

Volume 10, Issue 3 (Spring 2025)
Health in Emergencies and Disasters Quarterly 2025, 10(3): 153-166 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Moghaddamnia M T, Shahrestanaki Y A, Maroufizadeh S, Ghanbari Nikoo R, Pourvakhshoori N. Musculoskeletal Disorders of Emergency Medical Services Personnel and Their Associations With Job Content: A Cross-sectional Study. Health in Emergencies and Disasters Quarterly 2025; 10 (3) :153-166
URL: http://hdq.uswr.ac.ir/article-1-649-en.html
URL: http://hdq.uswr.ac.ir/article-1-649-en.html
Mohammad Taghi Moghaddamnia1 

 , Yousof Akbari Shahrestanaki2 , Saman Maroufizadeh3 , Reza Ghanbari Nikoo4 , Negar Pourvakhshoori *5
, Yousof Akbari Shahrestanaki2 , Saman Maroufizadeh3 , Reza Ghanbari Nikoo4 , Negar Pourvakhshoori *5
, Yousof Akbari Shahrestanaki2 , Saman Maroufizadeh3 , Reza Ghanbari Nikoo4 , Negar Pourvakhshoori *5
1- Social Determinants of Health Research Center, Shahid Beheshti Nursing and Midwifery School, Guilan University of Medical Sciences, Rasht, Iran.
2- Social Determinants of Health Research Center, Research Institute for Prevention of Non-Communicable Diseases, Qazvin University of Medical Sciences, Qazvin, Iran.
3- Department of Biostatistics, Faculty of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
4- Department of Nursing, Faculty of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
5- Department of Nursing, Faculty of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran. ,nvakhshoori@gmail.com
2- Social Determinants of Health Research Center, Research Institute for Prevention of Non-Communicable Diseases, Qazvin University of Medical Sciences, Qazvin, Iran.
3- Department of Biostatistics, Faculty of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
4- Department of Nursing, Faculty of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
5- Department of Nursing, Faculty of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran. ,
Full-Text [PDF 585 kb]
(953 Downloads)
| Abstract (HTML) (3033 Views)
Full-Text: (685 Views)
Introduction
Today, the emergency medical service (EMS) is one of the critical components of the healthcare system [1] since EMS can save lives by providing rapid, efficient, and effective care [2]. EMS meets specific health needs outside of hospitals, focusing on life-threatening injuries, patient transport, inter-facility transfers, and preparedness for missions in health emergencies [3]. Furthermore, EMS personnel are dispatched to road and non-road accidents [4]. Poor psychosocial conditions can negatively impact personnel health. Research over the past two decades has shown that poor psychosocial work conditions adversely affect health, particularly in EMS personnel, whose profession is often with challenges [5-8]. Job content poses multiple threats, including musculoskeletal disorders (MSDs) [9]. MSDs are among the prominent issues in occupational health and ergonomics. These disorders are prevalent across various jobs and a significant global challenge [10, 11, 12]. MSDs affect different body parts, such as muscles, bones, tendons, ligaments, joints, nerves, and blood vessels, leading to injury or discomfort accompanied by pain or inflammation. Work conditions can cause or exacerbate these disorders [9]. The consequences of MSDs in the workplace include disability, lost work time, compensation claims, and treatment costs [13].
Typically, employed individuals experience musculoskeletal discomfort at least once in their lifetime. Studies have shown that MSDs account for more than half of work absences and approximately 50% of occupational diseases [14]. Hence, special attention should be paid to the prevalence of these disorders in various work environments. Studies have reported that MSDs occur in healthcare professions (e.g. EMS technicians and nurses) and specialized fields (e.g. emergency rooms, orthopedics) [15-18]. It is also estimated that nearly one-third of all sick leave among healthcare personnel is related to these disorders [19]. A review of studies indicates that healthcare professionals are at risk of developing MSDs due to repetitive tasks, high workload, poor work conditions, patient transfer, psychological factors like job stress, and work shifts [20-23]. Dehdashti et al. assessed the posture of nurses at Velayat Hospital in Damghan City, Iran, during their job duties and its impact on the occurrence of MSDs. The results indicated that the risk of symptoms manifestation was high (risk levels of 2 and 3). The study also showed that the emergency department had the highest level of risk. The authors noted that corrective measures might be necessary in the intensive care unit (ICU) and coronary care unit (CCU) departments, but they believed these measures were especially crucial in the emergency and surgical departments [24]. Therefore, preventing MSDs in a working population requires evaluating job-related factors and individual characteristics and determining the association between these factors and disorders. The World Health Organization (WHO), the Occupational Safety and Health Administration of the USA (OSHA), and the UK Health and Safety Executive (HSE) have emphasized controlling and preventing these disorders, making them a priority. The nature of health and medical personnel’s jobs constantly exposes them to physical and psychological fatigue, so research on this topic is highly important. Such pressures and occupational injuries can adversely impact the services of EMS personnel to the entire community [25].
Studies indicate that considering job content as one of the psychosocial evaluation criteria that can lead to MSDs is important. It has been shown that a low level of job content among employees increases their vulnerability to MSDs [25]. Also, the relationship between job content and MSDs has been confirmed in various studies [26-28]. The nature, scope, and job content of pre-hospital EMS and the associated outcomes, including MSDs, considering variables such as culture, customs, climatic conditions in different regions of the country, demographic features, job characteristics regarding mission diversity, and the newly established nature of EMS organization, highlight the necessity of conducting studies in the field of pre-hospital EMS. Moreover, understanding the nature and content of EMS can enhance the job quality of its personnel. Ultimately, reducing the complications and outcomes associated with these disorders improves their quality of life and provides patients with more effective assistance. Therefore, this study was conducted to determine the relationship between job content and MSDs among operational staff of EMS working in Qazvin Province, Iran.
Materials and Methods
In the present analytical cross-sectional study, 163 samples of operational staff of EMS across 38 bases in Qazvin were selected by census method. The inclusion criteria for the study included having work experience of more than six months and agreement to participate in the study, while the exclusion criterion was partial (less than 50%) completion of the questionnaire. Furthermore, non-operational staff (supervisors or dispatchers) did not participate in the study. Data were collected using a three-part questionnaire. The first part included demographic characteristics (age, height, weight, marital status, smoking habits, alcohol consumption, education level, major, work experience, number of missions per shift, number of children, and physical activity). The second part contained the job content questionnaire (JCQ); the third consisted of the extended Nordic musculoskeletal questionnaire.
The JCQ contained 52 items, including 9 items for assessing the scale of decision latitude, 6 for the subscale of skill utilization, 3 for the subscale of decision authority, 5 for the scale of psychological job demands, 8 for social support, 4 for coworker social support, 4 for supervisor social support, 5 for physical job demands, 3 for physical effort, 2 for isometric physical load, and 3 for job insecurity. Each questionnaire item was scored on a 4-point Likert scale (strongly disagree=1 to strongly agree=4). To compute scores, a higher score than the sample mean should be considered for job demands, and a lower score than the sample mean for decision latitude [29]. The psychometric properties and reliability of the JCQ have been examined and confirmed in numerous studies; for instance, in the Sasaki et al. [6] study, the Cronbach α coefficients were calculated for each of the 4‐factor scores (i.e. psychological demand, decision latitude, supervisor support, and coworker support) of JCQ in Vietnamese staff. The Cronbach α>0.7 was the criterion for acceptability with the statistical significance P<0.05 [30-33]. Additionally, permission to use this tool was obtained from the questionnaire designer via email.
The extended Nordic musculoskeletal questionnaire (NMQ-E) includes 11 items covering 9 different body areas: Neck, shoulders, upper back, elbows, wrists/hands, lower back, pelvis/thighs, knees, and ankles/feet. This tool uses a binary format (yes=1 point, no=0 point) [30]. Scores are calculated based on the 9 body areas, ranging from 0 to 99 points, and the mean score is used for interpretation. The questionnaire is completed through self-reporting (on paper, by phone, online) or via interview. Responses are given in a yes-no format and a 5-point Likert scale ranging from “strongly agree” to “strongly disagree.” The questionnaire covers 9 body areas (three upper extremities, three spine areas, and three lower extremities). Thus, a completed questionnaire can provide 99 data points (excluding age-related data). The questions first inquire about the presence or absence of pain throughout life, its prevalence, and finally, the consequences of the pain. Respondents must answer all questions about one body area before moving to another. If a “yes” response is given to any question about a specific body area, the respondent continues answering the questions for that area until all questions are completed. If the response is “no,” the respondent stops answering questions for that area, and the remaining questions are automatically considered negative, moving on to other body areas. The validity and reliability of this tool have been confirmed in various studies [29, 34]. In the Mokhtarinia study, the translation and localization of the NMQ-E were deemed easy and acceptable. All the items in the questionnaire had acceptable face validity. The intra-class correlation coefficient and the standard error of measurement of the Persian version of the NMQ-E were deemed acceptable (SEM=0.56-1.76 and ICC>0.7), and the Kappa coefficient was calculated as 0.78-1.00 [34].
The study data were collected after obtaining approval from the Ethics Committee and the Research Office of Guilan University of Medical Sciences (GUMS), giving an introduction letter to the relevant center, and obtaining agreement from the responsible authorities and permission to be present in the research environment. Then, the study objectives were explained to the participants, and the importance of confidentiality and the voluntary nature of participation were emphasized. Moreover, the participants could withdraw from completing the questionnaire. The questionnaires were filled out without inserting names. Data analysis was performed using SPSS software, version 16. Quantitative variables were reported as Mean±SD for data analysis, and qualitative variables were reported as frequency (percentage). In univariate analyses, logistic regression (LR) models (crude odds ratios) were used to examine the relationship between individual job variables and job content status with MSDs. In multivariate analyses, multiple LR models (adjusted odds ratios) were used to determine factors associated with MSDs to control and adjust for other variables. The data were analyzed using SPSS software, version 16, and a significance level was considered at 0.05.
