

Volume 11, Issue 2 (Winter 2026)
Health in Emergencies and Disasters Quarterly 2026, 11(2): 129-138 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mehri S, Geybati F, Habibi Soola A, Asadi H. Driving Behavior of Pre-hospital Emergency Personnel in Ardabil Province. Health in Emergencies and Disasters Quarterly 2026; 11 (2) :129-138
URL: http://hdq.uswr.ac.ir/article-1-711-en.html
URL: http://hdq.uswr.ac.ir/article-1-711-en.html



1- Department of Emergency Nursing, School of Nursing and Midwifery, Ardabil University of Medical Sciences, Ardabil, Iran.
2- Department of Emergency Nursing, School of Nursing and Midwifery, Ardabil University of Medical Sciences, Ardabil, Iran. ,asadihosein115@gmail.com
2- Department of Emergency Nursing, School of Nursing and Midwifery, Ardabil University of Medical Sciences, Ardabil, Iran. ,
Full-Text [PDF 495 kb]
(555 Downloads)
| Abstract (HTML) (1924 Views)
Full-Text: (300 Views)
Introduction
Emergency medical services (EMS) play a pivotal role in providing prompt medical assistance and transporting patients during emergencies, often making the difference between life and death [1]. Central to the delivery of EMS is the emergency ambulance service, which ensures that patients receive timely and effective care [2]. In Iran, the responsibility of driving ambulances typically falls on emergency medical technicians (EMTs) and paramedics, who must balance their roles as both drivers and medical caregivers [3]. This dual responsibility places immense pressure on these personnel, as they are tasked with ensuring the safety of patients, fellow ambulance crew members, and other road users, including drivers and pedestrians [4, 5]. Even the slightest error in judgment or driving behavior can have catastrophic consequences, endangering the lives of everyone inside and outside the ambulance [6].
Driving an ambulance is inherently risky, with numerous hazards identified in the literature [7]. One of the most significant risks is the potential for accidents caused by high-speed and aggressive driving, which are often necessitated by the urgency of emergency situations [8]. Alarmingly, the fatality rate for emergency medical personnel involved in motor vehicle accidents is four times higher than that of other occupational groups [9]. This heightened risk is compounded by the stressful nature of their work, which requires them to provide life-saving medical care to critically ill or injured patients while simultaneously navigating through traffic under time constraints [10, 11]. The psychological and physical stress experienced by ambulance drivers can impair their decision-making abilities and reaction times, further increasing the likelihood of accidents [12, 13].
Despite the critical importance of safe and efficient ambulance driving, there has been limited research on the driving behavior of emergency medical personnel, particularly in high-stress environments. Moreover, little attention has been paid to how driving behavior impacts the medical condition of patients during transport and the overall quality of care provided [14]. While pre-hospital and ambulance care research has made significant strides in areas, such as emergency medicine, traumatology, clinical assessments, and patient referrals, the specific challenges and risks associated with ambulance driving remain underexplored [15]. This gap in the literature highlights the need for a deeper understanding of the factors influencing the driving behavior of EMS personnel and their implications for patient safety and care quality.
This study aimed to assess the driving behavior of ambulance drivers, who are also emergency medical personnel, in Ardabil Province, Iran. By examining the factors that contribute to risky driving practices, such as stress, fatigue, and the demands of providing medical care, this research sought to identify strategies for improving safety and efficiency in emergency medical transport. The findings of this study will contribute to the growing body of knowledge on EMS safety and provide evidence-based recommendations for reducing accidents and enhancing the quality of pre-hospital care.
Materials and Methods
Between June 2023 and August 2023, a cross-sectional descriptive study was conducted in Ardabil Province. Initially, the total number of pre-hospital emergency personnel was 442. Based on a total population sampling method with eligibility criteria, 42 individuals were excluded due to having less than six months of experience in pre-hospital emergency services. Consequently, the questionnaires were distributed to 400 eligible personnel. Inclusion criteria included at least six months of work experience, willingness to participate, and no concurrent involvement in similar research. Incomplete questionnaire responses were considered the exclusion criterion. Out of the 400 distributed questionnaires, 380 were fully completed and included in the final analysis.
Data collection was carried out using two tools: A demographic questionnaire and the Manchester driving behavior questionnaire (MDBQ). The demographic questionnaire comprised ten items, including age, marital status, employment status, work experience (in years), education level, field of study, workplace, type of work shift, ambulance driving experience, and history of ambulance-related accidents. The MDBQ, developed by Parker and Reason at the University of Manchester, was used to assess driving behavior [14]. This scale is based on the premise that errors and violations in driving have distinct psychological origins and require different corrective approaches, making it essential to differentiate between them in research. The MDBQ consists of 50 items rated on a Likert scale ranging from 0 to 5, capturing two dimensions: The type of driving behavior and the level of risk posed to others. Abnormal driving behaviors are categorized into four types: lapse errors, slips, deliberate violations, and unintentional violations. These behaviors are further classified based on the level of risk they pose: Behaviors that pose no risk to others and merely provide a sense of comfort (low-risk probability).
Behaviors that are likely to endanger others (moderate-risk probability).
Behaviors that certainly endanger others (high-risk probability).
Lapse errors, reflecting memory and attention failures, included items, such as “I forget where I left my car in a car park” and “I start to drive away from the traffic lights without realizing that they are still red.”
Slips, representing attention or observation failures, included questions, like “I misread the signs and take the wrong turn” and “I fail to notice pedestrians crossing when turning into a side street.”
Deliberate violations, indicating intentional breaches of traffic rules, were assessed with items, such as “I disregard the speed limits on a motorway” and “I drive especially close to the car in front to signal that I want them to go faster.”
Unintentional violations, referring to rule-breaking due to misjudgment or inattention, included items, like “I exceed the speed limit without realizing it” and “I misjudge the speed of an oncoming vehicle when overtaking.”
The MDBQ has demonstrated strong psychometric properties. Parker and Reason [14] reported reliability coefficients of 0.81 for errors and 0.75 for violations in a test-retest study with an 80-driver sample over a seven-week interval. In the current study, the Cronbach’s α coefficient for the MDBQ was calculated at 0.89, indicating high internal consistency.
Data collection was conducted in person by the researcher, who visited both urban and road emergency bases to engage directly with personnel who met the inclusion criteria. The researcher clearly explained the study’s objectives, significance, and relevance to participants, emphasizing the confidentiality and anonymity of their responses. Written informed consent was obtained from all participants, and they were assured of their right to withdraw from the study at any stage without facing any consequences.
