was 54.05±7.76, at an average level. Table 2 shows other research variables’ Mean±SD and their correlation using the Pearson ICC test.
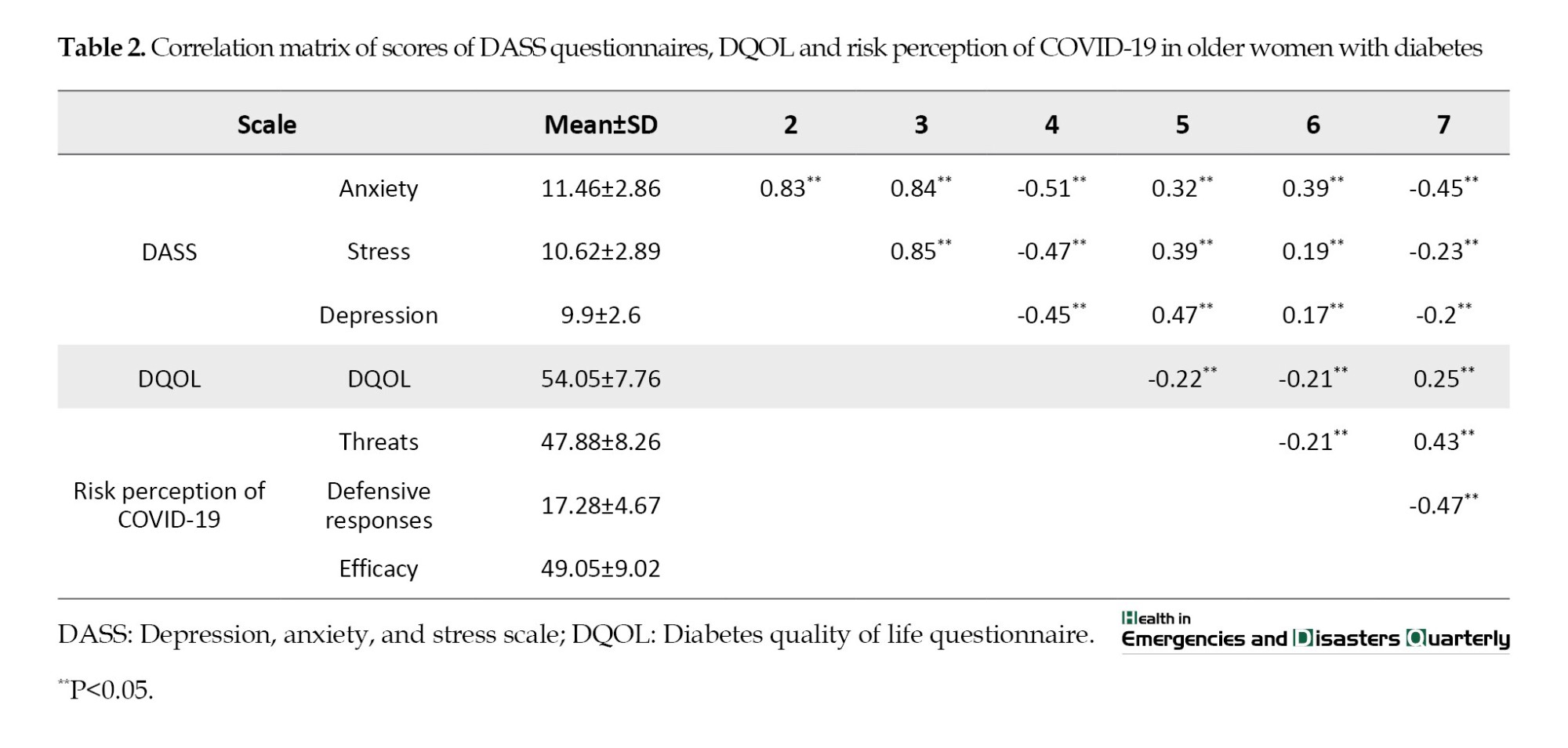
As can be seen, among the mental health conditions, the highest average belongs to anxiety, and among the dimensions of the risk perception of COVID-19, the efficacy dimension had an inverse and significant relationship with the anxiety of participants in the study (r=-0.45, P≤0.05). Furthermore, an inverse and statistically significant association was found between the quality of life, defensive responses and perceived threat dimensions. On the other hand, the relationship between efficacy and the quality of life of older adults was direct and significant, which means that people with more confidence in their ability to deal with COVID-19 had a better quality of life (P≤0.05).
The one-way variance analysis showed that participants’ mental health conditions (stress, anxiety, depression) and quality of life scores have significant differences based on demographic factors such as marital status, education level and type of chronic disease (P≤0.05). Consequently, the Scheffe test results show that divorced older women, compared to married ones and illiterate older women, compared to those literate and above, have the highest anxiety, stress, and depression scores and the lowest quality of life scores. Also, older women with cancer have the highest anxiety, stress and depression scores. Also, they have one of the lowest quality of life scores among other diseases.
Multiple linear regression analysis was used to investigate the relationship between the dimensions of the risk perception of COVID-19 and demographic variables with the scores of anxiety, stress, depression and quality of life of older women (Table 3). The findings show that the mean anxiety scores in divorced or unmarried older adults are 2.42 and 1.75 points higher than married ones, respectively. Compared to those without formal education, older adults with a middle school education and a diploma have lower anxiety scores. Compared to older women with high blood pressure, those with cancer experience a higher anxiety score, and older women with kidney problems experience a lower anxiety score. Anxiety score increases with higher age and threat score while drops with increasing efficacy score (P≤0.05).
