

Volume 11, Issue 1 (Autumn 2025)
Health in Emergencies and Disasters Quarterly 2025, 11(1): 21-32 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sohrabizadeh S, Bahramzadeh A. A Comparative Review of Disaster Risk Reduction Measures Related to the Health Systems in Iran, Iraq and Afghanistan. Health in Emergencies and Disasters Quarterly 2025; 11 (1) :21-32
URL: http://hdq.uswr.ac.ir/article-1-658-en.html
URL: http://hdq.uswr.ac.ir/article-1-658-en.html



1- Air Quality and Climate Change Research Center, Research Institute for Health Sciences and Environment, Shahid Beheshti University of Medical Sciences, Tehran, Iran. , sohrabizadeh@sbmu.ac.ir
2- Department of Health in Disasters and Emergencies, School of Public Health and Safety, Shahid Behehshti University of Medical Sciences, Tehran, Iran.
2- Department of Health in Disasters and Emergencies, School of Public Health and Safety, Shahid Behehshti University of Medical Sciences, Tehran, Iran.
Keywords: Disaster risk reduction (DRR), Health system, Eastern Mediterranean region (EMRO), Iran, Iraq, Afghanistan
Full-Text [PDF 590 kb]
(1255 Downloads)
| Abstract (HTML) (2790 Views)

Description of the included articles
All included articles were published between 1993 and 2023. The final articles comprised 8 qualitative studies, 3 quantitative studies, and 2 mixed-method studies. The all-hazard approach was the most common disaster approach, which was considered in DRR studies performed in all three settings (4 studies on earthquakes, 2 on drought, and 7 on other hazards) (Table 1).
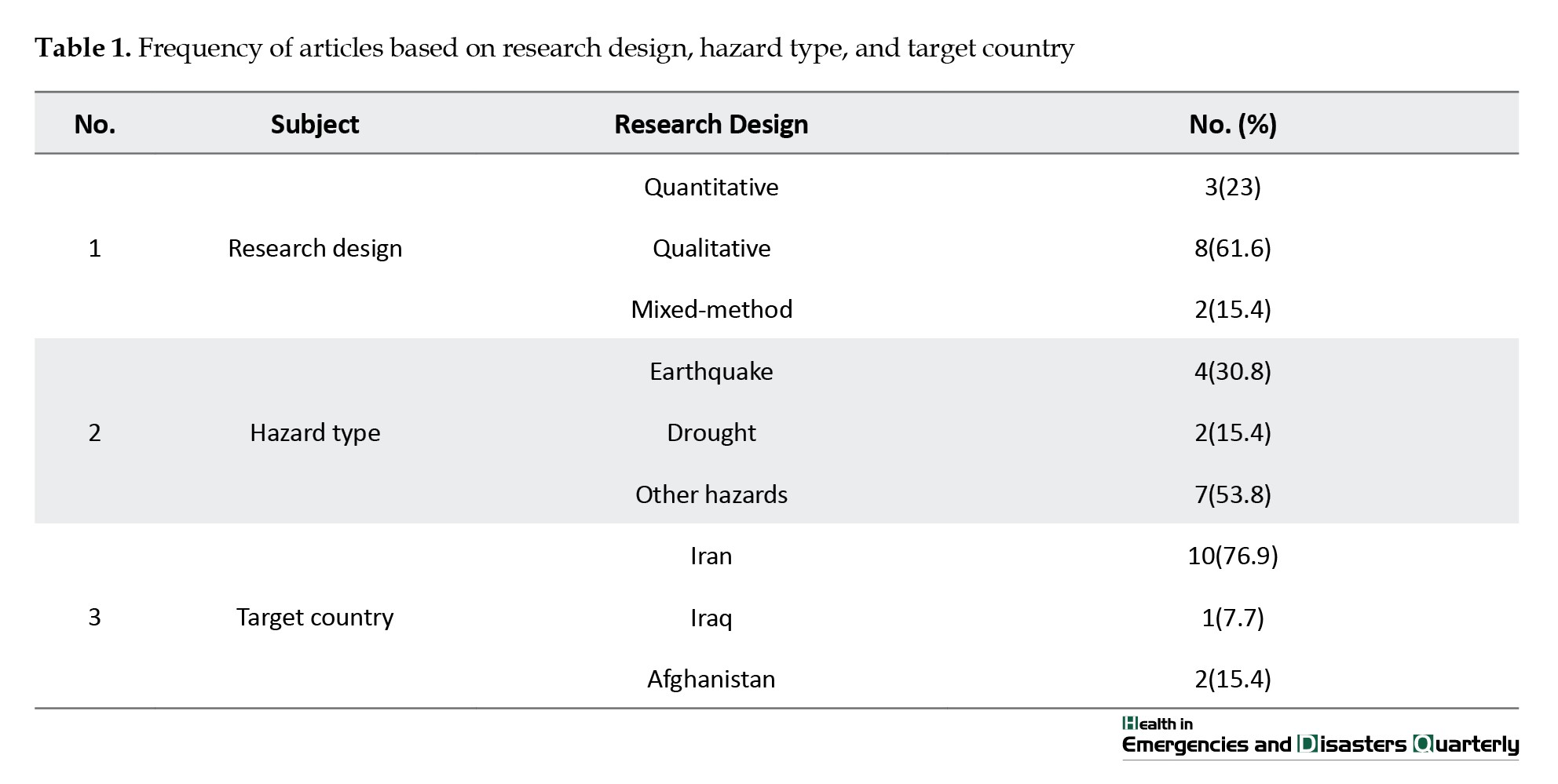
Iran had the highest number of publications regarding DRR and prevention measures (76.9%) compared to Iraq and Afghanistan.
Regarding the disaster management phases, 38% of all included papers were related to the preparedness phase, while the remaining 62% reported on the mitigation and preparedness phases together. Furthermore, the actions taken for DRR were categorized into plans, strategies, and policies. Accordingly, planning for pre-disaster measures was the most common action conducted by countries (62%). In addition, 69% of all included articles investigated pre-disaster measures in the simulated scenario-based hazard conditions rather than in real disasters (Table 2).

Study descriptions based on Iraq, Afghanistan, and Iran
The studies were categorized by country and explained in more detail to highlight the important measures conducted in each setting (Table 3).

Iraq
Of all the included papers, one article reported the necessity of resilience and mitigation for disaster health management in Iraq. This paper focused on planning and policy concerning real disasters and conflicts [15]. The authors highlighted the challenges of health system destruction after disasters (e.g. affecting public and reproductive health services, damage to health facilities), as well as implications for improving the resilience of health systems, such as establishing crisis management plans based on stakeholders’ participation.