Results
The study included 163 male participants aged 21-55 years. The Mean±SD age of the participants was 34.42±7.47 years. In total, 57.67% of the participants were overweight. Most participants were married (68.10%), and 53.37% had no children. Most participants were non-Turk and non-Kurd (53.99%). Among the participants, 73.01% had studied EMS and mostly had an associate degree (46.63%). Most participants engaged in physical activity weekly (56.44%). In total, 32.52% were smokers, and only 9.20% consumed alcohol. Additionally, 12.27% had a history of accidents, and only 6.75% had chronic illnesses. Most participants had less than 11 years of work experience (52.76%) (minimum: 1 year; maximum: 29 years), with a Mean±SD of 10.02±6.55 years. In total, 59.51% were working at urban emergency bases. Most participants had a 24-hour shift schedule (54.60%), and 68.71% had 10-20 shifts per month. The Mean±SD number of monthly shifts was 12.22±4.71. Most participants had 1-6 missions (60.12%), and only 8.59% had a second job.
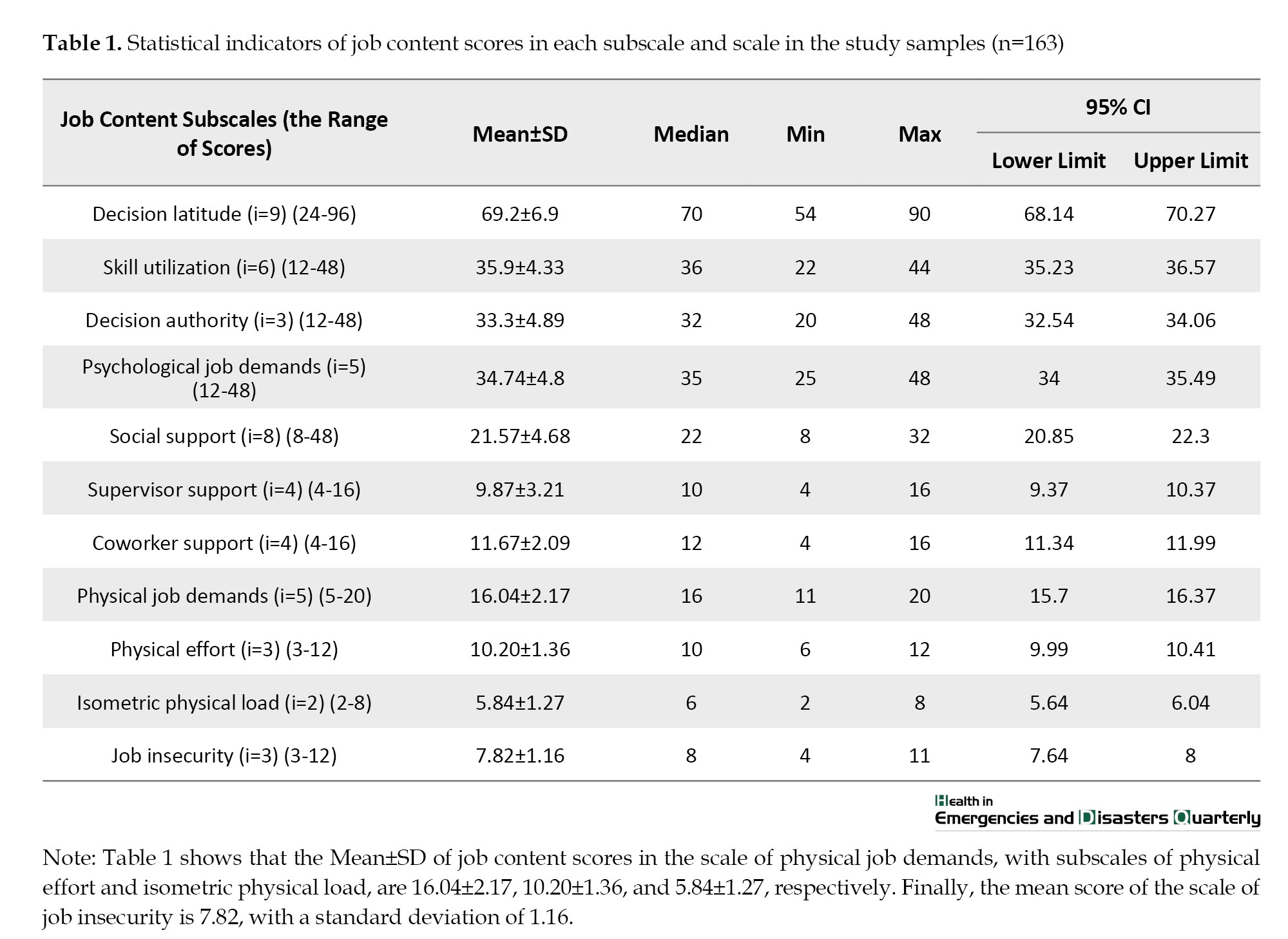
The results showed that the higher the mean score of the decision latitude and social support scale, the lower the stress is. Conversely, the higher the mean score of the psychological job demands, physical job demands, and job insecurity scale, the higher the stress is. The Mean±SD of the scores in the decision latitude scale, with subscales of skill utilization and decision authority, were 69.20±6.90, 35.90±4.33, and 33.30±4.89, respectively. The Mean±SD score in the psychological job demands scale was 34.74±4.80. In the social support scale, with supervisor and coworker support subscales, the Mean±SD scores were 21.57±4.68, 9.87±3.21, and 11.67±2.09, respectively. Also, the Mean±SD of the job content score in the physical job demands scale, with subscales of physical effort and isometric physical load, were 16.04±2.17, 10.20±1.36, and 5.84±1.27, respectively. Finally, the job insecurity scale’s Mean±SD score was 7.82±1.16 (Table 1).
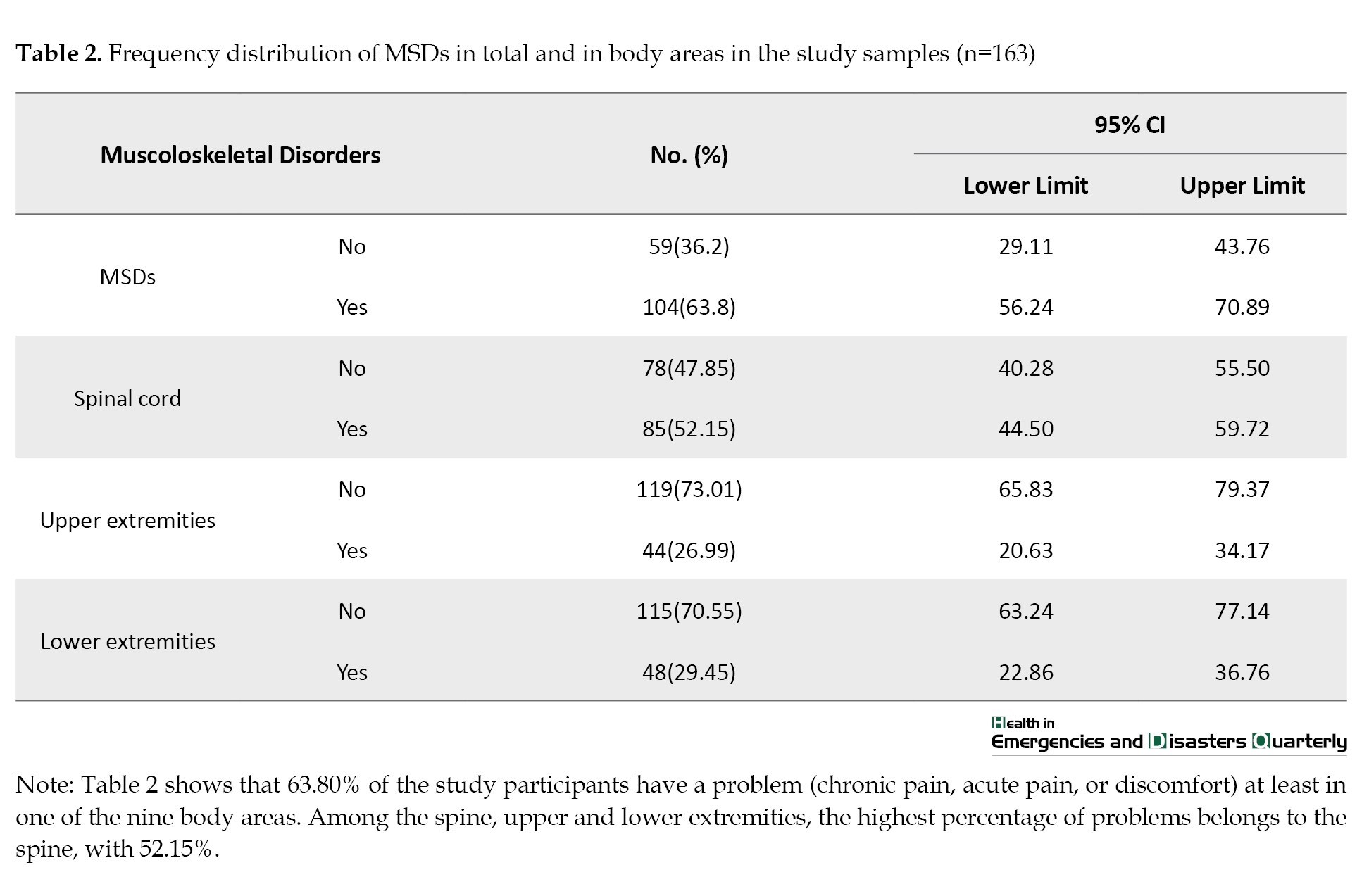
The results of the Kolmogorov-Smirnov test showed that none of the subscales and scales’ scores were normally distributed. The study results also showed that 63.80% of the research samples had a problem (chronic pain, acute pain, or discomfort) in at least one of the 9 body areas. Among the spine, upper and lower extremities, the highest percentage of problems was in the spine at 52.15% (Table 2).
