

Volume 10, Issue 4 (Summer 2025)
Health in Emergencies and Disasters Quarterly 2025, 10(4): 279-290 |
Back to browse issues page



Ethics code: IR.SKUMS.REC.1401.151
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sheikhi R A, Heidari M, Jafari H, Heydarpoor S, Yadollahi S, Pakjouei S. Ambulance Crash During Emergency Operation in Iran: A Qualitative Study. Health in Emergencies and Disasters Quarterly 2025; 10 (4) :279-290
URL: http://hdq.uswr.ac.ir/article-1-618-en.html
URL: http://hdq.uswr.ac.ir/article-1-618-en.html
Rahim Ali Sheikhi1 

 , Mohammad Heidari *2 , Hamid Jafari3 , Sadegh Heydarpoor4 , Salman Yadollahi4 , Shahrzad Pakjouei5
, Mohammad Heidari *2 , Hamid Jafari3 , Sadegh Heydarpoor4 , Salman Yadollahi4 , Shahrzad Pakjouei5
, Mohammad Heidari *2 , Hamid Jafari3 , Sadegh Heydarpoor4 , Salman Yadollahi4 , Shahrzad Pakjouei5
1- Community-Oriented Nursing Midwifery Research Center, Shahrekord University of Medical Sciences, Shahrekord, Iran.
2- Community-Oriented Nursing Midwifery Research Center, Shahrekord University of Medical Sciences, Shahrekord, Iran. ,Heidari@skums.ac.ir
3- Department of Health in Emergency and Disaster, Sirjan School of Medical Sciences, Sirjan, Iran.
4- Disaster and Emergency Medical Management Center, Shahrekord University of Medical Sciences, Shahrekord, Iran.
5- Health in Emergency and Disaster Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Community-Oriented Nursing Midwifery Research Center, Shahrekord University of Medical Sciences, Shahrekord, Iran. ,
3- Department of Health in Emergency and Disaster, Sirjan School of Medical Sciences, Sirjan, Iran.
4- Disaster and Emergency Medical Management Center, Shahrekord University of Medical Sciences, Shahrekord, Iran.
5- Health in Emergency and Disaster Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Full-Text [PDF 475 kb]
(1449 Downloads)
| Abstract (HTML) (4309 Views)
Full-Text: (1901 Views)
Introduction
Medical care management outside the hospital is handled by prehospital emergency medical services (PEMS). It is a vital component of the healthcare system, intended to respond to crashes and time-sensitive illnesses. PEMS plays a critical role as the first line of treatment for emergency patients [1]. The system’s activities include answering phone calls, dispatching to the scene, providing on-site care by trained professionals and continuing care in a vehicle, such as an ambulance [2].
Working in PEMS is one of the most challenging and stressful situations within the healthcare system, and ensuring the safety of patients and responders is the top priority during PEMS care [3]. PEMS faces three main challenges: Challenges in human resources (individual characteristics of human resources and personnel’s dissatisfaction), challenges in an organization (structural challenges, lack of equipment, and human resource limitation) and sociocultural challenges (environmental-social and cultural challenges) [4, 5].
The danger of ambulance transport is inherent. There is ample evidence that the ambulance is a challenging work environment with many risks for patients and EMTs [6]. EMTs must travel during daytime and nighttime hours and encounter various hazardous weather, road, and traffic conditions. Ambulance drivers frequently face stressful situations as they travel at high speeds and in vehicles with poor maneuverability [7].
One of the main challenges for EMTs is driving an ambulance and crash caused by emergency services. It is essential to investigate the crash prevention and care services provided by EMTs in the PEMS and the challenges involved in improving safety services at the EMS level. EMTs possess substantial knowledge in this field and are well-informed about the associated challenges [4]. ACs have always been among the challenges of the health and treatment field for various reasons, including the social burden of the crash, the possibility of morbidity and mortality of patients, companions and EMTs, and the high cost of rebuilding damaged ambulances [7].
ACs can harm the PEMS. They may make ambulances inoperable and reduce emergency capacity. They can injure technicians and patients in the ambulance and damage third parties. They can also incur costs, like ambulance repairs and compensation for the injured [8]. According to the police report, about 1000 ACs occurred in 2021. Encountering ACs can create many problems for the personnel involved, and up to 15% of these crashes can result in the deaths of EMTs, which are preventable [9]. The potential for injuries to EMTs and delays in patient care caused by ACs has caused global attention. Ambulance delays pose a significant barrier to patients receiving timely care and can worsen a patient’s condition. Traffic congestion has caused delays that have led to the deaths of more than 20% of patients in need of emergency treatment while on their way to a treatment center [10]. ACs are four times more likely to cause fatalities than other types of crashes, according to research [11]. The occupational fatality rate among EMS workers in the US was estimated at 12.7 per 100000 workers per year, compared with a national average of 5 per 100000 workers per year [12]. There are at least 6500 yearly crashes because of inadequate vehicle performance standards, improper maintenance, variable operator training, and failure to use safety restraints correctly [13].
Accurate data on ACs during operations in Iran has not been recorded or published. In a study by Shakeri and Ghanion, 46 ACs were reported during 2012-2016. Most ACs (35%) occurred in 2014. Of the 109 reported injuries resulting from ACs, 42 cases (39%) and 13 cases (25%) were related to the injuries and death of the ambulance driver and technician, respectively [14]. However, the National Medical Emergency Organization has run programs like “defensive driving” training in recent years. The effectiveness of such programs has not yet been adequately proven [15].
The Haddon matrix approach was developed in the 1950s and utilized during the 1960s and 1970s. The fundamental concept of systems theory is that incidents happen when there is misalignment in the relationships between the components of complex systems. This approach holds that all the components are equally crucial for the road system’s successful operation. Systems theory aims to mitigate crashes by modifying the elements of the transportation system. It emphasizes the importance of road engineering and vehicle safety. As a crash prevention theory, systems theory has been more successful than other theories. In developed countries, crash rates have been significantly reduced due to improvements in road systems, traffic control, and vehicle design [16].
Iran has areas that are difficult to reach, rural roads that are sometimes unsafe and a lack of enough ambulances. The quality and timeliness of emergency medical assistance are impacted by this situation, which creates financial and psychological problems. EMTs’ experiences during emergency operations were examined in a research study using the Haddon matrix framework. The study aims to identify safety issues and propose solutions to improve EMS and reduce adverse consequences.
Materials and Methods
Research design
A framework analysis approach was used in this qualitative study, which is a method for qualitative data analysis [17]. This study used the basic framework derived from the Haddon matrix approach. Systems theory posits that crashes are caused by misalignments in the relationships between the components of a complex system. According to this approach, for the successful operation of the road, none of the components of the transportation system (human, vehicle, and road) can be considered more important than the other components [16].
Participants and data collection
The data were collected through in-depth and semi-structured interviews. The research team developed the interview questions with input from the literature and then reviewed and modified them with feedback from several experts. The main question was, “How was your experience of a crash with an ambulance during an operation?” and specific questions followed. The participants were EMTs with experience in at least one AC. The sampling was purposeful and continued until data saturation. A total of 18 interviews were conducted with EMTs, lasting between 60 and 90 minutes each. The interviews were recorded with the participants’ informed consent, and a consent form was completed at their workplace. The researchers immediately transcribed the recordings.
The inclusion criteria require willingness and consent to participate in the study, possession of a B1 or B2 type certificate, a minimum of 3 years of operational work experience in PEMS, and participation in at least one AC during emergency missions. The exclusion criteria also include unwillingness to continue participating in the research process.
Data analysis
The data were analyzed using the framework analysis method with MAXQDA software, version 10. This method combines the initial idea (deductive approach) and experimental issues (inductive approach) in the analysis process. We used framework analysis to analyze the responses to question 9. Framework analysis is a rigorous five-stage method for analyzing qualitative data. The five stages are as follows: Familiarization with the responses by reading completed questionnaires, identifying key themes in the responses (we also used predefined issues focusing on benefits, problems, and study objectives to develop the thematic framework), indexing that involves copying all relevant participant quotes from the questionnaires and placing them in a Word document under relevant themes/subthemes identified by participant number, charting that involves iteratively reviewing and revising the initial framework (we abandoned initial benefit/problem themes because participants viewed some themes as either benefits or problems and reach an agreement on a final four-theme framework that includes subthemes), mapping and interpretation that involves charting the themes with a summary of the main descriptive comments and creating an explanatory account.
The authors can provide the index of all responses and framework history upon request [17].
Rigor
The researchers spent enough time gaining a deep and accurate understanding of the information to ensure the accuracy of the data. Four criteria were used to assess the validity and reliability of this study: Acceptability, similarity, conformability, and transferability. To this end, several experts reviewed and revised the interviews and the codes and categories that emerged from them. The credibility of the findings was also assured with constant engagement with the subject matter. Qualitative research experts reviewed and confirmed the interviews and codes. The study’s methods were detailed so others could verify and improve the findings. Two people, similar to the participants, confirmed the findings’ transferability. They were not participants [18].