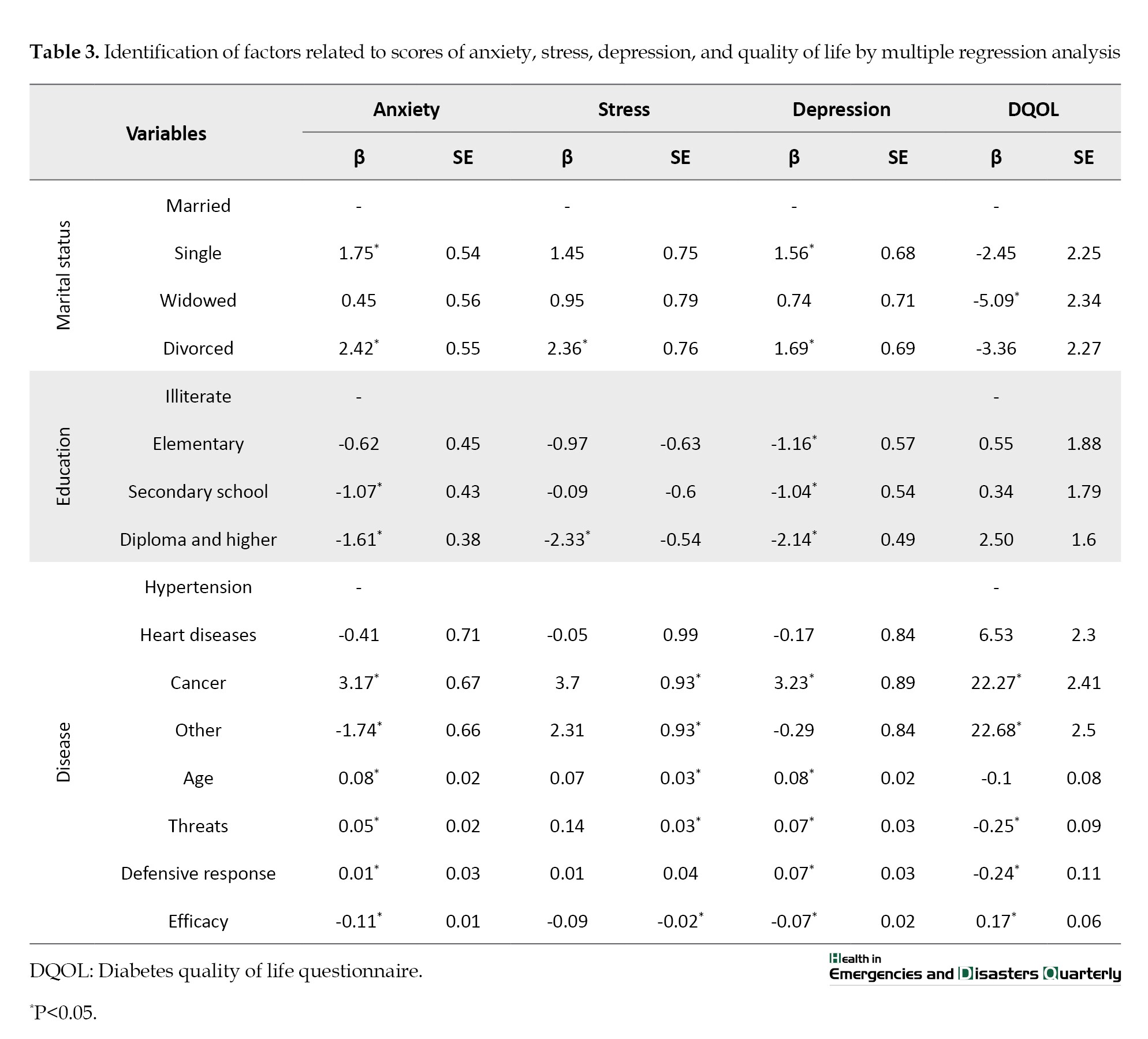
The mean stress score in divorced older adults was significantly higher (2.46 points) than in married ones. Compared to those without formal education, older women with diplomas have a stress score of 2.33 points lower (P≤0.05). Compared to older women with high blood pressure, those with cancer or kidney problems experience a higher stress score. Stress scores increase with old age and threat scores, while they drop with increasing efficacy scores (P≤0.05).
The mean depression scores in divorced and unmarried older adults are 1.69 and 1.56 points higher than married ones, respectively. With the increase in education, the depression score decreases significantly (P≤0.05). Compared to older women with hypertension, those with cancer experience more depression. Depression scores increase with increasing age and threat scores while dropping with increasing defensive response and efficacy scores (P≤0.05). Regarding the variable of quality of life, those who have lost their spouse experience a lower quality of life compared to older individuals who are still married.
The mean quality of life score in older women with heart diseases, cancer and kidney diseases is higher than those with high blood pressure. The research participants saw a decrease in their quality of life scores as their threat and defensive response scores grew. Conversely, an increase in their efficacy score significantly improved their quality of life score (P≤0.05).
Discussion
The present study was conducted to assess the relationship between the risk perception of COVID-19 and the quality of life and mental health conditions in older women with diabetes. A total of 250 older women with diabetes participated in the study. According to the study results, older women with diabetes had a slightly higher quality of life than the average. Additionally, individuals with higher levels of education and those who were married experienced better quality of life. In this regard, a study in Malaysia reports a high quality of life in diabetic older adults, which is not consistent with the results of the present study [26]. However, in one study conducted in Saudi Arabia, the quality of life of older adults with diabetes is reported as average, which aligns with the present study’s findings [27]. In general, by reviewing the previous studies and the findings of the present study, it can be concluded that the difference in the quality of life levels in older adults with diabetes can be influenced by socioeconomic status, age, education level, cultural and social factors, the availability of healthcare services and comorbidities. These factors can affect the mental experiences and general well-being of diabetic patients [27, 28]. Furthermore, the evidence indicates that gender inequalities in access to health care and the heightened susceptibility of women to physical and mental illnesses can have a detrimental impact on their quality of life. Therefore, attention should be paid to the quality of life of older women, especially those with chronic diseases such as diabetes [29].
According to the findings of this study, the scores of the mental health conditions of older diabetic women were at an average level. In the results of a study in Turkey, which was conducted on diabetic older adults during the period of COVID-19, the level of anxiety, stress and depression of the participants is reported to be higher than in the present study [30]. It seems that mental pressure, fear of virus infection, unknown nature of the disease, and quarantine of diabetic patients during the period of COVID-19 are among the reasons for the prevalence of mental disorders in this period, which has been mentioned in many studies [31, 32]. In the present study, older adults reported higher levels of anxiety compared to stress and depression. Also, in the results of studies conducted in Saudi Arabia and Iran, the prevalence of anxiety in diabetic older adults was higher than depression and stress. Factors such as marital status (being single), poor socioeconomic conditions, female gender and the presence of comorbidities are factors that aggravate mental distress (stress, depression and anxiety), which are consistent with the findings of the present study [33, 34]. In the results of other studies, it is also stated that anxiety is common among chronic diseases, especially in the field of diabetes, which can double the risk of anxiety [35].