Afghanistan
A total of 2 papers addressed the mitigation and DRR measures in the form of planning and policies. Regarding disaster status, these articles considered both real disasters and simulated scenario-based disasters. The vulnerability reduction of buildings in Kabul was the main issue of the authors, who suggested implementing building codes and training engineers to prevent serious health damage resulting from disasters [16]. In addition, droughts, as a climatic disaster, were identified as an important triggering factor for food shortages in Afghanistan. The authors emphasized the necessity of developing an adaptation plan during drought periods [17].
Iran
A total of 10 articles examined the prevention and mitigation issues in the context of Iran. Of these papers, 60% addressed mitigation and DRR issues, while the remaining 40% focused on preparedness. Regarding disaster type, 30% of the included studies dealt with real disasters, and the remaining 70% considered simulated-scenario-based disasters. In addition, 50%, 0% and 50% of articles focused on planning, strategy, and policy, respectively.
The challenges and problems of disaster management were reviewed and reassessed, focusing on the experiences from the Bam earthquake. The authors declared that the important challenges of disaster management during the Bam earthquake were the inadequate coordination and communication between managers and relief organizations. It was emphasized that a unified comprehensive disaster management approach can help improve the DRR and prevention measures and plans [18]. Furthermore, improving disaster risk governance in the health system of Iran requires consideration of effective governance, a prevention culture, and the risk management process. All disaster risk governance documents should be investigated at the national level to develop DRR policies and strategies [19]. The resilience of healthcare centers was investigated, focusing on the structural, non-structural, and safety aspects. This article suggests planning for improving preparedness and flexibility of healthcare centers in Iran [20].
The challenges of early warning systems in the health sector were studied, and the authors identified various political, structural, and management challenges. Regarding management challenges, inadequate education, information, and communication management challenges, weak coordination, insufficient resources, and the lack of rules, protocols, and guidelines were identified. Considering that the establishment or development of a comprehensive early warning system in the health sector was the focus of the authors [21]. Schools are among the important sectors that need to implement health measures in disasters, focusing on DRR and prevention. Accordingly, improving awareness and knowledge in schools can play an important role in improving the safety of students. School officials, students, and parents need to be educated and informed about DRR and prevention measures in schools [22].
The article entitled “how much the Iranian government spent on disasters in the last 100 years- a critical policy analysis” reported that the Iranian government has spent money at the time of disaster strikes rather than on disaster risk management over the last 100 years. In other words, the response and recovery phases received more focus in budget allocation compared to mitigation and DRR in Iran [23]. The implementation of the Sendai Framework for DRR, which is considered one of the important international guidelines in the field of DRR and prevention, was studied in the context of Iran. Accordingly, continuous educational planning and cultural modification are needed to facilitate the long-term implementation of Sendai framework measures in Iran [24].
The challenges faced by the Iranian health system during the Kermanshah earthquake were identified as socio-cultural and psychological factors. The authors indicated that these factors could be considered major challenges for Iran’s health system during disasters and crises. Therefore, policymakers need to consider social, cultural, and psychological elements alongside healthcare factors when planning for DRR and prevention in Iran [25]. Affordable, resilient housing was highlighted as an important issue for improving DRR and prevention following the western earthquake in Iran. Accordingly, challenges, such as inappropriate structures, low-quality materials, and dangerous placements of structures, were identified concerning resilient housing for earthquakes. The modification of construction policies along with making new policies can enhance the structural and non-structural resilience, thereby improving DRR measures [26]. Community-based DRR measures focusing on droughts were considered based on gender distribution in literacy and employment sections in Iran. The authors declared that considering the vulnerabilities and capacities of both female and male populations living in drought-affected regions can improve their health status and resilience during droughts [27].
Discussion
The present review was conducted to compare DRR and prevention strategies and plans of Iran, Iraq, and Afghanistan reported in the literature. The findings showed that Iran benefits from more investigation and evidence-based studies on DRR and prevention compared to Iraq and Afghanistan. While Iraqi publications focused on conflicts and emergencies, the Afghanistan and Iran studies selected an all-hazard approach and natural hazards as the type of disasters. All included studies dealt with the aspects of DRR and prevention in the health systems directly and indirectly. Policies, strategies, and plans related to DRR and pre-disaster measures were suggested more by Iranian investigators compared to researchers from Iraq and Afghanistan.
Our review revealed that the disaster-prone countries, especially the ones in the Middle East, need to establish effective plans and policies focused on DRR and prevention. Similarly, a review of post-disaster health lessons learned in 12 Asian countries highlighted the importance of DRR and preparedness measures before disasters occur. The authors emphasized that investing in community and national health service preparedness should be recognized as a priority for hazard-prone countries. The areas studied for preparedness included health donations and medical volunteers, as well as field hospital preparedness, with a focus on providing material and logistical support post-disasters [28].
In the current review, the structural, non-structural, and functional safety of the health systems and communities, focusing on the community involvement in conducting DRR and prevention plans, were mentioned by all authors from three countries. In accordance with our findings, a review of major earthquakes between 2000 and 2010 suggested that the structural and social factors are influential. DRR and mitigation measures, especially resilient construction, are important for reducing mortality in developing countries. Hospitals, fire departments, and facilities, such as water, telephone, and police stations, also need to be prepared for future earthquakes [29].
Our findings declared that all 3 countries need to consider DRR plans and strategies in the disaster management of their health systems. Similarly, a review of strategies for educating the DRR reported that although most countries tried to begin the DRR education plans and activities, such actions are inadequate, and they need to fill the gap between the current and optimal situations. Establishing the learning and teaching strategies can promote the effectiveness of DRR measures at the community and national levels [30]. DRR education and training are important for the hazard-prone countries, such as Iran, Iraq, and Afghanistan, that suffer from high levels of vulnerabilities.
Climate-related disasters, such as droughts, were considered in the articles included in our review. Accordingly, a review study explained the connection between DRR, climate change adaptation, and sustainable development over the past 30 years. The authors suggested that climate change adaptation is not a subset of DRR, as they have differences and similarities in their scope. However, integrating DRR and climate change adaptation, focusing on governance mechanisms, can decrease the risks of climatic disasters and improve future resilience in countries [31].
Similarly, a review of DRR and climate change adaptations focusing on the governance gap in Malaysia reported that this country needs to integrate climate change into DRR strategies and policies. The authors suggested assessing current strategies and identifying areas for DRR governance and policy-making in Malaysia [32]. In accordance with our findings, a rapid review of the current DRR efforts in Saudi Arabia for extreme heat, droughts, floods, and sandstorms showed that the country has made progress in building codes, infrastructure, early warning systems, and public awareness. The authors implied that emphasizing practical measures for disaster risk management, along with increased efforts to improve important aspects of DRR (e.g. safer buildings, public awareness, and policy-making), can make the country more resilient to disasters [33].