Results
Demographic characteristics
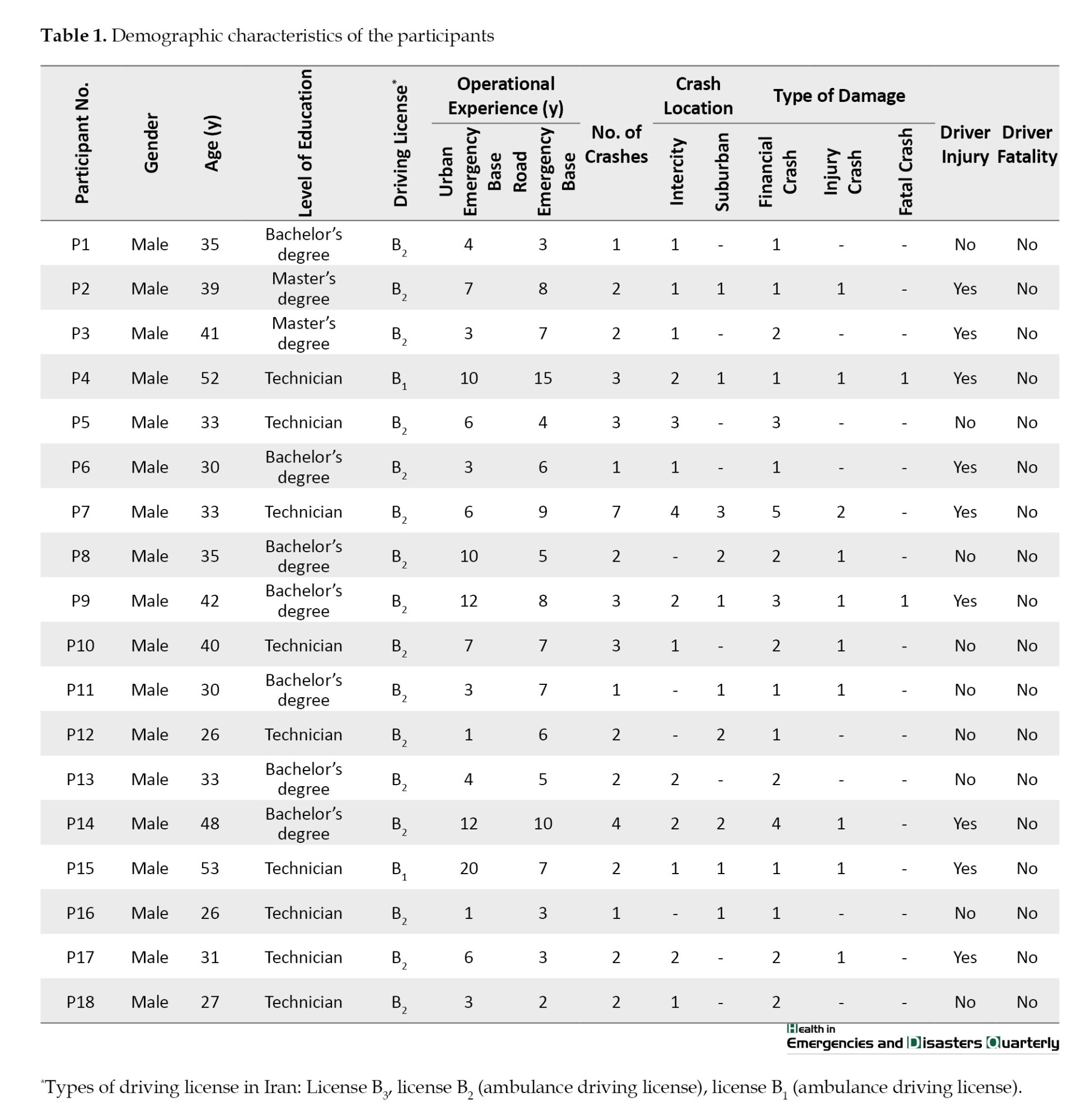
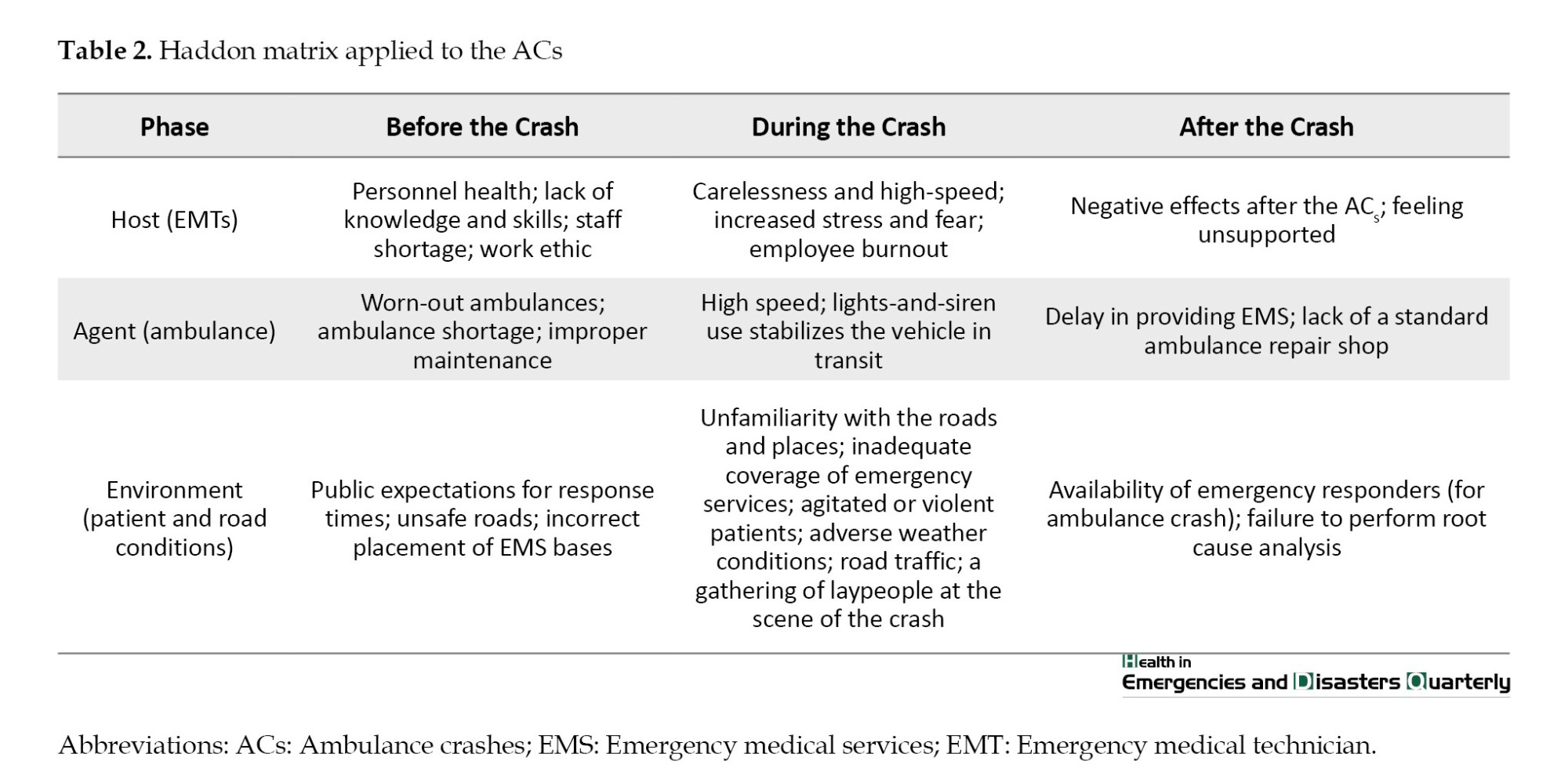
All 18 study participants were male. It should be noted that in Iran’s PEMS, EMTs are exclusively male [19]. The participants’ age range was between 26 and 52. Additional information about the participants can be found in Table 1. Table 2 classified the findings into three main classes and 27 subclasses based on the Haddon matrix framework in three phases: Before, during and after the crash.
Host (EMTs)
Before the crash took place
In the PEMS, each emergency base has an ambulance staffed with two EMTs dispatched to assist in receiving the mission from the dispatch unit. According to the work rules, both EMTs must possess a special license to drive an ambulance (B2 type) and one of them will be responsible for driving the ambulance when dispatched to the scene.
Personnel health
Physical fitness and mental health are assessed at the time of student admission to the emergency medicine field. This evaluation is also required for employment at PEMS [2]. Unfortunately, throughout the years of service, such assessments have not been performed, and the physical and mental well-being of the staff has not been taken into account or evaluated.
Recruitment in the PEMS is done among university graduates, and there are two stages of written and practical tests. Physical criteria include height, weight, body mass index (BMI), physical fitness tests, mental tests, etc. The most crucial challenge in recruitment is the lack of graduates, and a reduction follows this in the number of applicants for employment [20].
“When EMTs are relieved from physical fitness requirements due to recruitment, they may pay less attention to staying fit and agile. This condition can lead to weight gain, reduced mobility and decreased agility and reaction time during emergency operations. I have also heard that some EMTs may turn to drug abuse, which can reduce their concentration, accuracy, and decision-making ability while driving and performing operations” (participant [P] 3).
Lack of knowledge and skills
EMTs lack knowledge and skill in two main areas. First is the understanding of driving laws and regulations. EMTs lack sufficient knowledge about driving rules and regulations in the country, leading to non-compliance. The laws regarding emergency vehicles include exceptions, leading to misunderstandings. This misunderstanding may result in false confidence and potentially cause crashes while driving.
“I didn’t have 100% knowledge of the traffic rules, and I thought the ambulance was always right in an emergency, and you could go at any speed and in any direction. However, it was not like that. The traffic rules change over time, and we don’t always have enough information about them, so sometimes this lack of knowledge leads us to not comply with them” (P9).
Most of Iran’s PEMS workforce is young. Most recruits are between 22 and 25. Some employees lack driving experience and do not possess a driver’s license. In Iran, individuals can obtain a driver’s license at 18, so even those with permits have limited driving experience. While having a driver’s license is a requirement for employment at PEMS, in recent years, due to personnel shortages, EMTs without a permit have been hired with the expectation that they obtain one within a specified period. Consequently, many young EMTs have their first driving experience while operating an ambulance and thus may lack sufficient driving skills. Given the unique challenges of driving an ambulance in emergencies and the drivers’ lack of experience, the risk of crashes is heightened.