Concerning the dimensions of risk perception of COVID-19, people with higher levels of efficacy (perceived self-efficacy and perceived response efficacy) suffer from less stress, depression, and anxiety and report a better quality of life. In the results of other studies, it has been stated that self-efficacy as a positive mental state reduces the level of anxiety, depression and stress [36, 37]. Self-efficacy can contribute to proactive behavior and the ability to engage in healthy behavior. Also, people with high self-efficacy can control their emotions better [20]. As a result, high self-efficacy can increase the ability to do different tasks and maintain personal health, resulting in better life quality [38]. In addition, based on the findings of this study, the perceived response efficacy scores also indicate that older adults with a positive assessment of the effectiveness of preventive measures in the field of preventing health measures report a lower level of anxiety, depression and stress, which is consistent with the results of a study conducted in China [39].
The findings of this study showed that threat (perceived sensitivity and severity) has a positive relationship with the levels of stress, depression, and anxiety in older adults. It means that older people with more fear about contracting COVID-19 and its consequences report more anxiety, depression and stress and have a lower quality of life. This research finding was also consistent with the results of two other studies from China and Poland [39, 40]. The results of studies have shown that the perceived threat of an epidemic can trigger people’s concern for their future and lead to experiencing negative perceptions about future consequences, resulting in uncertainty, fear, increasing vulnerability, and reducing the quality of people’s lives [41]. The findings of this research show that defensive responses (denial, reaction, and avoidance) about COVID-19 have a positive relationship with the level of stress, depression, and anxiety of the research participants and a negative relationship with the quality of life. In general, defense mechanisms are unconscious psychological strategies that people use to protect themselves from anxiety caused by unacceptable feelings or thoughts [42]. During COVID-19, perceived stress and tension caused by quarantine, social distancing, and other preventive measures related to the COVID-19 pandemic can stimulate psychological defense mechanisms [43]. It has been theorized that defensive responses to COVID-19 are probably immature because anxiety caused by COVID-19 can be temporarily relieved by ideas such as distortion of external reality [44]. The results of other studies also state that a reaction such as denial is an ineffective coping technique for issues associated with a chronic illness and may affect treatment adherence, especially in the field of diabetes and COVID-19, which can have serious consequences [45, 46]. For this reason, the findings of the present study also show that defensive responses are associated with increased levels of anxiety, stress and depression and decreased quality of life.
Conclusion
The results of this study demonstrate how psychological factors related to the perception of COVID-19 risk can impact mental health conditions and quality of life in older women with diabetes. Factors such as self-efficacy and perceived response efficacy in addressing COVID-19 risks are directly associated with reduced levels of stress, anxiety, and depression, as well as improved quality of life in this population. Conversely, defensive responses and perceived threats related to COVID-19 are linked to increased stress, anxiety, depression, and decreased quality of life. Therefore, it is essential to implement appropriate coping strategies to enhance older adults’ self-efficacy in crises like COVID-19. Additionally, efforts should be made to reduce defensive responses and perceived threats associated with such crises. Educational and counseling interventions can help individuals identify and improve effective coping strategies while boosting their self-efficacy.
Furthermore, raising awareness and providing accurate, evidence-based information about the real risks associated with crises can help mitigate over-perceived threats. Given the potential emergence of new and re-emerging diseases, health systems must pay special attention to the mental health of vulnerable populations. The findings from this study provide valuable insights for designing supportive interventions and health policies aimed at improving the mental health and quality of life of older adults with diabetes during critical situations such as the COVID-19 pandemic. This research also emphasizes that during crises, prioritizing mental health care is vital to prevent the onset of more severe issues.
Study limitations
The current study was cross-sectional, so it was impossible to investigate the causal relationship between the study variables. In this research, some questionnaires were used so that the data may be influenced by social desirability bias, recall error, and dishonesty. In addition, the limitations of similar studies made it less possible to compare the findings.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.REC.1401.536) and was conducted following health protocols related to COVID-19. The purpose of the study was communicated to older adults and their companions, who were assured that their information would be kept confidential. Subsequently, both verbal and written informed consent was obtained from them to participate in the study.
Funding
This study was financially supported by Mazandaran University of Medical Sciences, Sari, Iran (Code: 536).
Authors' contributions
Study design and data analysis: Shahab Papi and Abolfaz Hosseinnataj; Data collection: Farzaneh Naseri, Vahideh Rezapour, and Mohammadreza Alizadeh; Writing the original draft: Abdolhakim Jorbonyan and Hadi Najafi; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors of this article would like to thank all the people who participated in this research, especially older women with diabetes.
References
Health professionals describe risk perception as gathering, choosing and interpreting information regarding the negative impacts of diseases and events [1]. Risk perception is a fundamental element for behavior change. When exposed to a dangerous situation, two cognitive assessments are created in the human mind: Efficacy and threat assessments. These reactions can determine an individual’s behavior [2]. Research shows that increased risk perception can lead to preventive preparedness against disasters, effective response strategies, and increased resilience [3]. Risk perception is influenced by socioeconomic factors, personality traits and cultural dimensions of communities, which can play an essential role in disaster preparedness and risk reduction [4].
The COVID-19 pandemic is a natural disaster that has had far-reaching effects on different sectors, including healthcare, the economy, and social dynamics. Since its emergence, this virus has had a devastating impact on the global population, resulting in more than 167 million infections and at least three million deaths worldwide [5]. Although all age groups in society are at risk of contracting COVID-19, older adults are often more vulnerable due to their high vulnerability rate and multiple concurrent illnesses. The findings of a study conducted in Italy indicate that the average age of people who died due to COVID-19 was 79 for men and 82 for women. The results of this research also suggested that the course of COVID-19 in older adults with chronic diseases was very severe [6].
One of these chronic conditions is diabetes in older adults [7]. Studies have estimated the prevalence of COVID-19 in older adults with diabetes to be 14.5%, which is still increasing [8]. Diabetes is one of the most common metabolic disorders in older adults. The prevalence of this disease is higher, especially in older women, and its side effects affect almost all aspects of older adults’ lives [9]. This condition is exacerbated by concurrent COVID-19 infection, such as increased mental disorders, namely depression, anxiety, and stress, which we are witnessing today in many patients with diabetes [10]. Many older adults are exposed to psychological threats during and after the pandemic, affected by home quarantine conditions, feelings of loneliness, and loss of loved ones [11]. These conditions have aggravated the psychological problems of these individuals, and they may experience various psychological complications such as depression, anxiety, severe nervous attacks, physical symptoms, nervous shocks and posttraumatic stress symptoms, delirium, psychosis, and even suicide attempts [12].
