

Volume 10, Issue 4 (Summer 2025)
Health in Emergencies and Disasters Quarterly 2025, 10(4): 301-314 |
Back to browse issues page



Ethics code: IR.NKUMS.REC.1400.099
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Kamali N, Amini Z, Hatami S H, Khatib K, Mohammadi S. Musculoskeletal Disorders in Emergency Medical Services Staff: Predictors and Relationship With Occupational Stress. Health in Emergencies and Disasters Quarterly 2025; 10 (4) :301-314
URL: http://hdq.uswr.ac.ir/article-1-644-en.html
URL: http://hdq.uswr.ac.ir/article-1-644-en.html



1- Department of Operating Room, School of Allied Medical Sciences, North Khorasan University of Medical Sciences, Bojnourd, Iran.
2- Prehospital Emergency Center of North Khorasan Province, Bojnourd, Iran.
3- Student Research Committee, North Khorasan University of Medical Sciences, Bojnourd, Iran.
4- Department of Operating Room, Faculty of Allied Medical Sciences, Ilam University of Medical Sciences, Ilam, Iran. ,smohamadi91070@gmail.com
2- Prehospital Emergency Center of North Khorasan Province, Bojnourd, Iran.
3- Student Research Committee, North Khorasan University of Medical Sciences, Bojnourd, Iran.
4- Department of Operating Room, Faculty of Allied Medical Sciences, Ilam University of Medical Sciences, Ilam, Iran. ,
Keywords: Emergency medical technicians, Musculoskeletal disorders (MSD), Prehospital, Occupational stress, Job stress
Full-Text [PDF 545 kb]
(1712 Downloads)
| Abstract (HTML) (3549 Views)
Full-Text: (922 Views)
Introduction
Emergency medical services (EMS) staff, as a key group providing medical services to patients in emergencies, are exposed to various occupational risks, including musculoskeletal disorders (MSD), due to the nature of their work and job requirements [1, 2]. MSD is a primary factor of human and labor injuries that reduces productivity, increases disability and absenteeism in both developed and developing countries, and imposes a significant economic burden on governments and ministries of health [3].
Studies show that among medical service providers, EMS staff have the highest rate of early retirement, mostly due to musculoskeletal diseases [4]. In the investigation of a 12-month prevalence of injuries caused by occupational accidents among 2307 staff of prehospital EMS, the injury rate was reported as 15.61% [5]. According to a systematic review and meta-analysis, the prevalence of back pain in prehospital EMS personnel was 39.4% between 2000 and 2016, and its prevalence range was 0.9%-17.1% in different countries [6]. A recent review article found that the overall prevalence of skeletal disorders among EMS personnel was 56.52%. The prevalence rates in different body regions were as follows: The lower back (47.38%), upper back (35.15%), neck (31.19%), shoulder (30%), knee (27.07%), hand (20.70%), hip/thigh (19.48%), feet (19.11%) and elbow (17.36%) [7]. Ultimately, functional disability, expenditure on health and social resources, and reduced ability of individuals to work and participate in social life will be the consequences of MSD [8].
Research indicates that one-third of EMS staff suffer from a job-related injury at least once over 6 months [9]. Repetitive actions such as lifting objects, bending, turning, moving, and transporting patients, cardiopulmonary resuscitation, and even the type of shift work, along with psychological and psychosocial stress, are among the causes of MSD in this profession [10, 11].
Research evidence suggests that the risk of MSD is increased by exposure to psychosocial stressors [12]. Occupational stress is one of the essential work-related factors in EMS personnel, and it can be related to critical events during patient care. Hence, lack of support from superiors or colleagues, poor communication, organizational changes, salaries, wages and decreased or increased workforce put pressure on people, causing anxiety and worry in different professions [13, 14]. Occupational stress is an essential factor compromising the health of healthcare workers. Among job groups, healthcare employees have a higher rate of job stress; studies show that the organization and conditions of the work environment significantly impact the occurrence of job stress and MSD [15, 16]. The results of a review study indicate that exposure to occupational stress among prehospital emergency staff and a moderate level of job stress have been reported in some investigations, which require further attention [17].
Research indicates that the physical requirements of the work environment and the resulting workload, which are aspects of occupational stress, have a direct and indirect effect on musculoskeletal complaints; moreover, the psychosocial risk factors stemming from the dimensions of occupational stress are involved in the severity of MSD [18]. Based on the findings of a review study, occupational stress is the main factor of MSD in EMS personnel [1].
Considering what was discussed, the professional nature of medical emergencies and the difference in the geography of regions, the distances and dissimilarity of roads in various provinces of Iran for transfer of patients from various districts to treatment centers by prehospital EMS personnel, the present study was conducted to evaluate the prevalence of MSD, the predicting factors and relationship with occupational stress in EMS staff of Bojnourd.
Materials and Methods
Study population and sample
The present study investigated the frequency of MSD, the factors affecting them, and the relationship with occupational stress among prehospital EMS staff in 2022. The statistical population encompassed all the urban and road EMS employees of Bojnourd City and subordinate centers in Iran, including 6 urban bases, 5 road bases, 1 air ambulance and 1 dispatch and management center, which were selected by the census. It should be noted that the dispatch center in this province includes a telephone triage unit and an ambulance dispatch and management unit.
The inclusion criteria were at least 6 months of work record in prehospital EMS, absence of congenital musculoskeletal problems, lack of musculoskeletal problems caused by trauma or accidents unrelated to work, and no known neurological and mental diseases.
Data collection tools
Three questionnaires were used to collect information, namely demographic characteristics questionnaire, Nordic musculoskeletal questionnaire and occupational stress questionnaire:
1) Demographic characteristics include gender, age, marital status, work experience, education, field of study, workplace, regular exercise program, smoking, having a second job, and body mass index (BMI); 2) The Nordic musculoskeletal questionnaire identifies the prevalence of skeletal disorders in 9 areas of the body, including neck, shoulders, elbows, wrists/hands, upper back, lower back, one or both hips/thighs, one or both knees and one or both ankles/feet. This questionnaire, which is utilized to determine the prevalence of MSD, was designed and implemented in 1987 by Mokhtariniaet al. [19] at the Institute of Occupational Health in Nordic countries and is currently known as the Nordic questionnaire. In Iran, the validity and reliability of the questionnaire were reported at an acceptable level (more than 0.7) in research conducted by Mokhtarinia et al. [19]; 3) The occupational stress questionnaire comprises 46 questions and 4 dimensions (physical, occupational, group and organizational). This tool is based on a 4-point Likert scale where a score of 0 stands for never (no tension), and a score of 3 indicates the highest level of tension. To investigate occupational stress, the quartile statistical method was used, in which the overall and dimension scores are considered as follows:
1) Physical dimension: Low (<8), moderate (8-13) and high (>13); 2) Occupational dimension: Low (<29), moderate (29-46) and high (>46); 3) Group dimension: Low (<7), moderate (7-14) and high (>14); 4) Organizational dimension: Low (<18), moderate (18-26) and high (>26); 5) General level of occupational stress: Low (<61), moderate (61-94) and high (>94)
This questionnaire was developed by Danesh [20]. Since it was formulated for nurses working in the hospital, in Aghainejad’s study, the corresponding words were substituted, and the validity and reliability were examined. In this research, the Pearson correlation coefficient was 0.87. In addition, in terms of the validity of research, based on the Cronbach α, the internal validity values were 71%, 88%, 75% and 82% for physical, occupational, group and organizational dimensions, respectively [21]. In our study, the Aghainejad questionnaire was used, and the reliability of the occupational stress questionnaire was calculated using the Cronbach α of 0.96.
Data collection
After confirming the research title by obtaining permission from the Ethics Committee of North Khorasan University of Medical Sciences, the authorization letter was issued to 115 EMS security centers to coordinate with the base manager for the researcher’s reference to emergency bases as well as the 115 emergency communication and information centers to collect information. After coordinating the time to complete the questionnaires, the researcher visited the research environment. Then, the researcher introduced himself to the participants and explained the study’s purpose. Next, a questionnaire was provided to the staff if they expressed their desire and consent to participate. After receiving the necessary explanations about answering the questionnaires, the participants completed the questionnaires in the researcher’s presence. To reduce the effect of intervening factors in completing the questionnaires, the questionnaires were anonymous and the researcher provided sufficient and clear explanations for participants regarding the confidentiality of information and non-judgment regarding them.
Since the sampling method was a census, to reach all individuals and ensure that the individual completed the questionnaire, visits were made to the desired bases and centers during different work shifts. Therefore, the data collection took about a month.
Data analysis
The results of descriptive analysis were reported as frequency (percentage) for qualitative variables and as Mean±SD for quantitative variables. To investigate pairwise relationships, univariate logistic regression analysis was used based on the type of response variable, and multiple logistic regression analysis was employed to investigate the factors affecting each of the response variables by controlling the effect of other variables. This way, the target variable was considered dependent, and the other investigated variables were independent. All analyses were performed using SPSS software, version 26 statistical software. P<0.05 was considered to be statistically significant.