To minimize potential stress and ensure accurate responses, questionnaires were completed outside participants’ work shifts, allowing them adequate time and focus. The researcher remained available on-site to clarify any questions or ambiguities regarding the questionnaire. Once completed, the questionnaires were collected immediately and directly by the researcher to maintain data integrity and completeness.
To minimize social desirability bias, participants were assured of the anonymity and confidentiality of their responses, with no identifying information collected. They were informed that data would be analyzed collectively and that there were no right or wrong answers. The voluntary nature of participation and the right to withdraw at any time were also emphasized to encourage honest and unbiased responses.
Data analysis was performed using SPSS software, version 22. Descriptive statistics, including frequency distribution, Mean±SD, were used to summarize and categorize the data. Inferential statistical tests, such as the t-test, ANOVA, and multiple regression analysis, were employed to examine the relationships between demographic variables and MDBQ scores. The Kolmogorov-Smirnov test was used to assess the normal distribution of quantitative variables. A 95% confidence level and a significance level of 0.05 were applied in all statistical tests.
Results
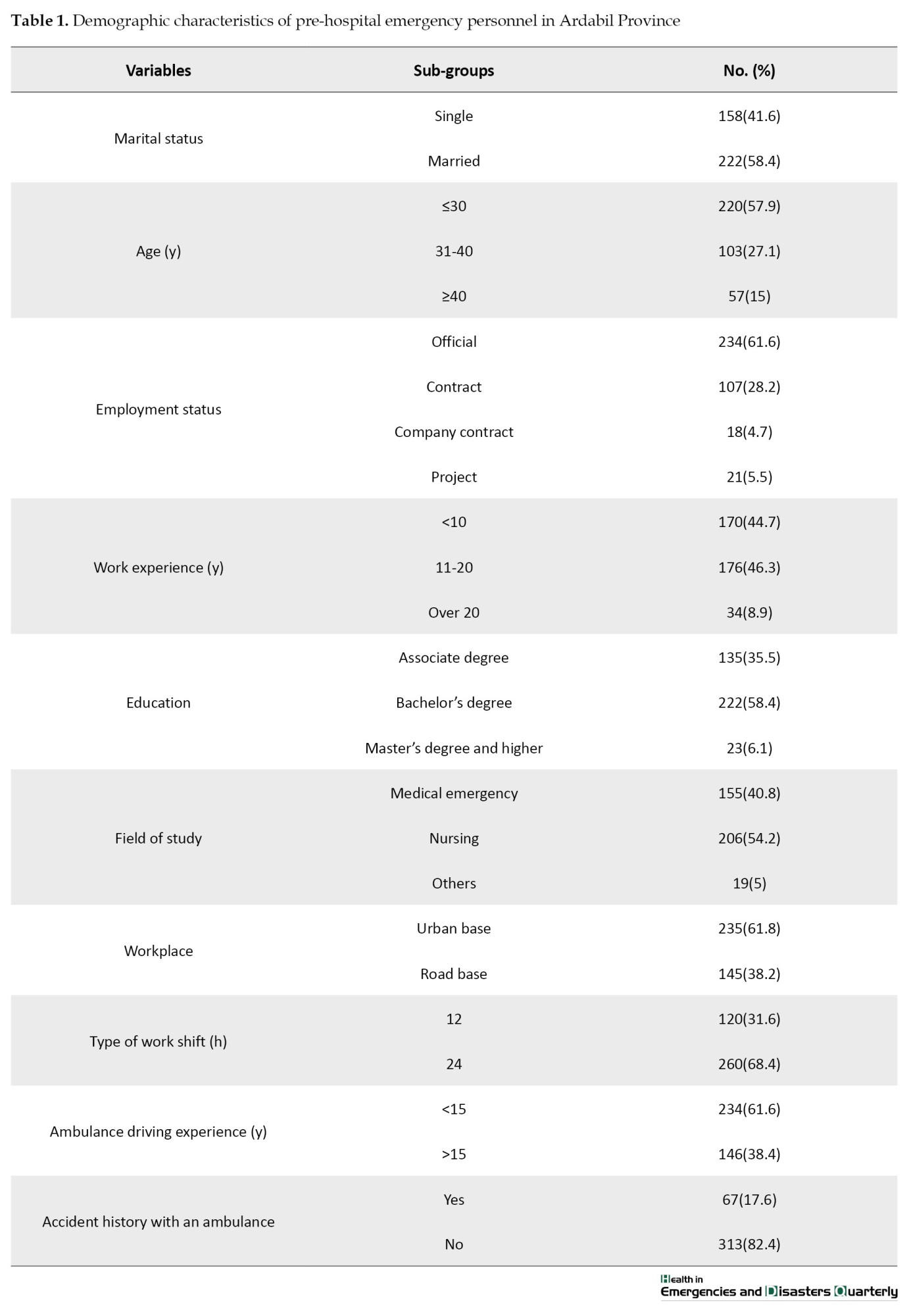
Of 380 personnel participating in this study, 100% were male with a mean age of 32.71±7.81 years, a maximum age of 51 years, and a minimum age of 23 years. Most study participants, 222(58.4%), were married, 234(61.6%) were officially employed, and 222 (58.4%) had a bachelor’s degree. The highest clinical work experience of personnel was 11-20 years (46.3%), with 260 individuals (68.4%) working in 24-hour shifts, 235(61.8%) personnel based in urban areas, and 313(82.4%) having no history of traffic accidents (Table 1).