“Many of us in the EMS lack experience driving ambulances. When we start working in the EMS, we often drive an ambulance for the first time, which presents its challenges. Ambulances are larger than our vehicles, making driving and parking more difficult. While having a driver’s license is a requirement, gaining driving experience and skills is crucial for effective rescue operations” (P4).
The primary responsibility of the PEMS is to maintain the ambulances, which are essential for carrying out missions. A lack of knowledge about an ambulance’s technical aspects can cause it to fail to meet required standards during missions. This condition may lead to crashes due to technical defects. Inadequate driving skills for ambulance operations are a significant factor in these crashes. PEMS in Iran uses only Mercedes-Benz Sprinter ambulances, and as a result, many EMTs, especially new personnel, lack the necessary skills to operate these ambulances.
“Driving an ambulance requires a high level of skill that not everyone has. Ambulances differ from regular cars and have a higher roof, making driving more challenging, especially at high speeds. Additionally, ambulances are not regularly available, and driving them typically requires working shifts to gain the necessary skills” (P6).
Staff shortage
One of the significant issues affecting the country’s PEMS is the shortage of EMTs, which has been a longstanding problem. Individuals with associate’s and bachelor’s degrees can enroll in PEMS training programs in Iran. However, the academic infrastructure for PEMS has not kept pace with its rapid development, resulting in a scarcity of specialized professionals in this field. The shortage of personnel has led to longer working hours, causing fatigue and job burnout and subsequently increasing the risk of crashes. Since resilience helps prevent job burnout, we should hire more resilient staff in this field [21]. Additionally, there is a shortage of EMTs holding a B2-type ambulance driver’s license. This shortage has led to hiring emergency medical degree holders without ambulance driver’s licenses, forcing licensed technicians to drive during missions, leading to fatigue and reduced focus, thereby increasing the risk of crashes.
“Every day, we face a staff shortage in the prehospital setting. This condition makes us even more concerned because forced overtime exhausts us and decreases our concentration. We find it difficult to focus as our thoughts revolve around being away from our families” (P2).
Work ethics
The lack of responsibility for the assigned duties has led to negligence in maintaining the ambulances. As a result, the useful life of these vehicles in the PEMS is shortened, and the ambulances do not perform efficiently during operations.
“Our colleagues usually do not take good care of ambulances. They take much better care of their cars because they have to pay for not taking care of them, but the government pays for the cost of the ambulances” (P10).
During the crash
Carelessness and high-speed
Time plays a crucial role in delivering PEMS. Prompt provision of medical assistance is essential, especially during the “golden time.” However, some EMTs may feel compelled to compensate for lost time by speeding and driving under unsafe conditions. One significant contributing factor to ambulance speeding and the increased risk of crashes is the dispatch unit’s announcement of emergency conditions for critical patients (Code: 10-33). Moreover, providing or receiving incorrect addresses for the assistance location adds to the pressure and stress experienced by EMTs.
“The role of the dispatch and operations unit is crucial. However, the use of the 10-33 code by the dispatch unit caused significant stress, which is not appropriate” (P6).
“The dispatch unit plays a crucial role. For instance, sending you to an area outside your range can make you nervous and lead to a crash. It’s important to follow the 10-33 code and move faster, but going too far can also create conditions for a crash. Additionally, if the dispatch provides the wrong address, it can confuse you and lead to driving errors such as crossing the road multiple times, reducing your concentration while driving” (P18).
Stress and fear
EMTs’ primary fears include arriving late, potential arguments and conflicts with patients and their families, and unfamiliar environments. Those with a history of crashes also fear another crash, injuring themselves, their colleagues, and the patient and being questioned by the organization.
“Increased fear and stress raise the probability of a crash. Error rates rise, and performance deteriorates, making it difficult to manage the crash scene. Work efficiency decreases, and normal control is lost. Mental conflict and signs of impatience arise, leading to aggressive reactions to even insignificant matters. This condition could escalate to conflicts with colleagues or patients” (P5).
Employee burnout
EMTs face stressful environments such as crash scenes with multiple injured and critical patients and increasing shifts without enough rest, which are very challenging to work in PEMS. Job stress can directly affect the emotional exhaustion, depersonalization, and personal inadequacy of PEMS workers and generally cause burnout [22].
“Our work is extremely demanding and sensitive. The increase in work shifts, driven by financial and economic needs, disrupts our sleep patterns and keeps us away from our families. All these factors contribute to our physical and mental exhaustion, leading us to lose our motivation to work gradually” (P11).
After the crash
Negative effects after the crash
Operational forces with a history of acute care suffer short- and long-term complications after a crash. They lose their confidence in driving and may not want to drive anymore, or they may drive at low speeds with excessive caution, causing delays and disruptions in the delivery of assistance. Posttraumatic stress disorder (PTSD) is one of the long-term complications that EMTs suffer from, especially in crashes involving injury and mortality, which can significantly affect their performance. Stigma from colleagues and the organization is also a significant factor contributing to the mental and emotional challenges faced by EMTs. The feeling of failure and self-blame intensifies among EMTs, leading to a loss of trust and reduced work efficiency, impacting their self-confidence, trust in the higher-level system, colleagues, and public trust in the PEMS.
“After the crash, I noticed a significant decrease in my performance. I had trouble concentrating and dwelling on the crash for extended periods. The fact that someone died in the crash left me feeling depressed and caused me to lose my appetite for quite some time. I struggled with low motivation at work and often blamed myself for what had happened. As a result, I became more cautious, driving slower and losing my sense of urgency. I was constantly vigilant, fearing another mishap. The incident stressed me and caused me to withdraw from friends, occasionally taking days or months off from work to collect myself” (P8).
“How your colleagues view your changes, and they label you as reckless and dangerous within the system, is very frustrating. This condition also impacts your personal life. You are no longer patient with other tasks and get upset about the next operation, sometimes even with yourself. The severe stress leads to digestive problems and vomiting, making it impossible for you to serve the patients effectively” (P14).
Feeling unsupported
After responding to a medical emergency, EMTs have expressed concerns about the lack of financial and psychological support from both the authorities and the organization. They are also facing an increased workload due to having to cover some of the costs of repairing and rebuilding the ambulance and insufficient insurance coverage for ambulances.
“The organization does not provide much support. It looks for the culprit but does not offer mental, physical, or financial assistance. It fails to address the root cause of the issue and does not try to prepare you for future work days. There is no plan in place, and there is no committee to address the important causes of the issue or provide solutions. Additionally, the organization does not offer access to a psychologist or take preventive measures to avoid similar incidents in the future” (P4).
Agent (ambulance)
Before the crash took place
Worn-out ambulances
The country’s ambulance system is in poor condition. Due to economic sanctions, new and updated ambulances have not been imported for many years. As a result, existing ambulances are being overused and do not meet emergency system standards. Most ambulances in the country are not domestically manufactured (Mercedes-Benz Sprinter), resulting in limited service centers and guarantees. This condition makes finding original auto spare parts challenging, leading to technical defects. The use of fake auto spare parts increases the risk of crashes.
“The country’s ambulance system is aging, with most ambulances being in service for over 15 to 20 years, well beyond their intended lifespan. It’s becoming increasingly challenging to find original spare parts, leading to the use of second-hand or non-original parts, which in turn lead to additional issues” (P13).
Ambulance shortage
The lack of new ambulances in the PEMS has led to a persistent shortage of vehicles, resulting in the overuse of existing ones. Ambulances are not allocated based on regional geography and climate conditions, leading to inefficiencies in cold and inaccessible areas. In urban settings, the size of ambulances can cause delays in providing aid, especially in older parts of the city. Additionally, the outdated ambulances lack modern features such as GPS, making it challenging to locate the assistance site.
“There has always been a shortage of ambulances. No new ambulances are available whenever a new emergency base is set up, so they must refurbish the existing ones and put them into service. Operating these ambulances in winter is extremely challenging, especially in the city’s narrow streets. The ambulances are unsuitable for such conditions” (P3).
Improper maintenance
Every vehicle requires regular checks and servicing to be ready for operation. However, an ambulance is a rescue vehicle and must always be prepared. One of the primary responsibilities of EMTs is to ensure the ambulance is operating correctly at the start of each shift, and this daily check should be documented.
During the crash
Speed and lights-and-siren use the stability of the vehicle in transit
Emergency providers often drive high-speed ambulances to reach sites quickly. This condition is especially true when a command or emergency (Code: 10-33) is issued from the dispatch center to allow the ambulance to pass through using lights and sirens. However, it is essential to note that this can also increase stress and distress for the driver, patient, patient’s companions, and other citizens.
“The new ambulances have good acceleration and speed. When the lights and sirens are on, the EMTs may experience increased stress and false confidence. This condition can lead to the belief that everyone is obligated to yield, allowing the ambulance to maneuver as needed, increasing the chance of a collision” (P8).
After the crash
Delay in providing EMS
A crash during the rescue operation causes interference and delays, which can result in injuries to the EMTs, patients, and their companions. Additionally, the ambulance is taken out of service after a crash. Due to the severe shortage of ambulances, replacing them becomes more challenging. Sometimes, EMTs are unfamiliar with the replacement ambulance, increasing the probability of errors or crashes.
Lack of standard ambulance repair shop
After a crash, the top priorities are to repair and reconstruct the ambulance so it can return to service quickly. A major challenge after a crash is the lack of authorized repair shops and auto parts. Non-standard repairs significantly raise the risk of future crashes.