Results
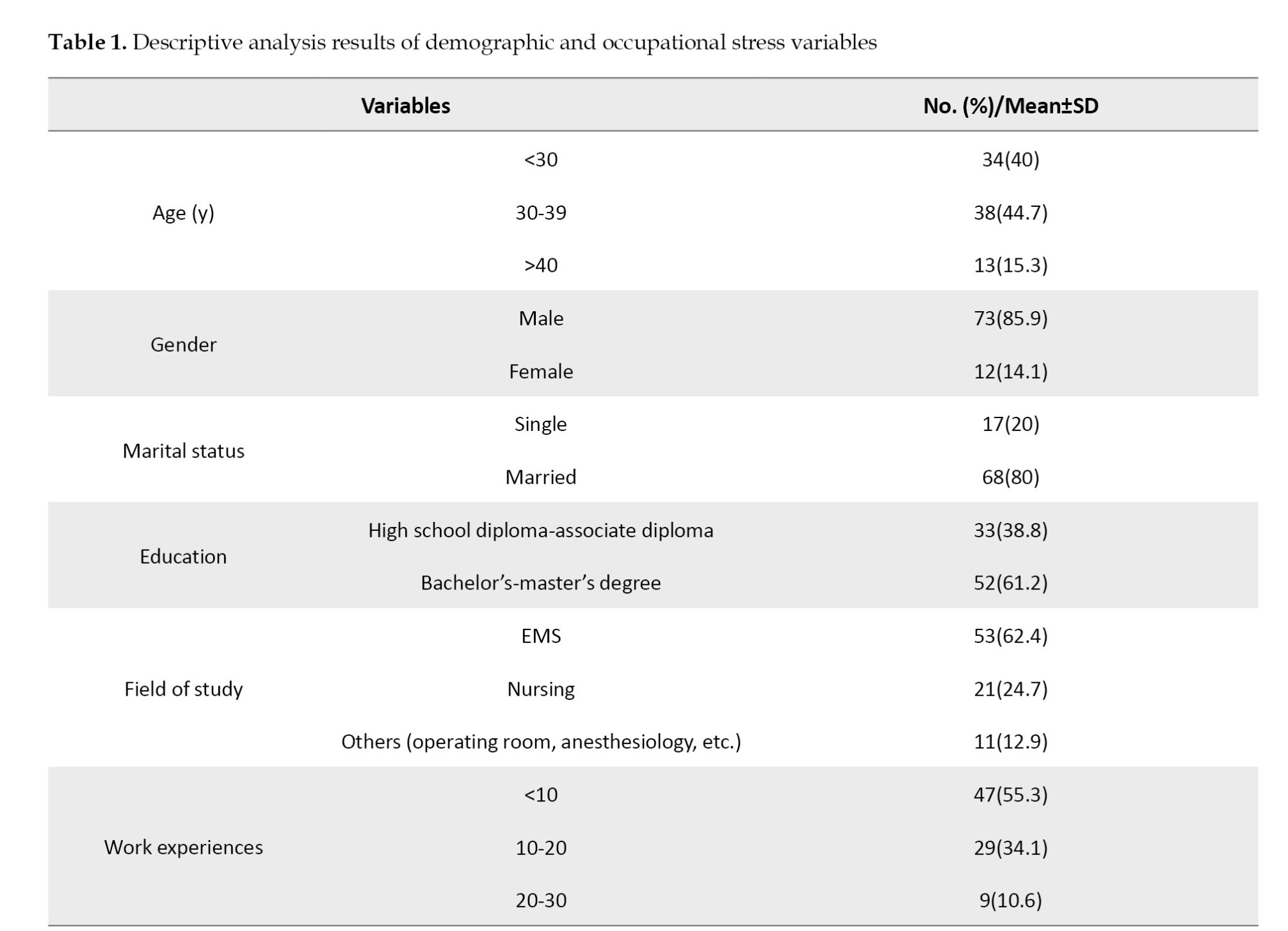
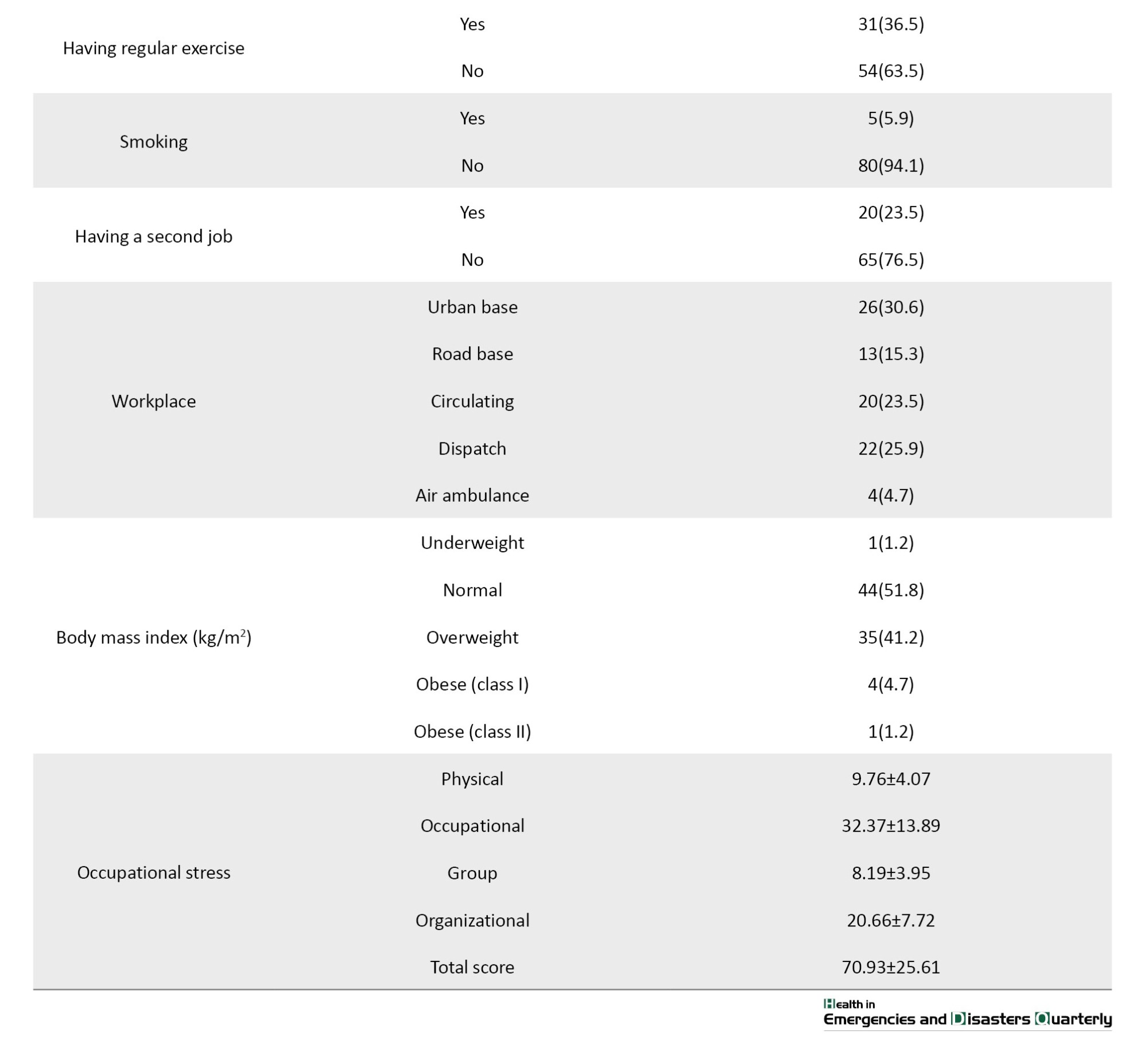
In the present study, 85 EMS staff participated with a mean age of 33.41±7.80 years (age range 24-60 years). Most participants were male (85.9%), married (80%) and held a degree in EMS (62.4%). The mean work experience of them was 9.41±7.03 years. The mean BMI was reported to be 25.03±3.55 kg/m2 and about half (51.8%) of the participants were in the normal BMI range. The overall score of occupational stress and all dimensions of the occupational stress questionnaire were moderate (Table 1).
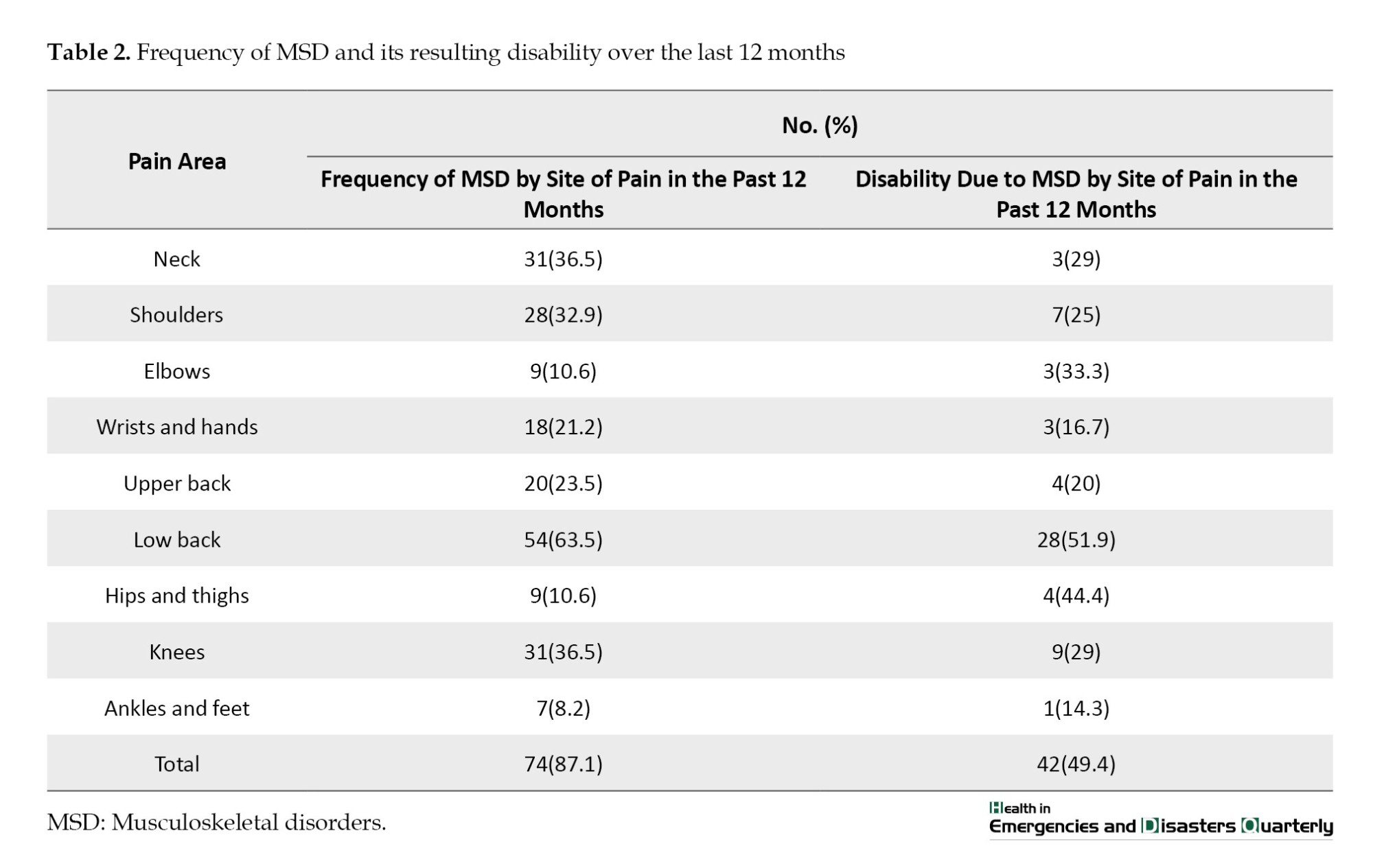
According to research results (Table 2), 87.1% of people in the present study suffered from MSD in at least one area of the body during the past year. The highest prevalence of symptoms was related to the lower back (63.5%), neck and knee (36.5%), shoulder (32.9%) and upper back (23.5%). In 49.4% of cases, people had to rest, reduce work activity, leave the workplace, or were unable to perform activities at work or home due to pain, discomfort, and disability caused by MSD in the past year.