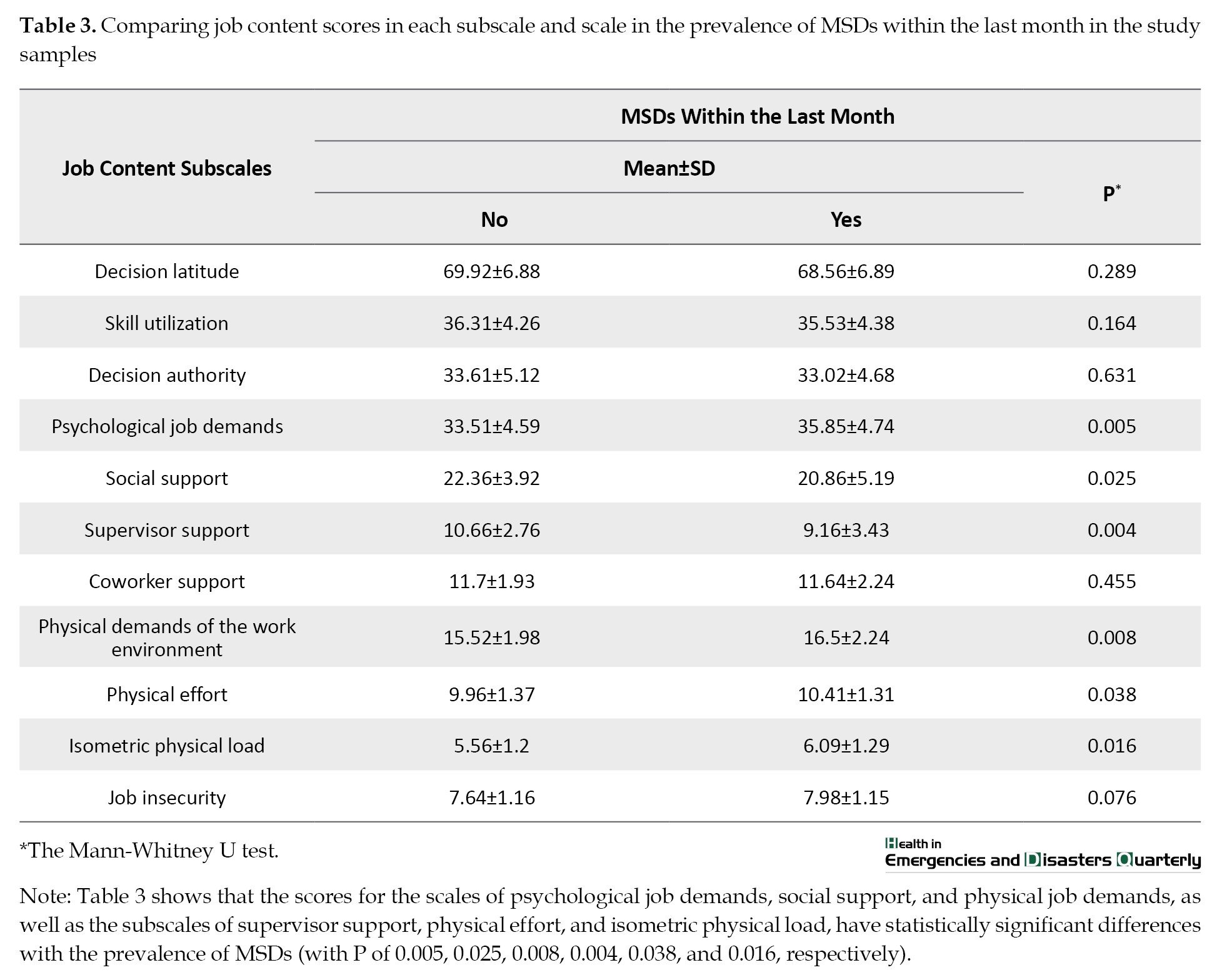
The findings showed that the highest frequency percentage of MSDs was in the lower back (46.01%) and neck (21.47%), and the lowest percentage was in the upper back (8.59%) and elbows (6.13%). Also, the lowest ages for the onset of MSDs were in the upper back and knees, with a Mean±SD of 28.79±5.98 and 29.22±6.42 years, respectively. The highest ages for the onset of these disorders were in the hip/thighs and shoulder, with a Mean±SD of 31.47±8.26 and 32.17±6.19, respectively. The highest percentage of hospitalization due to MSDs was in the lower back at 5.52%, and no one has been hospitalized due to shoulder, back, or wrist disorders. The results from studying the frequency distribution of the research samples showed that the disorders in the lower back were the most common cause of task changes among employees (13.50%.). The lower back was the most common MSD in the past 12 months at 36.20%. Due to these disorders in the lower back, 12.88% of the research samples were prevented from performing daily tasks, 22.70% visited physiotherapists and other health care professionals, 20.86% took medication, and only 6.75% took sick leave. The highest lifetime, annual, monthly, and point prevalence percentages of MSDs were in the lower back, followed by the neck. The lowest annual prevalence percentages of MSDs were in the elbows, hips/thighs, and ankles or feet. The lowest monthly prevalence was in the elbows, and the lowest point prevalence was in the upper back. The results of comparing job content scores in each of the subscales and scales in the past month showed that the scores for the scales of psychological job demands, social support, and physical demands of work environment, and the subscales of supervisor support, physical effort, and isometric physical load had a statistically significant difference with the prevalence of MSDs (P=0.005, P=0.025, P=0.008, P=0.004, P=0.038, and P=0.016, respectively). Individuals with these disorders had higher scores on the scales of psychological job demands, physical demands of the work environment, and the subscales of physical effort and isometric physical load. However, individuals with these disorders had lower scores in the social support scale and the supervisor support subscale (Table 3).
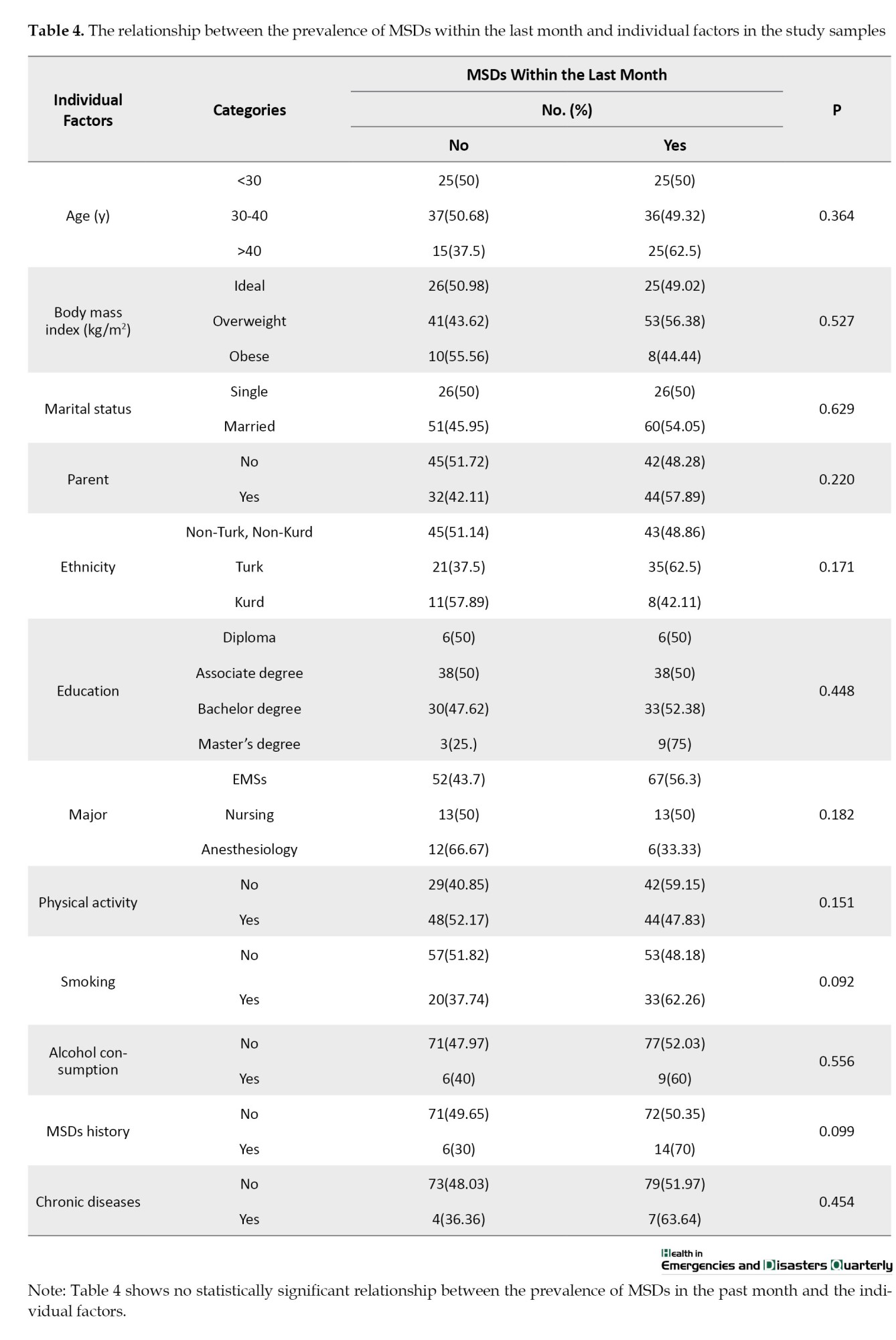
The study showed no statistically significant relationship between the prevalence of MSDs in the past month and individual factors (Table 4).