In this regard, Souza et al. (2021) investigated the mental health of individuals with diabetes during the COVID-19 pandemic. The findings of this study showed that 37.7%, 43.3% and 51.1% of patients had stress, anxiety, and depression, respectively. Additionally, being female, low income and education levels, loneliness, history of mental disorders, lack of physical activity, and smoking were among the factors that increased mental disorders in patients with diabetes [13]. Moreover, patients with diabetes may experience periods of low quality of life due to their limitations. The outbreak of COVID-19 and home quarantine led to reduced social connections and difficult access to doctors and medications in many patients with diabetes, resulting in disease recurrence and reduced quality of life for these patients [14]. In a separate study that investigated how the COVID-19 pandemic affected the quality of life for individuals with diabetes, it was discovered that stress and anxiety about contracting COVID-19 are significant factors contributing to a decline in the quality of life for many diabetic patients.
In contrast, awareness, social support, medical care, and physical activity increase the quality of life of patients with diabetes [15]. The quality of life for older adults can be easily compromised due to the deterioration in both physical and mental capabilities [16]. Consequently, it is crucial to identify and analyze factors that could enhance the quality of life for older adults, particularly during the COVID-19 pandemic [17]. Evidence indicates that engaging in protective behaviors, such as practicing good hygiene, utilizing masks and gloves, maintaining social distancing, avoiding unnecessary travel, and thoroughly washing hands with soap and water for at least 20 seconds, can significantly lower the risk of contracting COVID-19 and mitigate its effects [18]. However, following such protective and care programs requires individuals’ understanding of the risk of contracting the disease, which is an essential factor in people’s intention to adopt health behaviors [13].
Although we are now facing a significant reduction in mortality and risks compared to the peak of the COVID-19 outbreak, vulnerable groups, especially older adults with chronic diseases, are still at risk of contracting it and its consequences. Thus, considering what was discussed, older adults, particularly older women with diabetes, are at an increased risk of contracting this disease, which can lead to mental health disorders and a decline in quality of life. Evaluating the risk perception of COVID-19 in these individuals may aid in understanding their mental attitudes and subsequently facilitate educational interventions to promote behavior change. Therefore, the present study aimed to determine the relationship between COVID-19 risk perception and quality of life, stress, anxiety, and depression in older women with diabetes. Considering the high prevalence of diabetes and the aging population in Mazandaran Province, Iran, this research was conducted on older women with diabetes who visited health centers in Sari City, Mazandaran Province, in 2023.
Materials and Methods
Sample size and inclusion and exclusion criteria
The present study was a descriptive-analytical and correlational study conducted among older women with diabetes referring to Sari City (Iran) healthcare centers in 2023. The sample size of 250 (a 10% dropout rate was estimated) older adults was calculated based on Bastani et al.’s study [19] and using Equation 1:
Considering the type 1 error of 5%, the power of 80%, and the measurement error d=2. The inclusion criteria for entering the study were as follows: Having diabetes (based on medical records), being a woman, being at least 60 years old, and lacking a history of known psychiatric disorders (such as depression, anxiety, etc.) based on individual’s statements, presenting medical documents and willingness to participate in the research, not contracting COVID-19 during the study period, not being hospitalized and providing informed consent. The exclusion criterion included not completing the questionnaire (>5%).
Recruitment
The sampling method in the present study was divided into two stages: cluster random sampling and simple random sampling. According to the distribution of the population, the healthcare centers of Sari City were divided into four clusters in four geographical directions (north, south, west and east) and according to the size of each cluster, several healthcare centers were randomly selected (cluster random sampling). Then, according to the population covered by each healthcare center, older women with diabetes were recruited in the research (simple random sampling). It is worth mentioning that if the selected older women did not meet the criteria for entering the research, the sampling continued until the desired sample size was reached.
Data collection and research instruments
Data collection was carried out through the use of questionnaires. Given the differing literacy levels among the elderly participants, the researcher directly asked the respondents questions.
The risk perception questionnaire of COVID-19
Developed by Jahangiry et al. (2020), the risk perception questionnaire of COVID-19 consists of 38 items divided into three subscales: Efficacy (self-efficacy and perceived response efficacy), defensive responses, and perceived threat. It was designed based on the parallel process model to assess risk perception related to COVID-19. The efficacy subscale includes 15 items that evaluate participants’ beliefs regarding their capability to implement recommended COVID-19 responses and the effectiveness of these preventive measures. The defensive responses subscale, which encompasses denial, reaction, and avoidance, contains 8 items measuring individuals’ perceptions of the risk of contracting COVID-19. The perceived threat dimension includes 8 items that assess beliefs about the severity and sensitivity of COVID-19 and the associated risk of infection. Responses are scored on a 5-point Likert scale ranging from completely disagree (1 point) to completely agree (5 points). Lower scores reflect a reduced risk perception, while higher scores indicate an elevated risk perception. This questionnaire has demonstrated strong validity and reliability within Iranian society, with the Cronbach α coefficients ranging from 0.69 to 0.79, indicating acceptable internal consistency. Additionally, the reliability assessed through the intracluster correlation coefficient (ICC) among 195 Iranian participants yielded favorable results, ranging from 0.71 to 0.80 [20].
Depression anxiety and stress scale (21-item) (DASS-21)
Developed in 1995 by Parkitny et al. [21], DASS-21 consists of 21 items that evaluate each of the psychological constructs of “depression,” “anxiety” and “stress,” with 7 items [21]. This scale measures the severity of the main symptoms of depression, anxiety and stress. The final score of each subscale is obtained through the sum of the scores of the related questions. Responses range from “never” to “always.” For each option (never, little, sometimes, and always), a score of 1, 2, or 3 is assigned. The sum of the accumulated scores is interpreted as normal anxiety, depression, and stress up to a very severe level. This questionnaire has been validated by Sahibi et al. [22] for the Iranian population. The Cronbach α was reported as 0.94 for depression, 0.92 for anxiety and 0.82 for stress [22]. In the present study, the Cronbach α coefficients for the subscales of anxiety, depression, and stress were obtained as 0.75, 0.70 and 0.75, respectively. At the same time, the overall scale yielded a coefficient of 0.90, indicating the high reliability of the instrument.