Univariate logistic regression analysis was employed to investigate the relationship between demographic factors and the prevalence of MSD and the results are shown in Table 3.
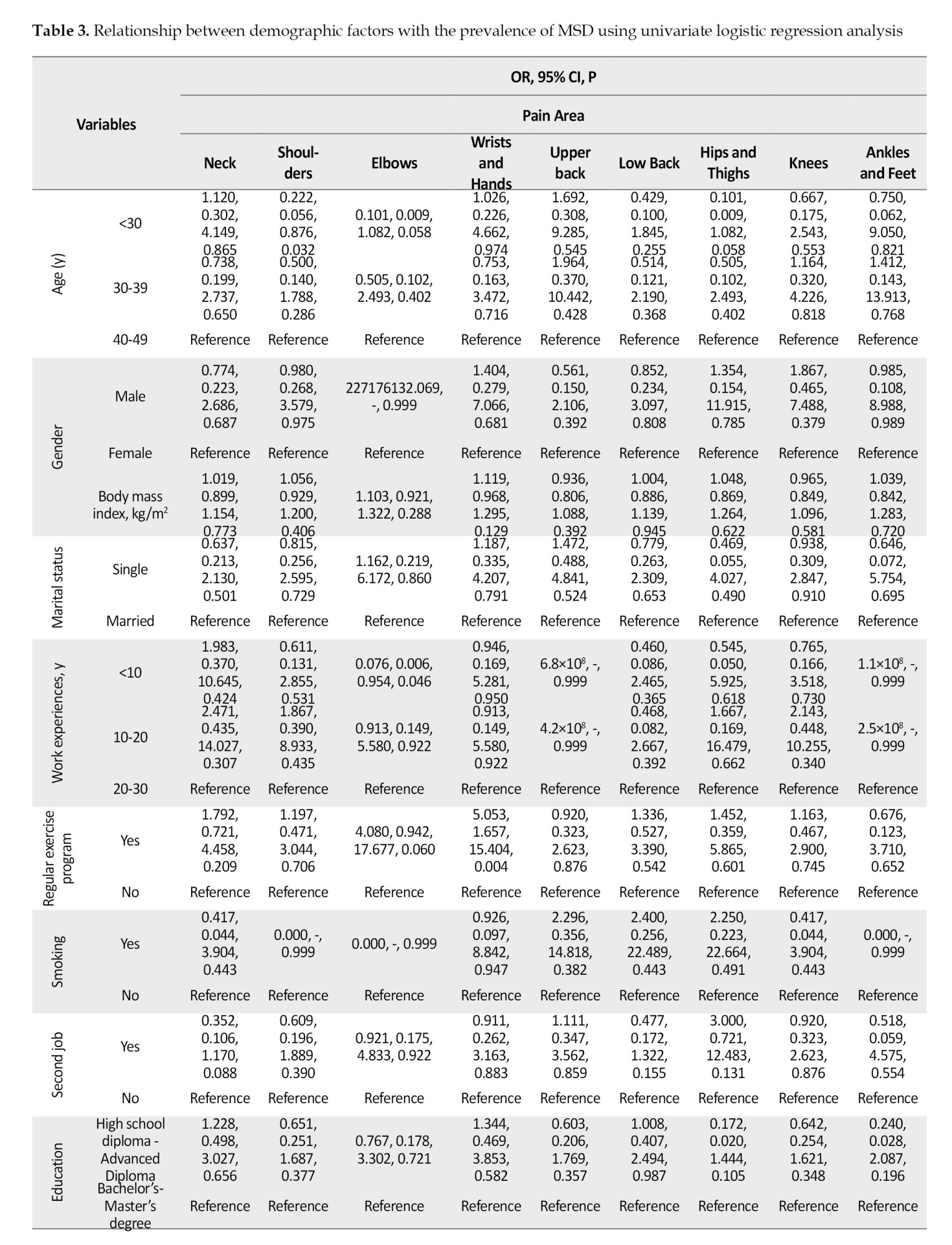
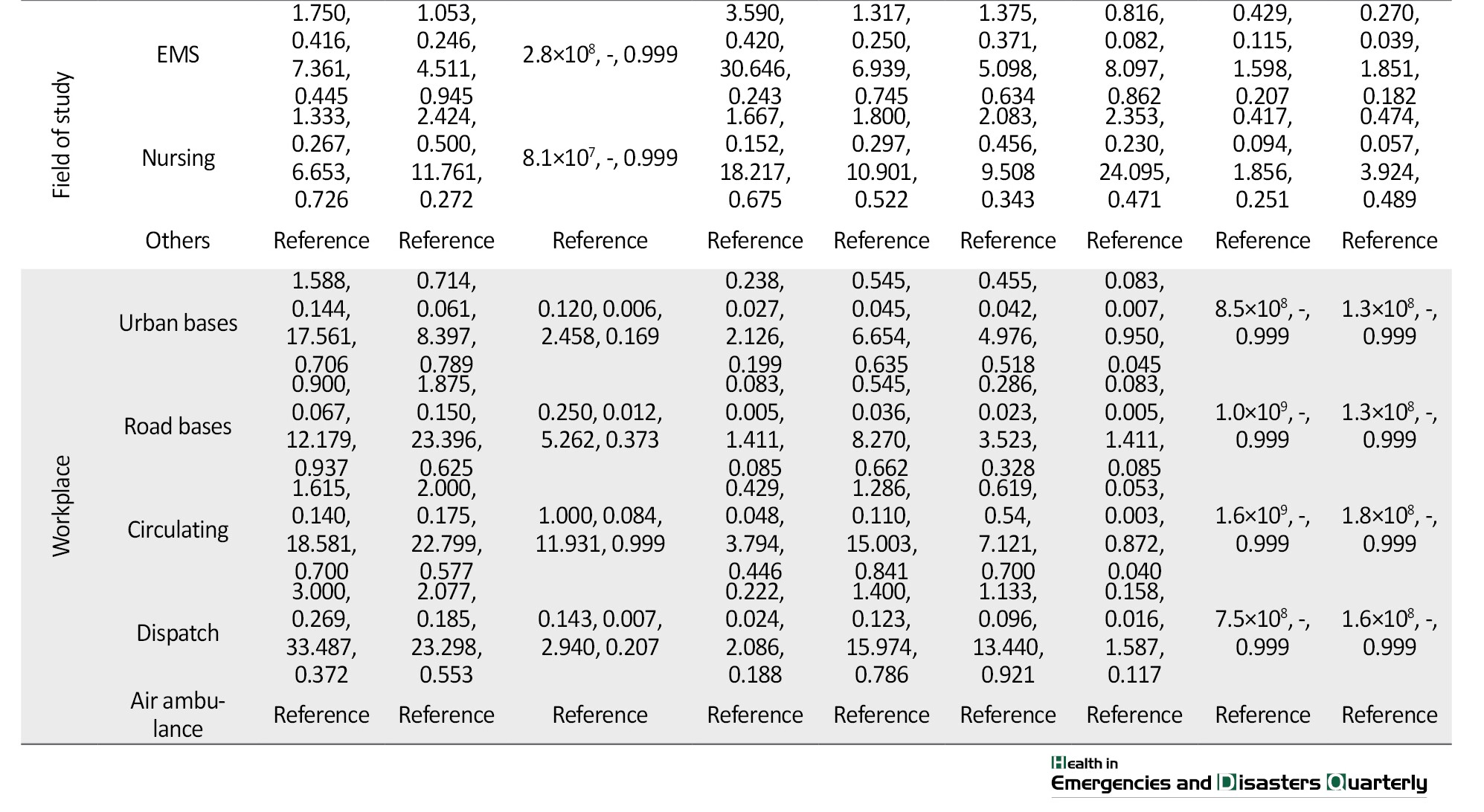
According to the results, none of the demographic variables significantly affected neck pain (P>0.05). The age variable had a significant impact on shoulder pain so that the chance of experiencing shoulder pain in people who were 40-49 years old was 4.50 times higher than those younger than 30 years (OR=0.222; 95% CI, 0.056%, 0.876%; P=0.032). The work experience variable had a significant effect on elbow pain so that the chance of experiencing elbow pain in those with 20-30 years of work experience was 13.16 times higher than in people whose work experience was <10 years (OR=0.076; 95% CI, 0.006%, 0.954%; P=0.046). The exercise variable significantly impacted wrist pain, so the chance of wrist pain in participants who exercised was 5.05 times higher than those who did not exercise (OR=5.053; 95% CI, 1.657%, 15.404%; P=0.004). The variable of the workplace had a significant effect on hip and thigh pain so that the chance of experiencing hip and thigh pain was 12.05 times higher in people whose workplace was in an air ambulance than in those working in an urban base (OR=0.083; 95% CI, 0.007%, 0.950%; P=0.045). Moreover, the likelihood of hip and thigh pain was 18.87 times higher in participants working in an air ambulance relative to those with a circulating workplace (OR=0.053, 95% CI, 0.003%, 0.872%; P=0.040). Further details are presented in Table 3.
Univariate logistic regression analysis was employed to investigate the relationship between occupational stress and the prevalence of MSD, as shown in Table 4.