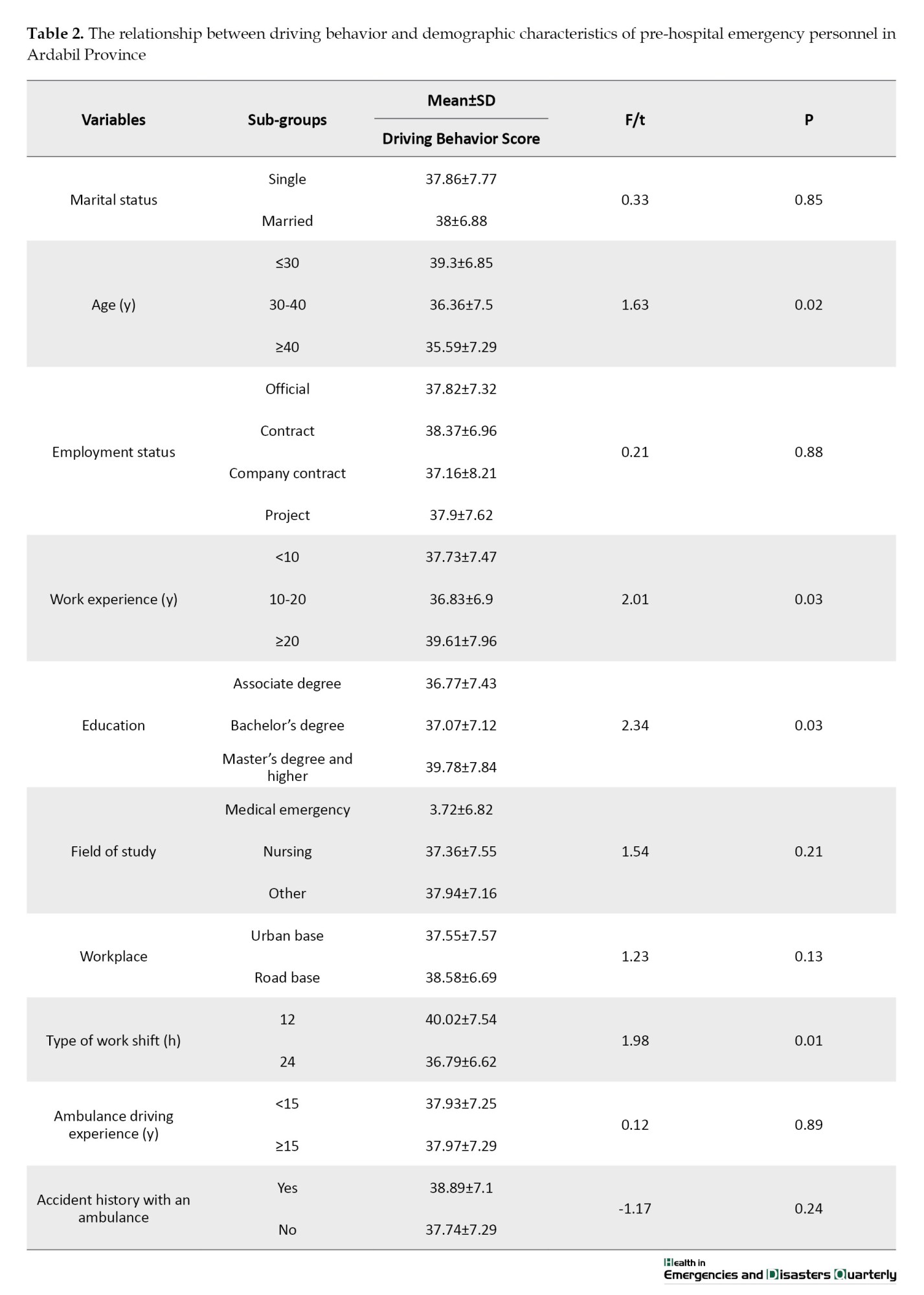
There was a statistically significant relationship between age (P=0.02), work experience (P=0.03), education (P=0.03), and type of work shift (0.01) and the driving behavior of personnel (Table 2).
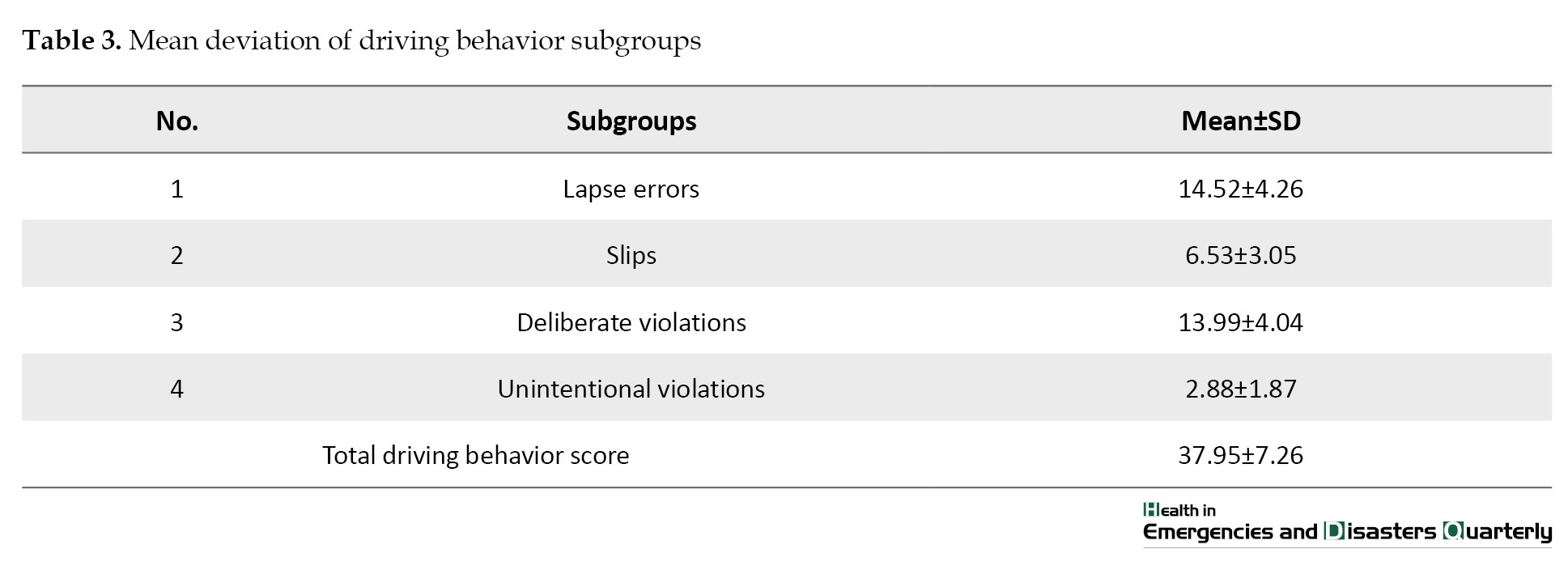
The total mean score of personnel driving behavior was 37.95±7.26. Also, the mean scores of driving slips, mistakes, intentional violations, and unintentional violations were 14.52±4.26, 6.53±3.05, 13.99±4.04, and 2.88±1.87, respectively (Table 3).