In addition, health facilities need structural and non-structural building resistance, as well as continuous development for broader resilience as a national strategy or set of rules. This can be strengthened by establishing standard instructions and methods in disaster prevention exercises within health systems, especially in developing countries [34]. Consequently, Iran’s health system has developed a safe hospital framework based on World Health Organization (WHO) guidelines, and accordingly, the annual assessment of hospitals and conducting disaster exercises twice a year have been implemented by all hospitals to meet accreditation criteria. It seems that Iraq and Afghanistan can benefit from the lessons learned and experiences of Iran’s health system to establish their DRR structures and measures within their health facilities.
Conclusion
This review focused on DRR policies, plans, and strategies that were reported by researchers from Iraq, Iran, and Afghanistan. DRR measures need to be integrated into all phases of disaster management plans developed for health systems in EMRO countries facing natural and technological hazards and high levels of vulnerabilities. According to our findings, the following suggestions can be considered by policymakers, managers, and researchers in DRR management and prevention.
Establishing a network or platform with the membership of health experts, researchers, and managers who are active in any field of DRR can be effective for sharing all research papers, guidelines, policy briefs, plans, and protocols related to DRR measures conducted in Iran, Iraq, and Afghanistan.
Joint research projects can be designed and conducted by health experts and researchers in DRR management and prevention who have published a considerable number of research and policy papers in Iran, Afghanistan, and Iraq to establish evidence-based policies at the regional levels.
Designing the long-term and short-term educational programs on DRR management and prevention in the health system can be helpful. The target group for such programs is experts, managers, and policymakers who play effective roles in implementing and incorporating DRR measures/plans in their health systems at the local and national levels.
The safety and resilience of health facilities can be considered by establishing rules, policies, and plans that require health officials to adhere to DRR and safety criteria or standards. Accordingly, annual assessments of health facilities can motivate officials to implement DRR and prevention measures within their institutions.
Community-based DRR management and prevention are suggested for involving people in all DRR plans and measures in all hazard-prone regions. Thus, considering the community as one of the main parts of DRR actions can improve community resilience and prevent future disasters.
Moreover, further research is needed to analyze and compare the DRR management and prevention documents published on specific websites or databases of all EMRO countries using their native languages.
Strengths and limitations
This comparative review highlighted the different aspects of DRR plans, strategies, and actions in Iran, Iraq, and Afghanistan as the hazard-prone countries in EMRO. Our findings provide a collection of what these countries have conducted and reported regarding DRR and prevention plans, policies, and measures. This can provide the opportunity to compare the current conditions of these countries, identify gaps, and optimize DRR plans and policies based on various contextual experiences.
There were several limitations during the review process. The PubMed database was used for searching the references since the research topic and keywords were widely applied by various papers published in many journals, making it nearly impossible to manage the large number of references. Since the health system was considered one of our inclusion criteria/keywords, we selected the PubMed database, which indexes health-related journals. Furthermore, our review included published articles in the fields of DRR and prevention and health; however, there is a possibility that some DRR measures or plans have been missed if they were not reported in the relevant databases or published in non-English languages.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by Ethics Committee of the School of Public Health and Safety, Shahid Beheshti University of Medical Sciences, Tehran, Iran (Code: IR.SBMU.PHNS.REC.1401.036).
Funding
This study was funded by the Air Quality and Climate Change Research Center at the Research Institute for Health Sciences and Environment in Shahid Beheshti University of Medical Sciences, Tehran, Iran (Grant No.: 43002269).
Authors' contributions
Conceptualization, data analysis, and project supervision: Sanaz Sohrabizadeh; Data collection: Amirhosein Bahramzadeh; Writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to appreciate all people who facilitate their research process.
Full-Text: (552 Views)
Introduction
Disasters affect people worldwide [1]. According to the United Nations Office for Disaster Risk Reduction (UNDRR) reports, disasters killed over 1.35 million people between 1997 and 2017. This report showed that the distribution of deaths in disasters was disproportionate in low- and middle-income countries (LMICs) compared to developed countries. The health effects of disasters are exacerbated by some factors, such as poverty, fast urbanization, poor infrastructure, inadequate basic health, and lack of warning systems [2]. A considerable number of disasters happened in the Eastern Mediterranean region (EMRO), including earthquakes in Pakistan (2005) and the Islamic Republic of Iran (2003), Horn of Africa droughts (2006), and Yemen landslides (2005). Responding to these disasters needs multi-sectoral capabilities at local, national, and international levels to save lives and prevent injuries and disabilities. Moreover, disasters indirectly affect the physical, environmental, and socio-cultural conditions (e.g. destroying health service infrastructure and community facilities) [3]. Thus, disasters are considered one of the causes of destruction, which can keep countries from further development [4].
Iran and its neighboring countries, such as Afghanistan and Iraq, are located in the EMRO suffering from the different consequences of disasters [5, 6]. The index for risk management (INFORM) ranked Iran, Iraq, and Afghanistan among the top 10 high-risk countries in terms of humanitarian crises in EMRO [7]. The INFORM scores of Iran, Iraq, and Afghanistan were reported to be 5.0, 6.6, and 8.1 in 2023, respectively.
In Iran, about 41 million people were affected by disasters between 1994 and 2013. Accordingly, Iran has been ranked among the top 10 countries with the highest number of people affected by disasters over the past 25 years [8]. Notable disasters, which occurred during the past decades, include the Rudbar-Manjil, Bam, Lorestan, and Zarand earthquakes between 1990 and 2006, the Golestan flash floods between 2000 and 2005, and the Gonu cyclone in 2007 [9]. On the other hand, Iraq confronts a wide range of natural and technological disasters (e.g. droughts, sandstorms, heat waves, floods, desertification, epidemics, and conflicts). The impacts of long-term wars and conflicts have negatively affected people’s lives and resulted in numerous destructions, such as the dysfunctions of disaster management systems and healthcare facilities [10]. In Afghanistan, about 7,016,889 people were affected by a combination of natural and technological disasters. Furthermore, Afghanistan suffered from 153200 internally displaced people in 2005. The consequences of such complex emergencies, along with political issues, have weakened the disaster health management systems in Afghanistan to recover from disasters effects [11].
Regarding the importance of disaster risk reduction (DRR) strategies to prevent the consequences of disasters, a number of frameworks were developed at the international level, such as the Sendai framework for DRR (SFDRR). SFDRR was established at the Third World Conference on DRR in 2015 following the Hyogo framework for DRR. SFDRR was adopted and approved by 187 countries to address the importance of disaster prevention and risk reduction [12]. Furthermore, the sustainable development goals (SDGs) agreement was approved in 2015 to determine the important aspects and indicators of development. Such international frameworks and agreements focus on the reduction of deaths and injuries in disasters, as well as preventing socio-economic and livelihood destruction post-disasters [12, 13]. However, merging DRR strategies and actions into disaster health management in the above-mentioned countries needs to be followed by policymakers and managers at local and national levels [1]. For instance, Iraq’s emergency management agencies continue to focus on the response-based approach to disaster management, neglecting the prevention, mitigation, and preparedness phases. This can happen due to the inadequate governance and awareness about the importance of DRR strategies at the national, regional, and local levels [10]. In Afghanistan, the lack of a national disaster management strategy and disaster preparedness sections, as well as insufficient public awareness, inadequate accessibility to healthcare services, and public health concerns have been reported [11, 14]. In Iran, a number of shortcomings in the disaster response and preparedness systems have been reported after the recent disasters, such as floods and COVID-19 pandemic. Thus, there is a need to focus on the related plans and address the underlying deficiencies [14].