“Ambulances have often been involved in crashes, and while air conditioning issues are sometimes unavoidable, they are not always fully repaired. Instead, they are rushed into service, meaning you could drive a vehicle with technical defects and non-original auto spare parts” (P5).
Environment (the route and location of the help requestor)
Before the crash took place
Unsafe roads and incorrect placement of emergency bases
Driving on non-standard roads, especially without warning signs, increases crash risks for EMTs. Improper site selection and establishing emergency bases in incident-prone areas can lead to longer travel distances to reach the scene of an emergency, increasing the probability of crashes on non-standard roads and delaying the time it takes to assist.
“The construction of the emergency base is done in the most distant and inappropriate place, so it takes a long time for the operation unit to enter urban or rural areas. This late arrival at the crash scene angered and caused complaints among the patient and his companions” (P4).
During the crash
Unfamiliarity with the route and place
The shortage of staff and frequent movement of EMTs between bases has made them unfamiliar with the area and the best routes for seeking help. The lack of online routing tools has made their work harder. Callers often provide incorrect or incomplete addresses in emergencies due to high stress. Also, animals on roads, especially in forests and rural areas, raise crash risks.
Inadequate coverage of EMS
Despite introducing the PEMS (portable emission measurement system) in the country, many areas and roads are still not adequately covered by the PEMS. This condition has led to delays in providing aid, increased burnout, and longer driving distances for the EMTs.
“Driving with an incorrect address, frequent stops to check the map, and many road crossings contribute to reduced focus on the road. Unfamiliarity with the area means not knowing alternate routes with less traffic, and longer routes increase travel time, potentially leading to crashes” (P17).
Agitated or violent patients, adverse weather conditions, road traffic, laypeople’s
The patient’s critical condition and their companions’ pressure can stress EMTs. This condition may cause them to speed in the ambulance. Weather conditions, road traffic, and bystanders gathering at the crash scene can also affect the relief effort. When a patient is in critical condition, the patient’s companions may urge the driver to go faster. The dispatcher unit also announces the critical situation, which may increase speed. Also, consider weather, slippery roads, heavy traffic (especially during school closures), bystanders at the crash scene, disruptions to treatment, and the risk of another crash.
After the crash
Availability of PEMS responders for AC and failure to perform root cause analysis
After a crash, an alternative ambulance must be available for relief operations. This is to minimize patients’ wait time in any situation. By analyzing the causes of these crashes, we can reduce their frequency. We should examine three areas: Personnel, vehicles and the environment.
“Unfortunately, air crashes always happen and are inevitable. However, their causes have never been scientifically and fundamentally investigated in our country, and written instructions have not been developed for air crashes. Unfortunately, the rate of such crashes is also increasing” (P11).
Discussion
The Haddon matrix has three key components that influence a crash. They are the host, agent, and the physical and social environment. Host refers to the individual or individuals at risk, such as EMTs or the patient. The agent refers to the energy applied during an injury, in this case, the ambulance. The physical environment refers to the injury site. It includes road design maintenance and ambulance design. The social environment refers to social, legal, and cultural norms and practices. The second dimension of the Haddon matrix shows the timing of factors that contribute to the event’s occurrence: Before the crash, crash, and after the crash [23]. In Haddon’s injury matrix, EMTs serve as hosts, allowing us to examine various aspects of injuries that occur in the ambulance during patient care and transport. According to the results, essential host factors that contribute to the safety and reduction of adverse events include personnel health, lack of knowledge and skills, human resource shortages, work ethic, carelessness, high speed, stress and fear, burnout, negative effects after the incident, and feeling unsupported. In the study by Brice et al., essential host factors that contribute to ambulance safety include physical fitness, sleepiness, education, knowledge, skills, and capabilities [5].
The skill of the EMS driver plays a crucial role in ensuring the safety of both the vehicle occupants and the patient’s medical outcome. The data showed that 78% of study participants had a history of crashes. Custalow and Gravitz’s study found that ambulance drivers in crashes often had prior crashes. Forty-nine percent of the EMS providers had previous crashes [24]. EMS providers in good physical condition can deliver EMS to patients more quickly and effectively. The prevalence of substance abuse among EMS providers is not well documented, but it is believed to be as high as 40% in other emergency response professions [25].
The shortage of EMTs in the field of PEMS has led to increased workload and fatigue among these EMS providers, eventually resulting in job burnout. EMS providers frequently work 12-hour or 24-hour shifts with limited opportunities for meals or rest, leading to fatigue and adverse side effects. It has been discovered that extended working hours result in more medical errors and adverse side effects [26]. Moshtagh Eshgh et al. examined the occupational stress of PEMS personnel in Iran. The results showed that PEMS personnel’s work stress caused burnout. It led to emotional exhaustion, depersonalization, and feelings of inadequacy. Addressing the sources of stress and implementing measures to manage it, such as enacting productivity promotion laws and providing training sessions to mitigate job stress, offering job support to employees, and involving them in decision-making processes, fosters optimal communication between supervisors and employees. Generally, organizations that empower their employees with decision-making authority tend to experience lower stress levels, ultimately reducing burnout among emergency providers [22].
In PEMS, there are several issues regarding ambulance operations. These issues include the aging of the national ambulance fleet, a shortage of ambulances, inadequate maintenance, ambulance speed, the use of sirens and lights, delayed EMS response, and a lack of standard ambulance service centers and repair facilities. In Iran, recent economic sanctions have led to challenges in importing new and updated ambulances, resulting in an extended lifespan for existing ambulances, with some being used for over 15 years. Additionally, these sanctions have hindered the official agency responsible for managing ambulances in the country, leading to non-standardized service and repair processes at alternative centers.
Various vehicle characteristics influence ambulance safety, and ambulances must be highly visible to drivers and pedestrians to prevent crashes during emergency operations. For instance, it has been proposed that high-visibility green or yellow are better at catching attention than commonly used colors like red or orange. However, this suggestion is not universally followed, and many EMS systems use colors that are not easily visible at night and do not uniquely distinguish ambulances [27]. Implementing provisions that allow EMS providers in the rear compartment to remain stationary and seated for extended periods can significantly reduce equipment falls and subsequent injuries. For instance, automatic chest compression devices, mechanical ventilators, or the use of technology to enable hands-free electronic radio communication between the front and rear cabs of the ambulance are potential current solutions that could allow EMS providers to remain seated and restrained. However, these technologies may be expensive and not cost-effective for many PEMS [5].
Response time serves as a performance criterion for PEMS. Using speed as a measure of quality lacks meaning. Ambulance emergency responses, which may involve high speed, lights and sirens, could increase the risk of being involved in crashes [23]. EMS providers should be permitted to use lights and sirens with caution. To do this safely, accurate and correct information must be transmitted from the dispatch unit to the operation unit [5]. Driving speed plays a crucial role in road safety, as the risk of road crashes generally increases with higher speeds [28]. Speed can stress patients, staff, and drivers, leading to unsafe vehicle operations, especially among untrained drivers [29]. There is a global debate about the pros and cons of driving ambulances at high speeds. Many studies indicate that the time saved during emergency driving is minimal compared to non-emergency driving. On average, only 1 to 4 minutes are saved in urban and rural areas [30].
According to the study results in the field of environmental factors (patient and road conditions), the following are identified as significant factors: Public expectations for response time, unsafe roads, incorrect placement of emergency bases, unfamiliarity with the road and place, inadequate coverage of emergency services, agitated or violent patients, weather conditions, traffic, laypeople, availability of emergency responders, and investigation of the root causes of crashes. Physical environmental factors contribute to an ambulance’s safety, including driving speed, weather, and road conditions. Ambulances must be on the road in various weather conditions during daytime and nighttime hours. When approaching emergency scenes, ambulances often encounter numerous distractions, such as other responders, traffic, and bystanders [5, 31].
Ray and Kupas et al. compared 311 rural ACs and 1434 urban crashes. Rural ACs are more common on snowy roads (13% vs 5%) and night without streetlights (25% vs 4%). Researchers observed that driver error causes most crashes (75% for rural areas, 93% for urban areas), with vehicle or environmental conditions impacting rural drivers (25% vs 7%). Injury severity was similar for both crash types, although rural crashes more often involved no injuries (33% vs 20%). Additionally, alcohol and/or drug use by drivers was rare, <1% [32].
Among the limitations of this study, the working conditions of PEMS were such that it was possible that they would be called to perform a mission at any time; therefore, sometimes the interviews were left half-finished. To solve this issue, the interview appointment was coordinated with the participants during their free and non-working hours, even if possible. Another limitation is the lack of a statistical system for accurate registration of ACs and the fact that sometimes minor crashes are not reported by the staff due to the fear of stigma, so exact statistics on the incidence of ACs during operations in the country are not available.
Conclusion
EMTs face a dangerous and challenging work environment in an ambulance while providing emergency care to patients. Numerous research studies have shown that crashes are common. It is essential to establish standard guidelines requiring EMS providers to have basic driving skills before beginning work. It should be noted that driving, like other cognitive and psychomotor skills, requires continuous and dynamic retraining and evaluation. Individuals in a previous crash are particularly at risk of a second crash. It is crucial to retrain drivers after a collision to emphasize safety standards. To reduce and prevent ACs, it is necessary to change protocols and regulations throughout the chain of care, especially related to ambulance operations, to reduce the speed limit. Ambulance drivers must understand the risks and benefits of rapid emergency transport to ensure the speed limit is followed. A slower ambulance speed does not affect the outcome of most patients except in critical cases because driving at higher speeds does not significantly reduce transport times. Considering the nature of PEMS work, ACs is likely to be involved in this profession. Therefore, it is recommended that a committee be formed to investigate such crashes. This committee will provide material and psychological support to the personnel involved in the crash and conduct a “root cause analysis” for each ACs to fundamentally examine the causes and provide necessary measures to eliminate the contributing factors.