Diabetes quality of life (DQOL) questionnaire
The DQOL was developed by Thomas and evaluates the quality of life of type 1 and 2 diabetic patients. This 60-item questionnaire was shortened to a 15-item questionnaire by Burroughs [23]. The items in this questionnaire relate to patient care behaviors and satisfaction regarding disease management. It employs a 5-point Likert scale for scoring, ranging from entirely dissatisfied (1 point) to completely satisfied (5 points). The minimum possible score is 15, while the maximum is 75. Higher scores reflect a better quality of life, whereas lower scores indicate a diminished quality of life. Specifically, a score between 0 and 18 signifies minimal quality of life, 19 to 37 indicates poor quality, 38 to 56 represents average quality, and 57 to 75 denotes good quality [24]. The internal consistency and the Cronbach α coefficient for the Iranian version of this tool was 0.77, which shows its appropriate validity in Iranian society [25].
Sociodemographic and clinical characteristics
Participants completed a questionnaire that included sociodemographic and clinical characteristics, such as gender, marital status, economic status, education level, occupational status, living arrangements, medical conditions, smoking and alcohol history, as well as a history of drug addiction.
Statistical analysis
In this study, SPSS software, version 24 was used to classify and analyze the data. Data were described using descriptive statistics, including frequency distribution table, Mean±SD. The Kolmogorov-Smirnov statistical test was used to determine the normal distribution of the data. According to the normal distribution of data (P≤0.05), parametric tests, analysis of variance (comparing the mean of more than two groups), and the Pearson correlation (relationship between two quantitative variables) were used. In addition, multiple linear regression was used to investigate the simultaneous relationship of variables with stress, depression, anxiety and quality of life. A significance level of <0.05 was considered significant.
Results
Participants characteristics
A total of 250 individuals participated in this study. Participants had a mean age of 67.04±6.26 years. Most of them were married (46.8%), illiterate (53.6%) and suffering from high blood pressure (58%). Other demographic information of the participants is shown in Table 1.
The mean quality of life score for older women with diabetes was 54.05±7.76, at an average level. Table 2 shows other research variables’ Mean±SD and their correlation using the Pearson ICC test.
As can be seen, among the mental health conditions, the highest average belongs to anxiety, and among the dimensions of the risk perception of COVID-19, the efficacy dimension had an inverse and significant relationship with the anxiety of participants in the study (r=-0.45, P≤0.05). Furthermore, an inverse and statistically significant association was found between the quality of life, defensive responses and perceived threat dimensions. On the other hand, the relationship between efficacy and the quality of life of older adults was direct and significant, which means that people with more confidence in their ability to deal with COVID-19 had a better quality of life (P≤0.05).
The one-way variance analysis showed that participants’ mental health conditions (stress, anxiety, depression) and quality of life scores have significant differences based on demographic factors such as marital status, education level and type of chronic disease (P≤0.05). Consequently, the Scheffe test results show that divorced older women, compared to married ones and illiterate older women, compared to those literate and above, have the highest anxiety, stress, and depression scores and the lowest quality of life scores. Also, older women with cancer have the highest anxiety, stress and depression scores. Also, they have one of the lowest quality of life scores among other diseases.
Multiple linear regression analysis was used to investigate the relationship between the dimensions of the risk perception of COVID-19 and demographic variables with the scores of anxiety, stress, depression and quality of life of older women (Table 3). The findings show that the mean anxiety scores in divorced or unmarried older adults are 2.42 and 1.75 points higher than married ones, respectively. Compared to those without formal education, older adults with a middle school education and a diploma have lower anxiety scores. Compared to older women with high blood pressure, those with cancer experience a higher anxiety score, and older women with kidney problems experience a lower anxiety score. Anxiety score increases with higher age and threat score while drops with increasing efficacy score (P≤0.05).
The mean stress score in divorced older adults was significantly higher (2.46 points) than in married ones. Compared to those without formal education, older women with diplomas have a stress score of 2.33 points lower (P≤0.05). Compared to older women with high blood pressure, those with cancer or kidney problems experience a higher stress score. Stress scores increase with old age and threat scores, while they drop with increasing efficacy scores (P≤0.05).
The mean depression scores in divorced and unmarried older adults are 1.69 and 1.56 points higher than married ones, respectively. With the increase in education, the depression score decreases significantly (P≤0.05). Compared to older women with hypertension, those with cancer experience more depression. Depression scores increase with increasing age and threat scores while dropping with increasing defensive response and efficacy scores (P≤0.05). Regarding the variable of quality of life, those who have lost their spouse experience a lower quality of life compared to older individuals who are still married.
The mean quality of life score in older women with heart diseases, cancer and kidney diseases is higher than those with high blood pressure. The research participants saw a decrease in their quality of life scores as their threat and defensive response scores grew. Conversely, an increase in their efficacy score significantly improved their quality of life score (P≤0.05).
Discussion
The present study was conducted to assess the relationship between the risk perception of COVID-19 and the quality of life and mental health conditions in older women with diabetes. A total of 250 older women with diabetes participated in the study. According to the study results, older women with diabetes had a slightly higher quality of life than the average. Additionally, individuals with higher levels of education and those who were married experienced better quality of life. In this regard, a study in Malaysia reports a high quality of life in diabetic older adults, which is not consistent with the results of the present study [26]. However, in one study conducted in Saudi Arabia, the quality of life of older adults with diabetes is reported as average, which aligns with the present study’s findings [27]. In general, by reviewing the previous studies and the findings of the present study, it can be concluded that the difference in the quality of life levels in older adults with diabetes can be influenced by socioeconomic status, age, education level, cultural and social factors, the availability of healthcare services and comorbidities. These factors can affect the mental experiences and general well-being of diabetic patients [27, 28]. Furthermore, the evidence indicates that gender inequalities in access to health care and the heightened susceptibility of women to physical and mental illnesses can have a detrimental impact on their quality of life. Therefore, attention should be paid to the quality of life of older women, especially those with chronic diseases such as diabetes [29].