Iran, Iraq, and Afghanistan have been ranked as highly hazard-prone countries where the public frequently suffers from the various consequences of disasters. DRR measures play important roles in promoting community sustainability and protecting people against disasters. Thus, the present review aimed to identify and compare the DRR and prevention strategies, plans, and policies established and implemented in Iran, Iraq, and Afghanistan in terms of health system functions to date. This study can help recognize and share the disaster risk management experiences of these countries with related local, national, and international agencies.
Materials and Methods
Design
The current comparative scoping review was performed using the preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 statement.
Databases and search strategy
At first, we searched several databases to find the scientific literature on DRR in EMRO countries (e.g. PubMed=5322, ScienceDirect=45725, and Google Scholar=1486000). Then, the authors faced a huge number of papers and documents during the initial search and found that it was impossible to collect and screen all documents. Therefore, we limited our database to manage such a large volume of references. Accordingly, based on the study’s aim, the PubMed database was applied for searching the literature. Furthermore, the selection of EMRO countries was limited to the three countries of Iran, Iraq, and Afghanistan. The journals indexed in the PubMed database are often related to various aspects of health systems. Google Scholar was used to check for any missing documents and to locate relevant ones. The literature search was conducted in October 2023.
The keywords for searching the PubMed database were selected based on similar references and articles, as well as suggestions from experts. The main keywords chosen were DRR, plan, strategy, policy, Iran, Afghanistan, and Iraq. The search strategy was created using AND/OR between keywords. Keywords were used in the text, abstracts, and titles of articles. The following search strategy was employed to find the relevant references in the U.S. National Library of Medicine (PubMed database):
(“Disaster risk reduction” OR “emergency risk reduction” OR “crisis risk reduction”) AND (polic* OR plan OR program OR guide OR rule OR framework OR instruction OR Decis* OR “policy-making” OR management OR administration) AND (Afghanistan OR Iran OR Iraq).
Eligibility criteria
The following inclusion and exclusion criteria were used to find the relevant references:
Inclusion criteria
Eligible studies were original research articles that reported on the establishment or implementation of pre-disaster plans, strategies, or policies addressing DRR and management measures. Only studies conducted in Iran, Iraq, or Afghanistan and published in English were included.
Exclusion criteria
Studies were excluded if they focused solely on the response or recovery phases of disaster management, were not published in English, or were presented in the form of books, conference papers, fact sheets, or guidelines. In addition, articles related to COVID-19, other epidemics, or technological disasters were excluded.
Study selection and analysis process
Study selection was performed by the researchers, considering the inclusion and exclusion criteria and using the abstracts and titles. The full texts of all relevant papers were read and analyzed by the researchers. Any paper that met one of the exclusion criteria was removed from the study selection process. In cases of disagreement regarding study selection, the authors independently carried out the procedure until they reached a consensus on including or excluding the references.
Once the study selection was accomplished and the relevant documents were included, primary analysis was performed to identify the characteristics of the selected literature. The authors designed a framework based on the basic information, such as setting, disaster/exposure, and outcomes, as well as the authors’ names, title, publication year, article type, and research design. In addition, a comparative analysis of included papers was conducted in terms of the following three criteria:
Disaster management cycle: Which phase of the disaster management cycle was considered for DRR measures or interventions (mitigation, preparedness, response, and recovery)?
Types of actions: Which kinds of actions were considered for DRR interventions/measures? (plans/programs, strategies, and policies)
Real or simulated scenario-based disasters: Were the DRR experiences related to real disasters or simulated ones?
All included references were assessed by the authors for accuracy and validity confirmation. Mendeley software, version 1.19.8 was used to manage the citations.
Results
A total of 861 papers were found through the initial search. Out of these, 423 articles were removed after reading the titles and abstracts based on the exclusion criteria. The full texts of 438 articles were read, and 13 articles were selected for the final analysis (Figure 1).
Disasters affect people worldwide [1]. According to the United Nations Office for Disaster Risk Reduction (UNDRR) reports, disasters killed over 1.35 million people between 1997 and 2017. This report showed that the distribution of deaths in disasters was disproportionate in low- and middle-income countries (LMICs) compared to developed countries. The health effects of disasters are exacerbated by some factors, such as poverty, fast urbanization, poor infrastructure, inadequate basic health, and lack of warning systems [2]. A considerable number of disasters happened in the Eastern Mediterranean region (EMRO), including earthquakes in Pakistan (2005) and the Islamic Republic of Iran (2003), Horn of Africa droughts (2006), and Yemen landslides (2005). Responding to these disasters needs multi-sectoral capabilities at local, national, and international levels to save lives and prevent injuries and disabilities. Moreover, disasters indirectly affect the physical, environmental, and socio-cultural conditions (e.g. destroying health service infrastructure and community facilities) [3]. Thus, disasters are considered one of the causes of destruction, which can keep countries from further development [4].
Iran and its neighboring countries, such as Afghanistan and Iraq, are located in the EMRO suffering from the different consequences of disasters [5, 6]. The index for risk management (INFORM) ranked Iran, Iraq, and Afghanistan among the top 10 high-risk countries in terms of humanitarian crises in EMRO [7]. The INFORM scores of Iran, Iraq, and Afghanistan were reported to be 5.0, 6.6, and 8.1 in 2023, respectively.
In Iran, about 41 million people were affected by disasters between 1994 and 2013. Accordingly, Iran has been ranked among the top 10 countries with the highest number of people affected by disasters over the past 25 years [8]. Notable disasters, which occurred during the past decades, include the Rudbar-Manjil, Bam, Lorestan, and Zarand earthquakes between 1990 and 2006, the Golestan flash floods between 2000 and 2005, and the Gonu cyclone in 2007 [9]. On the other hand, Iraq confronts a wide range of natural and technological disasters (e.g. droughts, sandstorms, heat waves, floods, desertification, epidemics, and conflicts). The impacts of long-term wars and conflicts have negatively affected people’s lives and resulted in numerous destructions, such as the dysfunctions of disaster management systems and healthcare facilities [10]. In Afghanistan, about 7,016,889 people were affected by a combination of natural and technological disasters. Furthermore, Afghanistan suffered from 153200 internally displaced people in 2005. The consequences of such complex emergencies, along with political issues, have weakened the disaster health management systems in Afghanistan to recover from disasters effects [11].