Ethical Considerations
Compliance with ethical guidelines
The present study was approved by the Ethics Committee of Shahrekord University of Medical Sciences, Shahrekord, Iran (Code: IR.SKUMS.REC.1401.151). After selecting the eligible participants, the researcher was introduced to them, and the study’s objectives were elaborated for the participants. The informed consent was obtained from the subjects, and they were assured that their information would remain confidential.
Funding
The project was financially supported by Shahrekord University of Medical Sciences, Shahrekord, Iran (Grant No.: 6499).
Authors' contributions
Study design and data analysis: Rahim Ali Sheikhi, Mohammad Heidari and Hamid Jafari; Data collection: Sadegh Heydarpoor; Review and editing: Mohammad Heidari; Data interpretation and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude to the Deputy of Research and Technology, the Community-Oriented Nursing Midwifery Research Center of Shahrekord University of Medical Sciences and all participants who assisted us in this research work.
References
Medical care management outside the hospital is handled by prehospital emergency medical services (PEMS). It is a vital component of the healthcare system, intended to respond to crashes and time-sensitive illnesses. PEMS plays a critical role as the first line of treatment for emergency patients [1]. The system’s activities include answering phone calls, dispatching to the scene, providing on-site care by trained professionals and continuing care in a vehicle, such as an ambulance [2].
Working in PEMS is one of the most challenging and stressful situations within the healthcare system, and ensuring the safety of patients and responders is the top priority during PEMS care [3]. PEMS faces three main challenges: Challenges in human resources (individual characteristics of human resources and personnel’s dissatisfaction), challenges in an organization (structural challenges, lack of equipment, and human resource limitation) and sociocultural challenges (environmental-social and cultural challenges) [4, 5].
The danger of ambulance transport is inherent. There is ample evidence that the ambulance is a challenging work environment with many risks for patients and EMTs [6]. EMTs must travel during daytime and nighttime hours and encounter various hazardous weather, road, and traffic conditions. Ambulance drivers frequently face stressful situations as they travel at high speeds and in vehicles with poor maneuverability [7].
One of the main challenges for EMTs is driving an ambulance and crash caused by emergency services. It is essential to investigate the crash prevention and care services provided by EMTs in the PEMS and the challenges involved in improving safety services at the EMS level. EMTs possess substantial knowledge in this field and are well-informed about the associated challenges [4]. ACs have always been among the challenges of the health and treatment field for various reasons, including the social burden of the crash, the possibility of morbidity and mortality of patients, companions and EMTs, and the high cost of rebuilding damaged ambulances [7].
ACs can harm the PEMS. They may make ambulances inoperable and reduce emergency capacity. They can injure technicians and patients in the ambulance and damage third parties. They can also incur costs, like ambulance repairs and compensation for the injured [8]. According to the police report, about 1000 ACs occurred in 2021. Encountering ACs can create many problems for the personnel involved, and up to 15% of these crashes can result in the deaths of EMTs, which are preventable [9]. The potential for injuries to EMTs and delays in patient care caused by ACs has caused global attention. Ambulance delays pose a significant barrier to patients receiving timely care and can worsen a patient’s condition. Traffic congestion has caused delays that have led to the deaths of more than 20% of patients in need of emergency treatment while on their way to a treatment center [10]. ACs are four times more likely to cause fatalities than other types of crashes, according to research [11]. The occupational fatality rate among EMS workers in the US was estimated at 12.7 per 100000 workers per year, compared with a national average of 5 per 100000 workers per year [12]. There are at least 6500 yearly crashes because of inadequate vehicle performance standards, improper maintenance, variable operator training, and failure to use safety restraints correctly [13].
Accurate data on ACs during operations in Iran has not been recorded or published. In a study by Shakeri and Ghanion, 46 ACs were reported during 2012-2016. Most ACs (35%) occurred in 2014. Of the 109 reported injuries resulting from ACs, 42 cases (39%) and 13 cases (25%) were related to the injuries and death of the ambulance driver and technician, respectively [14]. However, the National Medical Emergency Organization has run programs like “defensive driving” training in recent years. The effectiveness of such programs has not yet been adequately proven [15].
The Haddon matrix approach was developed in the 1950s and utilized during the 1960s and 1970s. The fundamental concept of systems theory is that incidents happen when there is misalignment in the relationships between the components of complex systems. This approach holds that all the components are equally crucial for the road system’s successful operation. Systems theory aims to mitigate crashes by modifying the elements of the transportation system. It emphasizes the importance of road engineering and vehicle safety. As a crash prevention theory, systems theory has been more successful than other theories. In developed countries, crash rates have been significantly reduced due to improvements in road systems, traffic control, and vehicle design [16].
Iran has areas that are difficult to reach, rural roads that are sometimes unsafe and a lack of enough ambulances. The quality and timeliness of emergency medical assistance are impacted by this situation, which creates financial and psychological problems. EMTs’ experiences during emergency operations were examined in a research study using the Haddon matrix framework. The study aims to identify safety issues and propose solutions to improve EMS and reduce adverse consequences.
Materials and Methods
Research design
A framework analysis approach was used in this qualitative study, which is a method for qualitative data analysis [17]. This study used the basic framework derived from the Haddon matrix approach. Systems theory posits that crashes are caused by misalignments in the relationships between the components of a complex system. According to this approach, for the successful operation of the road, none of the components of the transportation system (human, vehicle, and road) can be considered more important than the other components [16].
Participants and data collection
The data were collected through in-depth and semi-structured interviews. The research team developed the interview questions with input from the literature and then reviewed and modified them with feedback from several experts. The main question was, “How was your experience of a crash with an ambulance during an operation?” and specific questions followed. The participants were EMTs with experience in at least one AC. The sampling was purposeful and continued until data saturation. A total of 18 interviews were conducted with EMTs, lasting between 60 and 90 minutes each. The interviews were recorded with the participants’ informed consent, and a consent form was completed at their workplace. The researchers immediately transcribed the recordings.
The inclusion criteria require willingness and consent to participate in the study, possession of a B1 or B2 type certificate, a minimum of 3 years of operational work experience in PEMS, and participation in at least one AC during emergency missions. The exclusion criteria also include unwillingness to continue participating in the research process.
Data analysis
The data were analyzed using the framework analysis method with MAXQDA software, version 10. This method combines the initial idea (deductive approach) and experimental issues (inductive approach) in the analysis process. We used framework analysis to analyze the responses to question 9. Framework analysis is a rigorous five-stage method for analyzing qualitative data. The five stages are as follows: Familiarization with the responses by reading completed questionnaires, identifying key themes in the responses (we also used predefined issues focusing on benefits, problems, and study objectives to develop the thematic framework), indexing that involves copying all relevant participant quotes from the questionnaires and placing them in a Word document under relevant themes/subthemes identified by participant number, charting that involves iteratively reviewing and revising the initial framework (we abandoned initial benefit/problem themes because participants viewed some themes as either benefits or problems and reach an agreement on a final four-theme framework that includes subthemes), mapping and interpretation that involves charting the themes with a summary of the main descriptive comments and creating an explanatory account.
The authors can provide the index of all responses and framework history upon request [17].
Rigor
The researchers spent enough time gaining a deep and accurate understanding of the information to ensure the accuracy of the data. Four criteria were used to assess the validity and reliability of this study: Acceptability, similarity, conformability, and transferability. To this end, several experts reviewed and revised the interviews and the codes and categories that emerged from them. The credibility of the findings was also assured with constant engagement with the subject matter. Qualitative research experts reviewed and confirmed the interviews and codes. The study’s methods were detailed so others could verify and improve the findings. Two people, similar to the participants, confirmed the findings’ transferability. They were not participants [18].
Results
Demographic characteristics
All 18 study participants were male. It should be noted that in Iran’s PEMS, EMTs are exclusively male [19]. The participants’ age range was between 26 and 52. Additional information about the participants can be found in Table 1. Table 2 classified the findings into three main classes and 27 subclasses based on the Haddon matrix framework in three phases: Before, during and after the crash.
Host (EMTs)
Before the crash took place
In the PEMS, each emergency base has an ambulance staffed with two EMTs dispatched to assist in receiving the mission from the dispatch unit. According to the work rules, both EMTs must possess a special license to drive an ambulance (B2 type) and one of them will be responsible for driving the ambulance when dispatched to the scene.
Personnel health
Physical fitness and mental health are assessed at the time of student admission to the emergency medicine field. This evaluation is also required for employment at PEMS [2]. Unfortunately, throughout the years of service, such assessments have not been performed, and the physical and mental well-being of the staff has not been taken into account or evaluated.
Recruitment in the PEMS is done among university graduates, and there are two stages of written and practical tests. Physical criteria include height, weight, body mass index (BMI), physical fitness tests, mental tests, etc. The most crucial challenge in recruitment is the lack of graduates, and a reduction follows this in the number of applicants for employment [20].
“When EMTs are relieved from physical fitness requirements due to recruitment, they may pay less attention to staying fit and agile. This condition can lead to weight gain, reduced mobility and decreased agility and reaction time during emergency operations. I have also heard that some EMTs may turn to drug abuse, which can reduce their concentration, accuracy, and decision-making ability while driving and performing operations” (participant [P] 3).
Lack of knowledge and skills
EMTs lack knowledge and skill in two main areas. First is the understanding of driving laws and regulations. EMTs lack sufficient knowledge about driving rules and regulations in the country, leading to non-compliance. The laws regarding emergency vehicles include exceptions, leading to misunderstandings. This misunderstanding may result in false confidence and potentially cause crashes while driving.