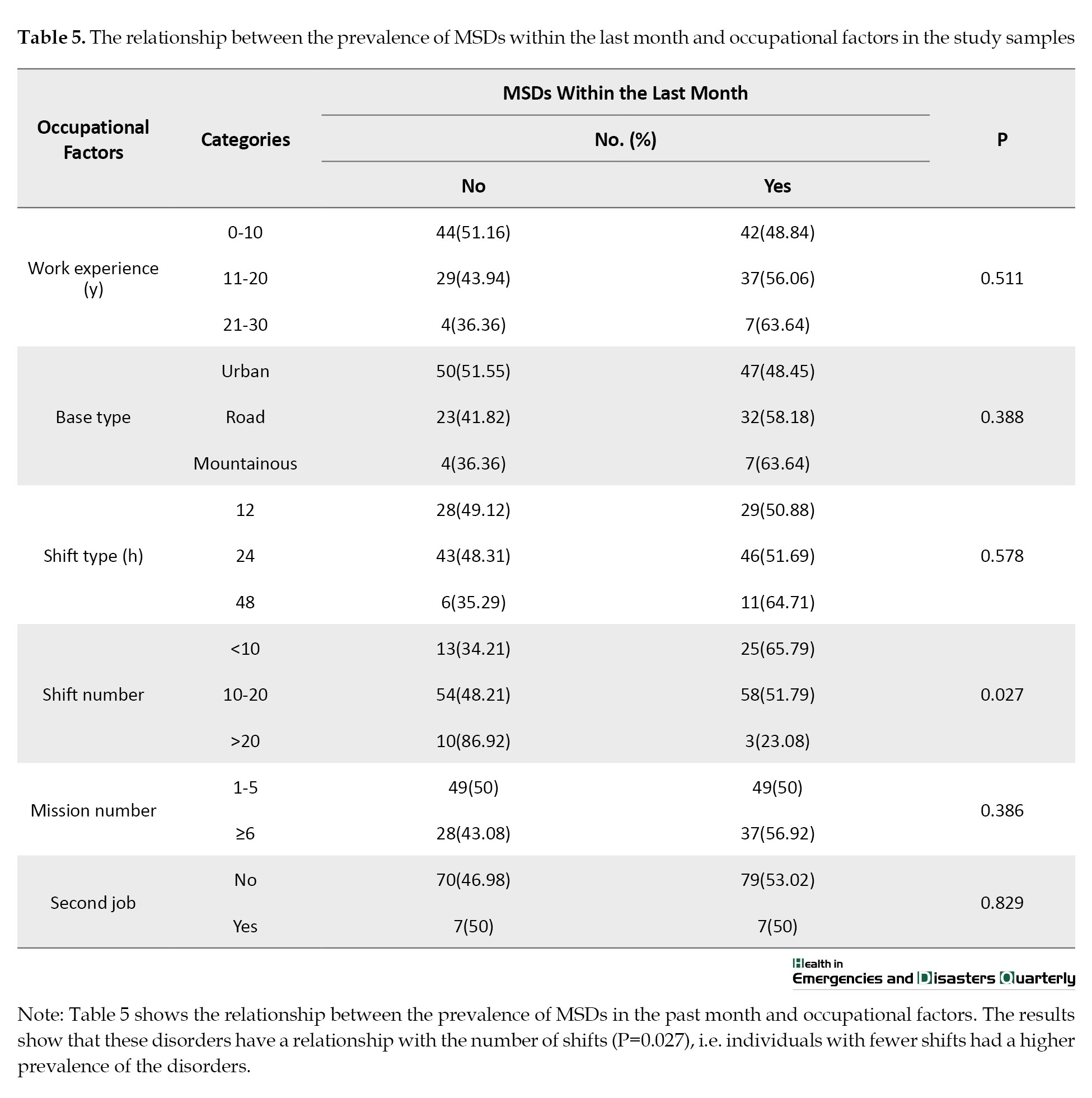
It showed that these disorders had a relationship with the number of shifts as an occupational factor (P=0.027), i.e, the individuals with fewer shifts had more disorders (Table 5).
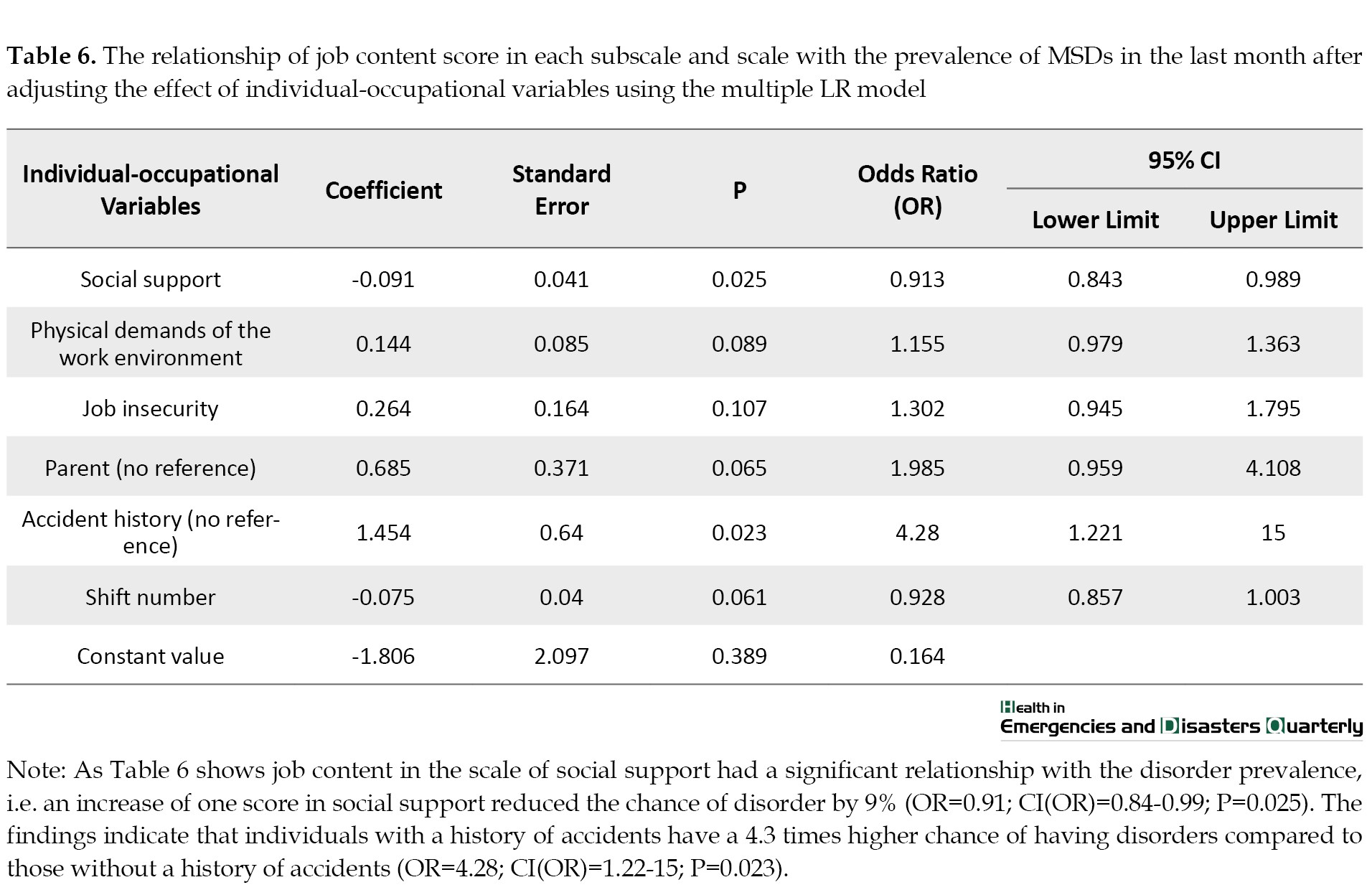
The effect of individual job variables was adjusted using the multiple LR with the backward LR method to determine the relationship between job content scores in each of the scores and the prevalence of MSDs in the past month. It was shown that job content in the social support scale had a significant relationship with the prevalence of the disorder, i.e. the probability of disorder prevalence decreased by 9% with an increase of one point in social support (odds ratio [OR]=0.91; CI(OR), 0.84-0.99; P=0.025). Among individual-job variables, a history of accidents had a statistically significant relationship with the prevalence of MSDs. The findings showed that individuals with a history of accidents had a 4.3 times higher chance of disorder prevalence than those without an accident history (OR=4.28; CI(OR), 1.22-15.00; P=0.023) (Table 6).
Discussion
The Mean±SD scores in the decision latitude scale, with subscales of skill utilization and decision authority, were 69.20±6.90, 35.90±4.33, and 33.30±4.89, respectively. The Mean±SD in the psychological job demands scale was 34.74±4.80. In the social support scale, with supervisor and coworker support subscales, the Mean±SD scores were 21.57±4.68, 9.87±3.21, and 11.67±2.09, respectively. Also, the Mean±SD of the job content score in the physical job demands scale, with physical effort and isometric physical load subscales, were 16.04±2.17, 10.2±1.36, and 5.84±1.27, respectively. Finally, the Mean±SD job insecurity scale score was 7.82±1.16. In the present study, the highest scores for job content status were seen in decision latitude or control, skill utilization, and decision authority. This finding is consistent with Aasa’s study in Sweden, which examined the job content status of 1187 emergency personnel [35]. However, contrary to the present study’s findings, a study in China by Zhang et al., involving 1560 emergency personnel, reports that physical effort and job insecurity are the most common fields among employees [36]. Differences in job content status in various studies may be attributed to variations in measurement tools, study methodologies, and individual and occupational differences among employees, such as major, gender, work experience, and shift type [37].
It was found that the higher the mean scores on the scales of decision latitude and social support are, the lower the stress is, while the higher the mean scores on the scales of psychological job demands, physical job demands, and job insecurity are, the higher the stress is. This finding was confirmed by Clari et al. in Italy in a study aimed at determining work-related MSDs in the upper extremities among operating room nurses [38]. However, contrary to the present study’s findings, Heydari et al. showed no relationship between the scores of decision latitude and social support in a study aimed at examining individual and occupational risk factors in the prevalence and outcomes of MSDs among 114 rescue personnel in Qazvin City, Iran [39]. Differences in study findings can be attributed to individual characteristics, such as prior MSD history, work experience, and different job conditions (number of shifts, major, and education) among the research samples.
The results of the present study showed that the highest lifetime, annual, monthly, and point prevalence percentages of MSDs were in the lower back, followed by the neck. Also, the lowest annual prevalence of MSDs was in the elbows, hips/thighs, and ankles or feet. The lowest monthly prevalence was in the elbows, and the lowest point prevalence was in the upper back. This finding was confirmed by the study of Bazazan et al. [40]. However, study findings from China [36], South Korea [19], and Sweden [35] were inconsistent with the present study’s results. The differences may be attributed to varying perceptions of physical activities among employees, the type and intensity of activities, and the workload of personnel shifts.
This study showed that 63.80% of the research samples had experienced problems (chronic pain, acute pain, or discomfort) in at least one of the 9 body areas. Among the spine, upper and lower extremities, the highest percentage of problems was seen in the spine at 52.15%. This finding was consistent with a study in the United States [41]. Conversely, Bazazan et al. reported that most pain issues were in the lower extremities [40]. The youngest age for the onset of MSDs was in the upper back and knees, with a Mean±SD of 28.79±5.98 and 29.22±6.42 years, respectively. The oldest age for the onset of these disorders was in the hips/thighs and shoulders, with a Mean±SD of 31.47±8.26 and 32.17±6.19 years, respectively. It is evident that the age variable, along with other variables, can influence the onset and type of disorders. Moreover, the highest percentage of hospitalizations due to MSDs was in the lower back, at 5.52%. No one was hospitalized due to shoulder, back, or wrist disorders. This finding is consistent with the study by Heydari et al. [39]. However, the study by Aasa in Sweden, which examined the job content status of 1187 EMS personnel [35], showed results contrary to the present study’s findings, indicating that shoulder and wrist disorders were also causes of hospitalization related to MSDs. The differences may be due to the occupational variables, such as the number of missions and the safety of the equipment used, and individual characteristics, such as work experience, education, age, and previous MSDs in the study participants.