Regarding the importance of disaster risk reduction (DRR) strategies to prevent the consequences of disasters, a number of frameworks were developed at the international level, such as the Sendai framework for DRR (SFDRR). SFDRR was established at the Third World Conference on DRR in 2015 following the Hyogo framework for DRR. SFDRR was adopted and approved by 187 countries to address the importance of disaster prevention and risk reduction [12]. Furthermore, the sustainable development goals (SDGs) agreement was approved in 2015 to determine the important aspects and indicators of development. Such international frameworks and agreements focus on the reduction of deaths and injuries in disasters, as well as preventing socio-economic and livelihood destruction post-disasters [12, 13]. However, merging DRR strategies and actions into disaster health management in the above-mentioned countries needs to be followed by policymakers and managers at local and national levels [1]. For instance, Iraq’s emergency management agencies continue to focus on the response-based approach to disaster management, neglecting the prevention, mitigation, and preparedness phases. This can happen due to the inadequate governance and awareness about the importance of DRR strategies at the national, regional, and local levels [10]. In Afghanistan, the lack of a national disaster management strategy and disaster preparedness sections, as well as insufficient public awareness, inadequate accessibility to healthcare services, and public health concerns have been reported [11, 14]. In Iran, a number of shortcomings in the disaster response and preparedness systems have been reported after the recent disasters, such as floods and COVID-19 pandemic. Thus, there is a need to focus on the related plans and address the underlying deficiencies [14].
Iran, Iraq, and Afghanistan have been ranked as highly hazard-prone countries where the public frequently suffers from the various consequences of disasters. DRR measures play important roles in promoting community sustainability and protecting people against disasters. Thus, the present review aimed to identify and compare the DRR and prevention strategies, plans, and policies established and implemented in Iran, Iraq, and Afghanistan in terms of health system functions to date. This study can help recognize and share the disaster risk management experiences of these countries with related local, national, and international agencies.
Materials and Methods
Design
The current comparative scoping review was performed using the preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 statement.
Databases and search strategy
At first, we searched several databases to find the scientific literature on DRR in EMRO countries (e.g. PubMed=5322, ScienceDirect=45725, and Google Scholar=1486000). Then, the authors faced a huge number of papers and documents during the initial search and found that it was impossible to collect and screen all documents. Therefore, we limited our database to manage such a large volume of references. Accordingly, based on the study’s aim, the PubMed database was applied for searching the literature. Furthermore, the selection of EMRO countries was limited to the three countries of Iran, Iraq, and Afghanistan. The journals indexed in the PubMed database are often related to various aspects of health systems. Google Scholar was used to check for any missing documents and to locate relevant ones. The literature search was conducted in October 2023.
The keywords for searching the PubMed database were selected based on similar references and articles, as well as suggestions from experts. The main keywords chosen were DRR, plan, strategy, policy, Iran, Afghanistan, and Iraq. The search strategy was created using AND/OR between keywords. Keywords were used in the text, abstracts, and titles of articles. The following search strategy was employed to find the relevant references in the U.S. National Library of Medicine (PubMed database):
(“Disaster risk reduction” OR “emergency risk reduction” OR “crisis risk reduction”) AND (polic* OR plan OR program OR guide OR rule OR framework OR instruction OR Decis* OR “policy-making” OR management OR administration) AND (Afghanistan OR Iran OR Iraq).
Eligibility criteria
The following inclusion and exclusion criteria were used to find the relevant references:
Inclusion criteria
Eligible studies were original research articles that reported on the establishment or implementation of pre-disaster plans, strategies, or policies addressing DRR and management measures. Only studies conducted in Iran, Iraq, or Afghanistan and published in English were included.
Exclusion criteria
Studies were excluded if they focused solely on the response or recovery phases of disaster management, were not published in English, or were presented in the form of books, conference papers, fact sheets, or guidelines. In addition, articles related to COVID-19, other epidemics, or technological disasters were excluded.
Study selection and analysis process
Study selection was performed by the researchers, considering the inclusion and exclusion criteria and using the abstracts and titles. The full texts of all relevant papers were read and analyzed by the researchers. Any paper that met one of the exclusion criteria was removed from the study selection process. In cases of disagreement regarding study selection, the authors independently carried out the procedure until they reached a consensus on including or excluding the references.
Once the study selection was accomplished and the relevant documents were included, primary analysis was performed to identify the characteristics of the selected literature. The authors designed a framework based on the basic information, such as setting, disaster/exposure, and outcomes, as well as the authors’ names, title, publication year, article type, and research design. In addition, a comparative analysis of included papers was conducted in terms of the following three criteria:
Disaster management cycle: Which phase of the disaster management cycle was considered for DRR measures or interventions (mitigation, preparedness, response, and recovery)?
Types of actions: Which kinds of actions were considered for DRR interventions/measures? (plans/programs, strategies, and policies)
Real or simulated scenario-based disasters: Were the DRR experiences related to real disasters or simulated ones?
All included references were assessed by the authors for accuracy and validity confirmation. Mendeley software, version 1.19.8 was used to manage the citations.
Results
A total of 861 papers were found through the initial search. Out of these, 423 articles were removed after reading the titles and abstracts based on the exclusion criteria. The full texts of 438 articles were read, and 13 articles were selected for the final analysis (Figure 1).
Description of the included articles
All included articles were published between 1993 and 2023. The final articles comprised 8 qualitative studies, 3 quantitative studies, and 2 mixed-method studies. The all-hazard approach was the most common disaster approach, which was considered in DRR studies performed in all three settings (4 studies on earthquakes, 2 on drought, and 7 on other hazards) (Table 1).
Iran had the highest number of publications regarding DRR and prevention measures (76.9%) compared to Iraq and Afghanistan.
Regarding the disaster management phases, 38% of all included papers were related to the preparedness phase, while the remaining 62% reported on the mitigation and preparedness phases together. Furthermore, the actions taken for DRR were categorized into plans, strategies, and policies. Accordingly, planning for pre-disaster measures was the most common action conducted by countries (62%). In addition, 69% of all included articles investigated pre-disaster measures in the simulated scenario-based hazard conditions rather than in real disasters (Table 2).
Study descriptions based on Iraq, Afghanistan, and Iran
The studies were categorized by country and explained in more detail to highlight the important measures conducted in each setting (Table 3).
Iraq
Of all the included papers, one article reported the necessity of resilience and mitigation for disaster health management in Iraq. This paper focused on planning and policy concerning real disasters and conflicts [15]. The authors highlighted the challenges of health system destruction after disasters (e.g. affecting public and reproductive health services, damage to health facilities), as well as implications for improving the resilience of health systems, such as establishing crisis management plans based on stakeholders’ participation.