“I didn’t have 100% knowledge of the traffic rules, and I thought the ambulance was always right in an emergency, and you could go at any speed and in any direction. However, it was not like that. The traffic rules change over time, and we don’t always have enough information about them, so sometimes this lack of knowledge leads us to not comply with them” (P9).
Most of Iran’s PEMS workforce is young. Most recruits are between 22 and 25. Some employees lack driving experience and do not possess a driver’s license. In Iran, individuals can obtain a driver’s license at 18, so even those with permits have limited driving experience. While having a driver’s license is a requirement for employment at PEMS, in recent years, due to personnel shortages, EMTs without a permit have been hired with the expectation that they obtain one within a specified period. Consequently, many young EMTs have their first driving experience while operating an ambulance and thus may lack sufficient driving skills. Given the unique challenges of driving an ambulance in emergencies and the drivers’ lack of experience, the risk of crashes is heightened.
“Many of us in the EMS lack experience driving ambulances. When we start working in the EMS, we often drive an ambulance for the first time, which presents its challenges. Ambulances are larger than our vehicles, making driving and parking more difficult. While having a driver’s license is a requirement, gaining driving experience and skills is crucial for effective rescue operations” (P4).
The primary responsibility of the PEMS is to maintain the ambulances, which are essential for carrying out missions. A lack of knowledge about an ambulance’s technical aspects can cause it to fail to meet required standards during missions. This condition may lead to crashes due to technical defects. Inadequate driving skills for ambulance operations are a significant factor in these crashes. PEMS in Iran uses only Mercedes-Benz Sprinter ambulances, and as a result, many EMTs, especially new personnel, lack the necessary skills to operate these ambulances.
“Driving an ambulance requires a high level of skill that not everyone has. Ambulances differ from regular cars and have a higher roof, making driving more challenging, especially at high speeds. Additionally, ambulances are not regularly available, and driving them typically requires working shifts to gain the necessary skills” (P6).
Staff shortage
One of the significant issues affecting the country’s PEMS is the shortage of EMTs, which has been a longstanding problem. Individuals with associate’s and bachelor’s degrees can enroll in PEMS training programs in Iran. However, the academic infrastructure for PEMS has not kept pace with its rapid development, resulting in a scarcity of specialized professionals in this field. The shortage of personnel has led to longer working hours, causing fatigue and job burnout and subsequently increasing the risk of crashes. Since resilience helps prevent job burnout, we should hire more resilient staff in this field [21]. Additionally, there is a shortage of EMTs holding a B2-type ambulance driver’s license. This shortage has led to hiring emergency medical degree holders without ambulance driver’s licenses, forcing licensed technicians to drive during missions, leading to fatigue and reduced focus, thereby increasing the risk of crashes.
“Every day, we face a staff shortage in the prehospital setting. This condition makes us even more concerned because forced overtime exhausts us and decreases our concentration. We find it difficult to focus as our thoughts revolve around being away from our families” (P2).
Work ethics
The lack of responsibility for the assigned duties has led to negligence in maintaining the ambulances. As a result, the useful life of these vehicles in the PEMS is shortened, and the ambulances do not perform efficiently during operations.
“Our colleagues usually do not take good care of ambulances. They take much better care of their cars because they have to pay for not taking care of them, but the government pays for the cost of the ambulances” (P10).
During the crash
Carelessness and high-speed
Time plays a crucial role in delivering PEMS. Prompt provision of medical assistance is essential, especially during the “golden time.” However, some EMTs may feel compelled to compensate for lost time by speeding and driving under unsafe conditions. One significant contributing factor to ambulance speeding and the increased risk of crashes is the dispatch unit’s announcement of emergency conditions for critical patients (Code: 10-33). Moreover, providing or receiving incorrect addresses for the assistance location adds to the pressure and stress experienced by EMTs.
“The role of the dispatch and operations unit is crucial. However, the use of the 10-33 code by the dispatch unit caused significant stress, which is not appropriate” (P6).
“The dispatch unit plays a crucial role. For instance, sending you to an area outside your range can make you nervous and lead to a crash. It’s important to follow the 10-33 code and move faster, but going too far can also create conditions for a crash. Additionally, if the dispatch provides the wrong address, it can confuse you and lead to driving errors such as crossing the road multiple times, reducing your concentration while driving” (P18).
Stress and fear
EMTs’ primary fears include arriving late, potential arguments and conflicts with patients and their families, and unfamiliar environments. Those with a history of crashes also fear another crash, injuring themselves, their colleagues, and the patient and being questioned by the organization.
“Increased fear and stress raise the probability of a crash. Error rates rise, and performance deteriorates, making it difficult to manage the crash scene. Work efficiency decreases, and normal control is lost. Mental conflict and signs of impatience arise, leading to aggressive reactions to even insignificant matters. This condition could escalate to conflicts with colleagues or patients” (P5).
Employee burnout
EMTs face stressful environments such as crash scenes with multiple injured and critical patients and increasing shifts without enough rest, which are very challenging to work in PEMS. Job stress can directly affect the emotional exhaustion, depersonalization, and personal inadequacy of PEMS workers and generally cause burnout [22].
“Our work is extremely demanding and sensitive. The increase in work shifts, driven by financial and economic needs, disrupts our sleep patterns and keeps us away from our families. All these factors contribute to our physical and mental exhaustion, leading us to lose our motivation to work gradually” (P11).
After the crash
Negative effects after the crash
Operational forces with a history of acute care suffer short- and long-term complications after a crash. They lose their confidence in driving and may not want to drive anymore, or they may drive at low speeds with excessive caution, causing delays and disruptions in the delivery of assistance. Posttraumatic stress disorder (PTSD) is one of the long-term complications that EMTs suffer from, especially in crashes involving injury and mortality, which can significantly affect their performance. Stigma from colleagues and the organization is also a significant factor contributing to the mental and emotional challenges faced by EMTs. The feeling of failure and self-blame intensifies among EMTs, leading to a loss of trust and reduced work efficiency, impacting their self-confidence, trust in the higher-level system, colleagues, and public trust in the PEMS.
“After the crash, I noticed a significant decrease in my performance. I had trouble concentrating and dwelling on the crash for extended periods. The fact that someone died in the crash left me feeling depressed and caused me to lose my appetite for quite some time. I struggled with low motivation at work and often blamed myself for what had happened. As a result, I became more cautious, driving slower and losing my sense of urgency. I was constantly vigilant, fearing another mishap. The incident stressed me and caused me to withdraw from friends, occasionally taking days or months off from work to collect myself” (P8).
“How your colleagues view your changes, and they label you as reckless and dangerous within the system, is very frustrating. This condition also impacts your personal life. You are no longer patient with other tasks and get upset about the next operation, sometimes even with yourself. The severe stress leads to digestive problems and vomiting, making it impossible for you to serve the patients effectively” (P14).
Feeling unsupported
After responding to a medical emergency, EMTs have expressed concerns about the lack of financial and psychological support from both the authorities and the organization. They are also facing an increased workload due to having to cover some of the costs of repairing and rebuilding the ambulance and insufficient insurance coverage for ambulances.
“The organization does not provide much support. It looks for the culprit but does not offer mental, physical, or financial assistance. It fails to address the root cause of the issue and does not try to prepare you for future work days. There is no plan in place, and there is no committee to address the important causes of the issue or provide solutions. Additionally, the organization does not offer access to a psychologist or take preventive measures to avoid similar incidents in the future” (P4).
Agent (ambulance)
Before the crash took place
Worn-out ambulances
The country’s ambulance system is in poor condition. Due to economic sanctions, new and updated ambulances have not been imported for many years. As a result, existing ambulances are being overused and do not meet emergency system standards. Most ambulances in the country are not domestically manufactured (Mercedes-Benz Sprinter), resulting in limited service centers and guarantees. This condition makes finding original auto spare parts challenging, leading to technical defects. The use of fake auto spare parts increases the risk of crashes.
“The country’s ambulance system is aging, with most ambulances being in service for over 15 to 20 years, well beyond their intended lifespan. It’s becoming increasingly challenging to find original spare parts, leading to the use of second-hand or non-original parts, which in turn lead to additional issues” (P13).
Ambulance shortage
The lack of new ambulances in the PEMS has led to a persistent shortage of vehicles, resulting in the overuse of existing ones. Ambulances are not allocated based on regional geography and climate conditions, leading to inefficiencies in cold and inaccessible areas. In urban settings, the size of ambulances can cause delays in providing aid, especially in older parts of the city. Additionally, the outdated ambulances lack modern features such as GPS, making it challenging to locate the assistance site.
“There has always been a shortage of ambulances. No new ambulances are available whenever a new emergency base is set up, so they must refurbish the existing ones and put them into service. Operating these ambulances in winter is extremely challenging, especially in the city’s narrow streets. The ambulances are unsuitable for such conditions” (P3).
Improper maintenance
Every vehicle requires regular checks and servicing to be ready for operation. However, an ambulance is a rescue vehicle and must always be prepared. One of the primary responsibilities of EMTs is to ensure the ambulance is operating correctly at the start of each shift, and this daily check should be documented.
During the crash
Speed and lights-and-siren use the stability of the vehicle in transit
Emergency providers often drive high-speed ambulances to reach sites quickly. This condition is especially true when a command or emergency (Code: 10-33) is issued from the dispatch center to allow the ambulance to pass through using lights and sirens. However, it is essential to note that this can also increase stress and distress for the driver, patient, patient’s companions, and other citizens.