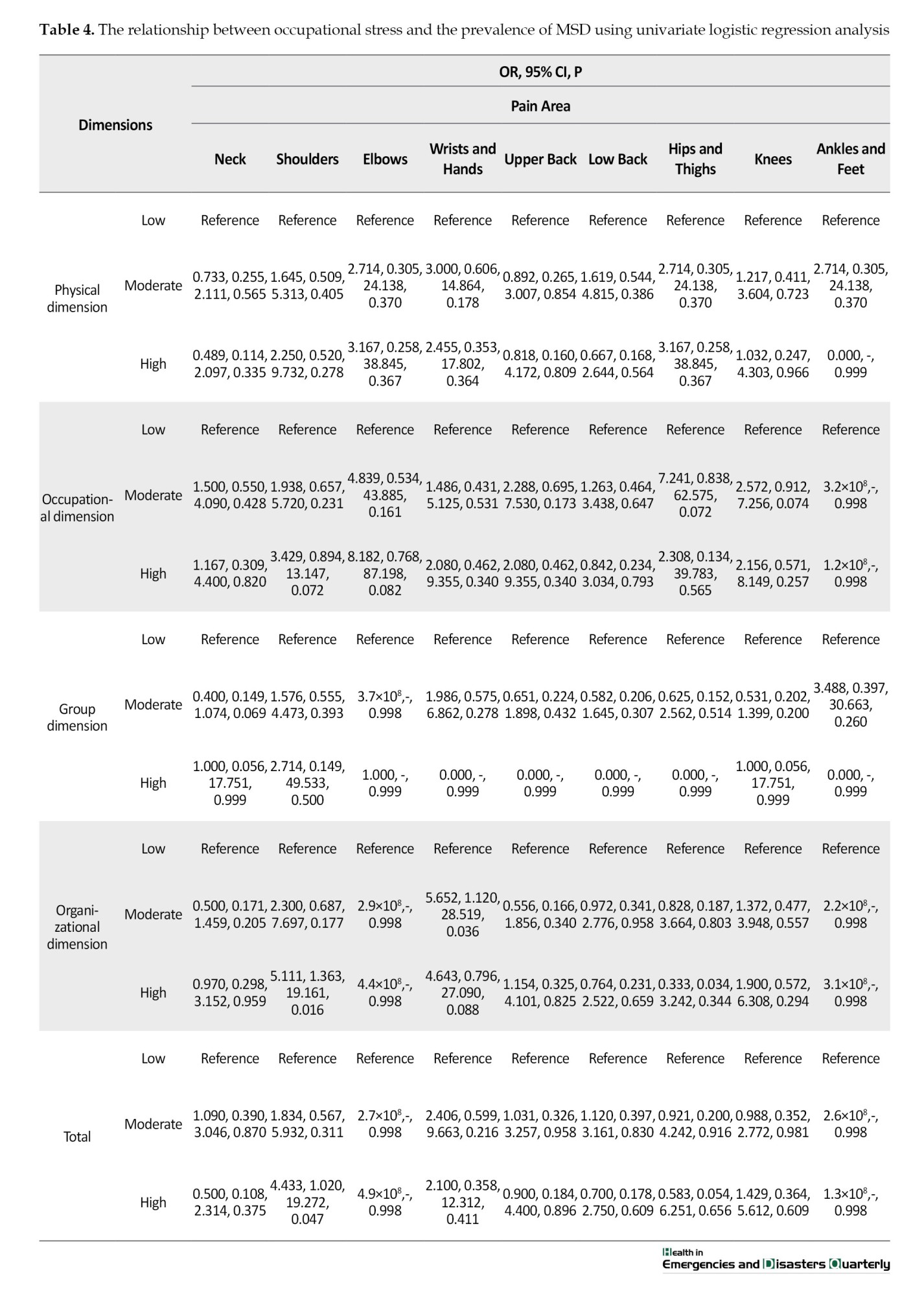
According to the results of univariate regression analysis, the chance of experiencing shoulder pain in people with high organizational stress was 5.11 times higher than in those with low organizational stress (OR=5.111; 95% CI, 1.363%, 19.161%; P=0.016), which was 4.43 times higher in people who in general had a high-stress level than those with a low-stress level (OR=4.433; 95% CI, 1.020%, 19.272%; P=0.047). The chance of experiencing wrist pain was 5.65 times higher in participants with moderate organizational stress (OR=5.652; 95% CI, 1.120%, 28.519%; P=0.036). The details are shown in Table 4.
To examine and control the effect of possible confounding variables more closely, demographic variables and dimensions of occupational stress whose impact on the prevalence of each MSD was significant at P<0.2 level were subject to multiple logistic regression tests, as shown in Table 5.
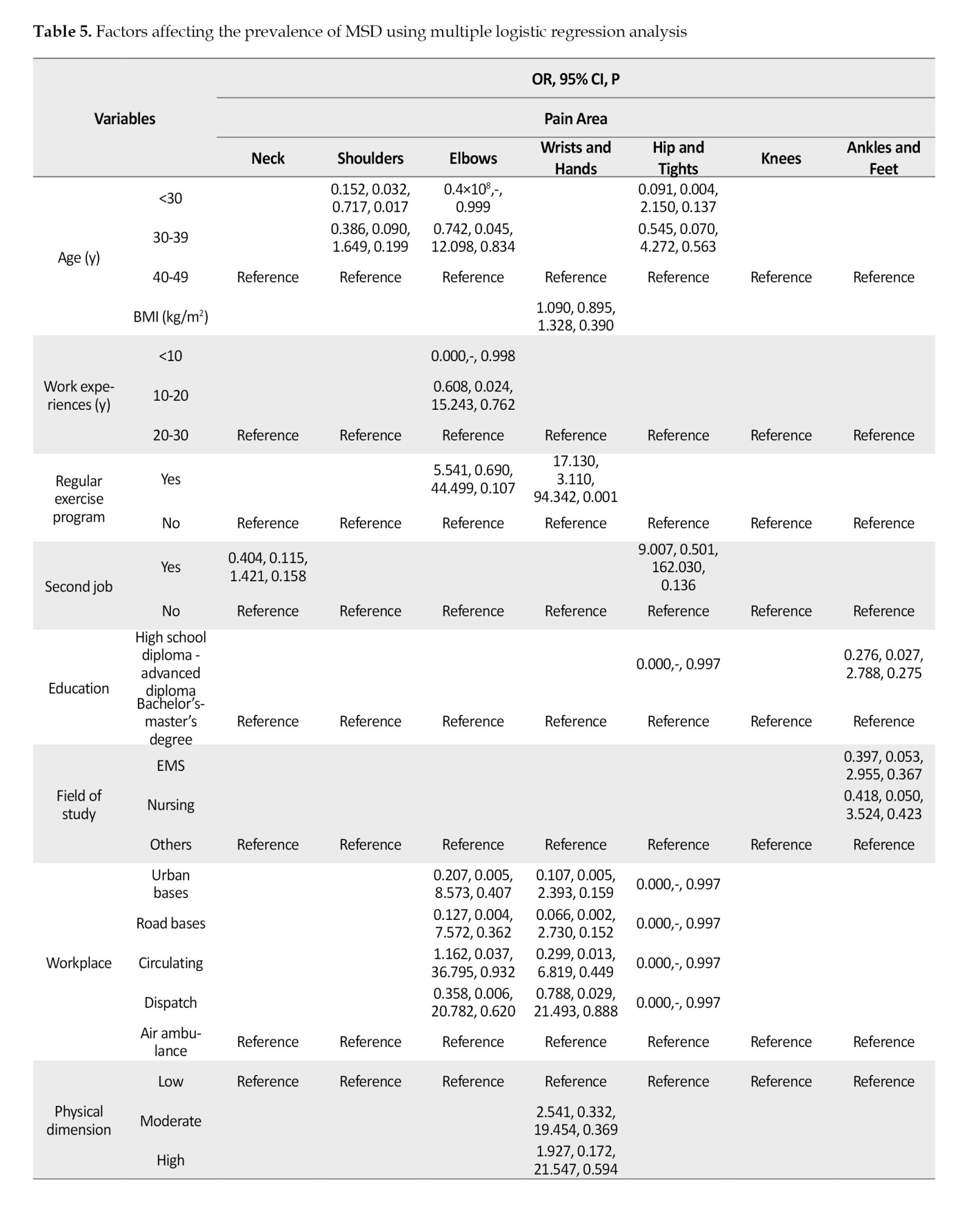
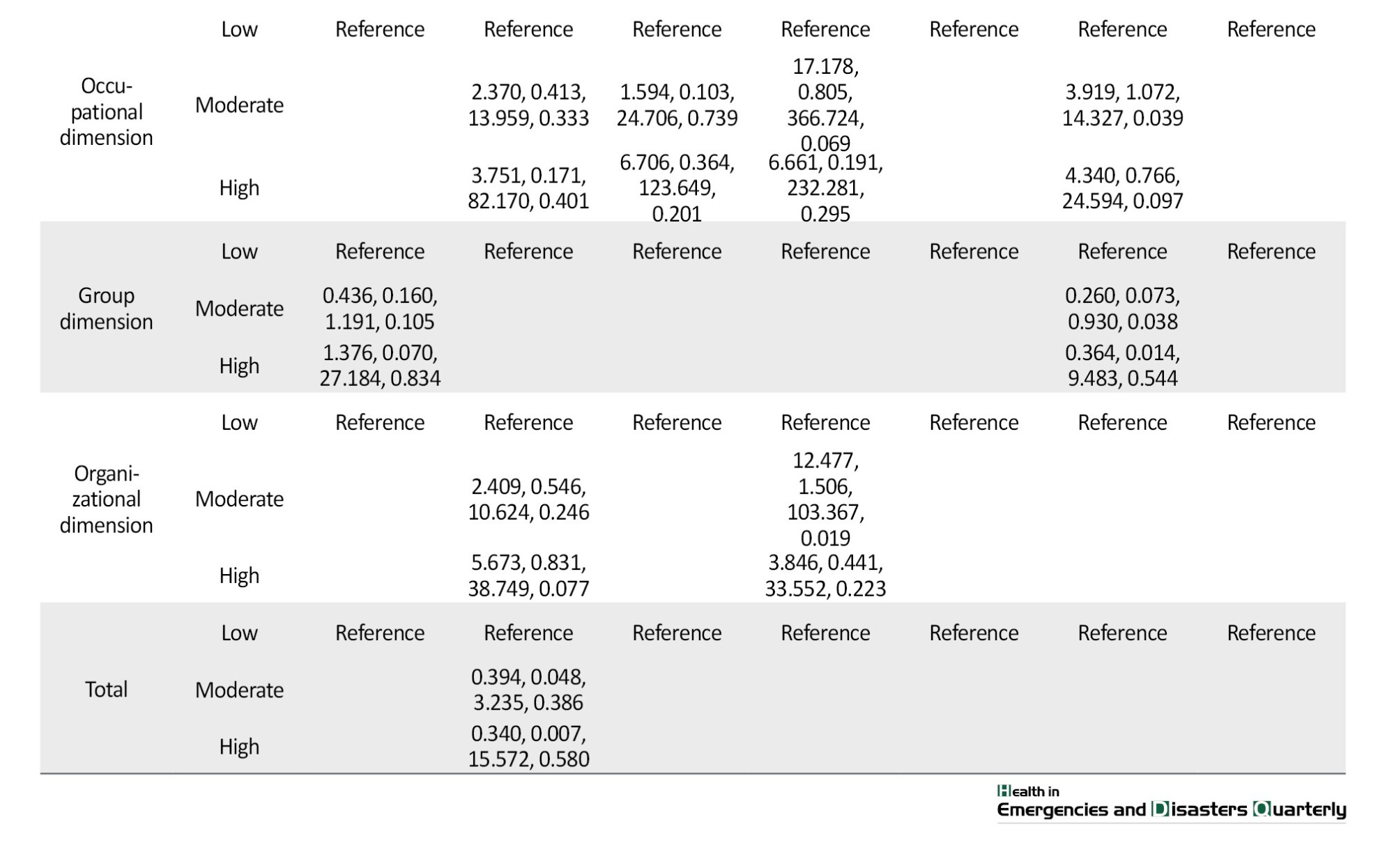
According to the obtained results, the age variable significantly impacted the prevalence of shoulder pain by controlling the effect of other variables. Hence, people 40-49 years old had a 5.6 times higher chance of experiencing shoulder pain than those younger than 30 (OR=0.152; 95% CI, 0.032%, 0.717%; P=0.017). By controlling the effect of other variables, the variables of exercise and organizational stress had a significant effect on the prevalence of wrist pain, so that people who exercised had 17.13 times more chance of experiencing wrist pain than those who did not exercise (OR=17.130; 95% CI, 3.110%; 94.342%; P=0.001). In addition, people with moderate organizational stress had a 12.48 times higher chance of experiencing wrist pain than those with low organizational stress (OR=12.477; 95% CI, 1.506%, 103.367%; P=0.019). By controlling the effect of other variables, the occupational stress variable has a significant impact on the prevalence of knee pain, so that those with a moderate level of occupational stress had a 3.92 times higher chance of experiencing knee pain than participants whose occupational stress was at a low level (OR=3.919; 95% CI, 1.072%, 14.327%; P=0.039). The details are shown in Table 5.