Afghanistan
A total of 2 papers addressed the mitigation and DRR measures in the form of planning and policies. Regarding disaster status, these articles considered both real disasters and simulated scenario-based disasters. The vulnerability reduction of buildings in Kabul was the main issue of the authors, who suggested implementing building codes and training engineers to prevent serious health damage resulting from disasters [16]. In addition, droughts, as a climatic disaster, were identified as an important triggering factor for food shortages in Afghanistan. The authors emphasized the necessity of developing an adaptation plan during drought periods [17].
Iran
A total of 10 articles examined the prevention and mitigation issues in the context of Iran. Of these papers, 60% addressed mitigation and DRR issues, while the remaining 40% focused on preparedness. Regarding disaster type, 30% of the included studies dealt with real disasters, and the remaining 70% considered simulated-scenario-based disasters. In addition, 50%, 0% and 50% of articles focused on planning, strategy, and policy, respectively.
The challenges and problems of disaster management were reviewed and reassessed, focusing on the experiences from the Bam earthquake. The authors declared that the important challenges of disaster management during the Bam earthquake were the inadequate coordination and communication between managers and relief organizations. It was emphasized that a unified comprehensive disaster management approach can help improve the DRR and prevention measures and plans [18]. Furthermore, improving disaster risk governance in the health system of Iran requires consideration of effective governance, a prevention culture, and the risk management process. All disaster risk governance documents should be investigated at the national level to develop DRR policies and strategies [19]. The resilience of healthcare centers was investigated, focusing on the structural, non-structural, and safety aspects. This article suggests planning for improving preparedness and flexibility of healthcare centers in Iran [20].
The challenges of early warning systems in the health sector were studied, and the authors identified various political, structural, and management challenges. Regarding management challenges, inadequate education, information, and communication management challenges, weak coordination, insufficient resources, and the lack of rules, protocols, and guidelines were identified. Considering that the establishment or development of a comprehensive early warning system in the health sector was the focus of the authors [21]. Schools are among the important sectors that need to implement health measures in disasters, focusing on DRR and prevention. Accordingly, improving awareness and knowledge in schools can play an important role in improving the safety of students. School officials, students, and parents need to be educated and informed about DRR and prevention measures in schools [22].
The article entitled “how much the Iranian government spent on disasters in the last 100 years- a critical policy analysis” reported that the Iranian government has spent money at the time of disaster strikes rather than on disaster risk management over the last 100 years. In other words, the response and recovery phases received more focus in budget allocation compared to mitigation and DRR in Iran [23]. The implementation of the Sendai Framework for DRR, which is considered one of the important international guidelines in the field of DRR and prevention, was studied in the context of Iran. Accordingly, continuous educational planning and cultural modification are needed to facilitate the long-term implementation of Sendai framework measures in Iran [24].
The challenges faced by the Iranian health system during the Kermanshah earthquake were identified as socio-cultural and psychological factors. The authors indicated that these factors could be considered major challenges for Iran’s health system during disasters and crises. Therefore, policymakers need to consider social, cultural, and psychological elements alongside healthcare factors when planning for DRR and prevention in Iran [25]. Affordable, resilient housing was highlighted as an important issue for improving DRR and prevention following the western earthquake in Iran. Accordingly, challenges, such as inappropriate structures, low-quality materials, and dangerous placements of structures, were identified concerning resilient housing for earthquakes. The modification of construction policies along with making new policies can enhance the structural and non-structural resilience, thereby improving DRR measures [26]. Community-based DRR measures focusing on droughts were considered based on gender distribution in literacy and employment sections in Iran. The authors declared that considering the vulnerabilities and capacities of both female and male populations living in drought-affected regions can improve their health status and resilience during droughts [27].
Discussion
The present review was conducted to compare DRR and prevention strategies and plans of Iran, Iraq, and Afghanistan reported in the literature. The findings showed that Iran benefits from more investigation and evidence-based studies on DRR and prevention compared to Iraq and Afghanistan. While Iraqi publications focused on conflicts and emergencies, the Afghanistan and Iran studies selected an all-hazard approach and natural hazards as the type of disasters. All included studies dealt with the aspects of DRR and prevention in the health systems directly and indirectly. Policies, strategies, and plans related to DRR and pre-disaster measures were suggested more by Iranian investigators compared to researchers from Iraq and Afghanistan.
Our review revealed that the disaster-prone countries, especially the ones in the Middle East, need to establish effective plans and policies focused on DRR and prevention. Similarly, a review of post-disaster health lessons learned in 12 Asian countries highlighted the importance of DRR and preparedness measures before disasters occur. The authors emphasized that investing in community and national health service preparedness should be recognized as a priority for hazard-prone countries. The areas studied for preparedness included health donations and medical volunteers, as well as field hospital preparedness, with a focus on providing material and logistical support post-disasters [28].
In the current review, the structural, non-structural, and functional safety of the health systems and communities, focusing on the community involvement in conducting DRR and prevention plans, were mentioned by all authors from three countries. In accordance with our findings, a review of major earthquakes between 2000 and 2010 suggested that the structural and social factors are influential. DRR and mitigation measures, especially resilient construction, are important for reducing mortality in developing countries. Hospitals, fire departments, and facilities, such as water, telephone, and police stations, also need to be prepared for future earthquakes [29].
Our findings declared that all 3 countries need to consider DRR plans and strategies in the disaster management of their health systems. Similarly, a review of strategies for educating the DRR reported that although most countries tried to begin the DRR education plans and activities, such actions are inadequate, and they need to fill the gap between the current and optimal situations. Establishing the learning and teaching strategies can promote the effectiveness of DRR measures at the community and national levels [30]. DRR education and training are important for the hazard-prone countries, such as Iran, Iraq, and Afghanistan, that suffer from high levels of vulnerabilities.
Climate-related disasters, such as droughts, were considered in the articles included in our review. Accordingly, a review study explained the connection between DRR, climate change adaptation, and sustainable development over the past 30 years. The authors suggested that climate change adaptation is not a subset of DRR, as they have differences and similarities in their scope. However, integrating DRR and climate change adaptation, focusing on governance mechanisms, can decrease the risks of climatic disasters and improve future resilience in countries [31].
Similarly, a review of DRR and climate change adaptations focusing on the governance gap in Malaysia reported that this country needs to integrate climate change into DRR strategies and policies. The authors suggested assessing current strategies and identifying areas for DRR governance and policy-making in Malaysia [32]. In accordance with our findings, a rapid review of the current DRR efforts in Saudi Arabia for extreme heat, droughts, floods, and sandstorms showed that the country has made progress in building codes, infrastructure, early warning systems, and public awareness. The authors implied that emphasizing practical measures for disaster risk management, along with increased efforts to improve important aspects of DRR (e.g. safer buildings, public awareness, and policy-making), can make the country more resilient to disasters [33].