“The new ambulances have good acceleration and speed. When the lights and sirens are on, the EMTs may experience increased stress and false confidence. This condition can lead to the belief that everyone is obligated to yield, allowing the ambulance to maneuver as needed, increasing the chance of a collision” (P8).
After the crash
Delay in providing EMS
A crash during the rescue operation causes interference and delays, which can result in injuries to the EMTs, patients, and their companions. Additionally, the ambulance is taken out of service after a crash. Due to the severe shortage of ambulances, replacing them becomes more challenging. Sometimes, EMTs are unfamiliar with the replacement ambulance, increasing the probability of errors or crashes.
Lack of standard ambulance repair shop
After a crash, the top priorities are to repair and reconstruct the ambulance so it can return to service quickly. A major challenge after a crash is the lack of authorized repair shops and auto parts. Non-standard repairs significantly raise the risk of future crashes.
“Ambulances have often been involved in crashes, and while air conditioning issues are sometimes unavoidable, they are not always fully repaired. Instead, they are rushed into service, meaning you could drive a vehicle with technical defects and non-original auto spare parts” (P5).
Environment (the route and location of the help requestor)
Before the crash took place
Unsafe roads and incorrect placement of emergency bases
Driving on non-standard roads, especially without warning signs, increases crash risks for EMTs. Improper site selection and establishing emergency bases in incident-prone areas can lead to longer travel distances to reach the scene of an emergency, increasing the probability of crashes on non-standard roads and delaying the time it takes to assist.
“The construction of the emergency base is done in the most distant and inappropriate place, so it takes a long time for the operation unit to enter urban or rural areas. This late arrival at the crash scene angered and caused complaints among the patient and his companions” (P4).
During the crash
Unfamiliarity with the route and place
The shortage of staff and frequent movement of EMTs between bases has made them unfamiliar with the area and the best routes for seeking help. The lack of online routing tools has made their work harder. Callers often provide incorrect or incomplete addresses in emergencies due to high stress. Also, animals on roads, especially in forests and rural areas, raise crash risks.
Inadequate coverage of EMS
Despite introducing the PEMS (portable emission measurement system) in the country, many areas and roads are still not adequately covered by the PEMS. This condition has led to delays in providing aid, increased burnout, and longer driving distances for the EMTs.
“Driving with an incorrect address, frequent stops to check the map, and many road crossings contribute to reduced focus on the road. Unfamiliarity with the area means not knowing alternate routes with less traffic, and longer routes increase travel time, potentially leading to crashes” (P17).
Agitated or violent patients, adverse weather conditions, road traffic, laypeople’s
The patient’s critical condition and their companions’ pressure can stress EMTs. This condition may cause them to speed in the ambulance. Weather conditions, road traffic, and bystanders gathering at the crash scene can also affect the relief effort. When a patient is in critical condition, the patient’s companions may urge the driver to go faster. The dispatcher unit also announces the critical situation, which may increase speed. Also, consider weather, slippery roads, heavy traffic (especially during school closures), bystanders at the crash scene, disruptions to treatment, and the risk of another crash.
After the crash
Availability of PEMS responders for AC and failure to perform root cause analysis
After a crash, an alternative ambulance must be available for relief operations. This is to minimize patients’ wait time in any situation. By analyzing the causes of these crashes, we can reduce their frequency. We should examine three areas: Personnel, vehicles and the environment.
“Unfortunately, air crashes always happen and are inevitable. However, their causes have never been scientifically and fundamentally investigated in our country, and written instructions have not been developed for air crashes. Unfortunately, the rate of such crashes is also increasing” (P11).
Discussion
The Haddon matrix has three key components that influence a crash. They are the host, agent, and the physical and social environment. Host refers to the individual or individuals at risk, such as EMTs or the patient. The agent refers to the energy applied during an injury, in this case, the ambulance. The physical environment refers to the injury site. It includes road design maintenance and ambulance design. The social environment refers to social, legal, and cultural norms and practices. The second dimension of the Haddon matrix shows the timing of factors that contribute to the event’s occurrence: Before the crash, crash, and after the crash [23]. In Haddon’s injury matrix, EMTs serve as hosts, allowing us to examine various aspects of injuries that occur in the ambulance during patient care and transport. According to the results, essential host factors that contribute to the safety and reduction of adverse events include personnel health, lack of knowledge and skills, human resource shortages, work ethic, carelessness, high speed, stress and fear, burnout, negative effects after the incident, and feeling unsupported. In the study by Brice et al., essential host factors that contribute to ambulance safety include physical fitness, sleepiness, education, knowledge, skills, and capabilities [5].
The skill of the EMS driver plays a crucial role in ensuring the safety of both the vehicle occupants and the patient’s medical outcome. The data showed that 78% of study participants had a history of crashes. Custalow and Gravitz’s study found that ambulance drivers in crashes often had prior crashes. Forty-nine percent of the EMS providers had previous crashes [24]. EMS providers in good physical condition can deliver EMS to patients more quickly and effectively. The prevalence of substance abuse among EMS providers is not well documented, but it is believed to be as high as 40% in other emergency response professions [25].
The shortage of EMTs in the field of PEMS has led to increased workload and fatigue among these EMS providers, eventually resulting in job burnout. EMS providers frequently work 12-hour or 24-hour shifts with limited opportunities for meals or rest, leading to fatigue and adverse side effects. It has been discovered that extended working hours result in more medical errors and adverse side effects [26]. Moshtagh Eshgh et al. examined the occupational stress of PEMS personnel in Iran. The results showed that PEMS personnel’s work stress caused burnout. It led to emotional exhaustion, depersonalization, and feelings of inadequacy. Addressing the sources of stress and implementing measures to manage it, such as enacting productivity promotion laws and providing training sessions to mitigate job stress, offering job support to employees, and involving them in decision-making processes, fosters optimal communication between supervisors and employees. Generally, organizations that empower their employees with decision-making authority tend to experience lower stress levels, ultimately reducing burnout among emergency providers [22].
In PEMS, there are several issues regarding ambulance operations. These issues include the aging of the national ambulance fleet, a shortage of ambulances, inadequate maintenance, ambulance speed, the use of sirens and lights, delayed EMS response, and a lack of standard ambulance service centers and repair facilities. In Iran, recent economic sanctions have led to challenges in importing new and updated ambulances, resulting in an extended lifespan for existing ambulances, with some being used for over 15 years. Additionally, these sanctions have hindered the official agency responsible for managing ambulances in the country, leading to non-standardized service and repair processes at alternative centers.
Various vehicle characteristics influence ambulance safety, and ambulances must be highly visible to drivers and pedestrians to prevent crashes during emergency operations. For instance, it has been proposed that high-visibility green or yellow are better at catching attention than commonly used colors like red or orange. However, this suggestion is not universally followed, and many EMS systems use colors that are not easily visible at night and do not uniquely distinguish ambulances [27]. Implementing provisions that allow EMS providers in the rear compartment to remain stationary and seated for extended periods can significantly reduce equipment falls and subsequent injuries. For instance, automatic chest compression devices, mechanical ventilators, or the use of technology to enable hands-free electronic radio communication between the front and rear cabs of the ambulance are potential current solutions that could allow EMS providers to remain seated and restrained. However, these technologies may be expensive and not cost-effective for many PEMS [5].
Response time serves as a performance criterion for PEMS. Using speed as a measure of quality lacks meaning. Ambulance emergency responses, which may involve high speed, lights and sirens, could increase the risk of being involved in crashes [23]. EMS providers should be permitted to use lights and sirens with caution. To do this safely, accurate and correct information must be transmitted from the dispatch unit to the operation unit [5]. Driving speed plays a crucial role in road safety, as the risk of road crashes generally increases with higher speeds [28]. Speed can stress patients, staff, and drivers, leading to unsafe vehicle operations, especially among untrained drivers [29]. There is a global debate about the pros and cons of driving ambulances at high speeds. Many studies indicate that the time saved during emergency driving is minimal compared to non-emergency driving. On average, only 1 to 4 minutes are saved in urban and rural areas [30].
According to the study results in the field of environmental factors (patient and road conditions), the following are identified as significant factors: Public expectations for response time, unsafe roads, incorrect placement of emergency bases, unfamiliarity with the road and place, inadequate coverage of emergency services, agitated or violent patients, weather conditions, traffic, laypeople, availability of emergency responders, and investigation of the root causes of crashes. Physical environmental factors contribute to an ambulance’s safety, including driving speed, weather, and road conditions. Ambulances must be on the road in various weather conditions during daytime and nighttime hours. When approaching emergency scenes, ambulances often encounter numerous distractions, such as other responders, traffic, and bystanders [5, 31].
Ray and Kupas et al. compared 311 rural ACs and 1434 urban crashes. Rural ACs are more common on snowy roads (13% vs 5%) and night without streetlights (25% vs 4%). Researchers observed that driver error causes most crashes (75% for rural areas, 93% for urban areas), with vehicle or environmental conditions impacting rural drivers (25% vs 7%). Injury severity was similar for both crash types, although rural crashes more often involved no injuries (33% vs 20%). Additionally, alcohol and/or drug use by drivers was rare, <1% [32].
Among the limitations of this study, the working conditions of PEMS were such that it was possible that they would be called to perform a mission at any time; therefore, sometimes the interviews were left half-finished. To solve this issue, the interview appointment was coordinated with the participants during their free and non-working hours, even if possible. Another limitation is the lack of a statistical system for accurate registration of ACs and the fact that sometimes minor crashes are not reported by the staff due to the fear of stigma, so exact statistics on the incidence of ACs during operations in the country are not available.