Discussion
The results of the present study show that the prevalence of MSD among EMS staff is high, and the highest prevalence belongs to the lower back, consistent with several other studies. In previous investigations on prehospital EMS personnel, the results of the studies of Nazzal et al. and Aljerian et al. show a high prevalence of MSD and the highest prevalence is related to the lower back [3, 22]. Möckel et al. reported the prevalence of pain in these people to be 58.64%, which was high, and the utmost degree of pain was related to the lumbar spine region [23]. In the study of Davison et al., the presence of MSD symptoms also is higher in the lumbar region [24]. The findings of a review study report that the annual prevalence of back pain among emergency medical technicians is 30-66% and its risk factors are mainly lifting patients, loading them in the ambulance, and working in an improper position [2]. In their review and meta-analysis, Sahebi et al. reported the prevalence of low back pain to be 50.30%, which had increased rapidly over time [1]. The results of Khosravi’s study indicate that low back pain is present in these people with high intensity, and a statistically significant relationship is reported between low back pain and people’s quality of life [25].
In our study, almost half of the participants had to stay and rest at home, leave the workplace, or take leave due to disability and discomfort caused by MSD over the past year. In line with our finding, in the study of Lonik et al., the prevalence of back pain is 65.0%; more than 30% of patients needed treatment and 15% were hospitalized [26].
Based on the results of the univariate logistic regression test, the predictors of MSD were age, work experience, exercise, the workplace, and organizational stress. The multivariate logistic regression test shows that age, exercise, organizational stress, and occupational stress are predictors of MSD.
In a review study by Sedrez et al., age and work as the first responders are shown with a high level of evidence of risk factors for MSD [27]. In Dropkin’s study, older people show a higher prevalence of musculoskeletal injuries than younger people and have lost their working days because of it [28]. According to the findings of Lonik et al.’s study, the incidence of back pain in older people is higher than in young people, but this difference is not statistically significant [26]. In Imani et al.’s study, about half of the people (46.3%) have back pain and a statistically significant relationship is reported between age, work experience, and physical-occupational factors with back pain [9]. In Nazzal et al.’s study, in addition to age and work experience, work-related MSD (WMSD) in at least one area of the body are significantly associated with male gender, high BMI, and low education level [22]. In Zhang’s study, older female ambulance nurses with higher BMI and who worked in shifts suffer more from lower back pain, and there is a relationship between job-related psychological factors and back pain [29]. In the study by Aljerian et al. the effect of the place of service on MSD is investigated, but contrary to our findings, there is no difference in the frequency of MSD based on the place of service [3].
In line with the present research, in most of the mentioned studies, MSD is present in EMS staff, and the frequency of low back pain is reported to be higher. According to the results of various studies [7, 10, 30, 31], MSD has a high prevalence among prehospital emergency staff due to the nature of this profession, including continuous movement of the patient at different levels, inappropriate positions in the ambulance, working with heavy equipment, long shifts, intense physical activity or lack of knowledge of correct principles of patient movement ergonomics. Early diagnosis and intervention in people with MSD can ultimately reduce the financial burden of the government and the disability budget; the awareness of EMS personnel and management of occupational risk factors are the main determinants of risk control in EMS [32]. In addition to the mentioned items, teaching the correct methods of lifting the stretcher, carrying and moving the patient and equipment, and boosting physical strength in the work program to prevent back pain are among the measures that can be taken to help EMS personnel [1].
In the present study, the level of occupational stress in research units is moderate, and some aspects of occupational stress are identified as factors affecting MSD. Given that various tools have been used to measure the stress of emergency medical workers, a detailed comparison with other studies is faced with limitations. The findings of Aghainejad et al.’s study show that 75.5% of EMS personnel suffer from moderate to high stress [21]. In the study of Mirzaei, 64.5% of EMS staff have experienced mild to moderate job stress [33]. In the findings of Afshari’s study, which was conducted qualitatively, the primary sources of perceived stress among EMS providers are critical work conditions, as well as personal and job conflicts [34]. In the study of Kodom-Wiredu et al. on emergency workers, the findings show that work demands and stress significantly affect WMSD and that the staff with higher stress levels are more prone to WMSD [35]. In a study by Sahraei et al. emergency medical staff who have MSD due to their jobs reported higher levels of stress than others. However, this difference was not statistically significant [36]. In the study of Möckel et al., people with chronic and recurrent pain report higher stress levels [23].
In previous investigations on nurses, like in Moradi and Barakat’s study, there is a significant relationship between the prevalence of disorders and occupational stress [37]. Azma et al.’s study shows occupational stress is effective in the rate of MSD [38]. In the study of Borhan Zehi, a significant relationship is reported between stress and MSD in the lumbar region [39]. In Tabatabai’s study, a significant difference is observed between the amount and sources of occupational stress with pain in the back, shoulder, and neck areas. The results of this study show a high prevalence of MSD in high-stress jobs and that the chronic and severe pain of staff is associated with severe disability and low quality of life [40]. Based on previous studies, an increase in occupational stress among employees can lead to a rise in MSD [7]. The physical demands of the workplace and the resulting workload, directly and indirectly, affect musculoskeletal complaints. In addition, psychosocial risk factors resulting from job stress dimensions are involved in the severity of MSD [18].
The literature shows that in addition to job stress, low job control, low job decision authority and low job satisfaction are significantly associated with an increased risk of MSD. Psychosocial risk factors such as inadequate social support, lack of control at work, and high workload were also associated with an increased risk of MSD. Workers with less social support often report longer recovery times after acute superficial musculoskeletal injuries [12].
The strength of our study comprises the inclusion of all individuals in different prehospital emergency departments, especially women. However, our study has several limitations that should be addressed in future studies. First, despite the census used in this study, the statistical population was small. Therefore, to obtain more accurate results and generalize them to the community of EMS staff, it is suggested that similar studies be conducted at a broader level with a larger statistical population. Second, the dispatch center staff’s workplace is fixed, so it is impossible to compare the mission’s duration and the distance traveled for transferring the patients, which could have affected MSD. Third, all the female staff in the present study work in the call triage center, and their work environment has more stable conditions than other units and centers. They do not work in operational units in direct interaction with patients and do not experience the difficult physical conditions of ambulances and missions, which could affect the study results. Fourth, although several demographic factors were studied in this study, other confounding factors, such as the amount of income, type, number of work shifts, and nutrition, were not investigated. These may affect the results of the study.
In addition, the lack of workforce, non-standard shifts, frequent missions, and lack of enough rest between missions, especially in the middle of the night, the use of worn-out ambulances, and the many twists and turns of the roads in this province are some of the things that need further investigation.
Conclusion
In conclusion, the present study’s findings might be valuable for a better understanding the current conditions of EMS staff in this region because this research is the first study in which the prevalence of MSD and its related factors in EMS staff is assessed in North Khorasan Province. Moreover, the findings of this research will be used as basic information for further studies in this occupational group.
In summary, the results of the present study indicate a high prevalence of MSD as well as an unfavorable level of occupational stress among EMS staff, which will naturally affect the quality of their personal and professional life and the services provided by them, which can increase their dissatisfaction. Therefore, it is recommended that relevant authorities receive the views, criticisms, and suggestions of prehospital emergency staff to investigate and better understand the causes of the current situation. It is also recommended that effective intervention and performance measures be considered to reduce occupational stress and MSD in EMS to help improve the health and quality of work-related factors and increase their productivity.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of North Khorasan University of Medical Sciences, Bojnourd, Iran (Code: IR.NKUMS.REC.1400.099).
Funding
This article was extracted from a research project (Code: IR.NKUMS.REC.1400.099) conducted through material and moral support of North Khorasan University of Medical Sciences, Bojnourd, Iran.
Authors' contributions
Data collection: Nasrin Kamali, Zakiyeh Amini and Kasra Khatib; Data analysis and interpretation: Nasrin Kamali and Seyed Hojjat Hatami; Draft manuscript preparation: Nasrin Kamali; Conceptualization, study design and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the prehospital emergency and incident management organization of North Khorasan University of Medical Sciences, Bojnurd, Iran, and all the participants for their cooperation.
References
Emergency medical services (EMS) staff, as a key group providing medical services to patients in emergencies, are exposed to various occupational risks, including musculoskeletal disorders (MSD), due to the nature of their work and job requirements [1, 2]. MSD is a primary factor of human and labor injuries that reduces productivity, increases disability and absenteeism in both developed and developing countries, and imposes a significant economic burden on governments and ministries of health [3].