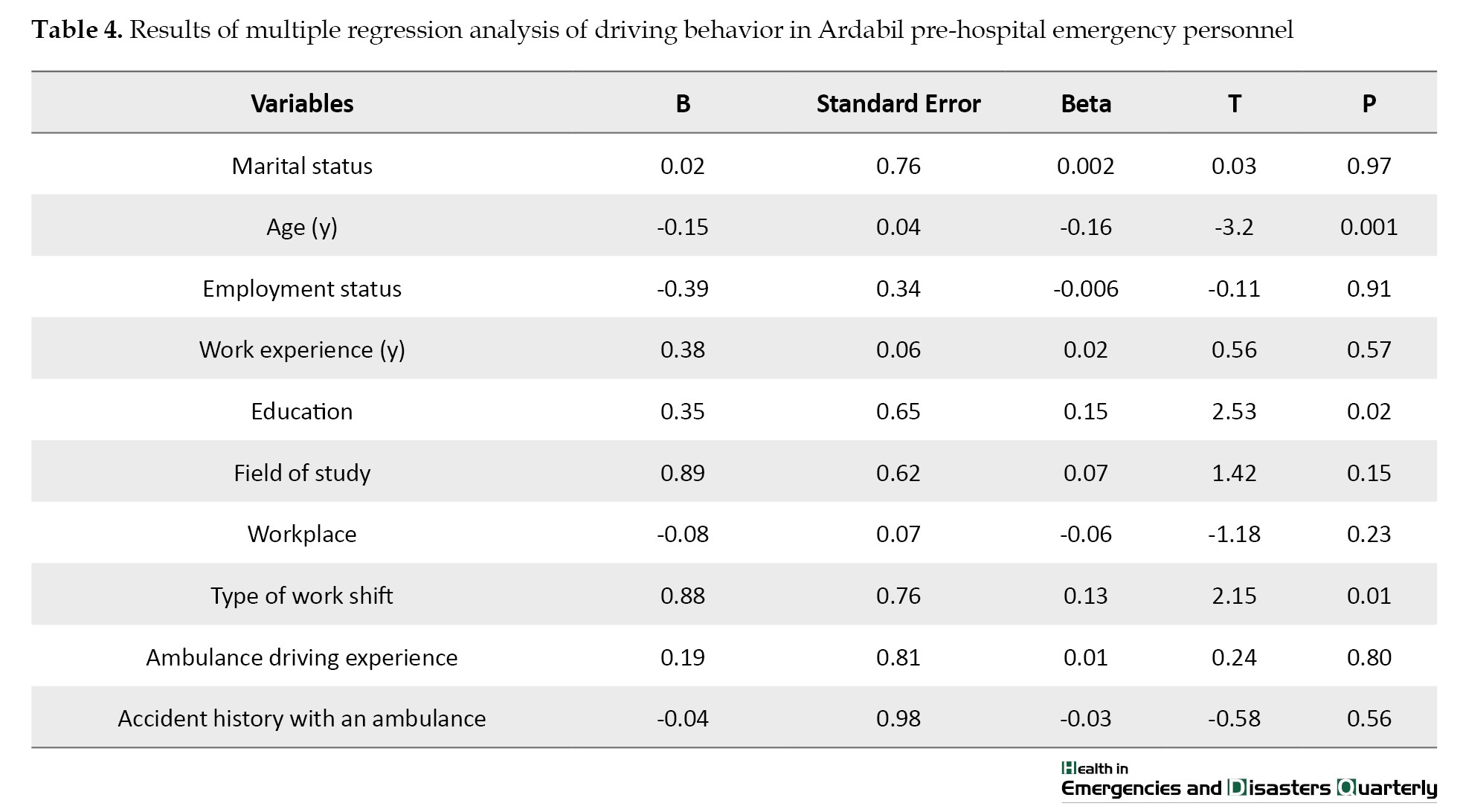
The results of multiple linear regression analysis showed age, education, and type of work shift were predictors of driving behavior. According to the obtained determination coefficients, 58% of the driving behavior changes were due to the variables mentioned in the model. The suggested regression model had an acceptable fit (F=56.56, P˂0.001) (Table 4).
Discussion
This study aimed to evaluate the driving behavior of emergency medical personnel in Ardabil Province. The present study is significant as it is one of the first to assess the driving behavior of emergency medical personnel operating ambulances. The driving behavior of pre-hospital emergency personnel can have a profound impact on both the clinical condition of the patient and the staff’s ability to provide effective care [1].
The results of this study revealed a significant relationship between age, work experience, education level, and type of work shift and the driving behavior of emergency medical personnel. These findings are consistent with previous research, which has highlighted the impact of occupational and demographic factors on driving behavior. For instance, Watanabe et al. found that ambulance personnel working 24-hour shifts experienced poor sleep quality and were 2.3 times more likely to suffer injuries compared to those working shorter shifts. Additionally, they reported higher levels of fatigue among 24-hour shift workers [2]. In contrast, Yenal et al. observed that personnel working 24-hour shifts had fewer accidents, suggesting that extended shifts may not always negatively impact driving safety [8]. This discrepancy could be attributed to differences in study design, sample characteristics, or even regional factors. Yenal et al.’s study may have involved a sample with different baseline driving behavior or environmental factors that moderated the effect of shift length on driving safety. Furthermore, cultural or organizational differences in how shifts are managed could also explain why longer shifts did not result in the same level of negative impact on driving behavior. Similarly, Eksi et al. reported no significant differences in gender, age, experience, or professional title among ambulance personnel involved in traffic accidents, which contrasts with the findings of the present study [11]. Moreover, Prohn and Herbig [10] demonstrated the value of simulator-based training in improving ambulance drivers’ awareness and reducing risky behavior, suggesting that education and ongoing skill development may be more decisive than experience alone. The lack of significant findings in Eksi et al.’s study may suggest potential limitations in sample size or the operationalization of key variables, such as experience or shift type. Moreover, their study might not have accounted for other important variables, such as the psychological impact of the work environment or the training provided to emergency personnel, which could mediate the relationship between demographic factors and driving behavior.
These contrasting findings highlight important gaps in the literature and emphasize the need for future research to critically examine the factors that contribute to these differences. A deeper exploration of the role of work environment, psychological stress, and other occupational factors could provide a more comprehensive understanding of how shift work impacts the driving behavior of emergency medical personnel.
Furthermore, Vatani et al. found that the mean age of drivers with a history of accidents was significantly higher than those without such a history, indicating that age can influence driving behavior [15]. This aligns partially with our findings, as our data also suggest that drivers with more years of experience tended to report better adherence to safe driving practices. However, unlike Vatani et al., we did not observe a direct correlation between age and accident history. This discrepancy may stem from differences in the studied populations; while their research focused on a broader range of public service drivers, our study was limited to emergency medical personnel in Ardabil Province, who often undergo more specialized training and face different stressors. The interplay between experience and factors, such as fatigue or stress appears to be crucial [4]. Although increased exposure to various driving situations can enhance judgment and reaction time, these benefits may be diminished under conditions of chronic fatigue, particularly in high-pressure roles, like emergency response [5]. For instance, a high number of missions per shift may lead to cognitive overload and reduced situational awareness, increasing the likelihood of accidents [9].