The results of this study showed that the score for the scale of social support and the subscale of supervisor support had statistically significant relationships with the prevalence of MSDs. Those with these disorders had lower scores on the social support scales and the supervisor support subscale. This finding is consistent with the study by Kim et al. [42,]. However, contrary to the present study’s findings, Zhang et al. studied 1560 emergency personnel and reported no statistically significant relationships between social support and supervisor support scores with the prevalence of MSDs [36]. This discrepancy may result from differences in the level of social support for emergency service personnel in different countries. Moreover, individuals with physical problems perceive job content as more burdensome, which can influence their scores in the social support scales and the supervisor support subscale.
The results of the present study showed that individuals with MSDs scored higher on the scales of psychological job demands, physical demands of work environment, and the subscales of physical effort and isometric physical load, whereas they scored lower on the scale of social support and the subscale of supervisor support. Individuals with these disorders scored higher on the scale of psychological work demands; however, they scored lower on the scale of social support and the subscale of supervisor support. The scores for the scales of psychological job demands, social support, and physical demands of the work environment and the subscales of supervisor support, physical effort, and isometric physical load had a statistically significant difference with the prevalence of MSDs. This finding was consistent with the study by Bazazan et al. [40]. Conversely, a study from China shows no relationship between the prevalence of MSDs and the scales of supervisor support, physical effort, and isometric physical load. This discrepancy may be attributed to differences in individual and occupational variables such as gender, age, work experience, major, and the number of missions [36, 43].
The results of the present study showed that the job content score only on the scale of social support had a significant relationship with the prevalence of these disorders, i.e, an increase of one point in social support reduced the chance of the disorder prevalence by 12%. This finding was confirmed by Clari et al. [38]. However, the study by Aasa in Sweden, which examined the job content status of 1187 EMS personnel, reports no relationship between the job content score in the social support scale and the prevalence of MSDs among operational personnel [35]. This finding may be due to individual differences in the research samples, such as gender, age, previous history of MSDs, and body mass index (BMI).
Among the individual-occupational variables, BMI and history of accidents had a statistically significant relationship with the prevalence of MSDs; i.e, each unit increase in BMI raises the chance of the disorder prevalence by 1.1 times. Furthermore, individuals with a history of accidents had a 5.5 times higher chance of the disorder prevalence compared to those without a history of accidents. The relationship between BMI and accident history with the prevalence of MSDs was confirmed by the study of Heydari et al. [39]. No opposing studies were found. Therefore, a higher BMI, which is along with being overweight, can be an important risk factor for the increased prevalence of MSDs among operational personnel in EMS due to its harmful physical effects.
Conclusion
Overall, given that 57.67% of the study participants were overweight and there is a direct relationship between BMI and the prevalence of MSDs, it is recommended to provide EMS personnel with education on healthy lifestyle practices, including weight loss. Also, future studies are encouraged to closely examine the relationship between BMI and the prevalence of MSDs and to focus on teaching healthy lifestyle habits to reduce weight among EMS personnel. Moreover, considering that the personnel received the lowest scores in job insecurity, physical effort, isometric physical load, and physical needs, appropriate measures should be taken to investigate the reasons for the low scores in these areas and implement interventions to enhance them. Given the direct relationship between social support and reduced prevalence of MSDs among EMS personnel, it is recommended to take action to provide greater social support to the personnel. Since the highest percentage of hospitalization due to MSDs has been related to the lower back (52.5%), and no one has been hospitalized due to shoulder, back, and wrist disorders, it is suggested that future training and potential actions focus on reducing the risk of lower back pain.
Since MSDs and their relationships with job content in EMSs who are the front line of out-of-hospital care for patients in different environments are very important, appropriate training and retraining courses related to strategies for self-care against job pressures must be provided for them. It also seems necessary to hold training classes by the training supervisors of medical centers and universities of medical sciences to familiarize personnel with personal care principles to prevent musculoskeletal injuries during work. On the other hand, training alone is not enough, but continuous evaluation of employees in terms of physical health and vital functions is necessary to prevent future damage. Also, it is important to include necessary training related to the job content in the nursing curriculum.
In the management field, after sufficiently recognizing the personnel exposed to musculoskeletal injuries, managers and policymakers can implement necessary interventions for the personnel exposed to injuries by formulating plans, such as self-care training during the mission to prevent possible injuries and appropriate interventions in the weak areas of job content. Also, holding national trauma congresses to exchange opinions, share specialized experiences, and introduce new scientific findings in prevention, relief, and treatment to improve the status of occupational content and muscle injuries among employees are effective measures.
Study limitations
Due to the conditions caused by the COVID-19 pandemic at the time of the study, restrictions on traffic, and reduced face-to-face interactions, the sampling was done slowly. To improve these conditions, the researchers tried to sample wherever possible. Additionally, some individuals were unwilling to cooperate due to personal and work-related issues, for which the researchers assured them of confidentiality and adherence to the principle of privacy.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Guilan University of Medical Sciences, Rasht, Iran (Code: IR.GUMS.REC.1400.212).
Funding
The paper was extracted from the master's thesis of Reza Ghanbari Nikoo, approved by the Department of Nursing, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran. This research did not receive any grant.
Authors' contributions
Study design: Negar Pourvakhshouri, and Mohammad Taghi Moghaddamnia; Data collection: Reza Ghanbari Nikoo; Data analysis: Saman Maroufizah; Writing the original draft: Negar Pourvakhshoori; Critical revisions for important intellectual content: Negar Pourvakhshoori, and Mohammad Taghi Moghaddamnia; Supervision: Mohammad Taghi Moghaddamnia, Yousof Akbari Shahrestanaki, and Negar Pourvakhshoori.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors appreciate all the EMS personnel who participated in this study.
References
Today, the emergency medical service (EMS) is one of the critical components of the healthcare system [1] since EMS can save lives by providing rapid, efficient, and effective care [2]. EMS meets specific health needs outside of hospitals, focusing on life-threatening injuries, patient transport, inter-facility transfers, and preparedness for missions in health emergencies [3]. Furthermore, EMS personnel are dispatched to road and non-road accidents [4]. Poor psychosocial conditions can negatively impact personnel health. Research over the past two decades has shown that poor psychosocial work conditions adversely affect health, particularly in EMS personnel, whose profession is often with challenges [5-8]. Job content poses multiple threats, including musculoskeletal disorders (MSDs) [9]. MSDs are among the prominent issues in occupational health and ergonomics. These disorders are prevalent across various jobs and a significant global challenge [10, 11, 12]. MSDs affect different body parts, such as muscles, bones, tendons, ligaments, joints, nerves, and blood vessels, leading to injury or discomfort accompanied by pain or inflammation. Work conditions can cause or exacerbate these disorders [9]. The consequences of MSDs in the workplace include disability, lost work time, compensation claims, and treatment costs [13].
Typically, employed individuals experience musculoskeletal discomfort at least once in their lifetime. Studies have shown that MSDs account for more than half of work absences and approximately 50% of occupational diseases [14]. Hence, special attention should be paid to the prevalence of these disorders in various work environments. Studies have reported that MSDs occur in healthcare professions (e.g. EMS technicians and nurses) and specialized fields (e.g. emergency rooms, orthopedics) [15-18]. It is also estimated that nearly one-third of all sick leave among healthcare personnel is related to these disorders [19]. A review of studies indicates that healthcare professionals are at risk of developing MSDs due to repetitive tasks, high workload, poor work conditions, patient transfer, psychological factors like job stress, and work shifts [20-23]. Dehdashti et al. assessed the posture of nurses at Velayat Hospital in Damghan City, Iran, during their job duties and its impact on the occurrence of MSDs. The results indicated that the risk of symptoms manifestation was high (risk levels of 2 and 3). The study also showed that the emergency department had the highest level of risk. The authors noted that corrective measures might be necessary in the intensive care unit (ICU) and coronary care unit (CCU) departments, but they believed these measures were especially crucial in the emergency and surgical departments [24]. Therefore, preventing MSDs in a working population requires evaluating job-related factors and individual characteristics and determining the association between these factors and disorders. The World Health Organization (WHO), the Occupational Safety and Health Administration of the USA (OSHA), and the UK Health and Safety Executive (HSE) have emphasized controlling and preventing these disorders, making them a priority. The nature of health and medical personnel’s jobs constantly exposes them to physical and psychological fatigue, so research on this topic is highly important. Such pressures and occupational injuries can adversely impact the services of EMS personnel to the entire community [25].
Studies indicate that considering job content as one of the psychosocial evaluation criteria that can lead to MSDs is important. It has been shown that a low level of job content among employees increases their vulnerability to MSDs [25]. Also, the relationship between job content and MSDs has been confirmed in various studies [26-28]. The nature, scope, and job content of pre-hospital EMS and the associated outcomes, including MSDs, considering variables such as culture, customs, climatic conditions in different regions of the country, demographic features, job characteristics regarding mission diversity, and the newly established nature of EMS organization, highlight the necessity of conducting studies in the field of pre-hospital EMS. Moreover, understanding the nature and content of EMS can enhance the job quality of its personnel. Ultimately, reducing the complications and outcomes associated with these disorders improves their quality of life and provides patients with more effective assistance. Therefore, this study was conducted to determine the relationship between job content and MSDs among operational staff of EMS working in Qazvin Province, Iran.
Materials and Methods
In the present analytical cross-sectional study, 163 samples of operational staff of EMS across 38 bases in Qazvin were selected by census method. The inclusion criteria for the study included having work experience of more than six months and agreement to participate in the study, while the exclusion criterion was partial (less than 50%) completion of the questionnaire. Furthermore, non-operational staff (supervisors or dispatchers) did not participate in the study. Data were collected using a three-part questionnaire. The first part included demographic characteristics (age, height, weight, marital status, smoking habits, alcohol consumption, education level, major, work experience, number of missions per shift, number of children, and physical activity). The second part contained the job content questionnaire (JCQ); the third consisted of the extended Nordic musculoskeletal questionnaire.