Studies show that among medical service providers, EMS staff have the highest rate of early retirement, mostly due to musculoskeletal diseases [4]. In the investigation of a 12-month prevalence of injuries caused by occupational accidents among 2307 staff of prehospital EMS, the injury rate was reported as 15.61% [5]. According to a systematic review and meta-analysis, the prevalence of back pain in prehospital EMS personnel was 39.4% between 2000 and 2016, and its prevalence range was 0.9%-17.1% in different countries [6]. A recent review article found that the overall prevalence of skeletal disorders among EMS personnel was 56.52%. The prevalence rates in different body regions were as follows: The lower back (47.38%), upper back (35.15%), neck (31.19%), shoulder (30%), knee (27.07%), hand (20.70%), hip/thigh (19.48%), feet (19.11%) and elbow (17.36%) [7]. Ultimately, functional disability, expenditure on health and social resources, and reduced ability of individuals to work and participate in social life will be the consequences of MSD [8].
Research indicates that one-third of EMS staff suffer from a job-related injury at least once over 6 months [9]. Repetitive actions such as lifting objects, bending, turning, moving, and transporting patients, cardiopulmonary resuscitation, and even the type of shift work, along with psychological and psychosocial stress, are among the causes of MSD in this profession [10, 11].
Research evidence suggests that the risk of MSD is increased by exposure to psychosocial stressors [12]. Occupational stress is one of the essential work-related factors in EMS personnel, and it can be related to critical events during patient care. Hence, lack of support from superiors or colleagues, poor communication, organizational changes, salaries, wages and decreased or increased workforce put pressure on people, causing anxiety and worry in different professions [13, 14]. Occupational stress is an essential factor compromising the health of healthcare workers. Among job groups, healthcare employees have a higher rate of job stress; studies show that the organization and conditions of the work environment significantly impact the occurrence of job stress and MSD [15, 16]. The results of a review study indicate that exposure to occupational stress among prehospital emergency staff and a moderate level of job stress have been reported in some investigations, which require further attention [17].
Research indicates that the physical requirements of the work environment and the resulting workload, which are aspects of occupational stress, have a direct and indirect effect on musculoskeletal complaints; moreover, the psychosocial risk factors stemming from the dimensions of occupational stress are involved in the severity of MSD [18]. Based on the findings of a review study, occupational stress is the main factor of MSD in EMS personnel [1].
Considering what was discussed, the professional nature of medical emergencies and the difference in the geography of regions, the distances and dissimilarity of roads in various provinces of Iran for transfer of patients from various districts to treatment centers by prehospital EMS personnel, the present study was conducted to evaluate the prevalence of MSD, the predicting factors and relationship with occupational stress in EMS staff of Bojnourd.
Materials and Methods
Study population and sample
The present study investigated the frequency of MSD, the factors affecting them, and the relationship with occupational stress among prehospital EMS staff in 2022. The statistical population encompassed all the urban and road EMS employees of Bojnourd City and subordinate centers in Iran, including 6 urban bases, 5 road bases, 1 air ambulance and 1 dispatch and management center, which were selected by the census. It should be noted that the dispatch center in this province includes a telephone triage unit and an ambulance dispatch and management unit.
The inclusion criteria were at least 6 months of work record in prehospital EMS, absence of congenital musculoskeletal problems, lack of musculoskeletal problems caused by trauma or accidents unrelated to work, and no known neurological and mental diseases.
Data collection tools
Three questionnaires were used to collect information, namely demographic characteristics questionnaire, Nordic musculoskeletal questionnaire and occupational stress questionnaire:
1) Demographic characteristics include gender, age, marital status, work experience, education, field of study, workplace, regular exercise program, smoking, having a second job, and body mass index (BMI); 2) The Nordic musculoskeletal questionnaire identifies the prevalence of skeletal disorders in 9 areas of the body, including neck, shoulders, elbows, wrists/hands, upper back, lower back, one or both hips/thighs, one or both knees and one or both ankles/feet. This questionnaire, which is utilized to determine the prevalence of MSD, was designed and implemented in 1987 by Mokhtariniaet al. [19] at the Institute of Occupational Health in Nordic countries and is currently known as the Nordic questionnaire. In Iran, the validity and reliability of the questionnaire were reported at an acceptable level (more than 0.7) in research conducted by Mokhtarinia et al. [19]; 3) The occupational stress questionnaire comprises 46 questions and 4 dimensions (physical, occupational, group and organizational). This tool is based on a 4-point Likert scale where a score of 0 stands for never (no tension), and a score of 3 indicates the highest level of tension. To investigate occupational stress, the quartile statistical method was used, in which the overall and dimension scores are considered as follows:
1) Physical dimension: Low (<8), moderate (8-13) and high (>13); 2) Occupational dimension: Low (<29), moderate (29-46) and high (>46); 3) Group dimension: Low (<7), moderate (7-14) and high (>14); 4) Organizational dimension: Low (<18), moderate (18-26) and high (>26); 5) General level of occupational stress: Low (<61), moderate (61-94) and high (>94)
This questionnaire was developed by Danesh [20]. Since it was formulated for nurses working in the hospital, in Aghainejad’s study, the corresponding words were substituted, and the validity and reliability were examined. In this research, the Pearson correlation coefficient was 0.87. In addition, in terms of the validity of research, based on the Cronbach α, the internal validity values were 71%, 88%, 75% and 82% for physical, occupational, group and organizational dimensions, respectively [21]. In our study, the Aghainejad questionnaire was used, and the reliability of the occupational stress questionnaire was calculated using the Cronbach α of 0.96.
Data collection
After confirming the research title by obtaining permission from the Ethics Committee of North Khorasan University of Medical Sciences, the authorization letter was issued to 115 EMS security centers to coordinate with the base manager for the researcher’s reference to emergency bases as well as the 115 emergency communication and information centers to collect information. After coordinating the time to complete the questionnaires, the researcher visited the research environment. Then, the researcher introduced himself to the participants and explained the study’s purpose. Next, a questionnaire was provided to the staff if they expressed their desire and consent to participate. After receiving the necessary explanations about answering the questionnaires, the participants completed the questionnaires in the researcher’s presence. To reduce the effect of intervening factors in completing the questionnaires, the questionnaires were anonymous and the researcher provided sufficient and clear explanations for participants regarding the confidentiality of information and non-judgment regarding them.
Since the sampling method was a census, to reach all individuals and ensure that the individual completed the questionnaire, visits were made to the desired bases and centers during different work shifts. Therefore, the data collection took about a month.
Data analysis
The results of descriptive analysis were reported as frequency (percentage) for qualitative variables and as Mean±SD for quantitative variables. To investigate pairwise relationships, univariate logistic regression analysis was used based on the type of response variable, and multiple logistic regression analysis was employed to investigate the factors affecting each of the response variables by controlling the effect of other variables. This way, the target variable was considered dependent, and the other investigated variables were independent. All analyses were performed using SPSS software, version 26 statistical software. P<0.05 was considered to be statistically significant.
Results
In the present study, 85 EMS staff participated with a mean age of 33.41±7.80 years (age range 24-60 years). Most participants were male (85.9%), married (80%) and held a degree in EMS (62.4%). The mean work experience of them was 9.41±7.03 years. The mean BMI was reported to be 25.03±3.55 kg/m2 and about half (51.8%) of the participants were in the normal BMI range. The overall score of occupational stress and all dimensions of the occupational stress questionnaire were moderate (Table 1).
According to research results (Table 2), 87.1% of people in the present study suffered from MSD in at least one area of the body during the past year. The highest prevalence of symptoms was related to the lower back (63.5%), neck and knee (36.5%), shoulder (32.9%) and upper back (23.5%). In 49.4% of cases, people had to rest, reduce work activity, leave the workplace, or were unable to perform activities at work or home due to pain, discomfort, and disability caused by MSD in the past year.
Univariate logistic regression analysis was employed to investigate the relationship between demographic factors and the prevalence of MSD and the results are shown in Table 3.
According to the results, none of the demographic variables significantly affected neck pain (P>0.05). The age variable had a significant impact on shoulder pain so that the chance of experiencing shoulder pain in people who were 40-49 years old was 4.50 times higher than those younger than 30 years (OR=0.222; 95% CI, 0.056%, 0.876%; P=0.032). The work experience variable had a significant effect on elbow pain so that the chance of experiencing elbow pain in those with 20-30 years of work experience was 13.16 times higher than in people whose work experience was <10 years (OR=0.076; 95% CI, 0.006%, 0.954%; P=0.046). The exercise variable significantly impacted wrist pain, so the chance of wrist pain in participants who exercised was 5.05 times higher than those who did not exercise (OR=5.053; 95% CI, 1.657%, 15.404%; P=0.004). The variable of the workplace had a significant effect on hip and thigh pain so that the chance of experiencing hip and thigh pain was 12.05 times higher in people whose workplace was in an air ambulance than in those working in an urban base (OR=0.083; 95% CI, 0.007%, 0.950%; P=0.045). Moreover, the likelihood of hip and thigh pain was 18.87 times higher in participants working in an air ambulance relative to those with a circulating workplace (OR=0.053, 95% CI, 0.003%, 0.872%; P=0.040). Further details are presented in Table 3.
Univariate logistic regression analysis was employed to investigate the relationship between occupational stress and the prevalence of MSD, as shown in Table 4.
According to the results of univariate regression analysis, the chance of experiencing shoulder pain in people with high organizational stress was 5.11 times higher than in those with low organizational stress (OR=5.111; 95% CI, 1.363%, 19.161%; P=0.016), which was 4.43 times higher in people who in general had a high-stress level than those with a low-stress level (OR=4.433; 95% CI, 1.020%, 19.272%; P=0.047). The chance of experiencing wrist pain was 5.65 times higher in participants with moderate organizational stress (OR=5.652; 95% CI, 1.120%, 28.519%; P=0.036). The details are shown in Table 4.
To examine and control the effect of possible confounding variables more closely, demographic variables and dimensions of occupational stress whose impact on the prevalence of each MSD was significant at P<0.2 level were subject to multiple logistic regression tests, as shown in Table 5.