In the present study, 67 cases (17.6%) reported being involved in an ambulance accident. This figure underscores a significant occupational hazard within the EMS system in Ardabil Province. Between 2012 and 2016, 46 cases of ambulance accidents were reported in Iran, with a peak in 2015 (35%). Of these, 52% involved EMS ambulances, and notably, 39% of the 109 injuries and 25% of the 53 fatalities were among ambulance drivers and technicians [16]. These statistics point to a concerning vulnerability among frontline EMS staff. When compared with international data, the picture becomes more complex. Türkdemir and Aysun documented 614 ambulance accidents in Turkey between 1960 and 2002, of which only 3 resulted in fatalities and 367 in injuries. In contrast, New York State records around 400 ambulance accidents annually, with approximately two injuries per day, and an estimated 75% of these accidents being preventable [17]. The considerably higher rate of preventable accidents in New York, despite presumably stricter regulations and advanced infrastructure, suggests that systemic and behavioral factors, such as adherence to safety protocols, road conditions, or driver training play a critical role. The differences across these contexts may be attributed to several factors. In Iran, particularly in provinces, like Ardabil, EMS systems often face constraints, such as limited resources, outdated vehicles, variable driver training standards, and inconsistent traffic law enforcement. Cultural differences in road-sharing behavior and public awareness may also influence accident rates. Practically, these findings highlight an urgent need for targeted interventions. Establishing standardized training protocols with a strong emphasis on defensive driving, improving public awareness about ambulance right-of-way, and implementing digital monitoring systems (such as telematics to monitor driving behavior) could help reduce accident rates. Furthermore, periodic risk assessments and the integration of traffic data into shift planning may help mitigate high-risk periods or routes, especially during peak hours or in congested urban centers. These strategies could significantly enhance safety for EMS personnel and the public they serve in Ardabil Province.
Multiple contributing factors have been identified in prior research. For example, Pappinen and Nordquist [5]highlighted how urgency level and seasonal conditions affect driving speed, which may increase accident risk in poor weather. Araújo et al. [9] noted additional psychological pressure faced by ambulance drivers during the COVID-19 pandemic, suggesting that both physical and mental load are essential considerations.
The findings of this study can significantly contribute to improving training programs, shift management, and safety protocols for emergency medical personnel in Ardabil Province. Given the significant relationship between age, work experience, education, and type of work shift and driving behavior, training programs should focus on enhancing safe driving awareness and skills, particularly for less experienced and younger personnel. Additionally, to reduce fatigue and improve performance, shift management should be adjusted to minimize long shifts (such as 24-hour shifts) and ensure adequate rest time for personnel. Moreover, implementing comprehensive safety protocols and conducting regular assessments of driving behavior can foster a safety culture, reduce accidents, and ultimately improve service quality and patient safety.
The present study has several limitations that should be considered. The data were collected using a self-report questionnaire, which is subject to response biases, including underreporting or overreporting of certain behaviors. This could affect the accuracy of the reported driving behaviors and may not fully reflect actual practices.
Also, the study was conducted exclusively among emergency medical personnel in Ardabil Province, which limits the generalizability of the findings. The unique characteristics of this region, such as workforce structure, training standards, and cultural factors, may not be representative of other regions or populations. Therefore, caution is needed when applying the findings to other geographical locations or contexts.
Another limitation pertains to gender bias in the study sample. The EMS in Ardabil Province exclusively employ male personnel in driving roles, and as such, the study’s findings are based on an all-male sample. The absence of female drivers in this context means that the study may not fully capture potential gender differences in driving behavior or safety practices. Future studies that include both male and female emergency personnel would provide a more comprehensive understanding of how gender may influence driving behavior in this context.
Lastly, the cross-sectional design of the study limits the ability to establish causal relationships between the variables. As a snapshot of the situation at a specific point in time, it does not allow for the examination of changes over time or the exploration of cause-and-effect dynamics between demographic factors and driving behavior.
Conclusion
Ambulance driving plays a critical role in ensuring patient health, well-being, and safety. Given its importance, cultivating a strong and safety-oriented driving culture should be recognized as a fundamental component of care delivery within EMS. The findings of this study, highlighting the notable incidence of ambulance accidents and the contributing factors, such as fatigue, high mission loads, and stress, underscore the urgent need for structured interventions. To address these challenges, specific and practical actions should be taken. First, EMS institutions in Ardabil Province can implement targeted training programs that not only enhance driving skills but also integrate modules on fatigue management, stress reduction, and situational awareness. Second, shift scheduling should be optimized to limit the number of missions per shift and ensure adequate rest periods, especially during high-demand hours. Third, establishing a standardized incident reporting and feedback system can help identify recurring risk patterns and inform continuous improvement efforts.
By promoting these strategies, EMS authorities can create a safer working environment for drivers and technicians, reduce the frequency of ambulance-related accidents, and ultimately improve the quality and safety of emergency medical response in the region.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Ardabil University of Medical Sciences, Ardabil, Iran (Code: IR.ARUMS.REC.1402.095). All methods were conducted in accordance with the Declaration of Helsinki. Participants’ privacy and confidentiality were maintained, and informed consent was obtained prior to their involvement in the study.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank everyone who contributed to this research.
References
Emergency medical services (EMS) play a pivotal role in providing prompt medical assistance and transporting patients during emergencies, often making the difference between life and death [1]. Central to the delivery of EMS is the emergency ambulance service, which ensures that patients receive timely and effective care [2]. In Iran, the responsibility of driving ambulances typically falls on emergency medical technicians (EMTs) and paramedics, who must balance their roles as both drivers and medical caregivers [3]. This dual responsibility places immense pressure on these personnel, as they are tasked with ensuring the safety of patients, fellow ambulance crew members, and other road users, including drivers and pedestrians [4, 5]. Even the slightest error in judgment or driving behavior can have catastrophic consequences, endangering the lives of everyone inside and outside the ambulance [6].
Driving an ambulance is inherently risky, with numerous hazards identified in the literature [7]. One of the most significant risks is the potential for accidents caused by high-speed and aggressive driving, which are often necessitated by the urgency of emergency situations [8]. Alarmingly, the fatality rate for emergency medical personnel involved in motor vehicle accidents is four times higher than that of other occupational groups [9]. This heightened risk is compounded by the stressful nature of their work, which requires them to provide life-saving medical care to critically ill or injured patients while simultaneously navigating through traffic under time constraints [10, 11]. The psychological and physical stress experienced by ambulance drivers can impair their decision-making abilities and reaction times, further increasing the likelihood of accidents [12, 13].