In addition, health facilities need structural and non-structural building resistance, as well as continuous development for broader resilience as a national strategy or set of rules. This can be strengthened by establishing standard instructions and methods in disaster prevention exercises within health systems, especially in developing countries [34]. Consequently, Iran’s health system has developed a safe hospital framework based on World Health Organization (WHO) guidelines, and accordingly, the annual assessment of hospitals and conducting disaster exercises twice a year have been implemented by all hospitals to meet accreditation criteria. It seems that Iraq and Afghanistan can benefit from the lessons learned and experiences of Iran’s health system to establish their DRR structures and measures within their health facilities.
Conclusion
This review focused on DRR policies, plans, and strategies that were reported by researchers from Iraq, Iran, and Afghanistan. DRR measures need to be integrated into all phases of disaster management plans developed for health systems in EMRO countries facing natural and technological hazards and high levels of vulnerabilities. According to our findings, the following suggestions can be considered by policymakers, managers, and researchers in DRR management and prevention.
Establishing a network or platform with the membership of health experts, researchers, and managers who are active in any field of DRR can be effective for sharing all research papers, guidelines, policy briefs, plans, and protocols related to DRR measures conducted in Iran, Iraq, and Afghanistan.
Joint research projects can be designed and conducted by health experts and researchers in DRR management and prevention who have published a considerable number of research and policy papers in Iran, Afghanistan, and Iraq to establish evidence-based policies at the regional levels.
Designing the long-term and short-term educational programs on DRR management and prevention in the health system can be helpful. The target group for such programs is experts, managers, and policymakers who play effective roles in implementing and incorporating DRR measures/plans in their health systems at the local and national levels.
The safety and resilience of health facilities can be considered by establishing rules, policies, and plans that require health officials to adhere to DRR and safety criteria or standards. Accordingly, annual assessments of health facilities can motivate officials to implement DRR and prevention measures within their institutions.
Community-based DRR management and prevention are suggested for involving people in all DRR plans and measures in all hazard-prone regions. Thus, considering the community as one of the main parts of DRR actions can improve community resilience and prevent future disasters.
Moreover, further research is needed to analyze and compare the DRR management and prevention documents published on specific websites or databases of all EMRO countries using their native languages.
Strengths and limitations
This comparative review highlighted the different aspects of DRR plans, strategies, and actions in Iran, Iraq, and Afghanistan as the hazard-prone countries in EMRO. Our findings provide a collection of what these countries have conducted and reported regarding DRR and prevention plans, policies, and measures. This can provide the opportunity to compare the current conditions of these countries, identify gaps, and optimize DRR plans and policies based on various contextual experiences.
There were several limitations during the review process. The PubMed database was used for searching the references since the research topic and keywords were widely applied by various papers published in many journals, making it nearly impossible to manage the large number of references. Since the health system was considered one of our inclusion criteria/keywords, we selected the PubMed database, which indexes health-related journals. Furthermore, our review included published articles in the fields of DRR and prevention and health; however, there is a possibility that some DRR measures or plans have been missed if they were not reported in the relevant databases or published in non-English languages.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by Ethics Committee of the School of Public Health and Safety, Shahid Beheshti University of Medical Sciences, Tehran, Iran (Code: IR.SBMU.PHNS.REC.1401.036).
Funding
This study was funded by the Air Quality and Climate Change Research Center at the Research Institute for Health Sciences and Environment in Shahid Beheshti University of Medical Sciences, Tehran, Iran (Grant No.: 43002269).
Authors' contributions
Conceptualization, data analysis, and project supervision: Sanaz Sohrabizadeh; Data collection: Amirhosein Bahramzadeh; Writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to appreciate all people who facilitate their research process.
References
- Ardalan A, Sohrabizadeh S. Assessing households preparedness for earthquakes: An exploratory study in the development of a valid and reliable Persian-version Tool. PLOS Currents Disasters. 2016; 8:ecurrents-dis. [DOI:10.1371/currents.dis.ccc8697279713e66887b928b839d0920]
- Ngaruiya C, Bernstein R, Leff R, Wallace L, Agrawal P, Selvam A, et al. Systematic review on chronic non-communicable disease in disaster settings. BMC Public Health. 2022; 22(1):1234. [DOI:10.1186/s12889-022-13399-z] [PMID]
- El Morjani Zel A, Ebener S, Boos J, Abdel Ghaffar E, Musani A. Modelling the spatial distribution of five natural hazards in the context of the WHO/EMRO atlas of disaster risk as a step towards the reduction of the health impact related to disasters. International Journal of Health Geographics. 2007; 6:8. [DOI:10.1186/1476-072X-6-8] [PMID]
- Mazhin SA, Farrokhi M, Noroozi M, Roudini J, Hosseini SA, Motlagh ME, et al. Criteria and components of the emergency and disaster database in Iran: A content analysis study. Journal of Education and Health Promotion. 2021; 10:407. [DOI:10.4103/jehp.jehp_93_21] [PMID]
- Aminizadeh M, Farrokhi M, Ebadi A, Masoumi G, Kolivand P, Khankeh H. Hospital preparedness challenges in biological disasters: A qualitative study. Disaster Medicine and Public Health Preparedness. 2022; 16(3):956-60. [DOI:10.1017/dmp.2020.434] [PMID]
- Aminizadeh M, Farrokhi M, Ebadi A, Masoumi GR, Kolivand P, Khankeh HR. Hospital management preparedness tools in biological events: A scoping review. Journal of Education and Health Promotion. 2019; 8:234. [DOI:10.4103/jehp.jehp_473_19] [PMID]
- European Commission. DRMKC- INFORM RISK. Brussels: European Commission; 2023. [Link]