According to the obtained results, the age variable significantly impacted the prevalence of shoulder pain by controlling the effect of other variables. Hence, people 40-49 years old had a 5.6 times higher chance of experiencing shoulder pain than those younger than 30 (OR=0.152; 95% CI, 0.032%, 0.717%; P=0.017). By controlling the effect of other variables, the variables of exercise and organizational stress had a significant effect on the prevalence of wrist pain, so that people who exercised had 17.13 times more chance of experiencing wrist pain than those who did not exercise (OR=17.130; 95% CI, 3.110%; 94.342%; P=0.001). In addition, people with moderate organizational stress had a 12.48 times higher chance of experiencing wrist pain than those with low organizational stress (OR=12.477; 95% CI, 1.506%, 103.367%; P=0.019). By controlling the effect of other variables, the occupational stress variable has a significant impact on the prevalence of knee pain, so that those with a moderate level of occupational stress had a 3.92 times higher chance of experiencing knee pain than participants whose occupational stress was at a low level (OR=3.919; 95% CI, 1.072%, 14.327%; P=0.039). The details are shown in Table 5.
Discussion
The results of the present study show that the prevalence of MSD among EMS staff is high, and the highest prevalence belongs to the lower back, consistent with several other studies. In previous investigations on prehospital EMS personnel, the results of the studies of Nazzal et al. and Aljerian et al. show a high prevalence of MSD and the highest prevalence is related to the lower back [3, 22]. Möckel et al. reported the prevalence of pain in these people to be 58.64%, which was high, and the utmost degree of pain was related to the lumbar spine region [23]. In the study of Davison et al., the presence of MSD symptoms also is higher in the lumbar region [24]. The findings of a review study report that the annual prevalence of back pain among emergency medical technicians is 30-66% and its risk factors are mainly lifting patients, loading them in the ambulance, and working in an improper position [2]. In their review and meta-analysis, Sahebi et al. reported the prevalence of low back pain to be 50.30%, which had increased rapidly over time [1]. The results of Khosravi’s study indicate that low back pain is present in these people with high intensity, and a statistically significant relationship is reported between low back pain and people’s quality of life [25].
In our study, almost half of the participants had to stay and rest at home, leave the workplace, or take leave due to disability and discomfort caused by MSD over the past year. In line with our finding, in the study of Lonik et al., the prevalence of back pain is 65.0%; more than 30% of patients needed treatment and 15% were hospitalized [26].
Based on the results of the univariate logistic regression test, the predictors of MSD were age, work experience, exercise, the workplace, and organizational stress. The multivariate logistic regression test shows that age, exercise, organizational stress, and occupational stress are predictors of MSD.
In a review study by Sedrez et al., age and work as the first responders are shown with a high level of evidence of risk factors for MSD [27]. In Dropkin’s study, older people show a higher prevalence of musculoskeletal injuries than younger people and have lost their working days because of it [28]. According to the findings of Lonik et al.’s study, the incidence of back pain in older people is higher than in young people, but this difference is not statistically significant [26]. In Imani et al.’s study, about half of the people (46.3%) have back pain and a statistically significant relationship is reported between age, work experience, and physical-occupational factors with back pain [9]. In Nazzal et al.’s study, in addition to age and work experience, work-related MSD (WMSD) in at least one area of the body are significantly associated with male gender, high BMI, and low education level [22]. In Zhang’s study, older female ambulance nurses with higher BMI and who worked in shifts suffer more from lower back pain, and there is a relationship between job-related psychological factors and back pain [29]. In the study by Aljerian et al. the effect of the place of service on MSD is investigated, but contrary to our findings, there is no difference in the frequency of MSD based on the place of service [3].
In line with the present research, in most of the mentioned studies, MSD is present in EMS staff, and the frequency of low back pain is reported to be higher. According to the results of various studies [7, 10, 30, 31], MSD has a high prevalence among prehospital emergency staff due to the nature of this profession, including continuous movement of the patient at different levels, inappropriate positions in the ambulance, working with heavy equipment, long shifts, intense physical activity or lack of knowledge of correct principles of patient movement ergonomics. Early diagnosis and intervention in people with MSD can ultimately reduce the financial burden of the government and the disability budget; the awareness of EMS personnel and management of occupational risk factors are the main determinants of risk control in EMS [32]. In addition to the mentioned items, teaching the correct methods of lifting the stretcher, carrying and moving the patient and equipment, and boosting physical strength in the work program to prevent back pain are among the measures that can be taken to help EMS personnel [1].
In the present study, the level of occupational stress in research units is moderate, and some aspects of occupational stress are identified as factors affecting MSD. Given that various tools have been used to measure the stress of emergency medical workers, a detailed comparison with other studies is faced with limitations. The findings of Aghainejad et al.’s study show that 75.5% of EMS personnel suffer from moderate to high stress [21]. In the study of Mirzaei, 64.5% of EMS staff have experienced mild to moderate job stress [33]. In the findings of Afshari’s study, which was conducted qualitatively, the primary sources of perceived stress among EMS providers are critical work conditions, as well as personal and job conflicts [34]. In the study of Kodom-Wiredu et al. on emergency workers, the findings show that work demands and stress significantly affect WMSD and that the staff with higher stress levels are more prone to WMSD [35]. In a study by Sahraei et al. emergency medical staff who have MSD due to their jobs reported higher levels of stress than others. However, this difference was not statistically significant [36]. In the study of Möckel et al., people with chronic and recurrent pain report higher stress levels [23].
In previous investigations on nurses, like in Moradi and Barakat’s study, there is a significant relationship between the prevalence of disorders and occupational stress [37]. Azma et al.’s study shows occupational stress is effective in the rate of MSD [38]. In the study of Borhan Zehi, a significant relationship is reported between stress and MSD in the lumbar region [39]. In Tabatabai’s study, a significant difference is observed between the amount and sources of occupational stress with pain in the back, shoulder, and neck areas. The results of this study show a high prevalence of MSD in high-stress jobs and that the chronic and severe pain of staff is associated with severe disability and low quality of life [40]. Based on previous studies, an increase in occupational stress among employees can lead to a rise in MSD [7]. The physical demands of the workplace and the resulting workload, directly and indirectly, affect musculoskeletal complaints. In addition, psychosocial risk factors resulting from job stress dimensions are involved in the severity of MSD [18].
The literature shows that in addition to job stress, low job control, low job decision authority and low job satisfaction are significantly associated with an increased risk of MSD. Psychosocial risk factors such as inadequate social support, lack of control at work, and high workload were also associated with an increased risk of MSD. Workers with less social support often report longer recovery times after acute superficial musculoskeletal injuries [12].
The strength of our study comprises the inclusion of all individuals in different prehospital emergency departments, especially women. However, our study has several limitations that should be addressed in future studies. First, despite the census used in this study, the statistical population was small. Therefore, to obtain more accurate results and generalize them to the community of EMS staff, it is suggested that similar studies be conducted at a broader level with a larger statistical population. Second, the dispatch center staff’s workplace is fixed, so it is impossible to compare the mission’s duration and the distance traveled for transferring the patients, which could have affected MSD. Third, all the female staff in the present study work in the call triage center, and their work environment has more stable conditions than other units and centers. They do not work in operational units in direct interaction with patients and do not experience the difficult physical conditions of ambulances and missions, which could affect the study results. Fourth, although several demographic factors were studied in this study, other confounding factors, such as the amount of income, type, number of work shifts, and nutrition, were not investigated. These may affect the results of the study.
In addition, the lack of workforce, non-standard shifts, frequent missions, and lack of enough rest between missions, especially in the middle of the night, the use of worn-out ambulances, and the many twists and turns of the roads in this province are some of the things that need further investigation.
Conclusion
In conclusion, the present study’s findings might be valuable for a better understanding the current conditions of EMS staff in this region because this research is the first study in which the prevalence of MSD and its related factors in EMS staff is assessed in North Khorasan Province. Moreover, the findings of this research will be used as basic information for further studies in this occupational group.
In summary, the results of the present study indicate a high prevalence of MSD as well as an unfavorable level of occupational stress among EMS staff, which will naturally affect the quality of their personal and professional life and the services provided by them, which can increase their dissatisfaction. Therefore, it is recommended that relevant authorities receive the views, criticisms, and suggestions of prehospital emergency staff to investigate and better understand the causes of the current situation. It is also recommended that effective intervention and performance measures be considered to reduce occupational stress and MSD in EMS to help improve the health and quality of work-related factors and increase their productivity.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of North Khorasan University of Medical Sciences, Bojnourd, Iran (Code: IR.NKUMS.REC.1400.099).
Funding
This article was extracted from a research project (Code: IR.NKUMS.REC.1400.099) conducted through material and moral support of North Khorasan University of Medical Sciences, Bojnourd, Iran.
Authors' contributions
Data collection: Nasrin Kamali, Zakiyeh Amini and Kasra Khatib; Data analysis and interpretation: Nasrin Kamali and Seyed Hojjat Hatami; Draft manuscript preparation: Nasrin Kamali; Conceptualization, study design and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the prehospital emergency and incident management organization of North Khorasan University of Medical Sciences, Bojnurd, Iran, and all the participants for their cooperation.