Despite the critical importance of safe and efficient ambulance driving, there has been limited research on the driving behavior of emergency medical personnel, particularly in high-stress environments. Moreover, little attention has been paid to how driving behavior impacts the medical condition of patients during transport and the overall quality of care provided [14]. While pre-hospital and ambulance care research has made significant strides in areas, such as emergency medicine, traumatology, clinical assessments, and patient referrals, the specific challenges and risks associated with ambulance driving remain underexplored [15]. This gap in the literature highlights the need for a deeper understanding of the factors influencing the driving behavior of EMS personnel and their implications for patient safety and care quality.
This study aimed to assess the driving behavior of ambulance drivers, who are also emergency medical personnel, in Ardabil Province, Iran. By examining the factors that contribute to risky driving practices, such as stress, fatigue, and the demands of providing medical care, this research sought to identify strategies for improving safety and efficiency in emergency medical transport. The findings of this study will contribute to the growing body of knowledge on EMS safety and provide evidence-based recommendations for reducing accidents and enhancing the quality of pre-hospital care.
Materials and Methods
Between June 2023 and August 2023, a cross-sectional descriptive study was conducted in Ardabil Province. Initially, the total number of pre-hospital emergency personnel was 442. Based on a total population sampling method with eligibility criteria, 42 individuals were excluded due to having less than six months of experience in pre-hospital emergency services. Consequently, the questionnaires were distributed to 400 eligible personnel. Inclusion criteria included at least six months of work experience, willingness to participate, and no concurrent involvement in similar research. Incomplete questionnaire responses were considered the exclusion criterion. Out of the 400 distributed questionnaires, 380 were fully completed and included in the final analysis.
Data collection was carried out using two tools: A demographic questionnaire and the Manchester driving behavior questionnaire (MDBQ). The demographic questionnaire comprised ten items, including age, marital status, employment status, work experience (in years), education level, field of study, workplace, type of work shift, ambulance driving experience, and history of ambulance-related accidents. The MDBQ, developed by Parker and Reason at the University of Manchester, was used to assess driving behavior [14]. This scale is based on the premise that errors and violations in driving have distinct psychological origins and require different corrective approaches, making it essential to differentiate between them in research. The MDBQ consists of 50 items rated on a Likert scale ranging from 0 to 5, capturing two dimensions: The type of driving behavior and the level of risk posed to others. Abnormal driving behaviors are categorized into four types: lapse errors, slips, deliberate violations, and unintentional violations. These behaviors are further classified based on the level of risk they pose: Behaviors that pose no risk to others and merely provide a sense of comfort (low-risk probability).
Behaviors that are likely to endanger others (moderate-risk probability).
Behaviors that certainly endanger others (high-risk probability).
Lapse errors, reflecting memory and attention failures, included items, such as “I forget where I left my car in a car park” and “I start to drive away from the traffic lights without realizing that they are still red.”
Slips, representing attention or observation failures, included questions, like “I misread the signs and take the wrong turn” and “I fail to notice pedestrians crossing when turning into a side street.”
Deliberate violations, indicating intentional breaches of traffic rules, were assessed with items, such as “I disregard the speed limits on a motorway” and “I drive especially close to the car in front to signal that I want them to go faster.”
Unintentional violations, referring to rule-breaking due to misjudgment or inattention, included items, like “I exceed the speed limit without realizing it” and “I misjudge the speed of an oncoming vehicle when overtaking.”
The MDBQ has demonstrated strong psychometric properties. Parker and Reason [14] reported reliability coefficients of 0.81 for errors and 0.75 for violations in a test-retest study with an 80-driver sample over a seven-week interval. In the current study, the Cronbach’s α coefficient for the MDBQ was calculated at 0.89, indicating high internal consistency.
Data collection was conducted in person by the researcher, who visited both urban and road emergency bases to engage directly with personnel who met the inclusion criteria. The researcher clearly explained the study’s objectives, significance, and relevance to participants, emphasizing the confidentiality and anonymity of their responses. Written informed consent was obtained from all participants, and they were assured of their right to withdraw from the study at any stage without facing any consequences.
To minimize potential stress and ensure accurate responses, questionnaires were completed outside participants’ work shifts, allowing them adequate time and focus. The researcher remained available on-site to clarify any questions or ambiguities regarding the questionnaire. Once completed, the questionnaires were collected immediately and directly by the researcher to maintain data integrity and completeness.
To minimize social desirability bias, participants were assured of the anonymity and confidentiality of their responses, with no identifying information collected. They were informed that data would be analyzed collectively and that there were no right or wrong answers. The voluntary nature of participation and the right to withdraw at any time were also emphasized to encourage honest and unbiased responses.
Data analysis was performed using SPSS software, version 22. Descriptive statistics, including frequency distribution, Mean±SD, were used to summarize and categorize the data. Inferential statistical tests, such as the t-test, ANOVA, and multiple regression analysis, were employed to examine the relationships between demographic variables and MDBQ scores. The Kolmogorov-Smirnov test was used to assess the normal distribution of quantitative variables. A 95% confidence level and a significance level of 0.05 were applied in all statistical tests.
Results
Of 380 personnel participating in this study, 100% were male with a mean age of 32.71±7.81 years, a maximum age of 51 years, and a minimum age of 23 years. Most study participants, 222(58.4%), were married, 234(61.6%) were officially employed, and 222 (58.4%) had a bachelor’s degree. The highest clinical work experience of personnel was 11-20 years (46.3%), with 260 individuals (68.4%) working in 24-hour shifts, 235(61.8%) personnel based in urban areas, and 313(82.4%) having no history of traffic accidents (Table 1).
There was a statistically significant relationship between age (P=0.02), work experience (P=0.03), education (P=0.03), and type of work shift (0.01) and the driving behavior of personnel (Table 2).
The total mean score of personnel driving behavior was 37.95±7.26. Also, the mean scores of driving slips, mistakes, intentional violations, and unintentional violations were 14.52±4.26, 6.53±3.05, 13.99±4.04, and 2.88±1.87, respectively (Table 3).
The results of multiple linear regression analysis showed age, education, and type of work shift were predictors of driving behavior. According to the obtained determination coefficients, 58% of the driving behavior changes were due to the variables mentioned in the model. The suggested regression model had an acceptable fit (F=56.56, P˂0.001) (Table 4).