The JCQ contained 52 items, including 9 items for assessing the scale of decision latitude, 6 for the subscale of skill utilization, 3 for the subscale of decision authority, 5 for the scale of psychological job demands, 8 for social support, 4 for coworker social support, 4 for supervisor social support, 5 for physical job demands, 3 for physical effort, 2 for isometric physical load, and 3 for job insecurity. Each questionnaire item was scored on a 4-point Likert scale (strongly disagree=1 to strongly agree=4). To compute scores, a higher score than the sample mean should be considered for job demands, and a lower score than the sample mean for decision latitude [29]. The psychometric properties and reliability of the JCQ have been examined and confirmed in numerous studies; for instance, in the Sasaki et al. [6] study, the Cronbach α coefficients were calculated for each of the 4‐factor scores (i.e. psychological demand, decision latitude, supervisor support, and coworker support) of JCQ in Vietnamese staff. The Cronbach α>0.7 was the criterion for acceptability with the statistical significance P<0.05 [30-33]. Additionally, permission to use this tool was obtained from the questionnaire designer via email.
The extended Nordic musculoskeletal questionnaire (NMQ-E) includes 11 items covering 9 different body areas: Neck, shoulders, upper back, elbows, wrists/hands, lower back, pelvis/thighs, knees, and ankles/feet. This tool uses a binary format (yes=1 point, no=0 point) [30]. Scores are calculated based on the 9 body areas, ranging from 0 to 99 points, and the mean score is used for interpretation. The questionnaire is completed through self-reporting (on paper, by phone, online) or via interview. Responses are given in a yes-no format and a 5-point Likert scale ranging from “strongly agree” to “strongly disagree.” The questionnaire covers 9 body areas (three upper extremities, three spine areas, and three lower extremities). Thus, a completed questionnaire can provide 99 data points (excluding age-related data). The questions first inquire about the presence or absence of pain throughout life, its prevalence, and finally, the consequences of the pain. Respondents must answer all questions about one body area before moving to another. If a “yes” response is given to any question about a specific body area, the respondent continues answering the questions for that area until all questions are completed. If the response is “no,” the respondent stops answering questions for that area, and the remaining questions are automatically considered negative, moving on to other body areas. The validity and reliability of this tool have been confirmed in various studies [29, 34]. In the Mokhtarinia study, the translation and localization of the NMQ-E were deemed easy and acceptable. All the items in the questionnaire had acceptable face validity. The intra-class correlation coefficient and the standard error of measurement of the Persian version of the NMQ-E were deemed acceptable (SEM=0.56-1.76 and ICC>0.7), and the Kappa coefficient was calculated as 0.78-1.00 [34].
The study data were collected after obtaining approval from the Ethics Committee and the Research Office of Guilan University of Medical Sciences (GUMS), giving an introduction letter to the relevant center, and obtaining agreement from the responsible authorities and permission to be present in the research environment. Then, the study objectives were explained to the participants, and the importance of confidentiality and the voluntary nature of participation were emphasized. Moreover, the participants could withdraw from completing the questionnaire. The questionnaires were filled out without inserting names. Data analysis was performed using SPSS software, version 16. Quantitative variables were reported as Mean±SD for data analysis, and qualitative variables were reported as frequency (percentage). In univariate analyses, logistic regression (LR) models (crude odds ratios) were used to examine the relationship between individual job variables and job content status with MSDs. In multivariate analyses, multiple LR models (adjusted odds ratios) were used to determine factors associated with MSDs to control and adjust for other variables. The data were analyzed using SPSS software, version 16, and a significance level was considered at 0.05.
Results
The study included 163 male participants aged 21-55 years. The Mean±SD age of the participants was 34.42±7.47 years. In total, 57.67% of the participants were overweight. Most participants were married (68.10%), and 53.37% had no children. Most participants were non-Turk and non-Kurd (53.99%). Among the participants, 73.01% had studied EMS and mostly had an associate degree (46.63%). Most participants engaged in physical activity weekly (56.44%). In total, 32.52% were smokers, and only 9.20% consumed alcohol. Additionally, 12.27% had a history of accidents, and only 6.75% had chronic illnesses. Most participants had less than 11 years of work experience (52.76%) (minimum: 1 year; maximum: 29 years), with a Mean±SD of 10.02±6.55 years. In total, 59.51% were working at urban emergency bases. Most participants had a 24-hour shift schedule (54.60%), and 68.71% had 10-20 shifts per month. The Mean±SD number of monthly shifts was 12.22±4.71. Most participants had 1-6 missions (60.12%), and only 8.59% had a second job.
The results showed that the higher the mean score of the decision latitude and social support scale, the lower the stress is. Conversely, the higher the mean score of the psychological job demands, physical job demands, and job insecurity scale, the higher the stress is. The Mean±SD of the scores in the decision latitude scale, with subscales of skill utilization and decision authority, were 69.20±6.90, 35.90±4.33, and 33.30±4.89, respectively. The Mean±SD score in the psychological job demands scale was 34.74±4.80. In the social support scale, with supervisor and coworker support subscales, the Mean±SD scores were 21.57±4.68, 9.87±3.21, and 11.67±2.09, respectively. Also, the Mean±SD of the job content score in the physical job demands scale, with subscales of physical effort and isometric physical load, were 16.04±2.17, 10.20±1.36, and 5.84±1.27, respectively. Finally, the job insecurity scale’s Mean±SD score was 7.82±1.16 (Table 1).
The results of the Kolmogorov-Smirnov test showed that none of the subscales and scales’ scores were normally distributed. The study results also showed that 63.80% of the research samples had a problem (chronic pain, acute pain, or discomfort) in at least one of the 9 body areas. Among the spine, upper and lower extremities, the highest percentage of problems was in the spine at 52.15% (Table 2).
The findings showed that the highest frequency percentage of MSDs was in the lower back (46.01%) and neck (21.47%), and the lowest percentage was in the upper back (8.59%) and elbows (6.13%). Also, the lowest ages for the onset of MSDs were in the upper back and knees, with a Mean±SD of 28.79±5.98 and 29.22±6.42 years, respectively. The highest ages for the onset of these disorders were in the hip/thighs and shoulder, with a Mean±SD of 31.47±8.26 and 32.17±6.19, respectively. The highest percentage of hospitalization due to MSDs was in the lower back at 5.52%, and no one has been hospitalized due to shoulder, back, or wrist disorders. The results from studying the frequency distribution of the research samples showed that the disorders in the lower back were the most common cause of task changes among employees (13.50%.). The lower back was the most common MSD in the past 12 months at 36.20%. Due to these disorders in the lower back, 12.88% of the research samples were prevented from performing daily tasks, 22.70% visited physiotherapists and other health care professionals, 20.86% took medication, and only 6.75% took sick leave. The highest lifetime, annual, monthly, and point prevalence percentages of MSDs were in the lower back, followed by the neck. The lowest annual prevalence percentages of MSDs were in the elbows, hips/thighs, and ankles or feet. The lowest monthly prevalence was in the elbows, and the lowest point prevalence was in the upper back. The results of comparing job content scores in each of the subscales and scales in the past month showed that the scores for the scales of psychological job demands, social support, and physical demands of work environment, and the subscales of supervisor support, physical effort, and isometric physical load had a statistically significant difference with the prevalence of MSDs (P=0.005, P=0.025, P=0.008, P=0.004, P=0.038, and P=0.016, respectively). Individuals with these disorders had higher scores on the scales of psychological job demands, physical demands of the work environment, and the subscales of physical effort and isometric physical load. However, individuals with these disorders had lower scores in the social support scale and the supervisor support subscale (Table 3).
The study showed no statistically significant relationship between the prevalence of MSDs in the past month and individual factors (Table 4).
It showed that these disorders had a relationship with the number of shifts as an occupational factor (P=0.027), i.e, the individuals with fewer shifts had more disorders (Table 5).
The effect of individual job variables was adjusted using the multiple LR with the backward LR method to determine the relationship between job content scores in each of the scores and the prevalence of MSDs in the past month. It was shown that job content in the social support scale had a significant relationship with the prevalence of the disorder, i.e. the probability of disorder prevalence decreased by 9% with an increase of one point in social support (odds ratio [OR]=0.91; CI(OR), 0.84-0.99; P=0.025). Among individual-job variables, a history of accidents had a statistically significant relationship with the prevalence of MSDs. The findings showed that individuals with a history of accidents had a 4.3 times higher chance of disorder prevalence than those without an accident history (OR=4.28; CI(OR), 1.22-15.00; P=0.023) (Table 6).
Discussion
The Mean±SD scores in the decision latitude scale, with subscales of skill utilization and decision authority, were 69.20±6.90, 35.90±4.33, and 33.30±4.89, respectively. The Mean±SD in the psychological job demands scale was 34.74±4.80. In the social support scale, with supervisor and coworker support subscales, the Mean±SD scores were 21.57±4.68, 9.87±3.21, and 11.67±2.09, respectively. Also, the Mean±SD of the job content score in the physical job demands scale, with physical effort and isometric physical load subscales, were 16.04±2.17, 10.2±1.36, and 5.84±1.27, respectively. Finally, the Mean±SD job insecurity scale score was 7.82±1.16. In the present study, the highest scores for job content status were seen in decision latitude or control, skill utilization, and decision authority. This finding is consistent with Aasa’s study in Sweden, which examined the job content status of 1187 emergency personnel [35]. However, contrary to the present study’s findings, a study in China by Zhang et al., involving 1560 emergency personnel, reports that physical effort and job insecurity are the most common fields among employees [36]. Differences in job content status in various studies may be attributed to variations in measurement tools, study methodologies, and individual and occupational differences among employees, such as major, gender, work experience, and shift type [37].
It was found that the higher the mean scores on the scales of decision latitude and social support are, the lower the stress is, while the higher the mean scores on the scales of psychological job demands, physical job demands, and job insecurity are, the higher the stress is. This finding was confirmed by Clari et al. in Italy in a study aimed at determining work-related MSDs in the upper extremities among operating room nurses [38]. However, contrary to the present study’s findings, Heydari et al. showed no relationship between the scores of decision latitude and social support in a study aimed at examining individual and occupational risk factors in the prevalence and outcomes of MSDs among 114 rescue personnel in Qazvin City, Iran [39]. Differences in study findings can be attributed to individual characteristics, such as prior MSD history, work experience, and different job conditions (number of shifts, major, and education) among the research samples.