References
- Sahebi A, Nateghinia S, Golitaleb M, Alizadeh S, Jahangiri K. The prevalence of low back pain in emergency medical services personnel: A systematic review and meta-analysis. Nursing Practice Today. 2022; 9(3):193-201. [DOI:10.18502/npt.v9i3.10221]
- Friedenberg R, Kalichman L, Ezra D, Wacht O, Alperovitch-Najenson D. Work-related musculoskeletal disorders and injuries among emergency medical technicians and paramedics: A comprehensive narrative review. Archives of Environmental & Occupational Health. 2022; 77(1):9-17. [DOI:10.1080/19338244.2020.1832038] [PMID]
- Aljerian N, Alshehri S, Masudi E, Albawardi AM, Alzahrani F, Alanazi R. The prevalence of musculoskeletal disorders among EMS personnel in Saudi Arabia, Riyadh. The Egyptian Journal of Hospital Medicine. 2018; 73(1):5777-82. [DOI:10.21608/ejhm.2018.11879]
- Wiitavaara B, Lundman B, Barnekow-Bergkvist M, Brulin C. Striking a balance--health experiences of male ambulance personnel with musculoskeletal symptoms: A grounded theory. Int J Nurs Stud. 2007; 44(5):770-9. [DOI:10.1016/j.ijnurstu.2006.02.007] [PMID]
- Möckel L, Arnold C, May T, Maaß L, Sohrabizadeh S, Hofmann T, ET AL. Twelve-month prevalence of injury due to an occupational accident in prehospital Emergency Medical Services staff: Data from the EMS Health Study. Journal of Emergency Medicine, Trauma & Acute Care. 2022; 2022(5):37. [DOI:10.5339/jemtac.2022.37]
- Yahyaei K, Yazdi K, Kolagari S, Rahmani H. Effect of patient transfer training on low back pain in prehospital emergency medical services personnel. Journal of Clinical and Basic Research. 2019; 3(4):31-6. [DOI:10.29252/jcbr.3.4.31]
- Tahernejad A, Makki F, Rezaei E, Marzban H, Tahernejad S, Sahebi A. Musculoskeletal disorders in emergency medical services personnel: A systematic review and meta-analysis. Public Health. 2024; 237:107-15. [DOI:10.1016/j.puhe.2024.08.020] [PMID]
- Greggi C, Visconti VV, Albanese M, Gasperini B, Chiavoghilefu A, Prezioso C, et al. Work-related musculoskeletal disorders: A systematic review and meta-analysis. Journal of Clinical Medicine. 2024; 13(13):3964. [DOI:10.3390/jcm13133964] [PMID]
- Imani A, Borna J, Alami A, Khosravan S, Hasankhani H, Bafandeh Zende M. Prevalence of low back pain and its related factors among pre-hospital emergency personnel in Iran. Journal of Emergency Practice and Trauma. 2019; 5(1):8-13. [DOI:10.15171/jept.2018.01]
- Amit LM, Hunter CS. Analyses of postures and musculoskeletal disorders of emergency medical technicians in the United States. Shift. 2023; 2(1):10-8. [Link]
- Mesri H, Mehri S, Aghamohammadi M. Comparison of problems related to 12 and 24-shift shift work in emergency medical technicians of Ardabil province. Occupational Medicine. 2023; 14(4):25-35. [DOI:10.18502/tkj.v14i4.12311]
- Afsharian A, Dollard MF, Glozier N, Morris RW, Bailey TS, Nguyen H, et al. Work-related psychosocial and physical paths to future musculoskeletal disorders (MSDs). Safety Science. 2023; 164:106177. [DOI:10.1016/j.ssci.2023.106177]
- Gharlipour Z. Occupational stress and mental health relationship in nurses. Advances in Nursing & Midwifery. 2014; 23(82):55-62. [DOI:10.22037/anm.v23i82.6314]
- Johnsen AM, Wagman P, Broström A, Fransson EI. Work, lifestyle and health-related factors among women and men working in the emergency medical services. International Journal of Occupational Safety and Ergonomics. 2024; 30(2):651-61. [DOI:10.1080/10803548.2024.2332115] [PMID]
- Motamedi S, Sajjadian I. [The mediating role of occupational stress in the relationship between coping strategies and job burden with quality of professional life in psychiatric emergency department nurses (Persian)]. Iranian Journal of Nursing Research. 2024; 19(2):34-49. [DOI:10.22034/IJNR.19.2.34]
- Hassanzadeh P, Ghahramani A, Mohebbi I. [An assessment of association between macro-ergonomics status and employees’ prevalence of musculoskeletal disorders and job stress outcomes in Urmia educational and medical hospitals (Persian)]. Iranian Journal of Ergonomics. 2020; 7(4):40-51. [DOI:10.30699/jergon.7.4.40]
- Farrokhi P, Irannejad B, Hajizadeh A. Job stress and its management methods among prehospital emergency staff in Iran: A systematic review. Journal of Rafsanjan University of Medical Sciences. 2022; 21(6):661-76. [DOI:10.52547/jrums.21.6.661]
- Gholami T, Heidari Pahlavian A, Akbarzadeh M, Motamedzade M, Heidari Moghadam R. [A structural equation modeling study of job stress and musculoskeletal disorders (Persian)]. Iranian Journal of Ergonomics. 2015; 3(3):51-64. [Link]
- Mokhtarinia H, Shafiee A, Pashmdarfard M. [Translation and localization of the extended nordic musculoskeletal questionnaire and the evaluation of the face validity and test-retest reliability of its Persian version (Persian)]. Iranian Journal of Ergonomics. 2015; 3(3):21-9. [Link]
- Danesh F. [Relationship between occupational stress and behavior response in nurses of hospitals dependent to medical science Kerman University (Persian)] [thesis]. Kerman: Islamic Azad University of Kerman, 2003.
- Aghaeinejad AA, Eshgh ZM, Peyman A, Chehrehgosha M. Prevalence of occupational stressors from the perspective of prehospital personnel in disaster and emergency medical management center. Advances in Environmental Biology. 2014; 2014:73-80. [Link]
- Nazzal MS, Oteir AO, Alrawashdeh A, Alwidyan MT, Obiedat Q, Almhdawi KA, et al. Prevalence of work-related musculoskeletal disorders and associated factors affecting emergency medical services professionals in Jordan: A cross-sectional study. BMJ Open. 2024; 14(4):e078601. [DOI:10.1136/bmjopen-2023-078601] [PMID]
- Möckel L, Gerhard A, Mohr M, Armbrust CI, Möckel C. Prevalence of pain, analgesic self-medication and mental health in German pre-hospital emergency medical service personnel: A nationwide survey pilot-study. International Archives of Occupational and Environmental Health. 2021; 94(8):1975-82. [DOI:10.1007/s00420-021-01730-x] [PMID]
- Davison C., Cotrim TP, Gonçalves S. Perception of musculoskeletal symptoms and psychosocial risk factors among a sample of Portuguese emergency medical technicians. In: Cotrim TP, Serranheira F, Sousa P, Hignett S, Albolino S, Tartaglia R, editors. Health and social care systems of the future: Demographic changes, digital age and human factors. Berlin: Springer; 2019. [DOI:10.1007/978-3-030-24067-7_6]
- Khosravi Bonjar A, Ahmadi Chenari H, Bazaz Kahani H, Mohammadi M. [Investigating the relationship between low back pain and quality of life in emergency medical personnel and the role of demographic variables in this regard (Persian)]. Occupational Medicine Quarterly Journal. 2021; 13(3):1-8. [DOI:10.18502/tkj.v13i3.8194]
- Lonik ET, Kamauzaman TT, Abdullah AA, Nor J, Ab Hamid SA. Prevalence of low-back pain among public ambulance workers in Kelantan, Malaysia. Malaysian Journal of Public Health Medicine. 2017; 17(1):126-35. [Link]
- Sedrez JA, Kasten APDS, Chaise FO, Candotti CT. Risk factors for work-related cardiovascularand musculoskeletal diseasesamong prehospital urgent care workers: A systematic review. Revista brasileira de medicina do trabalho. 2017; 15(4):355-63. [DOI:10.5327/Z1679443520170050] [PMID]
- Dropkin J, Power P, Rasul R, Moline J, Kim H. Effect of resiliency and age on musculoskeletal injuries and lost workdays in emergency medical service personnel. International Journal of Industrial Ergonomics. 2019; 69:184-93. [DOI:10.1016/j.ergon.2018.11.008]
- Zhang Q, Dong H, Zhu C, Liu G. Low back pain in emergency ambulance workers in tertiary hospitals in China and its risk factors among ambulance nurses: A cross-sectional study. BMJ Open. 2019; 9(9):e029264. [DOI:10.1136/bmjopen-2019-029264] [PMID]
- Barkhordarzadeh S, Choobineh A, Razeghi M, Cousins R, Mokarami H. Effects of an ergonomic intervention program based on the PRECEDE-PROCEED model for reducing work-related health problems and exposure risks among emergency medical dispatchers. Int Arch Occup Environ Health. 2022; 95(6):1389-99. [DOI:10.1007/s00420-022-01846-8] [PMID]
- Gür B, Yeşilnar M. Evaluation of working postures of emergency health services workers by REBA and RULA method. International Journal of Social and Humanities Sciences Research. 2024; 11(108):1230-6. [DOI:10.5281/zenodo.12638663]
- Senol V, Argun M, Celebi I. Evaluation of risk perception and management in emergency medical services providers working in pre-hospital areas in Kayseri, Turkey. Ethno-Medicine. 2018; 12(1):40-8. [DOI:10.31901/24566772.2018/12.01.522]
- Mirzaei A, Mozaffari N, Habibi Soola A. Occupational stress and its relationship with spiritual coping among emergency department nurses and emergency medical services staff. International Emergency Nursing. 2022; 62:101170. [DOI:10.1016/j.ienj.2022.101170] [PMID]
- Afshari A, Borzou SR, Shamsaei F, Mohammadi E, Tapak L. Perceived occupational stressors among emergency medical service providers: A qualitative study. BMC Emergency Medicine. 2021; 21(1):35. [DOI:10.1186/s12873-021-00430-6] [PMID]
- Kodom-Wiredu JK. Work demand, stress and work-related musculoskeletal disorders among emergency workers. International Journal of Workplace Health Management. 2019; 12(2):85-98. [DOI:10.1108/IJWHM-08-2018-0111]
- Sahraei MM, Molavi Verdanjani M, Soltanian A, Khatiban M. The relationship between musculoskeletal injuries and stress load in emergency medical staff of hamadan province in 2019. Avicenna Journal of Nursing and Midwifery Care. 2021; 29(1):23-34. [DOI:10.30699/ajnmc.29.1.23]
- Moradi B, Barakat S. Ergonomic assessment of musculoskeletal disorders risk factors in nurses using QEC method and its relation with job stress. Journal of Knowledge & Health. 2021; 16(1):41-50. [DOI:10.22100/jkh.v16i1.2555]
- Azma K, Hosseini A, Safarian MH, Abedi M. Evaluation of the relationship between musculoskeletal discomforts and occupational stressors among nurses. North American Journal of Medical Sciences. 2015; 7(7):322-7. [DOI:10.4103/1947-2714.161250] [PMID]
- Borhanzehi KH, Rigi ZE, Parast EY, Dadpisheh S. Investigation of the prevalence of musculoskeletal disorders and its relationship with mental health in nurses: A descriptive-analytical study. Occupational Medicine. 2021; 13(1):42-52. [Link]
- Tabatabaei S, Khani Jazani R, Kavousi Dolanghar A, Rostami K, Najafi Z. The relationship between rate and sources of job stress and musculoskeletal pains among the staff of one hospital in Tehran city, Iran. Qom University of Medical Sciences Journal. 2017; 11(4):72-9. [Link]
Type of article: Research |
Subject:
Emergency
Received: 2024/08/16 | Accepted: 2024/12/28 | Published: 2025/07/9
Received: 2024/08/16 | Accepted: 2024/12/28 | Published: 2025/07/9
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