Discussion
This study aimed to evaluate the driving behavior of emergency medical personnel in Ardabil Province. The present study is significant as it is one of the first to assess the driving behavior of emergency medical personnel operating ambulances. The driving behavior of pre-hospital emergency personnel can have a profound impact on both the clinical condition of the patient and the staff’s ability to provide effective care [1].
The results of this study revealed a significant relationship between age, work experience, education level, and type of work shift and the driving behavior of emergency medical personnel. These findings are consistent with previous research, which has highlighted the impact of occupational and demographic factors on driving behavior. For instance, Watanabe et al. found that ambulance personnel working 24-hour shifts experienced poor sleep quality and were 2.3 times more likely to suffer injuries compared to those working shorter shifts. Additionally, they reported higher levels of fatigue among 24-hour shift workers [2]. In contrast, Yenal et al. observed that personnel working 24-hour shifts had fewer accidents, suggesting that extended shifts may not always negatively impact driving safety [8]. This discrepancy could be attributed to differences in study design, sample characteristics, or even regional factors. Yenal et al.’s study may have involved a sample with different baseline driving behavior or environmental factors that moderated the effect of shift length on driving safety. Furthermore, cultural or organizational differences in how shifts are managed could also explain why longer shifts did not result in the same level of negative impact on driving behavior. Similarly, Eksi et al. reported no significant differences in gender, age, experience, or professional title among ambulance personnel involved in traffic accidents, which contrasts with the findings of the present study [11]. Moreover, Prohn and Herbig [10] demonstrated the value of simulator-based training in improving ambulance drivers’ awareness and reducing risky behavior, suggesting that education and ongoing skill development may be more decisive than experience alone. The lack of significant findings in Eksi et al.’s study may suggest potential limitations in sample size or the operationalization of key variables, such as experience or shift type. Moreover, their study might not have accounted for other important variables, such as the psychological impact of the work environment or the training provided to emergency personnel, which could mediate the relationship between demographic factors and driving behavior.
These contrasting findings highlight important gaps in the literature and emphasize the need for future research to critically examine the factors that contribute to these differences. A deeper exploration of the role of work environment, psychological stress, and other occupational factors could provide a more comprehensive understanding of how shift work impacts the driving behavior of emergency medical personnel.
Furthermore, Vatani et al. found that the mean age of drivers with a history of accidents was significantly higher than those without such a history, indicating that age can influence driving behavior [15]. This aligns partially with our findings, as our data also suggest that drivers with more years of experience tended to report better adherence to safe driving practices. However, unlike Vatani et al., we did not observe a direct correlation between age and accident history. This discrepancy may stem from differences in the studied populations; while their research focused on a broader range of public service drivers, our study was limited to emergency medical personnel in Ardabil Province, who often undergo more specialized training and face different stressors. The interplay between experience and factors, such as fatigue or stress appears to be crucial [4]. Although increased exposure to various driving situations can enhance judgment and reaction time, these benefits may be diminished under conditions of chronic fatigue, particularly in high-pressure roles, like emergency response [5]. For instance, a high number of missions per shift may lead to cognitive overload and reduced situational awareness, increasing the likelihood of accidents [9].
In the present study, 67 cases (17.6%) reported being involved in an ambulance accident. This figure underscores a significant occupational hazard within the EMS system in Ardabil Province. Between 2012 and 2016, 46 cases of ambulance accidents were reported in Iran, with a peak in 2015 (35%). Of these, 52% involved EMS ambulances, and notably, 39% of the 109 injuries and 25% of the 53 fatalities were among ambulance drivers and technicians [16]. These statistics point to a concerning vulnerability among frontline EMS staff. When compared with international data, the picture becomes more complex. Türkdemir and Aysun documented 614 ambulance accidents in Turkey between 1960 and 2002, of which only 3 resulted in fatalities and 367 in injuries. In contrast, New York State records around 400 ambulance accidents annually, with approximately two injuries per day, and an estimated 75% of these accidents being preventable [17]. The considerably higher rate of preventable accidents in New York, despite presumably stricter regulations and advanced infrastructure, suggests that systemic and behavioral factors, such as adherence to safety protocols, road conditions, or driver training play a critical role. The differences across these contexts may be attributed to several factors. In Iran, particularly in provinces, like Ardabil, EMS systems often face constraints, such as limited resources, outdated vehicles, variable driver training standards, and inconsistent traffic law enforcement. Cultural differences in road-sharing behavior and public awareness may also influence accident rates. Practically, these findings highlight an urgent need for targeted interventions. Establishing standardized training protocols with a strong emphasis on defensive driving, improving public awareness about ambulance right-of-way, and implementing digital monitoring systems (such as telematics to monitor driving behavior) could help reduce accident rates. Furthermore, periodic risk assessments and the integration of traffic data into shift planning may help mitigate high-risk periods or routes, especially during peak hours or in congested urban centers. These strategies could significantly enhance safety for EMS personnel and the public they serve in Ardabil Province.
Multiple contributing factors have been identified in prior research. For example, Pappinen and Nordquist [5]highlighted how urgency level and seasonal conditions affect driving speed, which may increase accident risk in poor weather. Araújo et al. [9] noted additional psychological pressure faced by ambulance drivers during the COVID-19 pandemic, suggesting that both physical and mental load are essential considerations.
The findings of this study can significantly contribute to improving training programs, shift management, and safety protocols for emergency medical personnel in Ardabil Province. Given the significant relationship between age, work experience, education, and type of work shift and driving behavior, training programs should focus on enhancing safe driving awareness and skills, particularly for less experienced and younger personnel. Additionally, to reduce fatigue and improve performance, shift management should be adjusted to minimize long shifts (such as 24-hour shifts) and ensure adequate rest time for personnel. Moreover, implementing comprehensive safety protocols and conducting regular assessments of driving behavior can foster a safety culture, reduce accidents, and ultimately improve service quality and patient safety.
The present study has several limitations that should be considered. The data were collected using a self-report questionnaire, which is subject to response biases, including underreporting or overreporting of certain behaviors. This could affect the accuracy of the reported driving behaviors and may not fully reflect actual practices.
Also, the study was conducted exclusively among emergency medical personnel in Ardabil Province, which limits the generalizability of the findings. The unique characteristics of this region, such as workforce structure, training standards, and cultural factors, may not be representative of other regions or populations. Therefore, caution is needed when applying the findings to other geographical locations or contexts.