According to the findings of this study, the scores of the mental health conditions of older diabetic women were at an average level. In the results of a study in Turkey, which was conducted on diabetic older adults during the period of COVID-19, the level of anxiety, stress and depression of the participants is reported to be higher than in the present study [30]. It seems that mental pressure, fear of virus infection, unknown nature of the disease, and quarantine of diabetic patients during the period of COVID-19 are among the reasons for the prevalence of mental disorders in this period, which has been mentioned in many studies [31, 32]. In the present study, older adults reported higher levels of anxiety compared to stress and depression. Also, in the results of studies conducted in Saudi Arabia and Iran, the prevalence of anxiety in diabetic older adults was higher than depression and stress. Factors such as marital status (being single), poor socioeconomic conditions, female gender and the presence of comorbidities are factors that aggravate mental distress (stress, depression and anxiety), which are consistent with the findings of the present study [33, 34]. In the results of other studies, it is also stated that anxiety is common among chronic diseases, especially in the field of diabetes, which can double the risk of anxiety [35].
Concerning the dimensions of risk perception of COVID-19, people with higher levels of efficacy (perceived self-efficacy and perceived response efficacy) suffer from less stress, depression, and anxiety and report a better quality of life. In the results of other studies, it has been stated that self-efficacy as a positive mental state reduces the level of anxiety, depression and stress [36, 37]. Self-efficacy can contribute to proactive behavior and the ability to engage in healthy behavior. Also, people with high self-efficacy can control their emotions better [20]. As a result, high self-efficacy can increase the ability to do different tasks and maintain personal health, resulting in better life quality [38]. In addition, based on the findings of this study, the perceived response efficacy scores also indicate that older adults with a positive assessment of the effectiveness of preventive measures in the field of preventing health measures report a lower level of anxiety, depression and stress, which is consistent with the results of a study conducted in China [39].
The findings of this study showed that threat (perceived sensitivity and severity) has a positive relationship with the levels of stress, depression, and anxiety in older adults. It means that older people with more fear about contracting COVID-19 and its consequences report more anxiety, depression and stress and have a lower quality of life. This research finding was also consistent with the results of two other studies from China and Poland [39, 40]. The results of studies have shown that the perceived threat of an epidemic can trigger people’s concern for their future and lead to experiencing negative perceptions about future consequences, resulting in uncertainty, fear, increasing vulnerability, and reducing the quality of people’s lives [41]. The findings of this research show that defensive responses (denial, reaction, and avoidance) about COVID-19 have a positive relationship with the level of stress, depression, and anxiety of the research participants and a negative relationship with the quality of life. In general, defense mechanisms are unconscious psychological strategies that people use to protect themselves from anxiety caused by unacceptable feelings or thoughts [42]. During COVID-19, perceived stress and tension caused by quarantine, social distancing, and other preventive measures related to the COVID-19 pandemic can stimulate psychological defense mechanisms [43]. It has been theorized that defensive responses to COVID-19 are probably immature because anxiety caused by COVID-19 can be temporarily relieved by ideas such as distortion of external reality [44]. The results of other studies also state that a reaction such as denial is an ineffective coping technique for issues associated with a chronic illness and may affect treatment adherence, especially in the field of diabetes and COVID-19, which can have serious consequences [45, 46]. For this reason, the findings of the present study also show that defensive responses are associated with increased levels of anxiety, stress and depression and decreased quality of life.
Conclusion
The results of this study demonstrate how psychological factors related to the perception of COVID-19 risk can impact mental health conditions and quality of life in older women with diabetes. Factors such as self-efficacy and perceived response efficacy in addressing COVID-19 risks are directly associated with reduced levels of stress, anxiety, and depression, as well as improved quality of life in this population. Conversely, defensive responses and perceived threats related to COVID-19 are linked to increased stress, anxiety, depression, and decreased quality of life. Therefore, it is essential to implement appropriate coping strategies to enhance older adults’ self-efficacy in crises like COVID-19. Additionally, efforts should be made to reduce defensive responses and perceived threats associated with such crises. Educational and counseling interventions can help individuals identify and improve effective coping strategies while boosting their self-efficacy.
Furthermore, raising awareness and providing accurate, evidence-based information about the real risks associated with crises can help mitigate over-perceived threats. Given the potential emergence of new and re-emerging diseases, health systems must pay special attention to the mental health of vulnerable populations. The findings from this study provide valuable insights for designing supportive interventions and health policies aimed at improving the mental health and quality of life of older adults with diabetes during critical situations such as the COVID-19 pandemic. This research also emphasizes that during crises, prioritizing mental health care is vital to prevent the onset of more severe issues.
Study limitations
The current study was cross-sectional, so it was impossible to investigate the causal relationship between the study variables. In this research, some questionnaires were used so that the data may be influenced by social desirability bias, recall error, and dishonesty. In addition, the limitations of similar studies made it less possible to compare the findings.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.REC.1401.536) and was conducted following health protocols related to COVID-19. The purpose of the study was communicated to older adults and their companions, who were assured that their information would be kept confidential. Subsequently, both verbal and written informed consent was obtained from them to participate in the study.
Funding
This study was financially supported by Mazandaran University of Medical Sciences, Sari, Iran (Code: 536).
Authors' contributions
Study design and data analysis: Shahab Papi and Abolfaz Hosseinnataj; Data collection: Farzaneh Naseri, Vahideh Rezapour, and Mohammadreza Alizadeh; Writing the original draft: Abdolhakim Jorbonyan and Hadi Najafi; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors of this article would like to thank all the people who participated in this research, especially older women with diabetes.