The results of the present study showed that the highest lifetime, annual, monthly, and point prevalence percentages of MSDs were in the lower back, followed by the neck. Also, the lowest annual prevalence of MSDs was in the elbows, hips/thighs, and ankles or feet. The lowest monthly prevalence was in the elbows, and the lowest point prevalence was in the upper back. This finding was confirmed by the study of Bazazan et al. [40]. However, study findings from China [36], South Korea [19], and Sweden [35] were inconsistent with the present study’s results. The differences may be attributed to varying perceptions of physical activities among employees, the type and intensity of activities, and the workload of personnel shifts.
This study showed that 63.80% of the research samples had experienced problems (chronic pain, acute pain, or discomfort) in at least one of the 9 body areas. Among the spine, upper and lower extremities, the highest percentage of problems was seen in the spine at 52.15%. This finding was consistent with a study in the United States [41]. Conversely, Bazazan et al. reported that most pain issues were in the lower extremities [40]. The youngest age for the onset of MSDs was in the upper back and knees, with a Mean±SD of 28.79±5.98 and 29.22±6.42 years, respectively. The oldest age for the onset of these disorders was in the hips/thighs and shoulders, with a Mean±SD of 31.47±8.26 and 32.17±6.19 years, respectively. It is evident that the age variable, along with other variables, can influence the onset and type of disorders. Moreover, the highest percentage of hospitalizations due to MSDs was in the lower back, at 5.52%. No one was hospitalized due to shoulder, back, or wrist disorders. This finding is consistent with the study by Heydari et al. [39]. However, the study by Aasa in Sweden, which examined the job content status of 1187 EMS personnel [35], showed results contrary to the present study’s findings, indicating that shoulder and wrist disorders were also causes of hospitalization related to MSDs. The differences may be due to the occupational variables, such as the number of missions and the safety of the equipment used, and individual characteristics, such as work experience, education, age, and previous MSDs in the study participants.
The results of this study showed that the score for the scale of social support and the subscale of supervisor support had statistically significant relationships with the prevalence of MSDs. Those with these disorders had lower scores on the social support scales and the supervisor support subscale. This finding is consistent with the study by Kim et al. [42,]. However, contrary to the present study’s findings, Zhang et al. studied 1560 emergency personnel and reported no statistically significant relationships between social support and supervisor support scores with the prevalence of MSDs [36]. This discrepancy may result from differences in the level of social support for emergency service personnel in different countries. Moreover, individuals with physical problems perceive job content as more burdensome, which can influence their scores in the social support scales and the supervisor support subscale.
The results of the present study showed that individuals with MSDs scored higher on the scales of psychological job demands, physical demands of work environment, and the subscales of physical effort and isometric physical load, whereas they scored lower on the scale of social support and the subscale of supervisor support. Individuals with these disorders scored higher on the scale of psychological work demands; however, they scored lower on the scale of social support and the subscale of supervisor support. The scores for the scales of psychological job demands, social support, and physical demands of the work environment and the subscales of supervisor support, physical effort, and isometric physical load had a statistically significant difference with the prevalence of MSDs. This finding was consistent with the study by Bazazan et al. [40]. Conversely, a study from China shows no relationship between the prevalence of MSDs and the scales of supervisor support, physical effort, and isometric physical load. This discrepancy may be attributed to differences in individual and occupational variables such as gender, age, work experience, major, and the number of missions [36, 43].
The results of the present study showed that the job content score only on the scale of social support had a significant relationship with the prevalence of these disorders, i.e, an increase of one point in social support reduced the chance of the disorder prevalence by 12%. This finding was confirmed by Clari et al. [38]. However, the study by Aasa in Sweden, which examined the job content status of 1187 EMS personnel, reports no relationship between the job content score in the social support scale and the prevalence of MSDs among operational personnel [35]. This finding may be due to individual differences in the research samples, such as gender, age, previous history of MSDs, and body mass index (BMI).
Among the individual-occupational variables, BMI and history of accidents had a statistically significant relationship with the prevalence of MSDs; i.e, each unit increase in BMI raises the chance of the disorder prevalence by 1.1 times. Furthermore, individuals with a history of accidents had a 5.5 times higher chance of the disorder prevalence compared to those without a history of accidents. The relationship between BMI and accident history with the prevalence of MSDs was confirmed by the study of Heydari et al. [39]. No opposing studies were found. Therefore, a higher BMI, which is along with being overweight, can be an important risk factor for the increased prevalence of MSDs among operational personnel in EMS due to its harmful physical effects.
Conclusion
Overall, given that 57.67% of the study participants were overweight and there is a direct relationship between BMI and the prevalence of MSDs, it is recommended to provide EMS personnel with education on healthy lifestyle practices, including weight loss. Also, future studies are encouraged to closely examine the relationship between BMI and the prevalence of MSDs and to focus on teaching healthy lifestyle habits to reduce weight among EMS personnel. Moreover, considering that the personnel received the lowest scores in job insecurity, physical effort, isometric physical load, and physical needs, appropriate measures should be taken to investigate the reasons for the low scores in these areas and implement interventions to enhance them. Given the direct relationship between social support and reduced prevalence of MSDs among EMS personnel, it is recommended to take action to provide greater social support to the personnel. Since the highest percentage of hospitalization due to MSDs has been related to the lower back (52.5%), and no one has been hospitalized due to shoulder, back, and wrist disorders, it is suggested that future training and potential actions focus on reducing the risk of lower back pain.
Since MSDs and their relationships with job content in EMSs who are the front line of out-of-hospital care for patients in different environments are very important, appropriate training and retraining courses related to strategies for self-care against job pressures must be provided for them. It also seems necessary to hold training classes by the training supervisors of medical centers and universities of medical sciences to familiarize personnel with personal care principles to prevent musculoskeletal injuries during work. On the other hand, training alone is not enough, but continuous evaluation of employees in terms of physical health and vital functions is necessary to prevent future damage. Also, it is important to include necessary training related to the job content in the nursing curriculum.
In the management field, after sufficiently recognizing the personnel exposed to musculoskeletal injuries, managers and policymakers can implement necessary interventions for the personnel exposed to injuries by formulating plans, such as self-care training during the mission to prevent possible injuries and appropriate interventions in the weak areas of job content. Also, holding national trauma congresses to exchange opinions, share specialized experiences, and introduce new scientific findings in prevention, relief, and treatment to improve the status of occupational content and muscle injuries among employees are effective measures.
Study limitations
Due to the conditions caused by the COVID-19 pandemic at the time of the study, restrictions on traffic, and reduced face-to-face interactions, the sampling was done slowly. To improve these conditions, the researchers tried to sample wherever possible. Additionally, some individuals were unwilling to cooperate due to personal and work-related issues, for which the researchers assured them of confidentiality and adherence to the principle of privacy.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Guilan University of Medical Sciences, Rasht, Iran (Code: IR.GUMS.REC.1400.212).
Funding
The paper was extracted from the master's thesis of Reza Ghanbari Nikoo, approved by the Department of Nursing, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran. This research did not receive any grant.
Authors' contributions
Study design: Negar Pourvakhshouri, and Mohammad Taghi Moghaddamnia; Data collection: Reza Ghanbari Nikoo; Data analysis: Saman Maroufizah; Writing the original draft: Negar Pourvakhshoori; Critical revisions for important intellectual content: Negar Pourvakhshoori, and Mohammad Taghi Moghaddamnia; Supervision: Mohammad Taghi Moghaddamnia, Yousof Akbari Shahrestanaki, and Negar Pourvakhshoori.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors appreciate all the EMS personnel who participated in this study.