- Mousavi G, Khorasani-Zavareh D, Ardalan A, Khankeh H, Ostadtaghizadeh A, Kamali M, et al. Continuous post-disaster physical rehabilitation: A qualitative study on barriers and opportunities in Iran. Journal of Injury & Violence Research. 2019;11(1):35-44. [DOI:10.5249/jivr.v11i1.1036] [PMID]
- Ardalan A, Masoomi G, Goya M, Ghaffari M, Miadfar J, Sarvar M, et al. Disaster health management: Iran’s progress and challenges. Iranian Journal of Public Health. 2009; 38(Supple 1):93-7. [Link]
- Al-Shamsi MTM. Disaster risk reduction in Iraq. Jamba (Potchefstroom, South Africa). 2019; 11(1):656. [DOI:10.4102/jamba.v11i1.656] [PMID]
- Tuhkanen S, Maijala H, Kernohan WG. A disaster preparedness and response project in Afghanistan: Participants' perceptions. Journal of Advanced Nursing. 2008; 64(3):287-97. [DOI:10.1111/j.1365-2648.2008.04708.x] [PMID]
- Aitsi-Selmi A, Murray V. The Sendai framework: Disaster risk reduction through a health lens. Bulletin of the World Health Organization. 2015; 93(6):362. [DOI:10.2471/BLT.15.157362] [PMID]
- Suppasri A, Muhari A, Syamsidik, Yunus R, Pakoksung K, Imamura F, et al. Vulnerability characteristics of tsunamis in Indonesia: Analysis of the global centre for disaster statistics database. Journal of Disaster Research. 2018; 13(6):1039-48. [DOI:10.20965/jdr.2018.p1039]
- Kaneda Y, Ozaki A, Hashemy T, Shrestha R, Madadi S. The importance of the Taliban and the international community collaboration in building support systems for experts working in earthquake-affected areas in Afghanistan-perspectives from a triple disaster experience in Fukushima. Disaster Medicine and Public Health Preparedness. 2023; 17:e265. [DOI:10.1017/dmp.2022.260] [PMID]
- Ibrahim S, Al-Dahir S, Al Mulla T, Lami F, Hossain SMM, Baqui A, et al. Resilience of health systems in conflict affected governorates of Iraq, 2014-2018. Conflict and Health. 2021; 15(1):76. [DOI:10.1186/s13031-021-00412-2] [PMID]
- Mohammadi M, Fujimi T. Impact of retrofitting work on vulnerability reduction of local buildings in Kabul, Afghanistan. Jamba. 2021; 13(1):1062. [DOI:10.4102/jamba.v13i1.1062] [PMID]
- Chen Y, Penton D, Karim F, Aryal S, Wahid S, Taylor P, et al. Characterisation of meteorological drought at sub-catchment scale in Afghanistan using station-observed climate data. PLoS One. 2023; 18(2):e0280522. [DOI:10.1371/journal.pone.0280522] [PMID]
- Kalantar Motamedi MH, Saghafinia M, Bararani AH, Panahi F. A reassessment and review of the Bam earthquake five years onward: What was done wrong? Prehospital and Disaster Medicine. 2009; 24(5):453-60. [DOI:10.1017/S1049023X00007317] [PMID]
- Safari M, Seyedin H, Jahangiri K. Disaster risk governance in Iran: Document analysis. Journal of Education and Health Promotion. 2019; 8(1):142. [DOI:10.4103/jehp.jehp_30_19] [PMID]
- Yari A, Zarezadeh Y, Fatemi F, Ardalan A, Vahedi S, Yousefi-Khoshsabeghe H, et al. Disaster safety assessment of primary healthcare facilities: A cross-sectional study in Kurdistan province of Iran. BMC Emergency Medicine. 2021; 21(1):23. [DOI:10.1186/s12873-021-00417-3] [PMID]
- Hosseini SH, Khankeh HR, Farrokhi M, Hosseini MA, Koolivand P, Raeiszadeh M. Early warning system-related challenges in health sector: A qualitative content analysis study in Iran. Journal of Education and Health Promotion. 2020; 9:38. [DOI:10.4103/jehp.jehp_510_19] [PMID]
- Hosseinighousheh S, Arefi MF, Pouya AB, Poursadeqiyan M. Health in disasters in Iranian schools: A systematic review. Journal of Education and Health Promotion. 2021; 10:365. [DOI:10.4103/jehp.jehp_1263_20] [PMID]
- Seddighi H, Seddighi S. How much the Iranian government spent on disasters in the last 100 years? A critical policy analysis. Cost Effectiveness and Resource Allocation. 2020; 18:46. [DOI:10.1186/s12962-020-00242-8] [PMID]
- Yousefi Khoshsabegheh H, Takian A, Ardalan A, Ostadtaghizadeh A, Saeedi B. Implementation of the Sendai framework in the health system in Iran: Identification of facilitators and obstacles. Journal of Environmental Health Science & Engineering. 2021; 19(2):1597-606. [DOI:10.1007/s40201-021-00715-9] [PMID]
- Mohammadpour M, Sadeghkhani O, Bastani P, Ravangard R, Rezaee R. Iranian's healthcare system challenges during natural disasters: the qualitative case study of Kermanshah earthquake. BMC Emergency Medicine. 2020; 20(1):75. [DOI:10.1186/s12873-020-00359-2] [PMID]
- Heidari M, Eskandary N, Miresmaeeli SS. The challenge of affordable housing in disasters: Western Iran earthquake in 2017. Disaster Medicine and Public Health Preparedness. 2020; 14(2):289-91. [DOI:10.1017/dmp.2019.5] [PMID]
- Sohrabizadeh S, Bahramzadeh A, Hanafi-Bojd AA. Climate change and gender: Mapping drought and gender gap in literacy and employment sections in Iran between 2011 and 2016. Medical Journal of The Islamic Republic of Iran. 2022; 36:146. [DOI:10.47176/mjiri.36.146] [PMID]
- de Ville de Goyet C. Health lessons learned from the recent earthquakes and Tsunami in Asia. Prehospital and Disaster Medicine. 2007; 22(1):15-21. [DOI:10.1017/S1049023X00004283] [PMID]
- Kalantar Motamedi MH, Sagafinia M, Ebrahimi A, Shams E, Kalantar Motamedi M. Major earthquakes of the past decade (2000-2010): A comparative review of various aspects of management. Trauma Monthly. 2012; 17(1):219-29. [DOI:10.5812/traumamon.4519] [PMID]
- Aghaei N, Seyedin H, Sanaeinasab H. Strategies for disaster risk reduction education: A systematic review. Journal of Education and Health Promotion. 2018; 7:98. [DOI:10.4103/jehp.jehp_31_18] [PMID]
- Wen J, Wan C, Ye Q, Yan J, Li W. Disaster risk reduction, climate change adaptation and their linkages with sustainable development over the past 30 years: A review. International Journal of Disaster Risk Scienc. 2023; 14(1):1-13. [DOI:10.1007/s13753-023-00472-3]
- Madnor MS, Harun AN, Ros FC. A review on disaster risk reduction and climate change adaptation: Gaps of governance in Malaysia. Journal of Management Info. 2023; 10(4):261-81. [Link]
- Al-Wathinani AM, Barten DG, Borowska-Stefańska M, Gołda P, AlDulijan NA, Alhallaf MA, et al. Driving Sustainable Disaster Risk Reduction: A rapid review of the policies and strategies in Saudi Arabia. Sustainability. 2023; 15(14):10976. [DOI:10.3390/su151410976]
- Luke J, Franklin R, Aitken P, Dyson J. Safer hospital infrastructure assessments for socio-natural disaster - A scoping review. Prehospital and Disaster Medicine. 2021; 36(5):627-35.[DOI:10.1017/S1049023X21000650] [PMID]
Type of article: Review |
Subject:
Emergency
Received: 2024/09/18 | Accepted: 2025/03/3 | Published: 2025/10/1
Received: 2024/09/18 | Accepted: 2025/03/3 | Published: 2025/10/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