References
- Cvetković VM, Radovanović MP, Milašinović SMJSp. Disaster risk communication: Attitudes of Serbian citizens. Sociološki pregled. 2021; 55(4):1610-47. [DOI:10.5937/socpreg55-34018]
- Papi S, Karimi Z, Zilaee M, Shahry P. Malnutrition and its relation to general health and multimorbidity in the older people. Journal of Holistic Nursing And Midwifery. 2019; 29(4):228-35. [DOI:10.32598/JHNM.29.4.228]
- Cai J, Hu S, Sun F, Tang L, Fan G, Xing H. Exploring the relationship between risk perception and public disaster mitigation behavior in geological hazard emergency management: A research study in Wenchuan county. Preventing Chronic Disease. 2023; 2:21. [DOI:10.20517/dpr.2023.26]
- Çelik İH, Kılıç TJDÜSBD. Disaster risk perception regarding culture and personality. Dumlupınar Üniversitesi Sosyal Bilimler Dergisi. 2023; (77):157-72. [DOI:10.51290/dpusbe.1264460]
- Papi S, Salimi M, Behboodi L, Dianat I, Jafarabadi M, Allahverdipour HJMRPM. Cognitive and balance performance of older adult women during COVID-19 pandemic quarantine: An ex post facto study. Przeglad Menopauzalny. 2022; 21(2):117-23. [DOI:10.5114/pm.2022.116976] [PMID]
- Kunz R, Minder M. COVID-19 pandemic: Palliative care for elderly and frail patients at home and in residential and nursing homes. Swiss Medical Weekly. 2020; 150(1314). [DOI:10.4414/smw.2020.20235] [PMID]
- Joensen L, Madsen K, Holm L, Nielsen K, Rod M, Petersen A, et al. Diabetes and COVID‐19: Psychosocial consequences of the COVID‐19 pandemic in people with diabetes in Denmark-what characterizes people with high levels of COVID‐19‐related worries? Diabetic Medicine. 2020; 37(7):1146-54. [DOI:10.1111/dme.14319] [PMID]
- Abdi A, Jalilian M, Sarbarzeh PA, Vlaisavljevic Z. Diabetes and COVID-19: A systematic review on the current evidences. Diabetes Research and Clinical Practice. 2020; 166:108347. [DOI:10.1016/j.diabres.2020.108347] [PMID]
- Mirzaei M, Rahmaninan M, Mirzaei M, Nadjarzadeh A. Epidemiology of diabetes mellitus, pre-diabetes, undiagnosed and uncontrolled diabetes in Central Iran: Results from Yazd health study. BMC Public Health. 2020; 20(1):1-9. [DOI:10.1186/s12889-020-8267-y] [PMID]
- Passanisi S, Pecoraro M, Pira F, Alibrandi A, Donia V, Lonia P, et al. Quarantine due to the COVID-19 pandemic from the perspective of pediatric patients with type 1 diabetes: A web-based survey. Frontiers in Pediatrics. 2020;8:491. [DOI:10.3389/fped.2020.00491] [PMID]
- Van Bortel T, Basnayake A, Wurie F, Jambai M, Koroma AS, Muana AT, et al. Psychosocial effects of an Ebola outbreak at individual, community and international levels. Bulletin of the World Health Organization. 2016; 94(3):210. [DOI:10.2471/BLT.15.158543] [PMID]
- Tucci V, Moukaddam N, Meadows J, Shah S, Galwankar SC, Kapur GB. The forgotten plague: Psychiatric manifestations of Ebola, Zika, and emerging infectious diseases. Journal of Global Infectious Diseases. 2017; 9(4):151. [DOI:10.4103/jgid.jgid_66_17] [PMID]
- Souza GFdA, Praciano GdAF, Ferreira Neto OdC, Paiva MC, Jesus RPFSd, Cordeiro ALN, et al. Factors associated with psychic symptomatology in diabetics during the COVID-19 pandemic. Revista Brasileira de Saúde Materno Infantil. 2021; 21(Suppl 1):177-86. [DOI:10.1590/1806-9304202100s100009]
- Gvozdanović Z, Farčić N, Šimić H, Buljanović V, Gvozdanović L, Katalinić S, et al. The impact of education, COVID-19 and risk factors on the quality of life in patients with type 2 diabetes. International Journal of Environmental Research and Public Health. 2021; 18(5):2332. [DOI:10.3390/ijerph18052332] [PMID]
- Alimehr M, Malayen S, Vafa FS, Tahmasebi MJ, Nikbina M, Doostifar K. The impact of coronavirus disease (COVID-19) on quality of life in diabetic patients. Clinical Diabetology. 2021; 10(3):237-42. [DOI:10.5603/DK.a2021.0024]
- Vahdani Nia MS, Goshtasebi A, Montazeri A, Maftoon F. [Health-related quality of life in an elderly population in Iran: A population-based study (Persian)]. Health Monitor Journal of the Iranian Institute for Health Sciences Research. 2005; 4(2):113-20. [Link]
- Der Sheng Sun HL, Yim HW, Won HS, Ko YH. The impact of sarcopenia on health-related quality of life in elderly people: Korean national health and nutrition examination survey. The Korean Journal of Internal Medicine. 2019; 34(4):877. [DOI:10.3904/kjim.2017.182] [PMID]
- Tavakoli A, Vahdat K, Keshavarz M. [Novel coronavirus disease 2019 (COVID-19): An emerging infectious disease in the 21st century (Persian)]. Iranian South Medical Journal. 2020; 22(6):432-50. [DOI:10.29252/ismj.22.6.432]
- Bastani F, Haghani H. [Perceived stress and fear of COVID-19 among the elderly referred to comprehensive health centers in Tehran, Iran (Persian)]. Iran Journal of Nursing. 2022; 35(136):134-49. [DOI:10.32598/ijn.35.2.256.16]
- Jahangiry L, Bakhtari F, Sohrabi Z, Reihani P, Samei S, Ponnet K, et al. Risk perception related to COVID-19 among the Iranian general population: An application of the extended parallel process model. BMC Public Health. 2020; 20(1):1571. [DOI:10.1186/s12889-020-09681-7] [PMID]
- Parkitny L, McAuley J. The Depression Anxiety Stress Scale (DASS). Journal of Physiotherapy. 2010; 56(3):204. [PMID]
- Sahebi A, Asghari MJ, Salari RS. [Validation of depression anxiety and stress scale (DASS-21) for an Iranian population( Persian)]. Developmental Psychology. 2005; 1(4):299-312. [Link]
- Burroughs TE, Desikan R, Waterman BM, Gilin D, McGill J. Development and validation of the diabetes quality of life brief clinical inventory. Diabetes Spectrum. 2004; 17(1):41-9. [DOI:10.2337/diaspect.17.1.41]
- Zanjani F, Mohammad Khan Kermanshahi S, Gholami Fesharaki M. [The effect of health promotion support program on quality of life in patients with type 2 diabetes (Persian)]. Qom University of Medical Sciences Journal. 2021; 15(4):296-305. [DOI:10.32598/qums.15.4.296]