Another limitation pertains to gender bias in the study sample. The EMS in Ardabil Province exclusively employ male personnel in driving roles, and as such, the study’s findings are based on an all-male sample. The absence of female drivers in this context means that the study may not fully capture potential gender differences in driving behavior or safety practices. Future studies that include both male and female emergency personnel would provide a more comprehensive understanding of how gender may influence driving behavior in this context.
Lastly, the cross-sectional design of the study limits the ability to establish causal relationships between the variables. As a snapshot of the situation at a specific point in time, it does not allow for the examination of changes over time or the exploration of cause-and-effect dynamics between demographic factors and driving behavior.
Conclusion
Ambulance driving plays a critical role in ensuring patient health, well-being, and safety. Given its importance, cultivating a strong and safety-oriented driving culture should be recognized as a fundamental component of care delivery within EMS. The findings of this study, highlighting the notable incidence of ambulance accidents and the contributing factors, such as fatigue, high mission loads, and stress, underscore the urgent need for structured interventions. To address these challenges, specific and practical actions should be taken. First, EMS institutions in Ardabil Province can implement targeted training programs that not only enhance driving skills but also integrate modules on fatigue management, stress reduction, and situational awareness. Second, shift scheduling should be optimized to limit the number of missions per shift and ensure adequate rest periods, especially during high-demand hours. Third, establishing a standardized incident reporting and feedback system can help identify recurring risk patterns and inform continuous improvement efforts.
By promoting these strategies, EMS authorities can create a safer working environment for drivers and technicians, reduce the frequency of ambulance-related accidents, and ultimately improve the quality and safety of emergency medical response in the region.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Ardabil University of Medical Sciences, Ardabil, Iran (Code: IR.ARUMS.REC.1402.095). All methods were conducted in accordance with the Declaration of Helsinki. Participants’ privacy and confidentiality were maintained, and informed consent was obtained prior to their involvement in the study.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank everyone who contributed to this research.
References
- Becker J, Hugelius K. Driving the ambulance: An essential component of emergency medical services: An integrative review. BMC Emergency Medicine. 2021; 21(1):160. [DOI:10.1186/s12873-021-00554-9] [PMID]
- Watanabe BL, Patterson GS, Kempema JM, Magallanes O, Brown LH. Is use of warning lights and sirens associated with increased risk of ambulance crashes? A contemporary analysis using national ems information system (NEMSIS) data. Annals of Emergency Medicine. 2019; 74(1):101-9. [DOI:10.1016/j.annemergmed.2018.09.032] [PMID]
- Asadi H, Habibi Soola A, Gheybati F, Davari M. Time indices of prehospital emergency services in Ardabil City, Iran, 2020. Health in Emergencies and Disasters Quarterly. 2021; 6(3):161-8. [DOI:10.32598/hdq.6.3.377.2]
- Hu W, Cicchino JB. Lowering the speed limit from 30 mph to 25 mph in Boston: Effects on vehicle speeds. Injury Prevention. 2020; 26(2):99-102. [DOI:10.1136/injuryprev-2018-043025] [PMID]
- Pappinen J, Nordquist H. Driving speeds in urgent and non-urgent ambulance missions during normal and reduced winter speed limit periods-A descriptive study. Nursing Reports. 2022; 12(1):50-8. [DOI:10.3390/nursrep12010006] [PMID]
- Venesoja A, Lindström V, Castrén M, Tella S. Prehospital nursing students' experiences of patient safety culture in emergency medical services-A qualitative study. Journal of Clinical Nursing. 2023; 32(5-6):847-58. [DOI:10.1111/jocn.16396] [PMID]
- Bui DP, Hu C, Jung AM, Pollack Porter KM, Griffin SC, French DD, et al. Driving behaviors associated with emergency service vehicle crashes in the U.S. fire service. Traffic Injury Prevention. 2018; 19(8):849-55. [DOI:10.1080/15389588.2018.1508837] [PMID]
- Yenal S, Gültekin T, Pakdemirli A. Driver behaviors of 112 emergency medical services personnel. Eurasian Journal of Emergency Medicine. 2020; 19(2):78-81. [DOI:10.4274/eajem.galenos.2020.90267]
- Araújo DV, Lima MMS, Fernandes CDS, Frota NM, Caetano JÁ, Galindo Neto NM, et al. Experience of ambulance drivers on transfer of suspected or confirmed patients for COVID-19. Revista Gaucha de Enfermagem. 2023; 44:e20210319. [DOI:10.1590/1983-1447.2023.20210319.en] [PMID]
- Prohn MJ, Herbig B. Traffic safety knowledge gain of ambulance drivers after simulator-based training. BMC Medical Education. 2022; 22(1):216. [DOI:10.1186/s12909-022-03279-w] [PMID]
- Eksi A, Celikli S, Catak I. Effects of the institutional structure and legislative framework on ambulance accidents in developing emergency medical services systems. Turkish Journal of Emergency Medicine. 2015; 15(3):126-30. [DOI:10.1016/j.tjem.2015.11.006] [PMID]
- Joshi RS, Goel P, Adatiya VH, Seth AS, Rasal AV. Eye donation: Knowledge, beliefs, awareness, and willingness among ambulance drivers in central India. Clinical Ophthalmology. 2023; 17:1263-9. [DOI:10.2147/OPTH.S401768] [PMID]
- Chew KS, Low MY. Types and risk factors of ambulance accidents: A scoping review. The Medical Journal of Malaysia. 2022; 77(1):60-70. [PMID]
- Parker D, Reason JT, Manstead ASR, Stradling SG. Driving errors, driving violations and accident involvement. Ergonomics. 1995; 38(5):1036-48. [DOI:10.1080/00140139508925170] [PMID]
- Vatani J, Rezaei S, Haghighi Malwani Z, Mohammadi S, Faghihnia Torshizi Y. Comparison of accident-prone behavioral indicators in car drivers. Iran Occupational Health. 2022: 12; 19(1):3. [DOI:10.52547/ioh.19.1.39]
- Shakri Kha, Ghanion A. [Investigation of ambulance accidents in Iran in 2015-2016 (Persian)]. Paper presented at: 8th International Congress on Health in Accidents and Disasters, Tehran, 2019 May 19; Tehran; Iran. [Link]
- New York State Department of Health. The operation of emergency medical services vehicles. New York: New York State Department of Health; 2020. [Link]
Type of article: Research |
Subject:
Emergency
Received: 2025/02/3 | Accepted: 2025/06/29 | Published: 2026/01/1
Received: 2025/02/3 | Accepted: 2025/06/29 | Published: 2026/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