References
- Cui ER, Beja-Glasser A, Fernandez AR, Grover JM, Mann NC, Patel MD. Emergency medical services time intervals for acute chest pain in the United States, 2015-2016. Prehospital Emergency Care. 2020; 24(4):557-65. [DOI:10.1080/10903127.2019.1676346] [PMID]
- Ghadiri Nejad M, Banar M. Emergency response time minimization by incorporating ground and aerial transportation. Annals of Optimization Theory and Practice. 2018; 1(1):43-57. [DOI:10.22121/aotp.2018.108905.1004]
- Chen AY, Yu TY. Network based temporary facility location for the Emergency Medical Services considering the disaster induced demand and the transportation infrastructure in disaster response. Transportation Research Part B: Methodological. 2016; 91:408-23. [DOI:10.1016/j.trb.2016.06.004]
- Pekanoja S, Hoikka M, Kyngäs H, Elo S. Non-transport emergency medical service missions - a retrospective study based on medical charts. Acta Anaesthesiologica Scandinavica. 2018; 62(5):701-8. [DOI:10.1111/aas.13071] [PMID]
- Pourvakhshoori N, Poursadeghiyan M, Khankeh HR, Harouni GG, Farrokhi M. The simultaneous effects of thermal stress and air pollution on body temperature of Tehran traffic officers. Journal of Environmental Health Science and Engineering. 2020; 18(1):279-84. [DOI:10.1007/s40201-020-00463-2] [PMID] [PMCID]
- Sasaki N, Imamura K, Thuy TTT, Watanabe K, Huong NT, Kuribayashi K, et al. Validation of the Job Content Questionnaire among hospital nurses in Vietnam. Journal of Occupational Health. 2020; 62(1):e12086. [DOI:10.1002/1348-9585.12086] [PMID] [PMCID]
- Armenta-Hernandez OD, Maldonado-Macias AA, Ortiz Solís M, Serrano-Rosa MÁ, Baez-López YA, Hernández-Arellano JL. Effects of Job Content and Physical Activity on Body Mass Index among obese managers of the Mexican manufacturing industry. International Journal of Environmental Research and Public Health. 2020; 17(11):3969. [DOI:10.3390/ijerph17113969] [PMID] [PMCID]
- Pourvakhshoori N, Khankeh HR, Stueck M, Farrokhi M. The association between air pollution and cancers: Controversial evidence of a systematic review. Environmental Science and Pollution Research International. 2020; 27(31):38491-500. [DOI:10.1007/s11356-020-10377-z] [PMID]
- Okezue OC, Anamezie TH, Nene JJ, Okwudili JD. Work-related musculoskeletal disorders among office workers in higher education institutions: A cross-sectional study. Ethiopian Journal of Health Sciences. 2020; 30(5):715-24. [DOI:10.4314/ejhs.v30i5.10] [PMID] [PMCID]
- Aljerian N, Alshehri S, Masudi E, Albawardi AM, Alzahrani F, Alanazi R. The prevalence of musculoskeletal disorders among EMS Personnel in Saudi Arabia, Riyadh. The Egyptian Journal of Hospital Medicine. 2018; 73(1):5777-82. [DOI:10.21608/ejhm.2018.11879]
- Davison C, Cotrim TP, Gonçalves S. Perception of musculoskeletal symptoms and psychosocial risk factors among a sample of portuguese emergency medical technicians. In: Cotrim T, Serranheira F, Sousa P, Hignett S, Albolino S, Tartaglia R, editors. Health and social care systems of the future: Demographic changes, digital age and human factors. HEPS 2019. Advances in Intelligent Systems and Computing, vol 1012. Cham: Springer; 2019. [DOI:10.1007/978-3-030-24067-7_6]
- Imani A, Borna J, Alami A, Khosravan S, Hasankhani H, Bafandeh Zende M. Prevalence of low back pain and its related factors among pre-hospital emergency personnel in Iran. Journal of Emergency Practice and Trauma. 2019; 5(1):8-13. [Link]
- Matifat E, Méquignon M, Cunningham C, Blake C, Fennelly O, Desmeules F. Benefits of Musculoskeletal Physical Therapy in Emergency Departments: A systematic review. Physical Therapy. 2019; 99(9):1150-66. [DOI:10.1093/ptj/pzz082] [PMID]
- Khoshakhlagh AH, Al Sulaie S, Mirzahosseininejad M, Yazdanirad S, Orr RM, Laal F, et al. Occupational stress and musculoskeletal disorders in firefighters: The mediating effect of depression and job burnout. Scientific Reports. 2024; 14(1):4649. [DOI:10.1038/s41598-024-55468-w] [PMID] [PMCID]
- Larouche D, Bellemare M, Prairie J, Hegg-Deloye S, Corbeil P. Overall risk index for patient transfers in total assistance mode executed by emergency medical technician-paramedics in real work situations. Applied Ergonomics. 2019; 74:177-85. [DOI:10.1016/j.apergo.2018.08.029] [PMID]
- Gerbaudo L, Violante B. [Relationship between musculoskeletal disorders and work-related awkward postures among a group of health care workers in a hospital (Italian)]. La Medicina del Lavoro. 2008; 99(1):29-39. [PMID]
- Zakerian SA, Afzalinejhad M, Mahmodi M, Sheibani N. Determining the efficiency of ergonomic belt during patient handling and its effect on reducing musculoskeletal disorders in nurses. SAGE Open Nursing. 2021; 7:23779608211057939. [DOI:10.1177/23779608211057939] [PMID] [PMCID]
- Gómez-Galán M, Pérez-Alonso J, Callejón-Ferre ÁJ, López-Martínez J. Musculoskeletal disorders: OWAS review. Industrial Health. 2017; 55(4):314-37. [DOI:10.2486/indhealth.2016-0191] [PMID] [PMCID]
- Lin SC, Lin LL, Liu CJ, Fang CK, Lin MH. Exploring the factors affecting musculoskeletal disorders risk among hospital nurses. Plos One. 2020; 15(4):e0231319. [DOI:10.1371/journal.pone.0231319] [PMID] [PMCID]
- Bornhöft L, Thorn J, Svensson M, Nordeman L, Eggertsen R, Larsson MEH. More cost-effective management of patients with musculoskeletal disorders in primary care after direct triaging to physiotherapists for initial assessment compared to initial general practitioner assessment. BMC Musculoskeletal Disorders. 2019; 20(1):186. [DOI:10.1186/s12891-019-2553-9] [PMID] [PMCID]
- Calvo-Lobo C, Becerro-de-Bengoa-Vallejo R, Losa-Iglesias ME, Rodríguez-Sanz D, López-López D, San-Antolín M. Biomarkers and nutrients in musculoskeletal disorders. Nutrients. 2021; 13(2):283. [DOI:10.3390/nu13020283] [PMID] [PMCID]
- da Costa BR, Vieira ER. Stretching to reduce work-related musculoskeletal disorders: A systematic review. Journal of Rehabilitation Medicine. 2008; 40(5):321-8. [DOI:10.2340/16501977-0204] [PMID]
- Zahiri HR, Addo A, Park AE. Musculoskeletal disorders in minimally invasive surgery. Advances in Surgery. 2019; 53:209-20. [DOI:10.1016/j.yasu.2019.04.020] [PMID]
- Dehdashti A, Mahjoubi Z, Salarinia A. Impact of nurse’s work related body postures on their musculoskeletal disorders. Koomesh. 2015; 16(3):338-46. [Link]
- Osonuga A, Ayokunle O, Josephine O, Dacosta A. Prevalence of musculoskeletal disorders among brewery workers in south-west Nigeria. International Journal of Medical Research & Health Sciences. 2019; 8(6):99-105. [Link]
- Sorour AS, El-Maksoud MM. Relationship between musculoskeletal disorders, job demands, and burnout among emergency nurses. Advanced Emergency Nursing Journal. 2012; 34(3):272-82. [DOI:10.1097/TME.0b013e31826211e1] [PMID]
- Pope-Ford R, Pope-Ozimba J. Musculoskeletal disorders and emergent themes of psychosocial factors and their impact on health in dentistry. Work. 2020; 65(3):563-71. [DOI:10.3233/WOR-203110] [PMID]
- Krishnan KS, Raju G, Shawkataly O. Prevalence of work-related musculoskeletal disorders: Psychological and physical risk factors. International Journal of Environmental Research and Public Health 2021; 18(17):9361. [DOI:10.3390/ijerph18179361] [PMID] [PMCID]
- Punnett L, Wegman DH. Work-related musculoskeletal disorders: The epidemiologic evidence and the debate. Journal of Electromyography and Kinesiology. 2004; 14(1):13-23. [DOI:10.1016/j.jelekin.2003.09.015] [PMID]
- Boas MV, Cerqueira A. Assessing stress at work: The Portuguese version of the Job Content Questionnaire. Avaliaçao Psicologica: Interamerican Journal of Psychological Assessment. 2017; 16:(1):70-7. [DOI:10.15689/ap.2017.1601.08]
- Santos KOB, Araújo TM, Carvalho FM, Karasek R. The job content questionnaire in various occupational contexts: Applying a latent class model. BMJ Open. 2017; 7(5):e013596. [DOI:10.1136/bmjopen-2016-013596] [PMID] [PMCID]
- Choobineh A, Ghaem H, Ahmedinejad P. Validity and reliability of the Persian (Farsi) version of the Job Content Questionnaire: A study among hospital nurses. Eastern Mediterranean Health Journal. 2011; 17(4):335-41. [DOI:10.26719/2011.17.4.335] [PMID]
- Tabatabaee Jabali SM, Ghaffari M, Pournik O, Ghalichi L, Tehrani Yazdi AR, Motevalian SA. Reliability and validity of Persian version of job content questionnaire in health care workers in Iran. The International Journal of Occupational and Environmental Medicine. 2013; 4(2):96-101. [PMID]
- Mokhtarinia H, Shafiee A, Pashmdarfard M. [Translation and localization of the Extended Nordic Musculoskeletal Questionnaire and the evaluation of the face validity and test-retest reliability of its Persian version (Persian)]. Iranian Journal of Ergonomics. 2015; 3(3):21-9. [Link]
- Aasa U, Barnekow-Bergkvist M, Angquist KA, Brulin C. Relationships between work-related factors and disorders in the neck-shoulder and low-back region among female and male ambulance personnel. Journal of Occupational Health. 2005; 47(6):481-9. [DOI:10.1539/joh.47.481] [PMID]
- Zhang Q, Dong H, Zhu C, Liu G. Low back pain in emergency ambulance workers in tertiary hospitals in China and its risk factors among ambulance nurses: A cross-sectional study. BMJ Open. 2019; 9(9):e029264. [DOI:10.1136/bmjopen-2019-029264] [PMID] [PMCID]
- Friedenberg R, Kalichman L, Ezra D, Wacht O, Alperovitch-Najenson D. Work-related musculoskeletal disorders and injuries among emergency medical technicians and paramedics: A comprehensive narrative review. Archives of Environmental & Occupational Health. 2022; 77(1):9-17. [DOI:10.1080/19338244.2020.1832038] [PMID]
- Clari M, Garzaro G, Di Maso M, Donato F, Godono A, Paleologo M, et al. Upper limb work-related musculoskeletal disorders in operating room nurses: A multicenter cross-sectional study. International Journal of Environmental Research and Public Health. 2019; 16(16):2844. [DOI:10.3390/ijerph16162844] [PMID] [PMCID]
- Heydari P, Varmazyar S, Hakimi C. [Investigation of Individual and occupational risk factors on the prevalence and consequence of musculoskeletal disorders among the Rescue Department Employees in Qazvin in Year 2016 (Persian)]. Journal of Health. 2019; 10(1):73-82. [DOI:10.29252/j.health.10.1.73]
- Bazazan A, Dianat I, Bahrampour S, Talebian A, Zandi H, Sharafkhaneh A, et al. Association of musculoskeletal disorders and workload with work schedule and job satisfaction among emergency nurses. International Emergency Nursing. 2019; 44:8-13. [DOI:10.1016/j.ienj.2019.02.004] [PMID]
- Landsbergis P, Johanning E, Stillo M, Jain R, Davis M. Work exposures and musculoskeletal disorders among railroad maintenance-of-way workers.Journal of Occupational and Environmental Medicine. 2019; 61(7):584-96. [DOI:10.1097/JOM.0000000000001614] [PMID]
- Kim MG, Kim KS, Ryoo JH, Yoo SW. Relationship between occupational stress and work-related musculoskeletal disorders in Korean Male Firefighters. Annals of Occupational and Environmental Medicine. 2013; 25(1):9. [DOI:10.1186/2052-4374-25-9] [PMID] [PMCID]
- Kang SK, Kim W. Work-related musculoskeletal disorders in firefighters. Journal of the Korean Medical Association. 2008; 51(12):1111-7. [DOI:10.5124/jkma.2008.51.12.1111]
Type of article: Research |
Subject:
Emergency
Received: 2024/08/25 | Accepted: 2024/11/15 | Published: 2025/04/1
Received: 2024/08/25 | Accepted: 2024/11/15 | Published: 2025/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