- Nasihatkon A, Pishva A, Habibzadh F, Tabatabai M, Taher QashqaeiZadeh T, Hojjat F, et al. [Determine the reliability and validity of clinical summary quality of life of diabetic patients (DQOL) to Persian (Persian)]. Iranian Journal of Diabetes and Metabolism. 2012; 11(5):483-7. [Link]
- Rosli NA, Mazapuspavina MY, Ismail Z, Elkudssiah Ismail N. Relationship of self efficacy in medication understanding with quality of life among elderly with type 2 diabetes mellitus on polypharmacy in Malaysia. International Journal of Environmental Research and Public Health. 2022; 19(5):3031. [DOI:10.3390/ijerph19053031] [PMID]
- Abualhamael SA, Baig M, Alghamdi W, Gazzaz ZJ, Al-Hayani M, Bazi A. Quality of life, stress, anxiety and depression and associated factors among people with type 2 diabetes mellitus in Western region Saudi Arabia. Frontiers in Psychiatry. 2024; 14:1282249. [DOI:10.3389/fpsyt.2023.1282249] [PMID]
- Khunkaew S, Fernandez R, Sim J. Health-related quality of life among adults living with diabetic foot ulcers: A meta-analysis. Quality of Life Research. 2019; 28(6):1413-27. [DOI:10.1007/s11136-018-2082-2] [PMID]
- Borhaninezhad V, Kazazi L, Haghi M, Chehrehnegar N. [Quality of life and its related factors among elderly with diabetes (Persian)]. Salmand. 2016; 11(1):162-73. [DOI:10.21859/sija-1101162]
- Ersoy S, Pehlivan S, Doğan DA, Ateş M, Ersoy İH. The Coronavirus Anxiety Level of Elderly Individuals with Diabetes Mellitus and Associated Factors during the COVID-19 Pandemic. Turkish Journal of Internal Medicine. 2024; 6(1):38-50. [DOI:10.46310/tjim.1290771]
- Al-Ajlouni YA, Park SH, Alawa J, Shamaileh G, Bawab A, El-Sadr WM, et al. Anxiety and depressive symptoms are associated with poor sleep health during a period of COVID-19-induced nationwide lockdown: A cross-sectional analysis of adults in Jordan. BMJ open. 2020; 10(12):e041995. [DOI:10.1136/bmjopen-2020-041995] [PMID]
- Stanton R, To QG, Khalesi S, Williams SL, Alley SJ, Thwaite TL, et al. Depression, anxiety and stress during COVID-19: associations with changes in physical activity, sleep, tobacco and alcohol use in Australian adults. International Journal of Environmental Research and Public Health. 2020; 17(11):4065. [DOI:10.3390/ijerph17114065] [PMID]
- Alzahrani A, Alghamdi A, Alqarni T, Alshareef R, Alzahrani A. Prevalence and predictors of depression, anxiety, and stress symptoms among patients with type II diabetes attending primary healthcare centers in the western region of Saudi Arabia: A cross-sectional study. International journal of mental health systems. 2019; 13:48. [DOI:10.1186/s13033-019-0307-6] [PMID]
- Azadi A, Taghinezhad H, Bastami M, Bastami A. [The study amount of anxiety and depression among elderly diabetic patients referred to Shahid Mostafa Khomeini in Ilam and Shohada Ashayer Hospitals in Khoramabad 2015 (Persian)]. Iranian Journal of Nursing Research. 2016; 11(3):1-9. [Link]
- Young-Hyman D, de Groot M, Hill-Briggs F, Gonzalez JS, Hood K, Peyrot M. Erratum. Psychosocial care for people with diabetes: A position statement of the American diabetes association. Diabetes care 2016; 39: 2126-2140. Diabetes Care. 2017; 40(2):287. [DOI:10.2337/dc17-er02] [PMID]
- Ibuka Y, Chapman GB, Meyers LA, Li M, Galvani AP. The dynamics of risk perceptions and precautionary behavior in response to 2009 (H1N1) pandemic influenza. BMC Infectious Diseases. 2010; 10:296. [DOI:10.1186/1471-2334-10-296] [PMID]
- Commodari E. The role of sociodemographic and psychological variables on risk perception of the flu. Sage Open. 2017; 7(3):2158244017718890. [DOI:10.1177/2158244017718890] [PMID]
- Bagheri MJ, Asgharnejad Farid A, Nasrolahi B. [The relationship between self-efficacy and quality of life through the mediating role of psychological well-being in the Elderly (Persian)]. Aging Psychology. 2022; 8(1):54-39. [DOI:10.22126/jap.2022.7431.1602]
- Zhang W, Xiong S, Zheng Y, Wu J. Response efficacy and self-efficacy mediated the relationship between perceived threat and psychic anxiety among college students in the early stage of the COVID-19 pandemic. International Journal of Environmental Research and Public Health. 2022; 19(5):2832. [DOI:10.3390/ijerph19052832] [PMID]
- Cypryańska M, Nezlek JB. Anxiety as a mediator of relationships between perceptions of the threat of COVID-19 and coping behaviors during the onset of the pandemic in Poland. Plos One. 2020; 15(10):e0241464. [DOI:10.1371/journal.pone.0241464] [PMID]
- Paredes MR, Apaolaza V, Fernandez-Robin C, Hartmann P, Yañez-Martinez D. The impact of the COVID-19 pandemic on subjective mental well-being: The interplay of perceived threat, future anxiety and resilience. Personality and Individual Differences. 2021; 170:110455. [DOI:10.1016/j.paid.2020.110455] [PMID]
- Bailey R, Pico J. Defense mechanisms. Treasure Island :StatPearls Publishing; 2023. [Link]
- Marčinko D, Jakovljević M, Jakšić N, Bjedov S, Mindoljević Drakulić A. The importance of psychodynamic approach during COVID-19 pandemic. Psychiatria Danubina. 2020; 32(1):15-21. [DOI:10.24869/psyd.2020.15] [PMID]
- Walker G, McCabe T. Psychological defence mechanisms during the COVID-19 pandemic: A case series. The European journal of psychiatry. 2021; 35(1):41-5. [DOI:10.1016/j.ejpsy.2020.10.005] [PMID]
- Avazzadeh S, Gilani N, Jahangiry L. Predictors of fear control related to COVID-19 among older population: an investigation on COVID-19 risk perception and health related quality of life during the pandemic. Health and Quality of Life Outcomes. 2023; 21(1):79. [DOI:10.1186/s12955-023-02167-1] [PMID]
- Lovibond PF, Lovibond SH. Depression anxiety and stress scales. Behaviour Research and Therapy. 1995. [DOI:10.1037/t39835-000]
Type of article: Research |
Subject:
Elderly
Received: 2024/05/26 | Accepted: 2024/12/30 | Published: 2025/07/9
Received: 2024/05/26 | Accepted: 2024/12/30 | Published: 2025/07/9
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