Conclusion
EMTs face a dangerous and challenging work environment in an ambulance while providing emergency care to patients. Numerous research studies have shown that crashes are common. It is essential to establish standard guidelines requiring EMS providers to have basic driving skills before beginning work. It should be noted that driving, like other cognitive and psychomotor skills, requires continuous and dynamic retraining and evaluation. Individuals in a previous crash are particularly at risk of a second crash. It is crucial to retrain drivers after a collision to emphasize safety standards. To reduce and prevent ACs, it is necessary to change protocols and regulations throughout the chain of care, especially related to ambulance operations, to reduce the speed limit. Ambulance drivers must understand the risks and benefits of rapid emergency transport to ensure the speed limit is followed. A slower ambulance speed does not affect the outcome of most patients except in critical cases because driving at higher speeds does not significantly reduce transport times. Considering the nature of PEMS work, ACs is likely to be involved in this profession. Therefore, it is recommended that a committee be formed to investigate such crashes. This committee will provide material and psychological support to the personnel involved in the crash and conduct a “root cause analysis” for each ACs to fundamentally examine the causes and provide necessary measures to eliminate the contributing factors.
Ethical Considerations
Compliance with ethical guidelines
The present study was approved by the Ethics Committee of Shahrekord University of Medical Sciences, Shahrekord, Iran (Code: IR.SKUMS.REC.1401.151). After selecting the eligible participants, the researcher was introduced to them, and the study’s objectives were elaborated for the participants. The informed consent was obtained from the subjects, and they were assured that their information would remain confidential.
Funding
The project was financially supported by Shahrekord University of Medical Sciences, Shahrekord, Iran (Grant No.: 6499).
Authors' contributions
Study design and data analysis: Rahim Ali Sheikhi, Mohammad Heidari and Hamid Jafari; Data collection: Sadegh Heydarpoor; Review and editing: Mohammad Heidari; Data interpretation and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude to the Deputy of Research and Technology, the Community-Oriented Nursing Midwifery Research Center of Shahrekord University of Medical Sciences and all participants who assisted us in this research work.
References
- Yang W, Cao Q, Qin L, Wang X, Cheng Z, Pan A, et al. Clinical characteristics and imaging manifestations of the 2019 novel coronavirus disease (COVID-19): A multi-center study in Wenzhou city, Zhejiang, China. Journal of Infection. 2020; 80(4):388-93. [DOI:10.1016/j.jinf.2020.02.016] [PMID]
- Shakeri K, Jafari M, Khankeh H, Seyedin H. History and structure of the fourth leading emergency medical service in the world; A review article. Archives of Academic Emergency Medicine. 2019; 7(1):e17. [PMID]
- Cooney DR, Larson J. Emergency Vehicles. In: Cooney DR, editor. Cooney's EMS Medicine. New York: McGraw-Hill Education; 2016. [Link]
- Bayrami R, Ebrahimipour H, Rezazadeh A. Challenges of prehospital emergency in Mashhad: Qualitative study. Hospital Journal. 2017; 16(2):82-90. [Link]
- Brice JH, Studnek JR, Bigham BL, Martin-Gill C, Custalow CB, Hawkins E, et al. EMS provider and patient safety during response and transport: proceedings of an ambulance safety conference. Prehospital Emergency Care. 2012; 16(1):3-19. [DOI:10.3109/10903127.2011.626106] [PMID]
- Weiss SJ, Ellis R, Ernst AA, Land RF, Garza A. A comparison of rural and urban ambulance crashes. The American Journal of Emergency Medicine. 2001; 19(1):52-6. [DOI:10.1053/ajem.2001.20001] [PMID]
- Eksi A, Celikli S, Catak I. Effects of the institutional structure and legislative framework on ambulance accidents in developing emergency medical services systems. Turkish Journal of Emergency Medicine. 2015; 15(3):126-30. [DOI:10.1016/j.tjem.2015.11.006] [PMID]
- Sethasathien A, Sirisamutr T, Wachiradilok P, Dairoop S, Nimma S. 529 Ambulance crash in Thailand. London: BMJ Publishing Group Ltd; 2016. [DOI:10.1136/injuryprev-2016-042156.529]
- Maguire BJ. Transportation-related injuries and fatalities among emergency medical technicans and paramedics. Prehospital and Disaster Medicine. 2011; 26(5):346-52. [DOI:10.1017/S1049023X11006601] [PMID]
- Li M, Vanberkel P, Carter AJ. A review on ambulance offload delay literature. Health Care Management Science. 2019; 22(4):658-75. [DOI:10.1007/s10729-018-9450-x] [PMID]
- Watanabe BL, Patterson GS, Kempema JM, Magallanes O, Brown LH. Is use of warning lights and sirens associated with increased risk of ambulance crashes? A contemporary analysis using National EMS information system (NEMSIS) data. Annals of Emergency Medicine. 2019; 74(1):101-9. [DOI:10.1016/j.annemergmed.2018.09.032] [PMID]
- Barishansky RM, Streger MR. Occupational fatalities in emergency medical services. Annals of Emergency Medicine. 2003; 42(1):160. [DOI:10.1016/S0196-0644(03)70046-8] [PMID]
- Araujo GDM. Agricultural all-terrain vehicle safety [doctoral dissertation]. Berkeley: University of California; 2022. [Link]
- Shakeri K, Ghanion A. [Investigation of ambulance accidents in Iran 2013-2017 (Persian)]. Paper presented at: 8th International Congress on Health in Emergencies and Disasters. 22 April 2017; Tehran, Iran. [Link]
- Arak University of Medical Sciences and Health Services. [Defensive driving training and additional skills (Persian)]. Arak: Arak University of Medical Sciences and Health Services; 2022. [Link]
- Baru A, Azazh A, Beza L. Injury severity levels and associated factors among road traffic collision victims referred to emergency departments of selected public hospitals in Addis Ababa, Ethiopia: The study based on the Haddon matrix. BMC Emergency Medicine. 2019; 19(1):1-10. [DOI:10.1186/s12873-018-0206-1] [PMID]
- Srivastava A, Thomson S. Framework analysis: A qualitative methodology for applied policy research. 2009. Journal of Administration and Governance. 2021; 4(2):72-9. [Link]
- Sadeghi T, Kazemi M. Nursing student's viewpoints and experiences about clinical evaluation by 360 degree approach. Journal of Qualitative Research in Health Sciences. 2016; 5(3):273-82. [Link]
- Heidari M, Aliakbari F, Heydarpoor S, Nehrir B, Yadollahi S. Prehospital emergency service challenges in the face of the COVID-19 pandemic in Iran. Disaster Medicine and Public Health Preparedness. 2023; 17:e217. [DOI:10.1017/dmp.2022.141] [PMID]
- Bahadori M, Nasiripur A, Tofighi S, Gohari M. Emergency medical services in Iran: An overview. Australasian Medical Journal. 2010; 3(6):335. [DOI:10.4066/AMJ.2010.218]
- Shoja Fard J, Poursadegh N, Shahrashob Q, Zangisheh, S. [The relationship between job burnout and resilience in medical emergency personnel in Tehran (Persian)]. Journal of Rescue and Relief. 2014; 6(2):58-68. [Link]
- Moshtagh Eshgh Z, Peyman A, Amirkhani A, Taghinejad F. [The relationship between occupational stresses with job burnout in prehospital emergency staff (Persian)]. Jorjani Biomedicine Journal. 2014; 2(2):41-33. [Link]
- Runyan CW. Using the Haddon matrix: Introducing the third dimension. Injury Prevention. 2015; 21(2):126-30. [DOI:10.1136/ip.4.4.302rep] [PMID]
- Custalow CB, Gravitz CS. Emergency medical vehicle collisions and potential for preventive intervention. Prehospital Emergency Care. 2004; 8(2):175-84. [DOI:10.1016/S1090-3127(03)00279-X]
- Donnelly E, Siebert D. Occupational risk factors in the emergency medical services. Prehospital and Disaster Medicine. 2009; 24(5):422-9. [DOI:10.1017/S1049023X00007251] [PMID]
- Patterson PD, Weaver MD, Frank RC, Warner CW, Martin-Gill C, Guyette FX, et al. Association between poor sleep, fatigue, and safety outcomes in emergency medical services providers. Prehospital Emergency Care. 2012; 16(1):86-97. [DOI:10.3109/10903127.2011.616261] [PMID]
- Kupas D. Prevention vehicle panel. Paper presented at NAEMSP Ambulance Safety Conference. 2010. [Link]
- Nilsson G. Traffic safety dimensions and the power model to describe the effect of speed on safety [doctoral dissertation]: Univ.Lund: Lund Institute of technology; 2004. [Link]
- Kahn CA, Pirrallo RG, Kuhn EM. Characteristics of fatal ambulance crashes in the United States: An 11-year retrospective analysis. Prehospital Emergency Care. 2001; 5(3):261-9. [DOI:10.1080/10903120190939751] [PMID]
- Ho J, Lindquist M. Time saved with the use of emergency warning lights and siren while responding to requests for emergency medical aid in a rural environment. Prehospital Emergency Care. 2001; 5(2):159-62. [DOI:10.1080/10903120190940056] [PMID]
- Solomon SS, Hill PF. Emergency vehicle accidents prevention, reconstruction and survey of state law. Arizona: Lawyers & Judges Publishing Company, Inc; 2002. [Link]
- Ray AF, Kupas DF. Comparison of crashes involving ambulances with those of similar-sized vehicles. PreHospital Emergency Care. 2005; 9(4):412-5. [DOI:10.1080/10903120500253813] [PMID]
Type of article: Research |
Subject:
traffic accidents
Received: 2024/05/14 | Accepted: 2025/01/19 | Published: 2025/07/9
Received: 2024/05/14 | Accepted: 2025/01/19 | Published: 2025/07/9
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
